


Curr. Oncol. 2026, 33(6), 323; https://doi.org/10.3390/curroncol33060323 - 29 May 2026
Abstract
Solitary fibrous tumor/hemangiopericytoma (SFT/HPC) of the central nervous system is a rare mesenchymal neoplasm with a propensity for late recurrence and distant metastasis. Pancreatic metastasis from intracranial SFT/HPC is exceptionally uncommon and may mimic primary pancreatic neoplasms, particularly pancreatic neuroendocrine tumor (PanNET). We
[...] Read more.
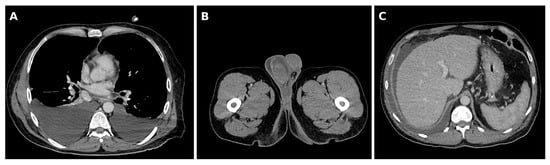
Solitary fibrous tumor/hemangiopericytoma (SFT/HPC) of the central nervous system is a rare mesenchymal neoplasm with a propensity for late recurrence and distant metastasis. Pancreatic metastasis from intracranial SFT/HPC is exceptionally uncommon and may mimic primary pancreatic neoplasms, particularly pancreatic neuroendocrine tumor (PanNET). We report a 52-year-old man with a documented history of recurrent intracranial SFT/HPC, historically diagnosed as hemangiopericytoma, who developed a hypervascular pancreatic tail lesion 11 years after the initial intracranial tumor diagnosis. Contrast-enhanced imaging and endoscopic ultrasound-guided fine-needle aspiration initially suggested a primary pancreatic neoplasm, including solid pseudopapillary neoplasm or PanNET, and a definitive preoperative diagnosis could not be established. Following laparoscopic resection, histopathological examination revealed a spindle-cell tumor with a rich vascular pattern. Immunohistochemistry documented STAT6 positivity, together with vimentin and Bcl-2 positivity, supporting the diagnosis of pancreatic metastasis from SFT/HPC. The patient later developed unresectable recurrent pancreatic disease and underwent stereotactic radiotherapy, showing radiological disease control at follow-up. This case highlights that pancreatic metastasis from intracranial SFT/HPC, although extremely rare, may occur after a prolonged latency period and mimic a hypervascular primary pancreatic neoplasm. In patients with a history of intracranial SFT/HPC, late metastatic disease should be considered, and definitive diagnosis relies on histopathological examination and targeted immunohistochemistry.
Full article
(This article belongs to the Section Gastrointestinal Oncology)
►
Show Figures
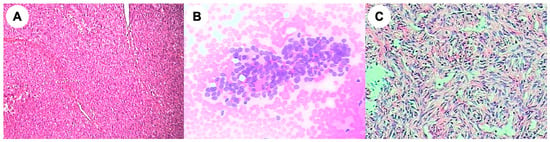
Figure 1







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}