
Clinical and Demographics Aspects of Foot Angioleiomyomas: Case Reports and Systematic Review
 ,
,
Abstract
1. Introduction and Clinical Significance
2. Case Presentation
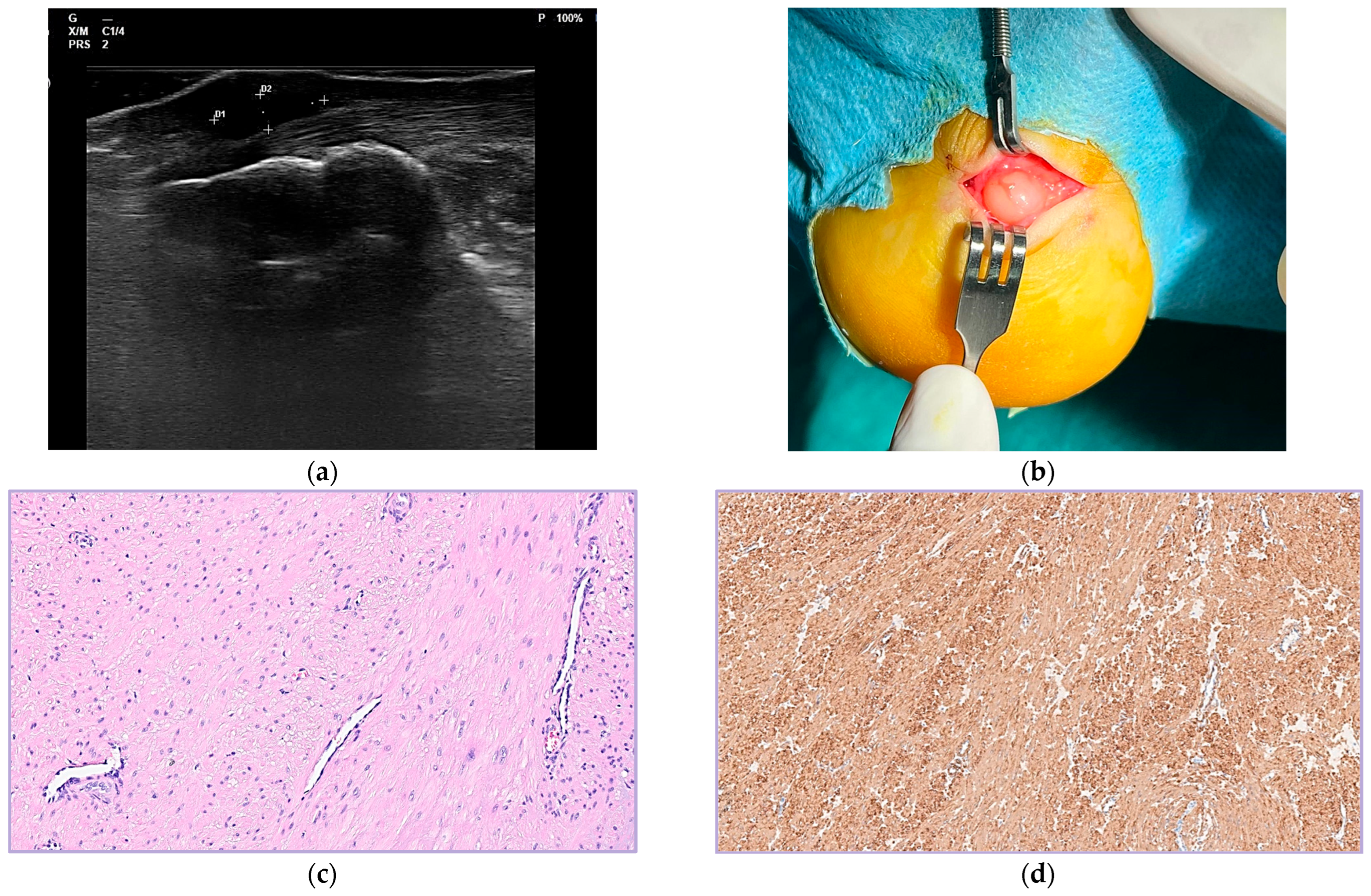
2.1. Case 1
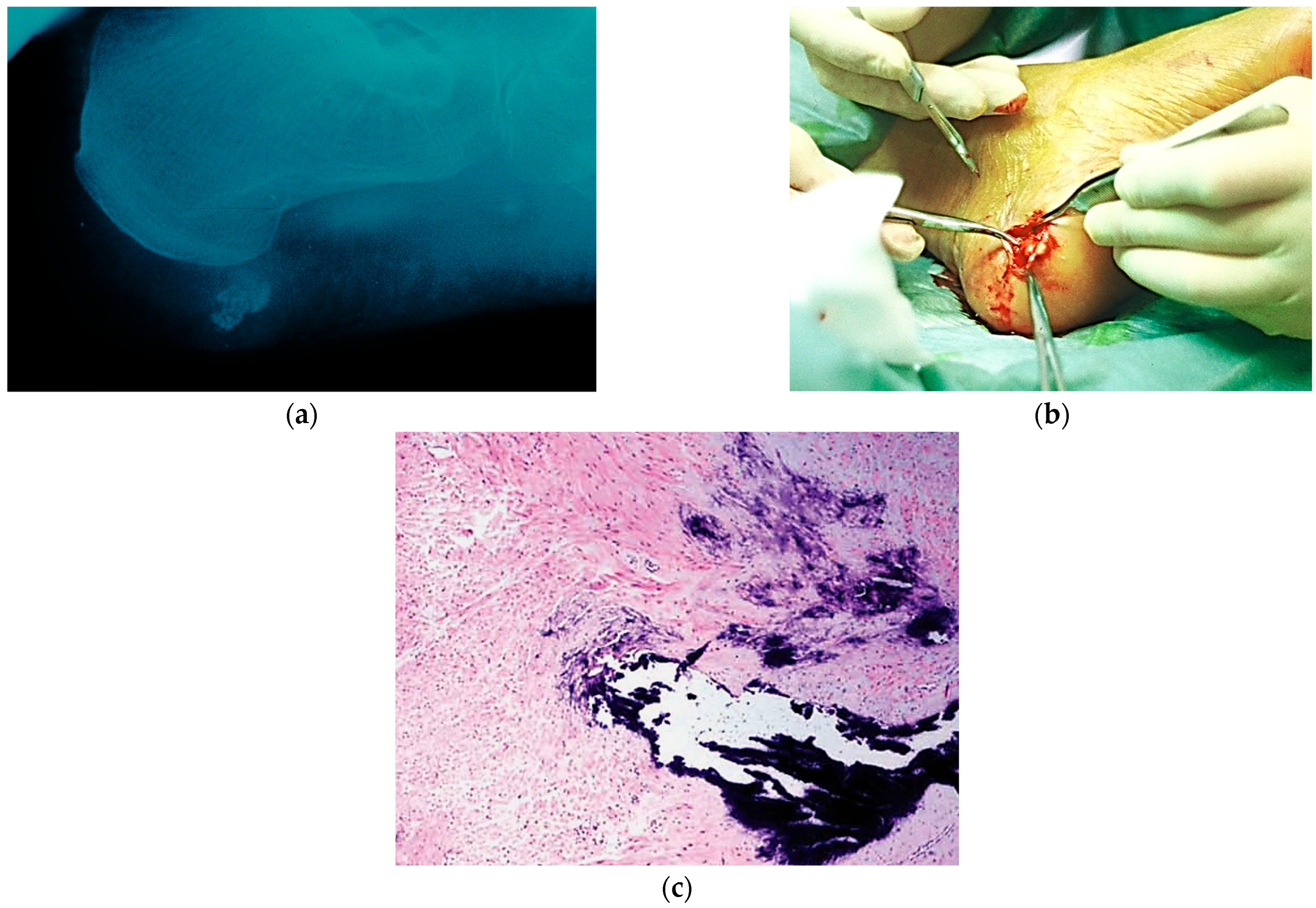
2.2. Case 2
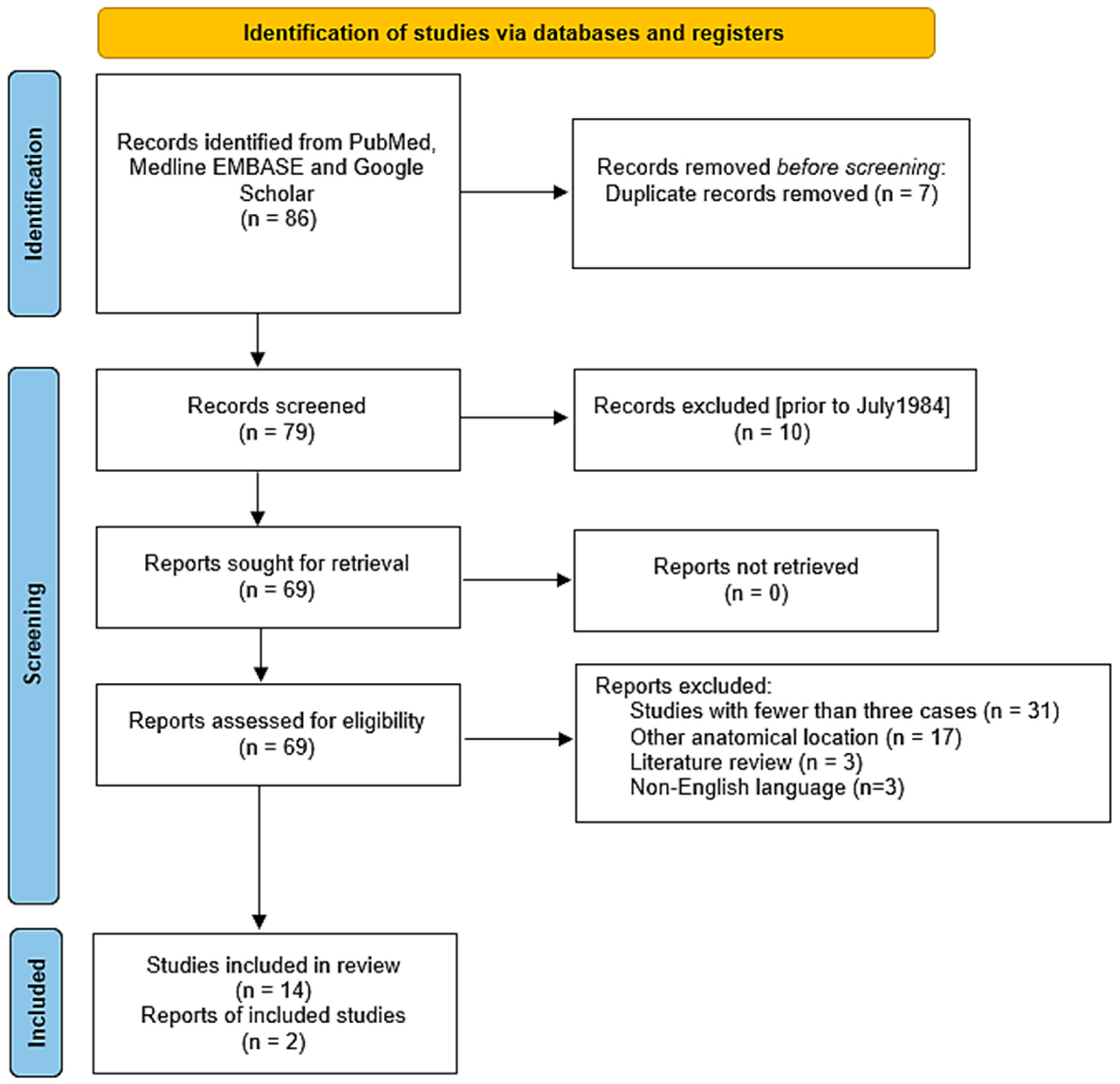
3. Materials and Methods
- A clearly stated aim: The question addressed should be precise and relevant considering the available literature (D1).
