






Diabetology 2026, 7(6), 103; https://doi.org/10.3390/diabetology7060103 - 28 May 2026
Abstract
►
Show Figures
Background: The prevalence of GDM is increasing and is associated with maternal health and neonatal complications. Therapeutic intervention for this condition is important for the health of both mothers and their unborn children. Objective: The present meta-analysis evaluates the effects of pharmacological, nutritional,
[...] Read more.
Background: The prevalence of GDM is increasing and is associated with maternal health and neonatal complications. Therapeutic intervention for this condition is important for the health of both mothers and their unborn children. Objective: The present meta-analysis evaluates the effects of pharmacological, nutritional, and physical activity interventions on maternal and neonatal outcomes in women with GDM, including glucometabolic control, weight gain, blood pressure, lipid profiles, and pregnancy complications. Methods: Multiple databases were systematically searched for studies investigating GDM interventions and their effects on maternal and neonatal outcomes, including at least one of the following endpoints: 2 h postprandial glycemia, FBG, HbA1c, triglycerides, cholesterol, weight gain, blood pressure, cesarean delivery, preeclampsia, gestational age at delivery, neonatal hypoglycemia, neonatal complications, birth weight, preterm birth, Apgar score at 5 min, macrosomia, and NICU admission. Initial screening identified 204 records, which were narrowed to 17 studies meeting the eligibility criteria for inclusion in the meta-analysis following multi-author relevance review. Six reviewers independently extracted data and resolved discrepancies through consensus. Study quality was appraised by two reviewers using the Cochrane Risk of Bias tool, and data were analyzed using the RevMan Web software with random-effects models. Results: Pharmacological, nutritional, and physical activity interventions in women with gestational diabetes mellitus demonstrated statistically significant reductions in gestational weight gain and cesarean delivery rates. No statistically significant effects were observed for HbA1c, fasting blood glucose, 2 h postprandial glucose, lipid profiles, or blood pressure. Several outcomes, including preeclampsia, neonatal hypoglycemia, neonatal complications, and NICU admission, showed non-significant trends toward benefit, but these findings were based on limited data and should be interpreted cautiously. No meaningful effects were observed for gestational age at delivery, neonatal birth weight, preterm birth, Apgar score, or macrosomia. Substantial heterogeneity was present across metabolic outcomes, limiting the interpretability of pooled estimates. Conclusions: Nutritional and physical activity interventions significantly reduce HbA1c, gestational weight gain, and cesarean delivery in women with GDM, with protective trends for preeclampsia and neonatal complications. However, effects on lipid profiles and blood pressure remain inconsistent. Personalized, multimodal strategies integrating pharmacological, nutritional, and lifestyle modifications are necessary for optimal GDM management.
Full article
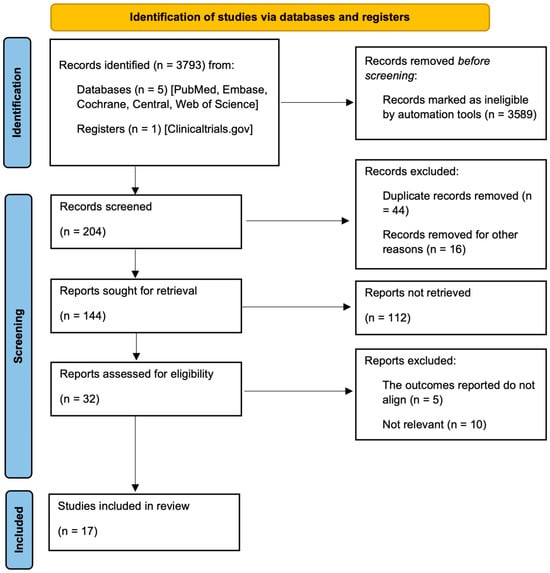
Figure 1

















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}