Abstract
This study examines the role of institutional governance in strengthening health systems in low- and middle-income countries (LMICs). The systematic review synthesizes findings from 75 studies to explore key themes such as leadership and institutional capacity, decentralisation, accountability mechanisms, financing and resource allocation, and digital governance. The study employs the institutional theory as a framework for analysis. The analysis reveals that strong leadership and institutional capacity are essential for navigating the complex institutional environments in LMICs, but path dependence and institutional inertia often hinder effective reform. Decentralisation efforts were found to be unsuccessful when local governance structures lacked the necessary resources and institutional capacity to implement reforms, leading to mimetic isomorphism, where decentralised models were adopted without adaptation to local contexts. Similarly, accountability mechanisms, including performance-based financing and regulatory frameworks, were often undermined by institutional weaknesses such as corruption and political interference. Financing and resource allocation were influenced by institutional factors, where historical patterns of centralized control limited the adoption of innovative financing models. Digital health technologies, although promising, were frequently hampered by insufficient infrastructure and political resistance to change. The study argues that successful health system strengthening in LMICs requires institutional adaptation and institutional work to overcome barriers such as political will, resource constraints, and institutional resistance. The findings contribute to the theoretical understanding of health governance in LMICs and provide practical insights for policymakers aiming to implement sustainable reforms. Future research should explore how institutional frameworks can be adapted to support resilient health systems in LMICs.
1. Introduction
Health system strengthening (HSS) in low- and middle-income countries (LMICs) remains a central concern for policy and governance, particularly as health systems confront persistent resource constraints, uneven service access, and rising burdens of communicable and non-communicable conditions. The COVID-19 era further exposed weaknesses in system coordination and continuity of essential services, reinforcing the need to strengthen primary health care (PHC) and integrated service delivery [1,2]. In this context, it has become increasingly apparent that health system performance in LMICs is not shaped solely by clinical capabilities or financing levels, but also by the quality of public administration and governance arrangements that structure policy design, implementation, oversight, and learning [3,4].
Within the available evidence, several administrative and governance strategies are consistently foregrounded as enabling conditions for improved service delivery and system functioning. At public sector management level, strengthening policy development and management systems has been linked to improved coordination and implementation capacity [3]. District-level management is also positioned as a decisive interface between national policy intent and frontline delivery, with administrative strengthening at this level often described as essential for improving responsiveness and performance [4]. Governance-oriented analyses further indicate that stewardship, accountability, institutional authority, and coordination are critical for strengthening specific sectors such as mental health systems in LMICs [5]. Where governance is undermined by corruption and weak accountability, service delivery may be compromised, particularly at the frontline where public trust and practical access to care are most directly experienced [6].
At the same time, the literature suggests that health system strengthening agendas increasingly depend on collaborative and intersectoral governance. Evidence from public administration research highlights the relevance of collaborative governance arrangements (bringing together state and non-state actors) to improve coordination, legitimacy, and shared accountability in public health in LMICs [7]. Systematic review evidence on partnerships indicates ongoing interest in how collaborations can be structured to support health system goals, while also implying the need for stronger administrative arrangements to manage partnerships effectively and sustainably [8]. The strategic importance of PHC also remains prominent, with evidence identifying multiple measures aimed at strengthening PHC systems and guiding health system responses in LMIC settings [2,9].
Innovation and learning-oriented governance have further dominated the health system strengthening discourse. Reviews on health information systems emphasize that improving the quality and use of routine health data requires more than technical fixes, pointing to the significance of institutional and administrative conditions that enable the uptake and use of data for decision-making [10]. Relatedly, scoping review evidence suggests that knowledge for health policy in LMICs remains unevenly institutionalised, raising questions about the administrative systems that support evidence use and policy learning [11]. The ‘learning health systems’ agenda similarly foregrounds continuous learning and adaptation as empowering priorities for LMICs [12]. In parallel, systematic scoping evidence indicates that digital innovations, including artificial intelligence, are increasingly examined for their potential contribution to strengthening health systems, while also implying the importance of supportive governance and system readiness for responsible adoption [13]. Digital health interventions for non-communicable disease management in PHC contexts further extend this evidence thus drawing attention to implementation conditions within LMIC health systems [14].
1.1. Contextualising the Study
Despite this expanding scholarship, important limitations remain in how the evidence is organised and synthesised. Existing reviews often concentrate on discrete components of health systems, such as corruption and frontline governance [6], PHC responses during COVID-19 [1,2], routine health information systems [10], digital health and artificial intelligence [13,14], performance-based financing [15], partnership modalities [8], co-design approaches [16], or intervention scale-up determinants [17]. While these contributions are valuable, they collectively suggest a fragmented evidence terrain in which public administration is frequently treated implicitly as a background condition rather than systematically examined as an integrated set of governance, management, accountability, coordination, and learning practices shaping health system strengthening outcomes across LMICs. Additionally, some areas of health system strengthening, such as resilience, are often explored conceptually or qualitatively [18], yet remain insufficiently connected to administrative mechanisms and governance strategies in a consolidated evidence synthesis.
Existing reviews have predominantly adopted specific analytical scopes. Governance-focused reviews, such as those by [5] sought to identify the key governance challenges, needs and potential strategies that may ensure the adequate integration of mental health into primary health care settings within six select LMICs. This study identified poor governance as an obstacle to the sustainable integration of mental health care in LMICs. The study focused on a specific scope by zooming into mental health in PHC and narrowed its scope to select six case studies. Therefore, the results are not generalisable to all LMICs, a broadened scope beyond six countries is desired. Furthermore, the review lacked the incorporation of the voices of civil society. Similarly, ref. [19] conducted a specific review to synthesize the available evidence and highlight the successes and challenges of health systems governance (HSG) towards UHC and global health security. Their study identified that context-specific health policy and health financing modalities were useful in accelerating the progress towards UHC and health security. The review showed that the ineffectiveness of adopting a one-size-fits-all HSG approach was a major challenge to achieving UHC amongst a plethora of other challenges including insufficient healthcare funding, lack of adequate health workforce and corruption. On the other hand, a review by [20] provides an extensive map of the studies that assess the impacts of a range of governance interventions on quality of care in LMICs. However, their review did not analyse the contextual, social and relational factors influencing the governance environment and its impacts on quality. Their review was further limited in that while it identified governance interventions, these did not constitute an exhaustive list of potential interventions to improve quality. This particular study will extend this scope by focusing on health system strengthening. It is evident that these reviews provide valuable insights into governance structures and their relationship to outcomes like quality and universal health coverage. However, these studies tend to isolate governance within specific domains (for instance mental health or UHC), thereby limiting their ability to capture the interconnected nature of administrative systems across leadership, financing, accountability, and service delivery.
There is also evidence of parallel stream of reviews which focused on PHC systems and service delivery. These include a critical study by [21] which reviewed evidence from 2010–2017 relating to PHC performance in LMICs. Their study acknowledged that there is need for strengthening PHC in LMICs, but research is lacking and fragmented. Similarly, ref. [22] in their review noted that strengthening systems of PHC is critical to improving health outcomes and overall health systems efficiency particularly in contexts where resources are limited. The authors also highlighted that there is still scarce knowledge on how to improve the organisation of PHC systems. However, their study focused only on LMICs in the Asia Pacific. Of particular interest, this review highlighted that the available literature remains skewed towards evidence from larger countries such as India and China and complex health systems analyses remain relatively scarce, noting that there are few systematic reviews or cross-country comparisons to draw out best practices. It is against this background that the need for this review arises. Recently, ref. [2] sought to synthesize what was already known about strengthening PHC in LMICs. These reviews are primarily concerned with identifying “what works” in PHC implementation and performance. However, the orientation towards focusing on interventions, delivery models, and system performance, requires to be complimented by reviews that interrogate the institutional logics and administrative structures that shape these outcomes. This is a gap that this review seeks to fill.
This review makes a distinct and original contribution by advancing a theory-driven, integrative synthesis of health system strengthening through the lens of the institutional theory. Specifically, it departs from prior reviews in two important ways. First, it reframes health system strengthening as an institutional phenomenon, rather than merely a technical or sectoral challenge. By applying the constructs of isomorphism, path dependence, and institutional work, the review systematically explains how LMIC health systems are shaped not only by policy choices but also by historical trajectories, external pressures, and the strategic actions of actors within bureaucratic systems. This moves beyond descriptive accounts of “what works” to provide a causal and explanatory framework for understanding reform outcomes. Secondly, the review offers a cross-cutting synthesis across multiple governance domains, including leadership, decentralisation, accountability, financing, and digital transformation. The novelty of this review lies not in identifying entirely new empirical findings, but in reorganising and reinterpreting existing evidence through a rigorous institutional lens. By doing so, it offers a more coherent and explanatory understanding of health system strengthening in LMICs. This positions the study as a critical bridge between health policy research and public administration theory and contributes to advancing a more theoretically informed and analytically integrated research agenda in global health governance.
This review contributes beyond existing syntheses by reframing health system strengthening in LMICs not merely as a technical, financing, service delivery, or policy implementation problem, but as an institutional governance problem. Existing reviews have generated important evidence on discrete areas such as primary health care strengthening, governance for quality, decentralisation, pay-for-performance, digital health, resource allocation, and learning health systems. However, these reviews tend to examine specific instruments or sub-systems in isolation. The added value of this review lies in integrating these separate strands into a single explanatory framework that shows how health system reforms are shaped by the institutional conditions in which they are introduced, adapted, resisted, or sustained.
The application of the institutional theory provides distinct explanatory leverage because it helps explain why similar reforms produce uneven outcomes across LMIC contexts. Rather than simply describing governance weaknesses, the review uses three institutional constructs to interpret reform dynamics. Isomorphism explains why LMIC health systems often adopt similar reform models, such as decentralisation, performance-based financing, accountability frameworks, digital health systems, or PHC strengthening strategies, under donor, professional, or global policy pressures. Path dependence explains why these reforms frequently fail to transform practice, because they are introduced into systems shaped by historical centralisation, weak local capacity, bureaucratic inertia, fragmented service delivery, and entrenched accountability problems. Institutional work explains how public administrators, health leaders, policy actors, and partnerships attempt to create, maintain, or disrupt institutional arrangements in order to make reforms operational.
Therefore, the review’s contribution is not simply that it identifies fragmentation in the literature. Its conceptual contribution is that it converts fragmentation into an integrated analytical model. It demonstrates that leadership, decentralisation, accountability, financing, and digital governance are not separate reform areas, but interconnected institutional processes. For example, decentralisation cannot be understood only as a structural reform; it must be analysed as a reform shaped by inherited centralised authority, external policy transfer, and the capacity of local actors to perform institutional work. Similarly, digital health is not only a technological intervention; it is an institutional process shaped by global digital-health norms, pre-existing infrastructure inequalities, and the ability of public agencies to adapt technology to local governance realities.
