


Curr. Oncol. 2026, 33(6), 307; https://doi.org/10.3390/curroncol33060307 - 25 May 2026
Abstract
Background: The transition from the parenteral to subcutaneous application of systemic oncological therapy represents one of the most important innovations in modern oncology, as it affects the quality of life of patients as well as the organization of work and the management of
[...] Read more.
Background: The transition from the parenteral to subcutaneous application of systemic oncological therapy represents one of the most important innovations in modern oncology, as it affects the quality of life of patients as well as the organization of work and the management of health services. The introduction of this change requires effective leadership, interdisciplinary cooperation, and the adaptation of existing processes in healthcare organizations. Methods: We conducted a systematic review of the professional and scientific literature, considering the purpose and goal of this research. We used electronic databases: Wiley Online Library, PubMed, COBBIS.SI, and Google Scholar web browser. Papers from 2017 to 2025 were considered and processed using meta-synthesis. Results: Recent studies confirm that the subcutaneous administration of immunotherapy and targeted therapy is as effective and safe as parenteral immunotherapy, while significantly reducing treatment time and improving patient experience. Discussion: The transition to subcutaneous application provides an opportunity to transform oncology care. From a management perspective, the introduction of subcutaneous application requires systematic change management, staff training, process adaptation, and interdisciplinary cooperation. The sustainable implementation of innovations depends on organization, communication, and management support.
Full article
(This article belongs to the Section Oncology Nursing)
►
Show Figures
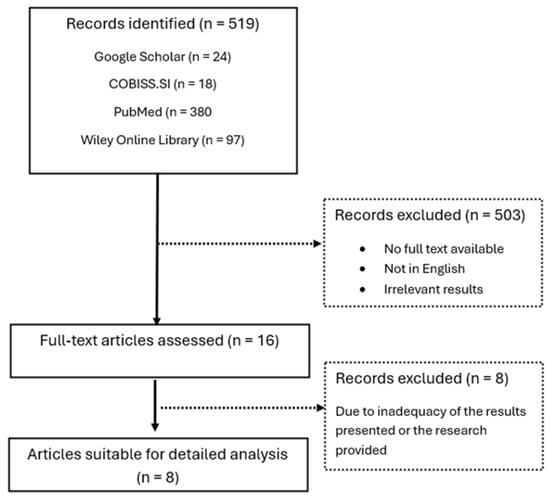
Figure 1














{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}