- Inclusion of consecutive patients (D2).
- Prospective data collection (D3).
- Explanation of the criteria used to evaluate the main outcome. Endpoints must be assessed on an intention-to-date basis (D4).
- Blind evaluation of objective endpoints and double-blind evaluation of subjective endpoints (D5).
- The follow-up period is appropriate for the purpose of the study (one year minimum) (D6).
- Loss to follow-up is less than 5% (D7).
- Prospective calculation of study size (D8).
4. Results
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| ALM | Angioleiomyoma (singular or plural depending on context) |
| CARE | CAse REport (guidelines for case reports) |
| CC BY | Creative Commons Attribution |
| EMBASE | Excerpta Medica Database |
| H/E | Hematoxylin and Eosin (histological stain) |
| MINORS | Methodological Index for Nonrandomized Studies |
| MRI | Magnetic Resonance Imaging |
| N/A | Not Available |
| PRISMA | Preferred Reporting Items for Systematic Reviews and Meta-Analyses |
| PROSPERO | International Prospective Register of Systematic Reviews |
| SMA | Smooth Muscle Actin |
| US | Ultrasound |
References
- Matos, M.; Soares, S.; Agaoua, M. Current Concepts of Foot and Ankle Angioleiomyoma. J. Foot Ankle Surg. 2023, 62, 746–749. [Google Scholar] [CrossRef]
- Hachisuga, T.; Hashimoto, H.; Enjoji, M. Angioleiomyoma. A Clinicopathologic Reappraisal of 562 Cases. Cancer 1984, 54, 126–130. [Google Scholar] [CrossRef]
- Morimoto, N. Angiomyoma (vascular leiomyoma).: A Clinicopathologic Study. Med. J. Kagoshima Univ. 1973, 24, 663–687. [Google Scholar]
- Bernard, M.; Le Nail, L.R.; de Pinieux, G.; Samargandi, R. Angioleiomyoma: An Update with a 142-Case Series. Life 2024, 14, 338. [Google Scholar] [CrossRef]
- Matsuyama, A.; Hisaoka, M.; Hashimoto, H. Angioleiomyoma: A clinicopathologic and immunohistochemical reappraisal with special reference to the correlation with myopericytoma. Hum. Pathol. 2007, 38, 645–651. [Google Scholar] [CrossRef]
- Maheshwari, A.V.; Temple, H.T.; Murocacho, C.A. Calcified angiomyomas of the foot: A case report. Foot Ankle Int. 2008, 29, 449–455. [Google Scholar] [CrossRef] [PubMed]
- Suárez-Peñaranda, J.M.; Pita da Veiga, G.; Pérez-Muñoz, N.; Fernández-Figueras, M.T. Acral Calcified Vascular Leiomyoma: Report of 3 Cases and Literature Review. Am. J. Dermatopathol. 2021, 43, 732–735. [Google Scholar] [CrossRef] [PubMed]
- Riley, D.S.; Barber, M.S.; Kienle, G.S.; Aronson, J.K.; von Schoen-Angerer, T.; Tugwell, P.; Kiene, H.; Helfand, M.; Altman, D.G.; Sox, H.; et al. CARE Guidelines for Case Reports: Explanation and Elaboration Document. J. Clin. Epidemiol. 2017, 89, 218–235. [Google Scholar] [CrossRef] [PubMed]