In this sense, the institutional theory is not used as a descriptive label but as an explanatory framework. It allows the review to move from asking “what governance strategies are used?” to asking “why do governance strategies succeed, fail, or become symbolic in LMIC health systems?” This provides a stronger conceptual contribution than prior reviews because it explains the mechanisms through which reform models travel, become embedded, encounter resistance, or require adaptation. The review consequently contributes to both health systems scholarship and public administration theory by showing that sustainable health system strengthening in LMICs depends not only on adopting evidence-based reforms, but on aligning reforms with institutional histories, administrative capacities, and actor-led processes of institutional change.
1.2. Aim of the Study
In alignment with PRISMA reporting standards, this systematic review aims to identify, appraise, and synthesise peer-reviewed evidence on the role of public administration in strengthening health systems in LMICs, with a specific focus on administrative and governance strategies that influence healthcare delivery and health governance. The review synthesises evidence on key domains reflected in the existing literature, including policy development and management capacity [3,4], governance and accountability mechanisms [5,6], collaborative and partnership-based approaches [7,8], PHC strengthening and service integration [1,2,9], and learning, evidence use, and digital innovations [10,11,12,13,14]. The review seeks to produce an integrated understanding of how administrative and governance capacities can be strengthened to support equitable, resilient, and effective health systems in LMIC contexts. The significance of this paper lies in its comprehensive examination of how digital innovations, learning health systems, and collaborative governance can collectively strengthen health systems in LMICs. The study uniquely emphasizes the need for local governance capacity-building, sustainable partnerships, and data-driven decision-making as critical enablers of effective health reforms in LMICs, providing a roadmap for future health system strengthening initiatives.
2. Theoretical Framework: Institutional Theory
The Institutional theory as developed by [23], emphasizes the role of institutional forces in shaping organizational behaviour. According to the theory, organizations do not operate in a vacuum; they are influenced by external institutional pressures that dictate what is considered legitimate behaviour. These external pressures can take the form of coercive forces (such as legal requirements), normative forces (stemming from professional standards), and mimetic forces (resulting from uncertainty and the desire to imitate successful models). In the context of health systems, these pressures can come from national governments, international organizations, and local cultural practices that shape how health policies are designed and implemented.
The Institutional theory also stresses the importance of path dependence, a concept that explains how past decisions and institutional arrangements can limit or shape future actions. This is particularly relevant in LMICs, where the legacies of colonialism, political instability, and economic inequalities often dictate the structure and functioning of public institutions, including health systems. As ref. [24] notes, institutions often have historical inertia, meaning that once certain governance structures or policies are established, they become difficult to change due to entrenched institutional norms and practices.
The Institutional theory has been widely debated and critiqued, particularly in relation to its application in public administration and health system governance. One of the primary areas of debate is the theory’s tendency to emphasize stability and conformity, often at the expense of considering how organizations innovate or adapt in response to changing external pressures. Scholars such as ref. [25] have argued that the institutional theory’s focus on isomorphism: the process through which organizations within a field become similar due to institutional pressures, can sometimes obscure the dynamism and change that occurs within organizations. In the context of health systems, particularly in LMICs, this critique is important because it highlights the need to consider how innovation and reform can occur, even within systems that appear to be highly institutionalized and resistant to change.
Another significant debate in the application of the institutional theory to public administration is its focus on the macro-level and the neglect of individual agency. While the institutional theory offers valuable insights into how institutional pressures shape organizational behaviour, it has been criticized for downplaying the role of individual actors within organizations who may challenge, resist, or reinterpret institutional norms. Ref. [26] suggests that the institutional theory, when applied to public administration, should be more attentive to the role of institutional work, the efforts of individuals and groups to create, maintain, or disrupt institutional arrangements. This is particularly relevant in the context of health system governance in LMICs, where individual leaders, bureaucrats, and civil society actors can play a crucial role in shaping policy outcomes.
The Institutional theory is particularly well-suited for analysing the complex, institutional dynamics that shape health system strengthening in LMICs. The theory provides a framework for understanding how formal health policies and governance reforms are influenced by a combination of political, cultural, and institutional forces. As ref. [27] argue, public administration systems are deeply embedded in their institutional environments, which shape the capacity of governments to implement health system reforms. In LMICs, this includes institutional factors such as bureaucratic structures, political legacies, and cultural norms, which often impede or facilitate the implementation of health policies.
In this study, the institutional theory helps explain the challenges and opportunities faced by public administrators in LMIC health systems, particularly as they attempt to balance global health initiatives with local political realities. For example, reforms such as decentralisation, performance-based financing, or digital health governance are often shaped by institutional legacies of centralized control or informal governance structures that prioritize political loyalty over service delivery. By applying the institutional theory, we can gain insights into the institutional barriers to effective governance and health system strengthening in LMICs, as well as the opportunities for reform that arise when actors challenge or reshape existing institutional arrangements.
The Institutional theory, therefore, offers a rich framework for analysing the institutional dynamics that shape health system strengthening in LMICs. It allows for an exploration of the governance challenges and opportunities inherent in these complex systems, while providing insights into how institutional forces (both formal and informal) impact policy implementation and reform. By examining the institutional context of health governance, this theory helps to illuminate the pathways through which institutional work can either promote or hinder the effective delivery of health services in LMICs. Despite its limitations, particularly regarding the neglect of individual agency and change, the Institutional theory remains a valuable tool for understanding the complex governance landscape of health systems in low- and middle-income countries.
3. Methodology
3.1. Eligibility Criteria
This systematic review applied predefined eligibility criteria to identify studies examining the role of public administration, governance, and management practices in strengthening health systems in LMICs. Eligible studies focused on health systems, primary health care, or public health systems in LMIC contexts and addressed administrative, governance, leadership, policy, accountability, coordination, financing, learning, or regulatory dimensions of health system strengthening. A wide range of study designs was considered, including qualitative, quantitative, and mixed-methods empirical studies, systematic reviews, scoping reviews, evidence gap maps, narrative reviews, policy analyses, conceptual papers, and doctoral dissertations. Protocol papers were retained where they contributed to methodological transparency in the field. To enhance clarity, rigour and reproducibility, the review adopted a clearly defined inclusion and exclusion criteria.
This review adopted a broad inclusion strategy because the phenomenon under investigation (public administration and institutional governance in LMIC health system strengthening) is methodologically and conceptually diverse. Relevant evidence is distributed across empirical studies, systematic and scoping reviews, policy analyses, conceptual papers, evidence gap maps, and doctoral dissertations. This breadth was necessary because the review did not seek to estimate the effect of a single intervention, but to explain how governance and administrative mechanisms shape health system strengthening across heterogeneous institutional contexts.
To avoid an unrestricted evidence base, inclusion was limited to studies that explicitly addressed LMIC health systems and engaged with at least one governance or public administration dimension, including leadership, management, decentralisation, accountability, financing, policy implementation, learning systems, or digital governance. Studies that focused only on clinical interventions without system-level governance relevance were excluded.
Heterogeneity was managed through a theory-driven synthesis strategy. Included studies were first categorised by study type and then coded deductively against the core constructs of the Institutional Theory: isomorphism, path dependence, and institutional work. They were subsequently grouped inductively into five thematic domains: leadership and institutional capacity, decentralisation and management, accountability mechanisms, financing and resource allocation, and digital governance. This process enabled different forms of evidence to be integrated within a common analytical framework while preserving methodological distinctions between empirical, review-based, conceptual, and policy-oriented studies.
The study used studies published between 2000 and 2025 covering a reasonable span of literature on LMICs. These studies were restricted to publications in English language to ensure consistency and accessibility of analysis across regional and international scholarly and professional audiences. Studies were excluded if they focused solely on clinical effectiveness without system-level or governance relevance, were conducted exclusively in high-income country settings, or did not engage with administrative or policy processes. Studies were also excluded if they were published outside the timeframe (2000–2025) and if they were published in a language other than English. For synthesis, studies were grouped thematically according to dominant governance and administrative domains.
3.2. Information Sources
The identification of studies was based primarily on structured searches of Scopus, Web of Science (WoS) and Google Scholar, supplemented by manual screening of reference lists from key health policy, governance, and health systems reviews. Citation tracking was undertaken to identify additional relevant studies referenced in included articles. The final search and consultation of information sources was completed in January 2026. Given the public health focus of the review, the included articles were published in numerous distinct and reputable public health journals such as BMC Public Health, BMC Health Services Research, Health Policy and Planning; and Health Research Policy and Systems.
3.3. Search Strategy
The search strategy was developed to systematically identify literature examining the role of public administration, governance, and management in strengthening health systems in LMICs. In accordance with PRISMA 2020 guidelines, the strategy was constructed to ensure transparency, replicability, and conceptual coverage across interdisciplinary domains [28].
The primary databases used for this review were Scopus, Web of Science and Google Scholar selected for their extensive coverage of peer-reviewed literature in public administration, health policy, and global health systems research. The final search was conducted on 18 January 2026, and all retrieved records reflect the database status at that time.
The search strategy combined key conceptual domains using Boolean operators (AND, OR) and truncation to capture variations in terminology. The search was executed using the TITLE-ABS-KEY fields in Scopus and Topic (TS) in WoS to ensure relevance to the study focus. For Google Scholar, due to platform limitations in advanced Boolean structuring, a simplified keyword-based approach was used. The full search string applied was as follows:
TITLE-ABS-KEY
(“health system strengthening” OR “health systems strengthening” OR “health system” OR “health systems” OR “primary health care” OR “primary healthcare”)
- AND
- (“public administration” OR governance OR management OR leadership OR accountability OR decentralisation OR decentralization OR financing OR “resource allocation” OR “learning system” OR “digital governance” OR policy)
- AND
- (“low- and middle-income countr” OR LMIC* OR “developing countr*” OR “low income countr*” OR “middle income countr*”)
The Boolean operator OR was used within each conceptual block to capture synonyms and related constructs, while AND was used to combine the three primary domains: (1) health systems, (2) governance and administration, and (3) LMIC context. Truncation (e.g., countr* and system*) was applied to capture plural and variant forms. Phrase searching using quotation marks ensured conceptual precision for key terms such as “health system strengthening” and “public administration.”
The following filters and limits were applied: (i) Document type: articles, reviews, and conference papers; (ii) Source type: peer-reviewed journals; (iii) language: English; (iv) Access: full-text availability (where accessible through institutional access).
To enhance the comprehensiveness of the search, manual screening of reference lists of included studies and key systematic reviews was conducted. In addition, forward citation tracking was used to identify relevant studies citing core articles in the field. These supplementary strategies were undertaken during the same review period and integrated into the final pool of eligible studies. This structured and reproducible search strategy ensured comprehensive coverage of literature at the intersection of public administration, institutional governance, and health system strengthening in LMICs, consistent with best practice recommendations for systematic reviews [28].
3.4. Selection Process
Study selection followed a two-stage process involving title and abstract screening, followed by full-text eligibility assessment. The study selection process followed the PRISMA 2020 reporting guidelines. After screening titles, abstracts and full texts according to the predefined eligibility criteria, 75 studies met the inclusion criteria and were retained for qualitative synthesis. These studies span the period 2003–2025 and collectively examine health systems strengthening (HSS), primary health care (PHC), governance, financing, management, digital health, and implementation strategies in low- and middle-income countries (LMICs). Figure 1 below captures the publication trends for the included studies in this review.
