

Gastrointest. Disord. 2026, 8(2), 25; https://doi.org/10.3390/gidisord8020025 - 18 May 2026
Abstract
Minimally invasive pancreas-preserving duodenal resection (MIPPDR) encompasses laparoscopic, robotic, and intentionally hybrid duodenal resections performed without pancreatic parenchymal excision, ranging from transduodenal local excision or ampullectomy to sleeve, segmental, subtotal, near-total, and total duodenectomy. This targeted narrative review was designed to provide a
[...] Read more.
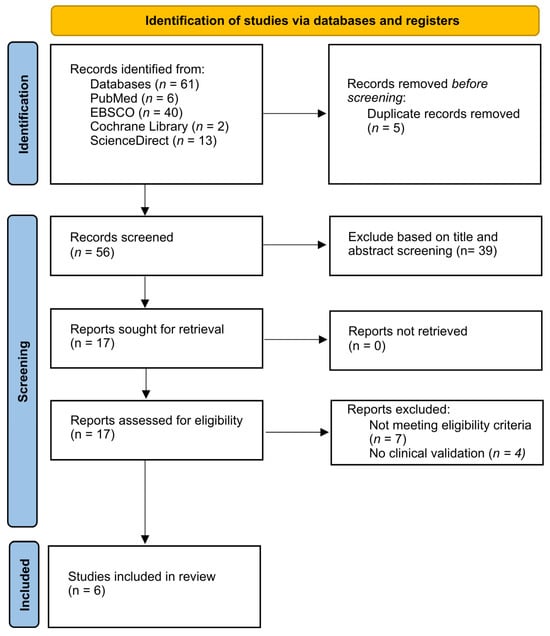
Minimally invasive pancreas-preserving duodenal resection (MIPPDR) encompasses laparoscopic, robotic, and intentionally hybrid duodenal resections performed without pancreatic parenchymal excision, ranging from transduodenal local excision or ampullectomy to sleeve, segmental, subtotal, near-total, and total duodenectomy. This targeted narrative review was designed to provide a clinically oriented synthesis of the available literature on indications, operative strategies, platform selection, reconstruction, perioperative outcomes, oncological adequacy, and functional considerations. A structured literature search was performed in PubMed/MEDLINE, Scopus, and Web of Science up to March 2026. The review focused on minimally invasive or intentionally hybrid pancreas-preserving duodenal resections reporting operative technique, perioperative outcomes, oncological outcomes, or functional sequelae. The minimally invasive literature consisted predominantly of case reports, technical notes, video articles, and small retrospective series, with substantial heterogeneity in lesion type, anatomical location, procedure extent, reconstruction, and outcome reporting. Laparoscopy appeared most reproducible for distal, infra-papillary, and limited resections with relatively low reconstructive burden, whereas robotics appeared to offer specific technical advantages for periampullary dissection, ductal identification, and intracorporeal reconstruction. However, the available evidence was insufficient to define firm comparative indications between platforms or to demonstrate superiority of one minimally invasive approach over another. Functional outcomes, despite their central relevance to the rationale of pancreas preservation, were poorly standardized and inconsistently reported. MIPPDR was therefore interpreted as a selective pancreas-preserving strategy positioned between advanced endoscopic therapy and pancreaticoduodenectomy. Future studies should adopt anatomy-based reporting, distinguish ampullary, periampullary, and distal duodenal disease, and include standardized functional endpoints.
Full article
(This article belongs to the Special Issue Minimally Invasive Surgery for Upper Gastrointestinal Tract Diseases: New Trends and Future Perspectives)
►
Show Figures
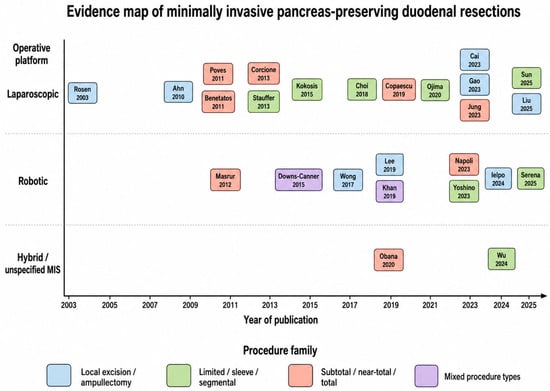
Figure 1
















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}