- Slim, K.; Nini, E.; Forestier, D.; Kwiatkowski, F.; Panis, Y.; Chipponi, J. Methodological index for non-randomized studies (minors): Development and validation of a new instrument. ANZ J. Surg. 2003, 73, 712–716. [Google Scholar] [CrossRef]
- Kirby, E.J.; Shereff, M.J.; Lewis, M.M. Soft-tissue tumors and tumor-like lesions of the foot. An analysis of eighty-three cases. J. Bone Jt. Surg. Am. 1989, 71, 621–626. [Google Scholar] [CrossRef]
- Gupte, C.; Butt, S.H.; Tirabosco, R.; Saifuddin, A. Angioleiomyoma: Magnetic resonance imaging features in ten cases. Skelet. Radiol. 2008, 37, 1003–1009. [Google Scholar] [CrossRef]
- Hammond, M.I.; Miner, A.G.; Piliang, M.P. Acral and digital angioleiomyomata: 14-year experience at the Cleveland Clinic and review of the literature. J. Cutan. Pathol. 2017, 44, 342–345. [Google Scholar] [CrossRef]
- Zhang, J.Z.; Zhou, J.; Zhang, Z.C. Subcutaneous Angioleiomyoma: Clinical and Sonographic Features with Histopathologic Correlation. J. Ultrasound Med. 2016, 35, 1669–1673. [Google Scholar] [CrossRef]
- Kitagawa, Y.; Sudo, Y.; Tsunoda, R.; Nanno, M.; Arai, S.; Takai, S. Association of Magnetic Resonance Imaging Features with Angioleiomyoma Histologic Subtype. J. Nippon. Med. Sch. 2021, 87, 318–324. [Google Scholar] [CrossRef] [PubMed]
- Ipponi, E.; Bechini, E.; Ruinato, A.D.; Franco, S.; D’Arienzo, A.; Andreani, L. Angioleiomyoma of the Foot: Clinical and Functional Outcomes of Surgical Treatment in a Case Series. J. Am. Podiatr. Med. Assoc. 2024, 114, 23–25. [Google Scholar] [CrossRef] [PubMed]
- Hsieh, M.H.; Izumi, M.; Nakatani, Y.; Ohara, K. Calcified angioleiomyoma—Histopathologic and ultrasonographic analysis of the calcification process. Dermatol. Sin. 2021, 39, 202–205. [Google Scholar] [CrossRef]
- Szolomayer, L.K.; Talusan, P.G.; Chan, W.F.; Lindskog, D.M. Leiomyoma of the Foot and Ankle: A Case Series. Foot Ankle Spec. 2017, 10, 270–273. [Google Scholar] [CrossRef] [PubMed]
- Yates, B.J. Angioleiomyoma: Clinical presentation and surgical management. Foot Ankle Int. 2001, 22, 670–674. [Google Scholar] [CrossRef]
- Kacerovsca, D.; Michal, M.; Kreuzberg, B.; Mukensnabl, P.; Kazacov, D. Acral calcified vascular leiomyoma of the skin:A rare clinicopathological variant of cutaneous vascular leiomyoma. J. Am. Acad. Dermatol. 2008, 59, 1000–1004. [Google Scholar] [CrossRef]
- Bodapati, V.S.; Sunderamoorthy, D. Angioleiomyoma—Rare soft tissue tumor of the foot and ankle, review of two patients and review of the literature. J. Surg. Case Rep. 2021, 2021, rjab535. [Google Scholar] [CrossRef]
- Matos, M.J.; Soares, S.; Schwab, J.M.; Tannast, M.; Seidel, A. Foot and ankle angioleiomyoma: A systematic review. BMC Musculoskelet. Disord. 2025, 26, 246. [Google Scholar] [CrossRef]
- Scheele, C.; Toepfer, A.; Beischl, S.; Dammerer, D.; Harrasser, N.; von Eisenhart-Rothe, R.; Lenze, F. Insights into the Distribution Patterns of Foot and Ankle Tumours: Update on the Perspective of a University Tumour Institute. J. Clin. Med. 2024, 13, 350. [Google Scholar] [CrossRef]