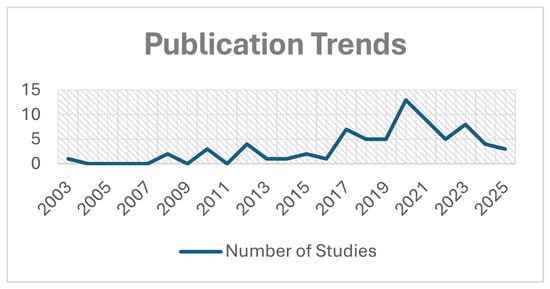
Figure 1.
Publication Trends.
The included literature comprised systematic reviews, scoping reviews, narrative reviews, global modelling analyses, empirical quantitative and qualitative studies, conceptual/theoretical papers, doctoral theses, and policy-oriented syntheses. No study was excluded at the final stage due to insufficient reporting of core outcomes relevant to health systems strengthening; however, several protocols and evidence gap maps were included primarily to characterise the evidence landscape rather than to contribute effect estimates [29,30].
3.5. Data Collection Process
Data were extracted from included studies using a structured extraction framework designed to capture study characteristics and governance-relevant content. Data collection was performed through careful reading of full texts. Extracted information was organised into structured tables and ensuring internal consistency across extracted fields. No direct contact with study authors was undertaken. (See Figure 2).
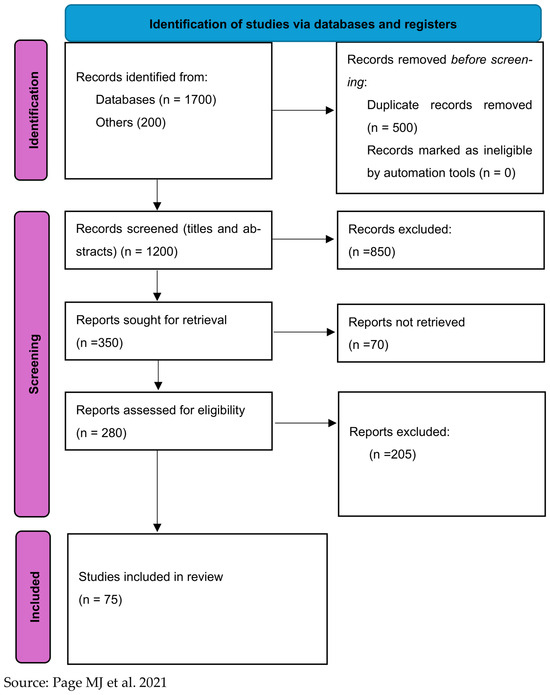
Figure 2.
PRISMA 2020 Flow Diagram: Screening and Selection of Studies on Institutional Dynamics of Health System Strengthening in Low- and Middle-Income Countries [28].
3.6. Data Extraction
Data extraction was conducted systematically to ensure consistency, transparency, and reproducibility of the review process. A standardised data extraction form was developed and refined through pilot testing on a subset of included studies to minimise ambiguity and ensure alignment with the review objectives. This approach follows best practice in systematic reviews, where structured extraction enhances comparability across heterogeneous sources.
The extraction template captured three core categories of information. First, bibliographic and study characteristics were recorded, including author(s), year of publication, study title, and type of study (e.g., journal article, systematic review, scoping review, or doctoral dissertation). Second, methodological characteristics were extracted, encompassing research design, data collection methods, analytical approaches, and the geographical or contextual setting of each study. Third, and most critically, substantive findings were extracted in direct alignment with the review’s analytical focus on public administration and health system strengthening.
Data extraction in this review was guided by a theory-informed approach, explicitly anchored in the institutional theory to ensure analytical coherence between the review objectives, coding process, and synthesis. A standardised data extraction framework was developed and iteratively refined to capture both descriptive study characteristics and deeper institutional dynamics shaping health system governance in LMICs.
The institutional theory informed the data extraction process in three critical ways. Firstly, the extraction framework was structured to identify how institutional pressures and structures shape governance outcomes. Particular attention was paid to manifestations of isomorphism, understood as the tendency of health systems to adopt similar governance models due to coercive (like donor influence), normative (like professional standards), and mimetic (like policy imitation) pressures [31]. During extraction, studies were examined for evidence of such pressures, including the adoption of global health policies, standardised accountability mechanisms, and externally driven reform models.
Secondly, the concept of path dependence guided the extraction of historical and structural factors influencing governance. Data were systematically captured on how past institutional arrangements (such as colonial administrative legacies, centralised governance systems, and entrenched bureaucratic norms) shape current policy implementation and reform trajectories [26]. This enabled the review to move beyond surface-level findings and identify how institutional continuity constrains or enables change in LMIC health systems.
Thirdly, the extraction process incorporated the concept of institutional work, focusing on the actions of actors (such as policymakers, administrators, and international stakeholders) in creating, maintaining, or transforming institutional arrangements [27]. Data were extracted on leadership practices, reform initiatives, and governance interventions that demonstrated efforts to either reinforce or disrupt existing institutional structures.
A theory-driven coding framework was employed to organise and analyse the extracted data. Initial coding categories were deductively derived from key institutional constructs (isomorphism, path dependence, and institutional work) and subsequently expanded through inductive refinement to capture emerging governance themes. This hybrid coding approach ensured both theoretical alignment and empirical sensitivity. Codes were grouped into broader thematic domains, including leadership and institutional capacity, decentralisation, accountability mechanisms, financing, and digital governance, with each theme explicitly mapped back to one or more institutional constructs.
To facilitate synthesis, all extracted data were organised into an evidence matrix, enabling systematic comparison across studies, contexts, and methodological approaches. Each study was coded not only for its substantive findings but also for its institutional characteristics, allowing the analysis to identify patterns of convergence and divergence across LMIC settings. This further allowed the synthesis to explain not only what governance issues were reported but how and why these issues persisted or changed across LMIC health systems. Where multiple findings were reported within a single study, each was coded separately to preserve analytical depth.
Where information was incomplete or unclear, only explicitly reported data were extracted, and no assumptions were made. This ensured methodological rigor and preserved the integrity of the synthesis process. Overall, the data extraction strategy enabled a comprehensive, theory-informed analysis of governance mechanisms in LMIC health systems, while maintaining alignment with established systematic review standards.
This approach enabled the institutional theory to function as an explanatory framework rather than a descriptive overlay. It allowed the review to interpret how reforms such as decentralisation, performance-based financing, accountability systems, and digital health adoption often circulate across LMICs through isomorphic pressures yet produce uneven outcomes because they encounter path-dependent institutional constraints. At the same time, the concept of institutional work helped identify the conditions under which public administrators, policymakers, health managers, and development partners adapted, negotiated, or transformed inherited governance arrangements. Thus, the analytical process created a transparent link between the included evidence, the coding framework, and the final thematic synthesis.
3.7. Risk of Bias Assessment
A formal risk-of-bias assessment using standard clinical appraisal tools was not undertaken due to the heterogeneity of the included evidence base, which comprised conceptual analyses, policy reviews, qualitative studies, scoping reviews, and evidence gap maps. This approach is consistent with established practice in governance- and policy-focused systematic reviews, where the aim is to synthesise institutional and administrative mechanisms rather than estimate intervention effects [28].
3.8. Effect Measures
No statistical effect measures were specified or calculated, as the review did not involve quantitative meta-analysis. The synthesis focused on conceptual, institutional, and governance-related contributions rather than effect size estimation.
3.9. Synthesis Methods
A narrative thematic synthesis approach was employed. Studies were first mapped against predefined governance and administrative domains, after which thematic patterns were identified and compared across contexts and study types. Data preparation involved tabulation of study characteristics and thematic contributions. Meta-analysis, subgroup analysis, meta-regression, and sensitivity analysis were not undertaken due to heterogeneity in study designs, analytical aims, and outcome domains.
3.10. Reporting Bias and Certainty Assessment
Formal assessment of reporting bias and certainty of evidence was not conducted, as the review did not synthesise quantitative outcomes. Instead, confidence in the body of evidence was addressed narratively by considering the consistency of themes, breadth of geographic representation, and diversity of methodological approaches across included studies.
4. Results
4.1. Study Characteristics
The 75 included studies were diverse in terms of study design, geographic focus, and methodological approach. The studies were primarily systematic reviews (n = 14), scoping reviews (n = 10), and empirical studies (n = 32), with the remaining studies (n = 19) being policy analyses, conceptual papers, and doctoral dissertations. These studies represented a wide array of LMICs across Africa, Asia, Latin America, and Eastern Europe, providing a broad perspective on the challenges and opportunities in health system governance. Most studies (n = 40) focused on health system governance and policy reforms at the national level, while others (n = 25) examined subnational governance and decentralisation efforts. The remaining studies (n = 10) addressed accountability mechanisms and performance monitoring in health service delivery, especially in the context of resource-limited settings.
Consistent with PRISMA 2020 reporting expectations for study characteristics, the 75 included studies were classified into five dominant thematic clusters based on each study’s primary analytical emphasis (noting that some studies are cross-cutting but were assigned once to avoid double counting). The evidence base remains dominated by evidence syntheses (systematic/scoping/narrative reviews and evidence gap maps), complemented by modelling studies, qualitative empirical work, policy/health policy analysis, and doctoral theses.
The included studies were grouped into five thematic clusters:
- conceptual and systems frameworks (n = 13) [12,18,32,33,34,35,36,37,38,39,40,41,42].
- governance and leadership (n = 23) [3,4,5,6,7,8,11,19,20,29,37,43,44,45,46,47,48,49,50,51,52,53,54].
- financing and resource allocation (n = 8) [15,55,56,57,58,59,60,61]
- primary health care performance and implementation (n = 20) [1,2,9,16,17,21,22,30,62,63,64,65,66,67,68,69,70,71,72,73].
- digital health and innovation (n = 11) [10,13,14,74,75,76,77,78,79,80,81].
These clusters were not treated as descriptive categories only; rather, they were used to identify how different reform domains reveal distinct institutional mechanisms. Conceptual and systems studies clarified the theoretical and policy architecture of health system strengthening, while governance and leadership studies demonstrated how institutional capacity, accountability, and authority structures shape reform implementation. Financing studies showed how allocation systems translate policy priorities into material capacity, whereas PHC and digital health studies revealed how reforms become operational only when embedded in local administrative routines.
4.2. Study Design and Methods Across Included Studies (n = 75)
In accordance with PRISMA guidance on describing study characteristics and methodological features of included evidence, this section presents a structured overview of the study design distribution across the 75 included studies. Classification is based strictly on design information explicitly identifiable from the study titles, journal type (e.g., Cochrane Database of Systematic Reviews), and clearly stated methodological descriptors (e.g., “systematic review,” “scoping review,” “qualitative study,” “modelling,” “evidence gap map,” “doctoral dissertation”). Where titles did not explicitly state the design, categorisation was conservatively based on journal conventions.
