







J. Clin. Med. 2026, 15(12), 4607; https://doi.org/10.3390/jcm15124607 (registering DOI) - 13 Jun 2026
Abstract
Background/Objectives: In case of EDTA-induced pseudothrombocytopenia (PTCP), MgSO4-anticoagulated tubes are recommended for platelet counting, requiring the collection of an additional tube. The aim of this study was to analyze whether complete blood count (CBC) and differential performed on MgSO4
[...] Read more.
Background/Objectives: In case of EDTA-induced pseudothrombocytopenia (PTCP), MgSO4-anticoagulated tubes are recommended for platelet counting, requiring the collection of an additional tube. The aim of this study was to analyze whether complete blood count (CBC) and differential performed on MgSO4-anticoagulated tubes were comparable to the results obtained on K3-EDTA samples, and to characterize the stability of the CBC over a 24 h period. Methods: In 355 patients (70 with a confirmed PTCP and 285 without PTCP), we compared CBC results obtained on K3-EDTA- and MgSO4-anticoagulated tubes, using DxH800 analyzers. In 33 cases, a differential was available for both anticoagulants, and for 10 patients, samples were re-analyzed 6, 12, and 24 h after the first determination. Results: In the presence or absence of clumps, white blood cell (WBC) count, hematocrit, and mean corpuscular volume (MCV) were slightly lower in MgSO4 than in K3-EDTA tubes, whereas mean corpuscular hemoglobin concentration (MCHC) was slightly higher. Mean platelet volume (MPV) was significantly lower on MgSO4- than on K3-EDTA-anticoagulated tubes. Values were highly correlated between both anticoagulants, and mean relative biases (MRBs) were below Ricos’s recommendations, except for MCHC and MPV. For differential, neutrophils were significantly lower on MgSO4- in comparison to K3-EDTA-anticoagulated tubes (MRB = −2.9%, below Ricos’s optimal bias). The morphology of white blood cells (WBCs) was similar on both anticoagulants. During storage at room temperature, MCV and red cell distribution width increased slightly, but the increase was more pronounced in K3-EDTA than in MgSO4 tubes. Conclusions: CBC and differentials obtained with the DxH 800 analyzer on MgSO4-anticoagulated samples are similar to those obtained with K3-EDTA, except for MPV.
Full article
(This article belongs to the Section Hematology)
►
Show Figures
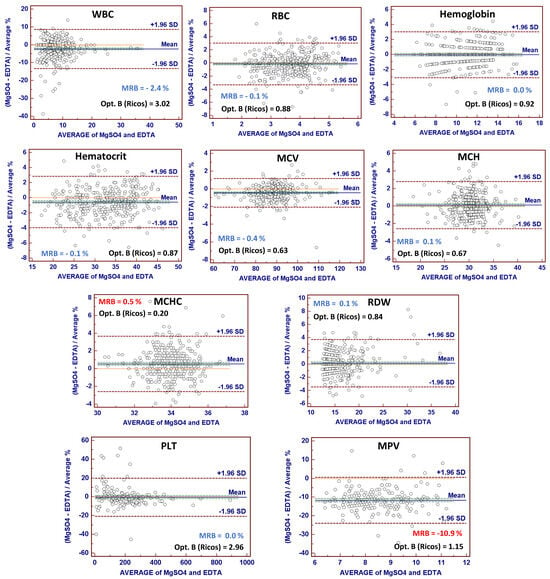
Figure 1







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}