






Curr. Oncol. 2026, 33(7), 416; https://doi.org/10.3390/curroncol33070416 - 10 Jul 2026
Abstract
The prognostic significance of next-generation sequencing (NGS) findings during the hormone-sensitive phase of prostate cancer remains incompletely characterized. This retrospective cohort study included 92 patients who underwent NGS analysis on tumor tissue between 2019 and 2025. The primary endpoint was time to castration-resistant
[...] Read more.
The prognostic significance of next-generation sequencing (NGS) findings during the hormone-sensitive phase of prostate cancer remains incompletely characterized. This retrospective cohort study included 92 patients who underwent NGS analysis on tumor tissue between 2019 and 2025. The primary endpoint was time to castration-resistant prostate cancer (CRPC) from androgen deprivation therapy (ADT) initiation; secondary endpoints were overall survival from ADT initiation (OS-ADT) and from diagnosis. Kaplan-Meier and Cox regression analyses were performed. CRPC developed in 66 patients (71.7%) at a median of 21.1 months. The most frequently altered genes were ATR (35.9%), PTEN (28.3%), TP53 (26.1%), and BRCA2 (15.2%). KMT2C alteration (5.4%) was the strongest independent genomic predictor of shorter time to CRPC (HR = 6.804, p = 0.003) and OS-ADT (HR = 4.730, p = 0.019). TP53 alteration independently predicted shorter OS-ADT (HR = 1.810, p = 0.038). High genomic burden independently predicted shorter time to CRPC (HR = 1.917, p = 0.032). Homologous recombination repair deficiency was not associated with outcomes, attributable to high ATR alteration frequency introducing pathway heterogeneity. Mismatch repair deficiency showed a borderline association with shorter OS-ADT (20.7 vs. 44.0 months; p = 0.060). An exploratory composite risk score stratified patients into three prognostic groups with markedly different outcomes (HR = 7.904, p = 0.001). NGS analysis during the hormone-sensitive phase identifies independent predictors of castration resistance, supporting its integration at ADT initiation for risk stratification and biomarker-guided treatment planning.
Full article
(This article belongs to the Special Issue Targeted Molecular Therapeutics for Urologic Cancers: Advances, Emerging Strategies, and the Road Ahead)
►
Show Figures
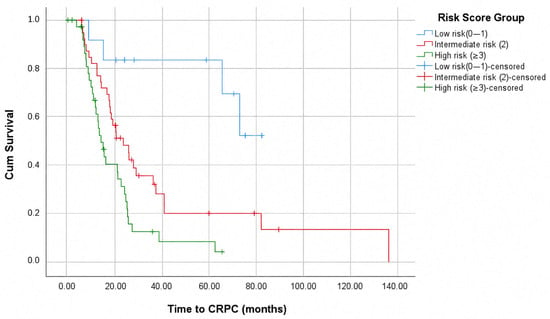
Figure 1










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}