The included evidence base was methodologically heterogeneous, comprising systematic reviews (n = 14), scoping reviews (n = 10), narrative/conceptual reviews (n = 18), qualitative empirical studies (n = 8), quantitative modelling/global data analyses (n = 3), mixed-methods studies (n = 12), and doctoral dissertations (n = 2). This heterogeneity was expected because public administration and health system governance are examined across multiple methodological traditions. Rather than treating all evidence as equivalent, the synthesis used study designs for different analytical purposes: reviews identified cross-contextual patterns, empirical studies provided contextual depth, modelling studies clarified financing and resource implications, and conceptual or policy papers supported theory-building. This design diversity therefore strengthened, rather than weakened, the institutional synthesis by allowing reform mechanisms to be examined across different forms of evidence. Figure 3 shows the distribution of the publication types used.
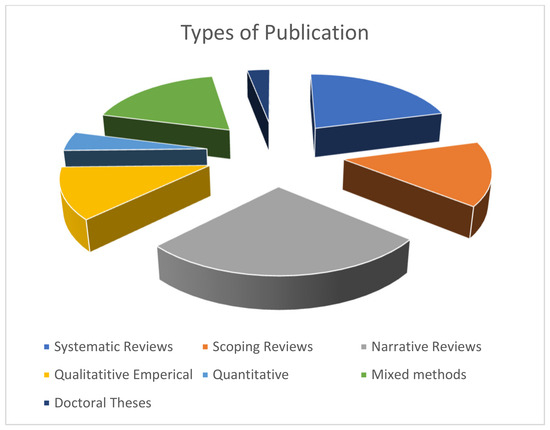
Figure 3.
Types of publication.
4.3. Geographical Distribution of Included Studies (n = 75)
In line with PRISMA 2020 guidance on reporting study characteristics, this section summarises the geographical focus of the 75 included studies based strictly on information explicitly identifiable from titles (e.g., “Sub-Saharan Africa,” “South and Southeast Asia,” “ASEAN,” “Asia–Pacific,” “LMICs,” “Malawi,” “South Africa,” “Punjab, Pakistan”). Where no specific country or region is mentioned in the title, the study is classified as multi-country LMIC/global focus.
Geographically, the evidence base was dominated by multi-country LMIC or global studies (n = 45; 60%), followed by Sub-Saharan Africa (n = 12; 16%), South and Southeast Asia (n = 9; 12%), Asia-Pacific studies (n = 3; 4%), and single-country studies (n = 6; 8%). This distribution indicates that the field is strongly oriented toward cross-national synthesis and global policy comparison, but less developed in deep country-level institutional analysis. Analytically, this matters because multi-country reviews are useful for identifying broad patterns of reform diffusion, while single-country and regional studies are better positioned to explain how path dependence, local political authority, bureaucratic capacity, and institutional work shape reform outcomes in specific settings. The limited number of country-specific studies therefore reinforces the need for future longitudinal and comparative institutional research across underrepresented LMIC regions. Figure 4 shows the geographical distribution of the included studies.
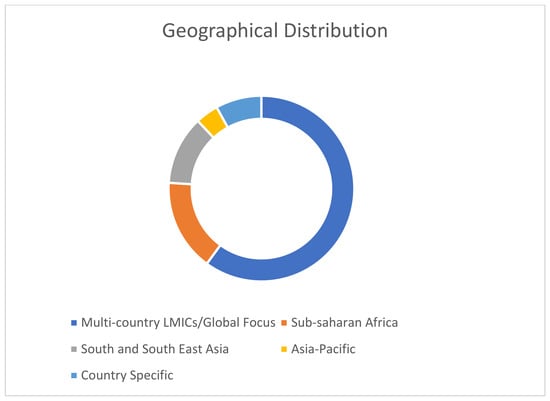
Figure 4.
Geographical Distribution of studies.
Overall, the descriptive distribution of studies was used as an analytical entry point rather than an end in itself. The dominance of multi-country reviews explains why the evidence base is strong in identifying recurring reform patterns, but weaker in explaining country-specific institutional trajectories. Conversely, the smaller body of country-specific and regional studies provides deeper insight into how reforms are mediated by path-dependent governance arrangements, local capacity, and actor-led institutional work. This justified the use of the Institutional Theory as a synthesising framework because it enabled the review to move beyond classifying studies by type or location and toward explaining how reform mechanisms operate across different LMIC contexts.
4.4. Synthesis Overview
The synthesis of the included studies followed a thematic analysis approach, grouping the findings under major governance domains relevant to the research questions: leadership and institutional capacity, decentralisation and management, accountability mechanisms, financing and resource allocation, and digital governance. This approach allowed for the identification of key patterns and themes across the studies, providing a comprehensive understanding of how public administration and governance structures shape health system strengthening in LMICs.
The synthesis highlighted several recurring themes:
- Leadership and institutional capacity were frequently cited as critical factors influencing the effectiveness of health system reforms, with the need for strong leadership and institutional support to drive policy change.
- Decentralisation was often presented as a key strategy for improving health system performance, although challenges related to local capacity, political resistance, and resource allocation were common.
- Accountability mechanisms, including performance-based financing and regulatory frameworks, were identified as important tools for improving service delivery, though political and institutional barriers often limited their effectiveness.
- Financing was a recurring challenge in LMIC health systems, with studies emphasizing the need for innovative financing mechanisms to ensure equitable access to services.
- The role of digital governance and technology adoption emerged as a growing focus, particularly in the context of e-health and digital health interventions, although challenges related to digital infrastructure and inequities in access were highlighted.
The review found that while governance reforms such as decentralisation, accountability mechanisms, and digital health interventions have the potential to improve health system performance in LMICs, their success is often contingent upon the institutional context in which they are implemented. In particular, political will, institutional capacity, and resource availability were frequently identified as key determinants of successful reform implementation. Additionally, the findings underscored the resilience of existing institutional structures in LMICs, where historical legacies and cultural norms continue to shape the effectiveness of governance reforms.
4.5. Certainty of Evidence Across Thematic Clusters
Consistent with PRISMA 2020 guidance on reporting certainty or confidence in the body of evidence, a GRADE-informed narrative assessment was undertaken across the five thematic clusters. Given the heterogeneity of study designs (systematic reviews, scoping reviews, modelling studies, qualitative research, and narrative analyses), certainty ratings are expressed qualitatively (High, Moderate, Low, Very Low) and justified using standard GRADE domains: risk of bias, inconsistency, indirectness, imprecision, and publication bias. No numerical downgrading was applied; rather, domains were interpreted at cluster level.
The majority of studies in the cluster on conceptual and systems frameworks are narrative reviews, conceptual analyses, and qualitative evidence syntheses. While these studies demonstrate theoretical coherence and conceptual convergence (e.g., systems thinking, resilience, learning health systems), they generally lack formal systematic search transparency and quantitative effect estimation. Therefore, the overall certainty is low. The risk of bias was moderate to high (interpretive and selection bias), and the inconsistency is low as evidenced by the strong conceptual alignment across studies. Confidence is limited regarding the magnitude of impact of systems-based approaches, although conceptual consensus is strong.
On the cluster, governance and leadership the overall certainty was low to moderate. This cluster contains a mix of systematic reviews, scoping reviews, qualitative studies, and policy analyses. Systematic reviews provide structured synthesis; however, governance constructs vary substantially across contexts. The risk of bias is moderate (variation in methodological rigor; qualitative sampling bias), while the inconsistency is moderate due to heterogeneous definitions of governance and leadership. Evidence suggests governance is critical to health system performance, particularly in Sub-Saharan Africa, but confidence in causal attribution to specific governance mechanisms remains moderate at best.
For financing and resource allocation, the overall certainty was moderate. This cluster includes Cochrane systematic reviews and macroeconomic modelling studies. Structured review methodology strengthens internal validity, and modelling provides cross-country quantitative estimates. The risk of bias is low to moderate due to strong review methods; modelling assumption sensitivity, while inconsistencies are moderate as evidenced by variation across country datasets. There is moderate confidence that financing mechanisms and expenditure levels influence system performance; however, projections remain sensitive to contextual economic conditions.
This cluster PHC performance and implementation contains the highest proportion of systematic reviews and overviews. In this cluster the overall certainty is moderate. Structured evidence syntheses (including Cochrane reviews) strengthen methodological robustness. The risk of bias is moderate (heterogeneity in included primary studies), and inconsistency is low to moderate (direct focus on PHC delivery outcomes). There is moderate confidence that structured PHC strengthening and implementation strategies improve service delivery outcomes. However, heterogeneity of interventions limits certainty regarding effect size consistency.
This digital health and innovation cluster is dominated by scoping reviews, innovation analyses, and qualitative studies, with limited controlled comparative evaluation. The overall certainty is low. The risk of bias is moderate to high (rapidly evolving field; descriptive designs) while the inconsistency is moderate (variation in digital intervention types and settings). While digital health is frequently positioned as transformative, particularly in South and Southeast Asia, the certainty of evidence regarding sustained system-level impact remains low.
Overall, the certainty of evidence across clusters ranges from low to moderate, reflecting methodological heterogeneity and regional concentration. While systematic reviews and modelling studies strengthen aspects of the evidence base, many conclusions remain grounded in conceptual synthesis and context-specific analyses.
5. Findings
This study set out to examine the institutional dynamics that shape health system strengthening in LMICs, framed through the lens of the Institutional theory. The findings reveal key insights into how leadership and institutional capacity, decentralisation, accountability mechanisms, financing and resource allocation, and digital governance influence the success and sustainability of health reforms in these settings. The Institutional Theory, with its emphasis on coercive isomorphism, path dependence, and institutional work, provides a compelling framework for understanding these challenges and opportunities in health governance in LMICs. The findings align with and extend existing theoretical frameworks by offering a deeper understanding of how institutional structures and governance dynamics shape the outcomes of health reforms and provide new insights into the institutional constraints that impede or facilitate effective health system strengthening.
The thematic synthesis revealed that governance and administrative factors influence health system strengthening through three cross-cutting institutional mechanisms: institutional alignment, institutional constraint, and institutional agency. Institutional alignment refers to the degree to which policy objectives, administrative authority, financing arrangements, implementation capacity, and accountability structures reinforce one another. Institutional constraint captures how historical legacies, centralised bureaucratic traditions, fragmented service delivery systems, and weak regulatory capacities shape the limits of reform. Institutional agency refers to the institutional work performed by policymakers, administrators, health managers, professional groups, and development partners to adapt, negotiate, maintain, or transform governance arrangements. These mechanisms cut across all five themes and explain why similar reforms produce different outcomes across LMIC contexts.
To avoid treating these themes as discrete descriptive categories, the synthesis interprets each theme as a mechanism through which institutional conditions shape reform outcomes. In this framing, leadership, decentralization, accountability, financing, and digital governance are not separate administrative issues; rather, they represent different sites where isomorphic pressures, path-dependent constraints, and institutional work interact. This analytical framing explains why similar reforms may be formally adopted across LMICs but produce uneven outcomes depending on whether they are institutionally aligned, historically constrained, or actively embedded by reform actors.
