


J. Cardiovasc. Dev. Dis., Volume 13, Issue 2 (February 2026) – 46 articles
Cover Story (view full-size image):
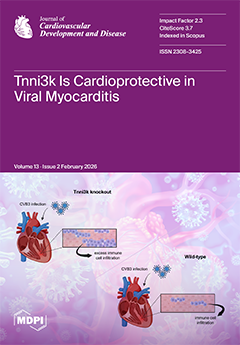
Viral infections that affect the heart induce an inflammatory response (myocarditis), which has the potential to cause heart failure or sudden cardiac death. Earlier studies in mice identified a genetic locus that influences the severity of immune cell infiltration into the heart after coxsackievirus infection. In this study by Tjen et al., Tnni3k, a candidate gene within this locus, is shown to be responsible for this phenotype. In the absence of Tnni3k, a greater number of immune cells, primarily macrophages, colonize the infected heart. Tnni3k is a cardiomyocyte-specific kinase, implicating a cardiomyocyte-specific mechanism that regulates immune cell response to viral infection. View this paper
- Issues are regarded as officially published after their release is announced to the table of contents alert mailing list.
- You may sign up for e-mail alerts to receive table of contents of newly released issues.
- PDF is the official format for papers published in both, html and pdf forms. To view the papers in pdf format, click on the "PDF Full-text" link, and use the free Adobe Reader to open them.
Previous Issue
Next Issue