




Curr. Oncol. 2026, 33(7), 417; https://doi.org/10.3390/curroncol33070417 - 11 Jul 2026
Viewed by 378
Abstract
►
Show Figures
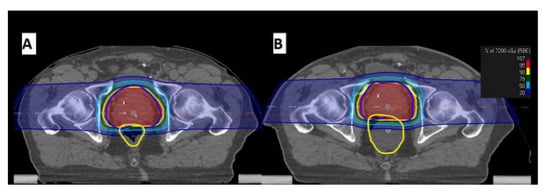
Focal therapy (FT) for localized prostate cancer induces architectural changes that complicate post-treatment multiparametric magnetic resonance imaging (mpMRI) surveillance. The Prostate Imaging after Focal Ablation (PI-FAB) system was developed to standardize the evaluation of in-field recurrence on mpMRI. This study assessed the diagnostic
[...] Read more.
Focal therapy (FT) for localized prostate cancer induces architectural changes that complicate post-treatment multiparametric magnetic resonance imaging (mpMRI) surveillance. The Prostate Imaging after Focal Ablation (PI-FAB) system was developed to standardize the evaluation of in-field recurrence on mpMRI. This study assessed the diagnostic performance and inter-reader agreement of PI-FAB following focal cryoablation for localized prostate cancer. In this retrospective study (October 2019 to January 2024), 85 patients (140 lesion sites) underwent post-FT mpMRI and biopsy. Two radiologists (11 and 4 years of experience) independently scored mpMRIs using the three-point PI-FAB scale. Metrics included sensitivity, specificity, PPV, NPV, and accuracy. Inter-reader agreement was measured via quadratic weighted Cohen’s kappa (κ). Reader 1 (more experienced) demonstrated 83.9% sensitivity, 84.4% specificity, 60.5% PPV, and 94.8% NPV. Reader 2 demonstrated 71.4% sensitivity, 87.5% specificity, 58.8% PPV, and 92.5% NPV. Both achieved 84.3% accuracy. Inter-reader agreement was moderate (κ = 0.60). PI-FAB provides good diagnostic performance for detecting in-field recurrence after cryoablation. While reader experience may impact sensitivity, moderate agreement across experience levels supports PI-FAB’s validity and potential clinical utility in standardizing post-FT surveillance.
Full article

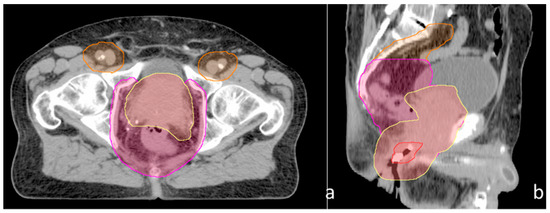
Figure 1






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}