- Córdoba-Fernández, A.; Sánchez-Robles, L.J.; Lobo-Martín, A. Tenosynovial Giant Cell Tumor in the Forefoot: Two Case Reports and Literature Review. J. Am. Podiatr. Med. Assoc. 2021, 111, 25. [Google Scholar] [CrossRef] [PubMed]
- Park, H.J.; Kim, S.S.; Lee, S.Y.; Choi, Y.J.; Chung, E.C.; Rho, M.H. Sonographic appearances of soft tissue angioleiomyomas: Differences from other circumscribed soft tissue hypervascular tumors. J. Ultrasound Med. 2012, 31, 1589–1595. [Google Scholar] [CrossRef]
- Ward, T.R.W.; Eastley, N.C.; Sheikh, N.; Ashford, R.U. Intralesional leiomyosarcoma malignant transformation from a biopsied benign angioleiomyoma of the proximal anterior tibia. BMJ Case Rep. 2024, 17, e259887. [Google Scholar] [CrossRef] [PubMed]
- Herren, D.B.; Zimmermann, A.; Büchler, U. Vascular leiomyoma in an index finger undergoing malignant transformation. J. Hand Surg. Br. 1995, 20, 484–487. [Google Scholar] [CrossRef] [PubMed]
- Trojani, M.; Contesso, G.; Coindre, J.M.; Rouesse, J.; Bui, N.B.; de Mascarel, A.; Goussot, J.F.; David, M.; Bonichon, F.; Lagarde, C. Soft-tissue sarcomas of adults; study of pathological prognostic variables and definition of a histopathological grading system. Int. J. Cancer 1984, 33, 37–42. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| CASE | Reported:  ; Inadequate: ; Inadequate:  ; No reported: ; No reported:  | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Study (Year) | D1 | D2 | D3 | D4 | D5 | D6 | D7 | D8 | Score | Bias risk |
| Bernard et al. (2024) [4] | | | | | | | | | 8 | Moderate |
| Gupte et al. (2008) [11] | | | | | | | | | 8 | Moderate |
| Hachisuga et al. (1984) [2] | | | | | | | | | 7 | Moderate |
| Hammond et al. (2017) [12] | | | | | | | | | 5 | Moderate |
| Ipponi et al. (2024) [15] | | | | | | | | | 10 | Low |
| Zhang et al. (2016) [13] | | | | | | | | | 8 | Moderate |
| Kitagawa et al (2020) [14] | | | | | | | | | 8 | Moderate |
| Maheshwari et al (2008) [6] | | | | | | | | | 9 | Low |
| Hsieh et al. (2021) [16] | | | | | | | | | 7 | Moderate |
| Suarez –Peñaranda et al. (2016) [7] | | | | | | | | | 7 | Moderate |
| Szolomayer et al. (2016) [17] | | | | | | | | | 8 | Moderate |
| Yates et al. (2001) [18] | | | | | | | | | 9 | Moderate |
| Kacerovsca et al. (2008) [19] | | | | | | | | | 3 | High |
| Bodapati et al. (2021) [20] | | | | | | | | | 3 | High |
| Author (Yr) | Total ALMs | Sex | Mean Duration of Symptoms (Yr) | Zone (N) | Mean Diameter Larger (mm) | Subtype (%) | Depth (%) | N of Calcified ALMs (%) |
|---|---|---|---|---|---|---|---|---|
| Bernard et al. (2024) [4] | 34 | 19F; 15M | N/A | Z1: (14) Z5: (2) N/A: (18) | N/A | Solid: (65) Venous: (17) Cavernous: (5) | Subcut: (85) Subap: (8) Cutan: (5) | N/A |