5.1. Leadership and Institutional Capacity
One of the most significant findings from this study was the centrality of leadership and institutional capacity in determining the success of health system reforms in LMICs. The review revealed that strong leadership is essential for navigating the complex and often fragmented institutional environments in which health systems operate. As refs. [24,82] argue, leadership in LMICs must not only manage policy reforms but also engage in institutional work, which involves actively shaping and reshaping the institutional environment to facilitate reform. This finding is consistent with the arguments of [27], who highlight that institutional work by leadership is crucial to creating and maintaining the institutional conditions for reform.
However, the findings also point to the path-dependent nature of health system governance in LMICs. Many countries face significant barriers to effective leadership due to historical legacies of centralized governance, political instability, and weak bureaucratic structures. These factors, identified in studies such as [5,26], create a resistance to change, where new leaders struggle to overcome institutional inertia. For example, the legacy of colonialism and authoritarian governance in many African countries often limits the ability of health leaders to implement reforms due to entrenched bureaucratic norms and political patronage systems. The Institutional theory helps explain these challenges by framing them within the context of institutional path dependence, where historical governance structures limit the capacity of leaders to implement new policies or governance frameworks. In contrast, strong leadership that engages in institutional work can transform the institutional landscape by overcoming these barriers. This finding aligns with the work of [27], who emphasize the transformative power of leadership in overcoming institutional constraints. Effective leadership is not just about directing policy but also about building the institutional capacity to support long-term reforms, as demonstrated in South Africa’s experience with health system decentralisation [5]. By fostering institutional capacity at both the central and local levels, leaders can help navigate the complex political dynamics that shape health governance in LMICs. Here, institutional agency as a mechanism is at work. Leadership matters because it translates reform intentions into organizational routines, coordinates fragmented actors, and creates administrative legitimacy for change. Where leadership is weak, reforms remain dependent on formal policy instruments alone; where leadership performs institutional work, reforms are more likely to become embedded in everyday governance practice.
Therefore, leadership emerged not merely as a managerial attribute but as an institutional mechanism through which reform capacity is created or constrained. Across the reviewed studies, leadership influenced health system strengthening by coordinating fragmented actors, sustaining policy direction, mobilising resources, and building administrative routines. However, leadership effects were mediated by path-dependent institutional environments. Where health systems were marked by weak bureaucratic capacity or fragmented governance, leadership was required to perform institutional work before reforms could be implemented meaningfully. Thus, leadership strengthened health systems not simply by issuing policy directives, but by reshaping the institutional conditions under which policy implementation became possible.
5.2. Decentralisation and Management
Decentralisation was identified as a major strategy for improving health service delivery in LMICs. The review revealed that decentralisation reforms are often seen as a means of enhancing local responsiveness, accountability, and community engagement. However, the findings also pointed to the challenges of decentralisation in many LMICs, where local governments often lack the institutional capacity to effectively manage health services. This finding aligns with [53,54] who note that decentralisation often fails due to weak local governance, insufficient resources, and political resistance from central governments. These studies highlight that decentralisation can result in mimetic isomorphism, where local governments simply replicate centralized systems without adapting them to the local context. These barriers should therefore be read less as ordinary implementation deficits and more as institutional effects. Weak local capacity reflects the path-dependent legacy of centralized administration, while political resistance reflects the persistence of authority structures that decentralization formally seeks to unsettle. Resource shortages, in turn, indicate a failure of institutional alignment, where responsibilities are devolved without matching fiscal authority or managerial capacity.
The findings also underscore the role of institutional path dependence in shaping the outcomes of decentralisation reforms. Many LMICs have a long history of centralized governance, where decision-making power is concentrated at the national level. This centralized legacy creates significant resistance to decentralisation, as local authorities often lack the institutional capacity and political autonomy needed to effectively manage health services. As ref. [23] suggest, institutional isomorphism leads to the adoption of decentralized models due to external pressures, but these models are often poorly implemented when local conditions are not taken into account. The Institutional theory suggests that successful decentralisation requires institutional adaptation at both the national and local levels. Institutional work by local leaders, who engage in negotiation and coordination with central governments, is crucial for overcoming the institutional barriers that hinder decentralisation. Ref. [53] found that local capacity-building efforts are essential for decentralisation to succeed. This aligns with the findings of this review, which emphasize the need for context-sensitive reforms that align decentralisation efforts with local institutional realities.
Decentralisation functioned as a mechanism of health system strengthening only when formal devolution was matched by administrative capacity, fiscal authority, and local accountability. The synthesis showed that decentralisation often failed when it was adopted through isomorphic policy transfer without sufficient adaptation to local institutional realities. In such cases, authority was formally decentralised while resources and decision-making power remained centralised. This produced implementation gaps and reinforced existing administrative hierarchies. The institutional explanation is therefore that decentralisation does not strengthen health systems by structure alone; it does so only when local institutions are empowered to convert transferred authority into operational capacity.
5.3. Accountability Mechanisms
Accountability mechanisms emerged as another central theme to improving health system performance, yet the findings indicated that these mechanisms often fail due to institutional barriers. Studies such as refs. [1,61] have highlighted the critical role of performance-based financing and regulatory frameworks in improving health service delivery. However, this review found that the implementation of these mechanisms is often hindered by corruption, political interference, and weak regulatory capacity. The Institutional theory helps explain these challenges by highlighting the role of institutional isomorphism, where external pressures to adopt accountability mechanisms do not always align with the local institutional context. The analytical implication is that accountability reforms fail not simply because oversight is weak, but because formal accountability tools are often layered onto institutional environments that have not internalized transparency, sanctioning authority, or routine administrative reporting. In such cases, accountability becomes ceremonial: it satisfies external expectations while leaving underlying governance behavior largely unchanged.
The findings from this review suggest that accountability mechanisms are more likely to succeed when they are contextualized and adapted to local conditions. Institutional work at the local level, such as engaging local leaders, strengthening regulatory frameworks, and aligning accountability mechanisms with local norms, is crucial for overcoming institutional resistance and ensuring the effectiveness of these mechanisms. Studies such as ref. [27] emphasize the importance of institutional work in adapting global models to local institutional contexts. This was evident in South Africa, where the adoption of performance-based financing models required institutional adaptation to local political dynamics and governance structures [5].
Accountability mechanisms influenced health system strengthening through their capacity to convert formal rules into enforceable administrative behaviour. However, the review showed that accountability reforms were frequently weakened when they operated in institutional contexts characterised by corruption, weak regulatory enforcement, poor information systems, or political interference. From an institutional perspective, this suggests that accountability mechanisms succeed when they become embedded in routine administrative practice but remain symbolic when introduced mainly as externally promoted compliance frameworks. Their effectiveness therefore depends on whether they are supported by institutional work that strengthens oversight, transparency, and managerial responsibility.
5.4. Financing and Resource Allocation
Financing and resource allocation was also key to the analysis, with findings indicating that inequitable resource distribution and chronic underfunding remain significant barriers to health system strengthening in LMICs. The review revealed that health financing systems in LMICs are heavily influenced by political priorities, bureaucratic inefficiencies, and historical patterns of resource allocation. This is consistent with the work of [65], who argue that institutional factors, such as political ideology and bureaucratic control, often shape health financing decisions more than health needs. The Institutional theory provides a useful lens for understanding how path dependence influences financing decisions in LMICs. Many LMICs have historically centralized control over health financing, leading to inequitable distribution of resources. The centralized legacy of resource allocation in these countries creates resistance to new financing models such as performance-based financing or public–private partnerships. This is in line with the findings from [55] who emphasize that institutional inertia often prevents the adoption of innovative financing models in LMICs. The findings from this review suggest that successful financing reforms require institutional adaptation and local capacity-building to overcome institutional barriers to equitable resource allocation. Institutional work by health leaders, policymakers, and civil society actors is critical to overcoming these barriers and ensuring that health financing is aligned with health needs rather than political priorities. This suggests that financing reforms influence health system strengthening through an institutional conversion mechanism: funds only become reform capacity when budgeting rules, administrative planning, and accountability systems are aligned. Where allocation practices remain path-dependent, additional funding may reproduce existing inequalities instead of correcting them.
Financing and resource allocation shaped health system strengthening by determining whether reform ambitions could be translated into material capacity. The synthesis indicates that financing reforms were constrained where allocation systems remained path-dependent, centralised, or politically driven. In such contexts, resource distribution reproduced historical inequalities rather than correcting them. The Institutional Theory helps explain why technically sound financing models may underperform when they are not supported by transparent budgeting, administrative accountability, and local planning capacity. Financing therefore operates as both a material and institutional mechanism: it enables health system strengthening only when allocation rules, administrative systems, and equity objectives are institutionally aligned.
5.5. Digital Governance
Digital governance emerged as an increasingly important aspect of health system strengthening in LMICs. The review found that while digital health technologies have the potential to improve access and efficiency, their implementation is often hindered by institutional barriers such as lack of infrastructure, digital illiteracy, and political resistance. This finding is consistent with the work of [13,83], who highlight the challenges of implementing digital health solutions in LMICs due to institutional resistance and technological constraints. The Institutional theory helps explain why digital health interventions often fail in LMICs. While international actors advocate for the adoption of digital health technologies, these technologies are often imposed without sufficient attention to the local institutional context. Mimetic isomorphism can lead to the adoption of global digital health models that are unsuited to local realities, resulting in poor implementation and limited impact. Institutional work, by local leaders and stakeholders, is necessary to ensure that digital health interventions are contextualized and adapted to local institutional capacities. The findings from this review support the argument that digital health interventions are more likely to succeed when they are tailored to local institutional contexts. This requires a shift from simply replicating global models to engaging in institutional work that adapts these models to local infrastructural needs and digital capabilities. Thus, the institutional mechanism is one of translation. Digital health reforms strengthen systems only when global technological models are translated into local administrative routines, data governance practices, workforce capabilities, and service delivery processes. Without this translation, digital reforms remain isomorphic symbols of modernization rather than instruments of institutional change.
Digital governance influenced health system strengthening through the institutionalisation of information, coordination, and decision-making systems. However, the adoption of digital health tools often reflected isomorphic pressure to modernise rather than context-sensitive institutional transformation. Where digital reforms were introduced into systems with weak infrastructure, limited data use, and inadequate managerial capacity, they risked becoming technological overlays rather than governance improvements. Digital health strengthened systems only when institutional work translated technology into usable administrative routines, data governance arrangements, and service delivery practices. The key mechanism is therefore not technological adoption itself, but institutional embedding.
Across the five themes, the synthesis shows that health system reform outcomes are shaped by the interaction between reform adoption, institutional inheritance, and actor-led adaptation. Isomorphism explains why similar reform models circulate across LMICs; path dependence explains why these models encounter uneven administrative and political conditions; and institutional work explains how reform actors either adapt or fail to embed them into practice. The central analytical finding is therefore that health system strengthening is not produced by reform adoption alone, but by the degree to which reforms become institutionally aligned, locally embedded, and supported by sustained administrative agency.
