- Case Report

Cytogenetic and Molecular Pattern of Primary Infertility Male Disorder of Sex Development Involving SRY Translocation on X Chromosome
- Saad Aldalaqan,
- Abdulaziz Alzahrani and
- Abdul A. Peer-Zada
- + 5 authors
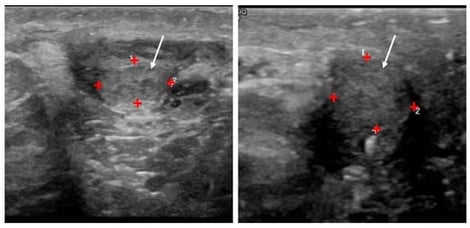
Background: Male DSD is a rare disorder in which individuals with an XX chromosomal background present as phenotypic males due to the presence of the SRY gene translocation. We present here cytogenetic and molecular characterization of rare phenotypic male patients with primary infertility involving SRY translocation on the X chromosome, resulting in the absence of Y centromeric sequences. Methods: Routine hormonal analysis, scrotal ultrasonography, karyotype and FISH analysis were performed. Results: Normal male appearing patients presented with a long history of primary infertility. Physical examination revealed bilateral small, soft testes but reportedly normal libido and erectile function. Hormonal analysis revealed hypergonadotropic hypogonadism with very low total testosterone, high FSH and LH. Semen analysis consistently revealed azoospermia, and multiple testicular sperm extraction procedures and bilateral varicocelectomy failed to retrieve sperm. Karyotyping and FISH showed 46,X,der(X)t(X;Y)(p22.1;p11.2), and SRY-positivity on the derivative X chromosome, respectively. Conclusions: These findings expand the spectrum of 46,XX male infertility with SRY-positivity and underscore the necessity of lifelong testosterone replacement therapy for the management of hypogonadism. Future efforts should aim to establish regional registries for DSD to document genetic diversity surveillance in underrepresented populations.
5 June 2026