


Curr. Oncol. 2026, 33(6), 340; https://doi.org/10.3390/curroncol33060340 (registering DOI) - 6 Jun 2026
Abstract
Short-term mortality following the last dose of immune checkpoint inhibitors (ICIs) is an increasingly recognized real-world outcome measure, yet its clinical predictors remain poorly characterized. This multicenter retrospective study included 458 consecutive patients with advanced melanoma, non-small cell lung cancer, or renal cell
[...] Read more.
Short-term mortality following the last dose of immune checkpoint inhibitors (ICIs) is an increasingly recognized real-world outcome measure, yet its clinical predictors remain poorly characterized. This multicenter retrospective study included 458 consecutive patients with advanced melanoma, non-small cell lung cancer, or renal cell carcinoma who received ICIs at four tertiary centers in Turkey between 2018 and 2023. The primary endpoint was 30-day mortality after the final ICI dose. Among 458 patients, 71 (15.5%) died within 30 days. Multivariable logistic regression identified ECOG performance status ≥ 2, number of metastatic sites ≥ 3, and log-transformed C-reactive protein-to-albumin ratio (log-CAR) as independent predictors of 30-day mortality in Model 1 (AUC 0.954), while ECOG PS ≥ 2, brain metastasis, metastatic sites ≥ 3, and log-NLR were independent predictors in Model 2 (AUC 0.912). In the lung cancer subgroup, log-CAR and NLR remained independent predictors while ECOG PS did not. Patients who died within 30 days had significantly shorter progression-free survival (1.18 vs. 4.63 months) and overall survival (2.30 vs. 14.39 months) compared with survivors. These findings suggest that routine assessment of inflammatory and nutritional biomarkers alongside tumor burden parameters may help identify patients at high risk of early mortality and inform the timing of supportive care in ICI-treated populations.
Full article
(This article belongs to the Section Palliative and Supportive Care)
►
Show Figures
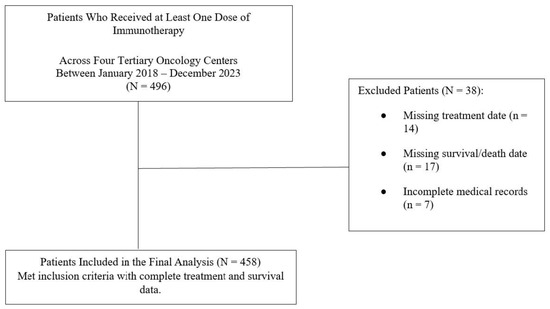
Figure 1


















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}