| Gupte et al. (2008) [11] | 3 | 3F | 2 | N/A | N/A | Solid: (100) | N/A | N/A |
| Hachisuga et al. (1984) [2] | 47 | 29F; 18M | N/A | N/A | N/A | Solid: (66) Venous: (23) Cavernous: (11) | N/A | N/A |
| Hammond et al. (2017) [12] | 15 | 9F; 6M | N/A | Z1: (6) Z3: (2) Z5: (2) N/A: (5) | N/A | N/A | N/A | N/A |
| Ipponi et al. (2024) [15] | 13 | 8F; 5M | 1.6 | Z1: (7) Z2: (1) Z4–Z5: (5) | 17.7 | N/A | N/A | N/A |
| Zhang et al. (2016) [13] | 33 | N/A | N/A | N/A | N/A | Solid: (66) Venous: (23) Cavernous: (11) | Subcut: (100) | N/A |
| Kitagawa et al. (2020) [14] | 6 | 5F; 1M | 2.8 | Z1: (1) Z5: (1) N/A: (4) | N/A | (N/A) | Subcut: (83.3) Subap: (16.6) | N/A |
| Maheshwari et al. (2008) [6] | 4 | 1F; 3M | 9.2 | Z2: (1) Z4: (2) Z5: (1) | 27 | Solid: (100) | Subcut: (100) | 4 (100) |
| Hsieh et al. (2021) [16] | 3 (60) | 3F | 16.6 | Z1: (2) Z3: (1) | N/A | Solid:(100) | Subcut: (100) | 3 (100) |
| Suárez-Peñaranda et al. (2021) [7] | 3 (100) | 1F; 2M | N/A | Z1: (2) Z3: (1) | 13 | Solid:(100) | Subcut: (75) Subap: (25) | 3 (100) |
| Szolomayer et al. (2016) [17] | 4 (100) | 4M | 10.0 | Z1: (2) Z3: (1) Z4: (1) | 22.7 | Solid:(100) | Subcut: (100) | None |
| Yates et al. (2001) [18] | 3 (100) | 2F; 1M | 10.0 | Z5: (3) | 20 | Solid:(100) | Subcut: (100) | 1 (25) |
| Kacerovsca el al. (2008) [19] | 2 (100) | 2F | 2 | Z1: (1) Z4: (1) | 37.5 | Solid:(100) | Subcut: (100) | 2 (100) |
| Bodapati et al. (2021) [20] | 2 (100) | 1F; 1M | 1.0 | Z1: (2) | 10.0 | Solid:(100) | Subcut: (100) | None |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Córdoba-Fernández, A.; Mir-Gil, J.; Díaz-Baena, C.; Ballesteros-Mora, M.; Córdoba-Jiménez, V.E.; Castro-Méndez, A. Clinical and Demographics Aspects of Foot Angioleiomyomas: Case Reports and Systematic Review. Surgeries 2025, 6, 66. https://doi.org/10.3390/surgeries6030066
Córdoba-Fernández A, Mir-Gil J, Díaz-Baena C, Ballesteros-Mora M, Córdoba-Jiménez VE, Castro-Méndez A. Clinical and Demographics Aspects of Foot Angioleiomyomas: Case Reports and Systematic Review. Surgeries. 2025; 6(3):66. https://doi.org/10.3390/surgeries6030066
Chicago/Turabian StyleCórdoba-Fernández, Antonio, Joaquín Mir-Gil, Carolina Díaz-Baena, Marina Ballesteros-Mora, Victoria Eugenia Córdoba-Jiménez, and Aurora Castro-Méndez. 2025. "Clinical and Demographics Aspects of Foot Angioleiomyomas: Case Reports and Systematic Review" Surgeries 6, no. 3: 66. https://doi.org/10.3390/surgeries6030066
APA StyleCórdoba-Fernández, A., Mir-Gil, J., Díaz-Baena, C., Ballesteros-Mora, M., Córdoba-Jiménez, V. E., & Castro-Méndez, A. (2025). Clinical and Demographics Aspects of Foot Angioleiomyomas: Case Reports and Systematic Review. Surgeries, 6(3), 66. https://doi.org/10.3390/surgeries6030066