6. Discussion and Implications
The strengthening of health systems in LMICs requires a multifaceted approach that includes leadership development, institutional capacity building, routine health data, collaborative governance, and the integration of digital innovations. These key elements work in tandem to address the challenges faced by LMICs while enhancing the effectiveness and sustainability of health system reforms. As shown in this study, a critical component of health system strengthening relates to the importance of leadership and institutional capacity. Similarly, ref. [3] have established a direct relationship between strengthening policy development and management systems as linked to an improved coordination and implementation capacity. This underscores the need for effective leadership at various levels of the health system, particularly at the district level, where the gap between national policy and frontline delivery is most apparent, effective management is crucial. Such district-level management is positioned as a decisive interface between national policy intent and frontline delivery, which signals the importance of local governance in translating high-level policies into concrete actions [4]. These findings are consistent with evidence suggesting that improving local management capacity not only enhances service delivery but also builds trust in the health system. However, challenges remain, particularly related to weak accountability and corruption, which continue to undermine service delivery, especially at the frontline where public trust and access to care are most directly affected [6].
In overcoming these barriers, digital health innovations have played a transformative role. For instance, the implementation of digital governance models and the adoption of AI technologies in South Asia have significantly enhanced the quality and accessibility of healthcare, breaking through historical governance barriers [74]. The use of mobile health apps and electronic health records is proving instrumental in bridging gaps in healthcare delivery, especially in underserved regions. In Kenya, mobile health (mHealth) applications are used to monitor antenatal care, allowing health workers to collect real-time data, which is then used for timely interventions. This system has notably reduced maternal mortality rates in rural areas, demonstrating the power of data-driven decision-making [2].
Furthermore, the concept of learning health systems has gained prominence in LMICs. Ref. [12] assert that “learning health systems aim to transform healthcare delivery by incorporating continuous feedback from routine health data to inform ongoing health system improvements”. Such systems are key to adapting and refining health practices based on real-time data, which fosters continuous improvement. A prime example of this is Bangladesh’s National Health Information System (NHIS), which integrates data from local clinics and health posts to track maternal and child health outcomes. The system generates real-time insights that guide health interventions at the district level, ensuring that resources are allocated based on identified needs, leading to better maternal care and improved health outcomes [75].
Moreover, AI is emerging as a valuable tool in predictive health modelling in LMICs with AI applications, such as predictive models for infectious diseases, being used to forecast disease outbreaks, optimize resource allocation, and manage patient care. For instance, in South Africa, AI-driven tools have been successfully employed to track the spread of tuberculosis and forecast hospital admissions, enhancing the planning and responsiveness of health systems [76]. These innovations provide actionable data that can significantly improve health system responses, particularly in areas with limited infrastructure and resources.
In addition to such technological innovations, collaborative and intersectoral governance remains a central pillar of health system strengthening. The role of collaborative governance arrangements, which bring together state and non-state actors, has been shown to improve coordination, legitimacy, and shared accountability in health systems. Evidence emphasizes that collaborative governance arrangements (bringing together state and non-state actors) are essential for improving coordination, legitimacy, and shared accountability in public health [7]. This is particularly important in LMICs, where a fragmented approach to governance often leads to inefficiencies. Rwanda’s Community Health Worker (CHW) program exemplifies successful intersectoral governance, where government health agencies, NGOs, and local communities collaborate to deliver essential health services in rural areas. The program has had a significant impact on improving access to primary healthcare and reducing maternal and child mortality rates [84].
However, the challenge remains in managing these collaborative partnerships effectively. It has been widely argued that while these partnerships can drive improvements, the administrative arrangements needed to support these partnerships are critical for their sustainability [8]. For instance, in Zambia, a partnership between the Ministry of Health and non-governmental organizations (NGOs) has shown promise in improving maternal health services. However, the success of such partnerships depends on sustained administrative support and resource allocation to ensure that they remain effective over time [4]. This highlights the importance of strong governance frameworks to manage and sustain intersectoral partnerships.
The evidence in this study suggests that health system strengthening in LMICs can be achieved through a combination of strong leadership, collaborative governance, digital innovations, and learning health systems. The integration of routine health data, AI technologies, and mHealth applications offers new pathways for improving health outcomes, particularly in resource-limited settings. Examples from the LMICs cases provide tangible evidence of the potential for digital health innovations to enhance service delivery and governance. However, to ensure long-term success, these innovations must be supported by robust administrative systems and sustained partnerships across sectors. As health systems evolve, the continued integration of data, technology, and collaborative frameworks will be key to achieving sustainable improvements in health service delivery and universal health coverage.
7. Recommendations for Future Research
Future studies could examine the role of individual agency in shaping health system governance and explore how leaders and civil society actors navigate institutional constraints to drive reform. There is a need for more longitudinal and quasi-experimental studies assessing how leadership reforms, decentralisation policies, and accountability mechanisms affect measurable health outcomes over time. Governance scholarship [20,46] would benefit from stronger causal designs linking institutional change to service delivery indicators.
Future research should move beyond national-level comparisons and examine subnational institutional variation. Studies such as [53] demonstrate the value of localised governance analysis. Political economy approaches could deepen understanding of how resource allocation decisions [58,65] are shaped by power dynamics. Furthermore, digital health evidence is concentrated in Asian contexts [74,77]. Research from African and Latin American LMICs is needed to assess transferability and equity implications of AI and digital health platforms. Additionally, long-term institutional integration studies are required beyond pilot implementation phases [13].
8. Conclusions
This study has provided a comprehensive analysis of the institutional dynamics influencing health system strengthening in LMICs, using the institutional theory as the primary theoretical framework. The study underscores the importance of strong leadership and institutional capacity in driving successful health reforms in LMICs. Effective management at the district level is particularly crucial in bridging the gap between national policies and frontline service delivery. The study concludes that the decentralization of decision-making and strengthening local management capacities can significantly improve health system performance, ensuring more responsive and context-specific interventions. However, weak accountability and corruption remain persistent challenges that must be addressed to ensure that reforms are sustainable and effective. The integration of digital health technologies such as AI, mobile health (mHealth) applications, and electronic health records has shown considerable potential in overcoming traditional barriers in health service delivery. While substantial progress has been made in integrating digital health innovations and improving local governance, significant challenges remain. The study highlights that administrative capacity, infrastructure for digital tools, and political will are critical to sustaining these reforms. As LMICs continue to explore innovative approaches to health system strengthening, there is an urgent need for capacity-building at both local and national levels, especially in managing and sustaining intersectoral partnerships and digital health initiatives. The integration of learning health systems and data-driven decision-making presents a significant opportunity for health systems to adapt and improve continuously, but this requires investment in data infrastructure and capacity-building for health professionals to use these tools effectively. This study reinforces the idea that health system strengthening in LMICs requires a holistic approach that combines strong leadership, effective governance, digital innovations, and collaborative governance. By focusing on local capacity-building, data-driven decision-making, and sustained partnerships, LMICs can move towards more resilient and responsive health systems, capable of addressing both current challenges and future demands in healthcare delivery.
Author Contributions
Conceptualization, J.N. and Z.M.; methodology, J.N. and Z.M.; software, J.N.; validation, J.N. and Z.M.; formal analysis, J.N. and Z.M.; investigation, J.N. and Z.M.; resources, J.N. and Z.M.; data curation, J.N. and Z.M.; writing—original draft preparation, J.N.; writing—review and editing, J.N. and Z.M.; visualization, J.N.; supervision, Z.M.; project administration, J.N. and Z.M.; funding acquisition, J.N. and Z.M. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Ethical review and approval were waived for this study due to the study using secondary sources publicly accessible and no interviews were conducted. The study was conducted in accordance with the Declaration of Helsinki, and in accordance with the Ethics Principles of Durban University of Technology.
Informed Consent Statement
Not Applicable.
Data Availability Statement
No new data were created or analyzed in this study.
Conflicts of Interest
The authors declare no conflict of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| ASEAN | Association of Southeast Asian Nations |
