



J. Pers. Med. 2026, 16(4), 210; https://doi.org/10.3390/jpm16040210 - 8 Apr 2026
Abstract
Background/Objectives: Blood glucose prediction (BGP) for individuals with type 1 diabetes (T1D) is a clinically essential yet highly challenging task in time series forecasting (TSF) and an important problem in personalised medicine. Accurate bespoke BGP is crucial for individualised T1D management, reducing complications,
[...] Read more.
Background/Objectives: Blood glucose prediction (BGP) for individuals with type 1 diabetes (T1D) is a clinically essential yet highly challenging task in time series forecasting (TSF) and an important problem in personalised medicine. Accurate bespoke BGP is crucial for individualised T1D management, reducing complications, and supporting patient-specific glycaemic risk mitigation. However, the pronounced volatility of glycaemic fluctuations in T1D, combined with the need for mathematical rigor and clinical relevance, hampers reliable prediction. This complexity underscores the demand to explore and enhance more advanced techniques. While adversarial learning is adept at modelling intricate data variability, its potential for BGP remains largely untapped. Methods: This work presents a novel approach for BGP by addressing a key limitation in conventional adversarial learning when applied to this task. Typically, these methods optimise prediction accuracy within a set horizon by minimising adversarial loss. This focus overlooks how predictions align with longer-term patterns, which are critical for clinical relevance in BGP, thereby yielding suboptimal results. To overcome this limitation, we introduce collaborative augmented adversarial learning, designed to improve the model’s temporal awareness. Incorporating collaborative interaction optimisation, this approach enables the model to reflect extended time dependencies beyond the immediate horizon, thereby improving both the clinical reliability of predictions and overall predictive performance. We develop and evaluate four learning systems for BGP: independent learning, adversarial learning, collaborative learning, and adversarial collaborative learning. The proposed systems were evaluated for two clinically relevant prediction horizons, namely 30 min and 60 min ahead. Results: The interdependent collaboratively augmented learning frameworks, validated using the well-established Ohio T1D datasets, demonstrate statistically significant superior performance in both clinical and mathematical evaluations. Conclusions: Beyond advancing BGP accuracy and clinical reliability, the proposed approach supports personalised medicine by improving subject-specific glucose forecasting from CGM data, with potential relevance for more individualised diabetes monitoring and decision support. The proposed approach also opens new avenues for advancements in other complex TSF domains, as outlined in our future work.
Full article
(This article belongs to the Special Issue Integrating Mathematical Modeling and Data Analysis in Personalized Medical Research)
►
Show Figures
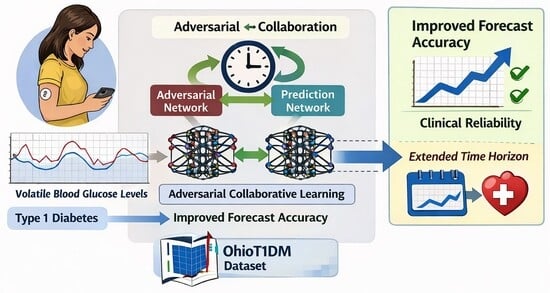
Graphical abstract
























{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}