





Surgeries 2026, 7(3), 83; https://doi.org/10.3390/surgeries7030083 - 10 Jul 2026
Abstract
Background: Despite modern technology of energy instruments, secure arterial vessel sealing remains a surgical challenge. Particularly in cases of fragile vessel walls or limited visibility, additional reinforcement techniques are potentially desirable. TachoSil®, a collagen-based, fibrin-coated fleece, is routinely employed in clinical
[...] Read more.
Background: Despite modern technology of energy instruments, secure arterial vessel sealing remains a surgical challenge. Particularly in cases of fragile vessel walls or limited visibility, additional reinforcement techniques are potentially desirable. TachoSil®, a collagen-based, fibrin-coated fleece, is routinely employed in clinical practice for hemostasis and suture support. Whether its external use in terms of collagen augmentation improves the burst strength of bipolarly sealed arteries is to be examined. Objective: To investigate the influence of a TachoSil® cuff on sealing quality and burst pressures after bipolar vessel sealing in a standardized ex vivo model. Materials and Methods: Porcine carotid arteries (outer diameter 5–7 mm) were examined in two groups: native vessels (group A, n = 12) and vessels with TachoSil® cuffs (group B, n = 12). Sealing was performed with marSeal® 5 plus and maXium® sealer. Burst pressures were measured by continuously increasing intraluminal pressure. Histological analyses were performed. Results: Mean burst pressures were significantly reduced in group B (805 ± 78 mbar) as compared to group A (1452 ± 275 mbar; p < 0.001). Histologically, no structural fusion between vessel walls and collagen fleece was observed. Conclusions: External collagen augmentation using TachoSil® leads to a significant reduction in the burst strength of bipolarly sealed arteries, despite unaltered sealing duration. The combination of collagen fleece and energy sealing does not have a synergistic effect and should not be used in planned vessel sealing. Further studies are needed to evaluate the underlying mechanisms and possible alternative augmentation strategies.
Full article
(This article belongs to the Section Cardiothoracic and Vascular Surgery)
►
Show Figures
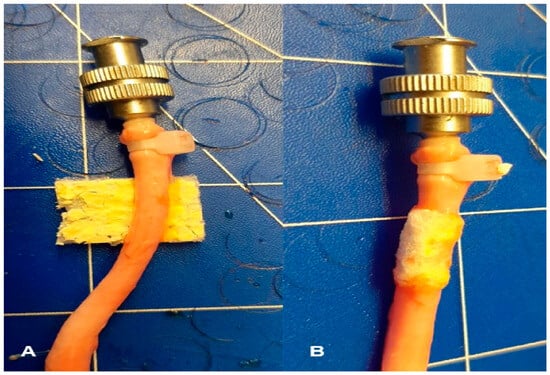
Figure 1
















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}