| LMIC | Low- and Middle-Income Countries |
| NHIS | National Health Information System |
| HSS | Health system strengthening |
| NGOs | Non-Governmental Organizations |
| WHO | World Health Organisation |
| NCD | Non-communicable Diseases |
| CHW | Community Health Worker |
| AI | Artificial Intelligence |
References
- Hasan, M.Z.; Neill, R.; Das, P.; Venugopal, V.; Arora, D.; Bishai, D.; Jain, N.; Gupta, S. Integrated health service delivery during COVID-19: A scoping review of published evidence from low-income and lower-middle-income countries. BMJ Glob. Health 2021, 6, e005667. [Google Scholar] [CrossRef] [PubMed]
- Peiris, D.; Sharma, M.; Praveen, D.; Bitton, A.; Bresick, G.; Coffman, M.; Dodd, R.; El-Jardali, F.; Fadlallah, R.; Flinkenflögel, M.; et al. Strengthening primary health care in the COVID-19 era: A review of best practices to inform health system responses in low-and middle-income countries. WHO South-East Asia J. Public Health 2021, 10, S6–S25. [Google Scholar] [CrossRef]
- Lane, J.; Andrews, G.; Orange, E.; Brezak, A.; Tanna, G.; Lebese, L.; Carter, T.; Naidoo, E.; Levendal, E.; Katz, A. Strengthening health policy development and management systems in low-and middle-income countries: South Africa’s approach. Health Policy OPEN 2020, 1, 100010. [Google Scholar] [CrossRef]
- Omar, M.A. Strengthening district health management in low-middle income countries: Reflections and way forward. J. Adm. Kesehat. Indones. 2020, 8, 123–140. [Google Scholar] [CrossRef]
- Petersen, I.; Marais, D.; Abdulmalik, J.; Ahuja, S.; Alem, A.; Chisholm, D.; Egbe, C.; Gureje, O.; Hanlon, C.; Lund, C.; et al. Strengthening mental health system governance in six low-and middle-income countries in Africa and South Asia: Challenges, needs and potential strategies. Health Policy Plan. 2017, 32, 699–709. [Google Scholar] [CrossRef]
- Naher, N.; Hoque, R.; Hassan, M.S.; Balabanova, D.; Adams, A.M.; Ahmed, S.M. The influence of corruption and governance in the delivery of frontline health care services in the public sector: A scoping review of current and future prospects in low and middle-income countries of south and south-east Asia. BMC Public Health 2020, 20, 880. [Google Scholar]
- Emerson, K. Collaborative governance of public health in low-and middle-income countries: Lessons from research in public administration. BMJ Glob. Health 2018, 3, e000381. [Google Scholar] [CrossRef]
- Fanelli, S.; Salvatore, F.P.; De Pascale, G.; Faccilongo, N. Insights for the future of health system partnerships in low and middle-income countries: A systematic literature review. BMC Health Serv. Res. 2020, 20, 571. [Google Scholar] [CrossRef]
- Langlois, E.V.; McKenzie, A.; Schneider, H.; Mecaskey, J.W. Measures to strengthen primary health-care systems in low-and middle-income countries. Bull. World Health Organ. 2020, 98, 781. [Google Scholar] [CrossRef] [PubMed]
- Lemma, S.; Janson, A.; Persson, L.Å.; Wickremasinghe, D.; Källestål, C. Improving quality and use of routine health information system data in low-and middle-income countries: A scoping review. PLoS ONE 2020, 15, e0239683. [Google Scholar] [CrossRef]
- Koon, A.D.; Windmeyer, L.; Bigdeli, M.; Charles, J.; El Jardali, F.; Uneke, J.; Bennett, S. A scoping review of the uses and institutionalisation of knowledge for health policy in low-and middle-income countries. Health Res. Policy Syst. 2020, 18, 7. [Google Scholar] [CrossRef]
- Sheikh, K.; Agyepong, I.; Jhalani, M.; Ammar, W.; Hafeez, A.; Pyakuryal, S.; Abimbola, S.; Ghaffar, A.; Swaminathan, S. Learning health systems: An empowering agenda for low-income and middle-income countries. Lancet 2020, 395, 476–477. [Google Scholar] [CrossRef] [PubMed]
- Ciecierski-Holmes, T.; Singh, R.; Axt, M.; Brenner, S.; Barteit, S. Artificial intelligence for strengthening healthcare systems in low-and middle-income countries: A systematic scoping review. npj Digit. Med. 2022, 5, 162. [Google Scholar] [CrossRef]
- Xiong, S.; Lu, H.; Peoples, N.; Duman, E.K.; Najarro, A.; Ni, Z.; Gong, E.; Yin, R.; Ostbye, T.; Palileo-Villanueva, L.M.; et al. Digital health interventions for non-communicable disease management in primary health care in low-and middle-income countries. npj Digit. Med. 2023, 6, 12. [Google Scholar] [CrossRef] [PubMed]
- Diaconu, K.; Witter, S.; Binyaruka, P.; Borghi, J.; Brown, G.W.; Singh, N.; Herrera, C.A. Appraising pay-for-performance in healthcare in low-and middle-income countries through systematic reviews: Reflections from two teams. Cochrane Database Syst. Rev. 2022, ED000157. [Google Scholar] [CrossRef]
- Singh, D.R.; Sah, R.K.; Simkhada, B.; Darwin, Z. Potentials and challenges of using co-design in health services research in low-and middle-income countries. Glob. Health Res. Policy 2023, 8, 5. [Google Scholar] [CrossRef]
- Bulthuis, S.E.; Kok, M.C.; Raven, J.; Dieleman, M.A. Factors influencing the scale-up of public health interventions in low-and middle-income countries: A qualitative systematic literature review. Health Policy Plan. 2020, 35, 219–234. [Google Scholar] [CrossRef] [PubMed]
- Grimm, P.Y.; Oliver, S.; Merten, S.; Han, W.W.; Wyss, K. Enhancing the understanding of resilience in health systems of low-and middle-income countries: A qualitative evidence synthesis. Int. J. Health Policy Manag. 2021, 11, 899. [Google Scholar] [CrossRef]
- Debie, A.; Khatri, R.B.; Assefa, Y. Successes and challenges of health systems governance towards universal health coverage and global health security: A narrative review and synthesis of the literature. Health Res. Policy Syst. 2022, 20, 50. [Google Scholar] [CrossRef]
- George, J.; Jack, S.; Gauld, R.; Colbourn, T.; Stokes, T. Impact of health system governance on healthcare quality in low-income and middle-income countries: A scoping review. BMJ Open 2023, 13, e073669. [Google Scholar] [CrossRef]
- Bitton, A.; Fifield, J.; Ratcliffe, H.; Karlage, A.; Wang, H.; Veillard, J.H.; Schwarz, D.; Hirschhorn, L.R. Primary healthcare system performance in low-income and middle-income countries: A scoping review of the evidence from 2010 to 2017. BMJ Glob. Health 2019, 4, e001551. [Google Scholar] [CrossRef] [PubMed]
- Dodd, R.; Palagyi, A.; Jan, S.; Abdel-All, M.; Nambiar, D.; Madhira, P.; Balane, C.; Tian, M.; Joshi, R.; Abimbola, S.; et al. Organisation of primary health care systems in low-and middle-income countries: Review of evidence on what works and why in the Asia-Pacific region. BMJ Glob. Health 2019, 4, e001487. [Google Scholar] [CrossRef]
- DiMaggio, P.J.; Powell, W.W. The iron cage revisited: Institutional isomorphism and collective rationality in organizational fields. Am. Sociol. Rev. 1983, 48, 147–160. [Google Scholar] [CrossRef]
- Peters, B.G. Institutional theory. In The SAGE Handbook of Governance; SAGE: Thousand Oaks, CA, USA, 2011; pp. 78–90. [Google Scholar]
- Luna-Reyes, L.F.; Gil-Garcia, J.R. Using institutional theory and dynamic simulation to understand complex e-Government phenomena. Gov. Inf. Q. 2011, 28, 329–345. [Google Scholar] [CrossRef]
- Thoenig, J.C. Institutional theories and public institutions: New agendas and appropriateness. In The SAGE Handbook of Public Administration; SAGE: Thousand Oaks, CA, USA, 2012; pp. 169–179. [Google Scholar]
- Pirrolas, O.A.C.; Correia, P.M.A.R. From Isomorphism to Institutional Work: The Advancement of Institutional Theory in Public Administration. Encyclopedia 2025, 5, 184. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akle, A.; Brennan, S.; et al. The PriSMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Saif-Ur-Rahman, K.M.; Mamun, R.; Anwar, I. Identifying gaps in primary healthcare policy and governance in low income and middle-income countries: Protocol for an evidence gap map. BMJ Open 2019, 9, e024316. [Google Scholar] [CrossRef]
- Munar, W.; Snilstveit, B.; Aranda, L.E.; Biswas, N.; Baffour, T.; Stevenson, J. Evidence gap map of performance measurement and management in primary healthcare systems in low-income and middle-income countries. BMJ Glob. Health 2019, 4, e001451. [Google Scholar] [CrossRef]
- Amenta, E.; Ramsey, K.M. Institutional theory. In Handbook of Politics: State and Society in Global Perspective; Springer: New York, NY, USA, 2010; pp. 15–39. [Google Scholar]
- Adam, T.; de Savigny, D. Systems thinking for strengthening health systems in LMICs: Need for a paradigm shift. Health Policy Plan. 2012, 27, iv1–iv3. [Google Scholar] [CrossRef]
- Adam, T.; Hsu, J.; De Savigny, D.; Lavis, J.N.; Røttingen, J.A.; Bennett, S. Evaluating health systems strengthening interventions in low-income and middle-income countries: Are we asking the right questions? Health Policy Plan. 2012, 27, iv9–iv19. [Google Scholar] [CrossRef] [PubMed]
- Shakarishvili, G.; Atun, R.; Berman, P.; Hsiao, W.; Burgess, C.; Lansang, M.A. Converging health systems frameworks: Towards a concepts-to-actions roadmap for health systems strengthening in low- and middle-income countries. Glob. Health Gov. 2010, 3. [Google Scholar]
- Balabanova, D.; Mills, A.; Conteh, L.; Akkazieva, B.; Banteyerga, H.; Dash, U.; Gilson, L.; Harmer, A.; Ibraimova, A.; Islam, Z.; et al. Good health at low cost 25 years on: Lessons for the future of health systems strengthening. Lancet 2013, 381, 2118–2133. [Google Scholar] [CrossRef]
- Gonzalez Block, M.A.; Mills, A. Assessing capacity for health policy and systems research in low- and middle-income countries. Health Res. Policy Syst. 2003, 1, 1. [Google Scholar] [CrossRef] [PubMed]
- Gilson, L.; Raphaely, N. The terrain of health policy analysis in low- and middle-income countries: A review of published literature 1994–2007. Health Policy Plan. 2008, 23, 294–307. [Google Scholar] [CrossRef]
- Kayesa, N.K.; Shung-King, M. The role of document analysis in health policy analysis studies in low and middle-income countries: Lessons for HPA researchers from a qualitative systematic review. Health Policy OPEN 2021, 2, 100024. [Google Scholar] [CrossRef]
- Okyere, D.O.; Lomazzi, M.; Peri, K.; Moore, M. Investing in health system resilience: A scoping review to identify strategies for enhancing preparedness and response capacity. Popul. Med. 2024, 6, 6. [Google Scholar] [CrossRef]
- Siddiqi, S.; Aftab, W.; Siddiqui, F.J.; Huicho, L.; Mogilevskii, R.; Friberg, P.; Lindgren-Garcia, J.; Causevic, S.; Khamis, A.; Shah, M.M.; et al. Global strategies and local implementation of health and health-related SDGs: Lessons from consultation in countries across five regions. BMJ Glob. Health 2020, 5, e002859. [Google Scholar] [CrossRef]
- Witter, S.; Sheikh, K.; Schleiff, M. Learning health systems in low-income and middle-income countries: Exploring evidence and expert insights. BMJ Glob. Health 2022, 7, e008115. [Google Scholar] [CrossRef]
- Kalaris, K.W. Developing an Understanding of Networks in LMIC Health Systems: How and Why Networks Change Practices to Improve Service Delivery and Quality of Care. Doctoral Dissertation, University of Oxford, Oxford, UK, 2024. [Google Scholar]
- Agyepong, I.A.; Lehmann, U.; Rutembemberwa, E.; Babich, S.M.; Frimpong, E.; Kwamie, A.; Olivier, J.; Teddy, G.; Hwabamungu, B.; Gilson, L. Strategic leadership capacity building for Sub-Saharan African health systems and public health governance: A multi-country assessment of essential competencies and optimal design for a Pan African DrPH. Health Policy Plan. 2018, 33, ii35–ii49. [Google Scholar] [CrossRef] [PubMed]
- Bennett, S.; Glandon, D.; Rasanathan, K. Governing multisectoral action for health in low-income and middle-income countries: Unpacking the problem and rising to the challenge. BMJ Glob. Health 2018, 3, e000880. [Google Scholar] [CrossRef] [PubMed]
- Ciccone, D.K.; Vian, T.; Maurer, L.; Bradley, E.H. Linking governance mechanisms to health outcomes: A review of the literature in low-and middle-income countries. Soc. Sci. Med. 2014, 117, 86–95. [Google Scholar] [CrossRef] [PubMed]
- Cobos Muñoz, D.; Merino Amador, P.; Monzon Llamas, L.; Martinez Hernandez, D.; Santos Sancho, J.M. Decentralization of health systems in low- and middle-income countries: A systematic review. Int. J. Public Health 2017, 62, 219–229. [Google Scholar] [CrossRef]
- Effa, E.; Arikpo, D.; Oringanje, C.; Udo, E.; Esu, E.; Sam, O.; Okoroafor, S.; Oyo-Ita, A.; Meremikwu, M. Human resources for health governance and leadership strategies for improving health outcomes in low-and middle-income countries: A narrative review. J. Public Health 2021, 43, i67–i85. [Google Scholar] [CrossRef]
- Houngbo, P.T.; Coleman, H.L.S.; Zweekhorst, M.; De Cock Buning, T.; Medenou, D.; Bunders, J.F.G. A model for good governance of healthcare technology management in the public sector: Learning from evidence-informed policy development and implementation in Benin. PLoS ONE 2017, 12, e0168842. [Google Scholar] [CrossRef]
- Jailobaeva, K.; Falconer, J.; Loffreda, G.; Arakelyan, S.; Witter, S.; Ager, A. An analysis of policy and funding priorities of global actors regarding noncommunicable disease in low-and middle-income countries. Glob. Health 2021, 17, 68. [Google Scholar] [CrossRef]
- Madon, S.; Krishna, S. Theorizing community health governance for strengthening primary healthcare in LMICs. Health Policy Plan. 2022, 37, 706–716. [Google Scholar] [CrossRef]
- Saif-Ur-Rahman, K.M.; Mamun, R.; Nowrin, I.; Hossain, S.; Islam, K.; Rumman, T.; Kabir, E.; Rahman, A.; Dahal, N.; Anwar, I. Primary healthcare policy and governance in low-income and middle-income countries: An evidence gap map. BMJ Glob. Health 2019, 4, e001453. [Google Scholar] [CrossRef]
- Zwanikken, P.A.; Alexander, L.; Scherpbier, A. Impact of MPH programs: Contributing to health system strengthening in low-and middle-income countries? Hum. Resour. Health 2016, 14, 52. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Masefield, S.C.; Msosa, A.; Grugel, J. Challenges to effective governance in a low-income healthcare system: A qualitative study of stakeholder perceptions in Malawi. BMC Health Serv. Res. 2020, 20, 1142. [Google Scholar] [CrossRef]
- Khatri, R.B.; Endalamaw, A.; Erku, D.; Wolka, E.; Nigatu, F.; Zewdie, A.; Assefa, Y. Contribution of health system governance in delivering primary health care services for universal health coverage: A scoping review. PLoS ONE 2025, 20, e0318244. [Google Scholar] [CrossRef] [PubMed]
- Stenberg, K.; Hanssen, O.; Edejer, T.T.T.; Bertram, M.; Brindley, C.; Meshreky, A.; Rosen, J.E.; Stover, J.; Verboom, P.; Sanders, R.; et al. Financing transformative health systems towards achievement of the health Sustainable Development Goals: A model for projected resource needs in 67 low-income and middle-income countries. Lancet Glob. Health 2017, 5, e875–e887. [Google Scholar] [CrossRef]
- Erlangga, D.; Powell-Jackson, T.; Balabanova, D.; Hanson, K. Determinants of government spending on primary healthcare: A global data analysis. BMJ Glob. Health 2023, 8, e012562. [Google Scholar] [CrossRef]
- Myint, C.Y.; Pavlova, M.; Thein, K.N.N.; Groot, W. A systematic review of the health-financing mechanisms in the Association of Southeast Asian Nations countries and the People’s Republic of China: Lessons for the move towards universal health coverage. PLoS ONE 2019, 14, e0217278. [Google Scholar] [CrossRef]
- Love-Koh, J.; Griffin, S.; Kataika, E.; Revill, P.; Sibandze, S.; Walker, S. Methods to promote equity in health resource allocation in low-and middle-income countries: An overview. Glob. Health 2020, 16, 6. [Google Scholar] [CrossRef] [PubMed]
- Kodali, P.B. Achieving universal health coverage in low-and middle-income countries: Challenges for policy post-pandemic and beyond. Risk Manag. Healthc. Policy 2023, 16, 607–621. [Google Scholar] [CrossRef] [PubMed]
- Khattak, A.F.; Rahman, A.U.; Khattak, M.; Qazi, M.; Gilani, H.; Khan, A.; Rehman, A.U. Toward sustainable healthcare systems: A low and middle-income Country’s case for investing in healthcare reforms. Cureus 2023, 15, e39345. [Google Scholar] [CrossRef]
- Witter, S.; Fretheim, A.; Kessy, F.L.; Lindahl, A.K. Paying for performance to improve the delivery of health interventions in low-and middle-income countries. Cochrane Database Syst. Rev. 2012, 15, CD007899. [Google Scholar] [CrossRef] [PubMed]
- Kruk, M.E.; Porignon, D.; Rockers, P.C.; Van Lerberghe, W. The contribution of primary care to health and health systems in low-and middle-income countries: A critical review of major primary care initiatives. Soc. Sci. Med. 2010, 70, 904–911. [Google Scholar] [CrossRef]
- Bitton, A.; Ratcliffe, H.L.; Veillard, J.H.; Kress, D.H.; Barkley, S.; Kimball, M.; Secci, F.; Wong, E.; Basu, L.; Taylor, C.; et al. Primary health care as a foundation for strengthening health systems in low-and middle-income countries. J. Gen. Intern. Med. 2017, 32, 566–571. [Google Scholar] [CrossRef]
- Frost, D.; Mahmud, M.; Kaiser, M.S.; Musoke, D.; Henry, P.; Islam, S. Innovative approaches to strengthening health systems in low and middle-income countries: Current models, developments, and challenges. Health Policy Technol. 2021, 10, 100567. [Google Scholar] [CrossRef]
- Basu, S.; Andrews, J.; Kishore, S.; Panjabi, R.; Stuckler, D. Comparative performance of private and public healthcare systems in low and middle-income countries: A systematic review. PLoS Med. 2012, 9, e1001244. [Google Scholar] [CrossRef]
- Khan, V.; Khan, A.F.; Junaid, A.; Khan, J.S. Strategies to Enhance Healthcare Delivery at Lower Cost and Greater Efficiency: A Qualitative Study of Hospital Administrators in Punjab, Pakistan. Pak. J. Public Health 2025, 15, 95–99. [Google Scholar] [CrossRef]
- Lewin, S.; Lavis, J.N.; Oxman, A.D.; Bastías, G.; Chopra, M.; Ciapponi, A.; Flottorp, S.; Martí, S.G.; Pantoja, T.; Rada, G.; et al. Supporting the delivery of cost-effective interventions in primary health-care systems in low-income and middle-income countries: An overview of systematic reviews. Lancet 2008, 372, 928–939. [Google Scholar] [CrossRef] [PubMed]
- Simen-Kapeu, A.; Reserva, M.E.; Ekpini, R.E. Galvanizing action on primary health care: Analyzing bottlenecks and strategies to strengthen community health systems in West and Central Africa. Glob. Health Sci. Pract. 2021, 9, S47–S64. [Google Scholar] [CrossRef] [PubMed]
- Bhattacharyya, O.; Khor, S.; McGahan, A.; Dunne, D.; Daar, A.S.; Singer, P.A. Innovative health service delivery models in low- and middle-income countries-what can we learn from the private sector? Health Res. Policy Syst. 2010, 8, 24. [Google Scholar] [CrossRef]
- Pantoja, T.; Opiyo, N.; Lewin, S.; Paulsen, E.; Ciapponi, A.; Wiysonge, C.S.; Herrera, C.A.; Rada, G.; Penaloza, B.; Dudley, L.; et al. Implementation strategies for health systems in low-income countries: An overview of systematic reviews. Cochrane Database Syst. Rev. 2017, 2017, CD011086. [Google Scholar] [CrossRef]
- Rowe, A.K.; Rowe, S.Y.; Peters, D.H.; Holloway, K.A.; Chalker, J.; Ross-Degnan, D. Effectiveness of strategies to improve health-care provider practices in low-income and middle-income countries: A systematic review. Lancet Glob. Health 2018, 6, e1163–e1175. [Google Scholar] [CrossRef] [PubMed]
- Bradley, E.H.; Taylor, L.A.; Cuellar, C.J. Management matters: A leverage point for health systems strengthening in global health. Int. J. Health Policy Manag. 2015, 4, 411. [Google Scholar] [CrossRef]
- Kassai, R.; Van Weel, C.; Flegg, K.; Tong, S.F.; Han, T.M.; Noknoy, S.; Dashtseren, M.; Le An, P.; Ng, C.J.; Khoo, E.M.; et al. Priorities for primary health care policy implementation: Recommendations from the combined experience of six countries in the Asia–Pacific. Aust. J. Prim. Health 2020, 26, 351–357. [Google Scholar] [CrossRef]
- Adhikari, S.; Ahmed, I.; Bajracharya, D.; Khanal, B.; Solomon, C.; Jayaratne, K.; Mamum, K.A.A.; Talukder, M.S.H.; Shakya, S.; Manandhar, S.; et al. Transforming healthcare through just, equitable and quality driven artificial intelligence solutions in South Asia. npj Digit. Med. 2025, 8, 139. [Google Scholar] [CrossRef]
- Rahman, M. Identifying Evidence-Based Strategies to Strengthen the Ability of Social Enterprises to Scale Health Impact in Low-and Middle-Income Countries. Doctoral Dissertation, Duke University, Durham, NC, USA, 2023. [Google Scholar]
- Kepper, M.M.; Fowler, L.A.; Kusters, I.S.; Davis, J.W.; Baqer, M.; Sagui-Henson, S.; Xiao, Y.; Tarfa, A.; Yi, J.C.; Gibson, B.; et al. Expanding a behavioral view on digital health access: Drivers and strategies to promote equity. J. Med. Internet Res. 2024, 26, e51355. [Google Scholar] [CrossRef]
- Yi, S.; Yam, E.L.Y.; Cheruvettolil, K.; Linos, E.; Gupta, A.; Palaniappan, L.; Rajeshuni, N.; Vaska, K.G.; Schulman, K.; Eggleston, K.N. Perspectives of digital health innovations in low-and middle-income health care systems from South and Southeast Asia. J. Med. Internet Res. 2024, 26, e57612. [Google Scholar] [CrossRef] [PubMed]
- Hadjiat, Y. Healthcare inequity and digital health—A bridge for the divide, or further erosion of the chasm? PLoS Digit. Health 2023, 2, e0000268. [Google Scholar] [CrossRef]
- Jianming, Z.; Maqbool, M. Digital Health Transformation in Asian Healthcare Systems. J. Soc. Inform. Glob. Health 2022, 1, 01–15. [Google Scholar]
- Labrique, A.B.; Wadhwani, C.; Williams, K.A.; Lamptey, P.; Hesp, C.; Luk, R.; Aerts, A. Best practices in scaling digital health in low- and middle-income countries. Glob. Health 2018, 14, 103. [Google Scholar] [CrossRef]
- Wyber, R.; Vaillancourt, S.; Perry, W.; Mannava, P.; Folaranmi, T.; Celi, L.A. Big data in global health: Improving health in low-and middle-income countries. Bull. World Health Organ. 2015, 93, 203–208. [Google Scholar] [CrossRef]
- Vandenabeele, W. Toward a public administration theory of public service motivation: An institutional approach. Public Manag. Rev. 2007, 9, 545–556. [Google Scholar] [CrossRef]
- Zheng, D.; Chen, J.; Huang, L.; Zhang, C. E-government adoption in public administration organizations: Integrating institutional theory perspective and resource-based view. Eur. J. Inf. Syst. 2013, 22, 221–234. [Google Scholar] [CrossRef]
- Gilson, L.; Lehmann, U.; Schneider, H. Practicing governance towards equity in health systems: LMIC perspectives and experience. Int. J. Equity Health 2017, 16, 171. [Google Scholar] [CrossRef] [PubMed]




Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license.