Abstract
Background/Objectives: Barbed sutures have been recognised to offer numerous advantages compared to traditional sutures in minimally invasive procedures including holding tension. However, they are also associated with increased reports of small bowel obstructions (SBOs) in laparoscopic procedures. We are the first to conduct a review on the incidence of SBOs secondary to the use of barbed sutures in robotic surgery. Our aim is to raise awareness about this rare complication and promote early recognition and timely intervention, leading to a reduction in the incidence of severe complications and thereby improving patient outcomes. Methods: A systematic review of the literature was performed by searching the Ovoid Medline, PubMed and Cochrane Databases. After applying our exclusion criteria of articles unavailable in English, seven articles remained. We examined the literature and calculated the median and mean ranges for surgical procedures, time to presentation, symptoms of presentation, type of complications involving the bowel, the type of barbed suture and the additional length of hospital stay. Results: Our systematic review revealed eight cases of bowel obstruction secondary to the use of a barbed suture during robotic surgery. Robotic sacrocolpopexy had the highest complication rate: the median time to presentation was 14 days with vomiting being the most common presenting symptom. Most cases were resolved with a diagnostic laparoscopy and truncation of the barbed suture, and length of re-admission was a median of 4 days. Discussion: The introduction of new devices always carries advantages as well as unfortunate complications. Minimisation of complications through learnt surgical techniques including shortening thread tails and prompt recognition of the complication on re-presentation are key to optimising future patient care. Conclusions: Further prospective trials in this field will be useful to assess the appropriate use of the barbed suture as well as research dedicated to exploring alternate adhesive sutures.
1. Introduction
Since the 1960s, barbed sutures have evolved and been adopted for use across multiple specialties including general and gynaecological surgery [1]. Currently, the different types of barbed sutures available on the market are QuillTM knotless tissue closure device (AngiotechTM, Vancouver, BC, Canada), V-LocTM by CovidienTM (CovidienTM, Mansfield, MA, USA) and StratafixTM by EthiconTM (EthiconTM, Cincinnati, OH, USA) [2]. They all present unidirectional or bidirectional barbs orientated in the opposite direction of the needle, which means constant tension can be achieved after a single tightening of the barbed material [1].
The barbs also eliminate the need to tie knots to anchor and finish a suture line, one of the most time-consuming and challenging tasks in minimally invasive surgery [3]. This has led to wide adoption of the barbed suture in laparoscopic surgery. Additional advantages of its use include a reduction in surgical site infections and increased formation of healthy granulation tissue [4]. Gynaecologists readily adopted barbed suture use in myomectomies [5], sarcolpopexies [6] and to close vaginal cuffs [7], and general surgeons used them primarily in laparoscopic inguinal hernia repairs [8], biliary surgery [9] and in the formation of gastro-jejunal anastomoses in gastric bypasses [10]. Unfortunately, with increased use also came increased rates of unintended complications. This included numerous reports of small bowel obstructions caused by bowel becoming entangled in the tail of barbed sutures, leading to negative patient sequelae including re-operation and prolonged hospital re-admissions [2,11,12].
Worldwide, there has been a significant rise in the use of robotic-assisted surgery (RAS), replacing common laparoscopic procedures and accounting for approximately 3% of all surgeries globally [13]. The self-anchoring as well as self-fixing properties of the barbed suture material, removing the need for a surgical assistant, have meant the suture has been widely adopted in robotic surgery across the gynaecological [14], general surgical [15] and urological fields [16]. Additional reported benefits include increased haemostasis [17], shortening of total operative times [17], shortening of time to complete an anastomosis [17] and improved surgical outcomes [18]. However, the unintended complication of the barbed suture tail entangling adjacent small bowel, mesentery or omentum leading to serosal injury, obstruction or volvulus remains a serious risk with increased barbed suture use in robotic surgery [19].
This is the first study to provide an independent overview of the bowel complications that may occur following the use of barbed sutures in robotic surgery, whilst considering the benefits and disadvantages of barbed suture use. Our aim is to raise awareness about this rare complication, to reduce the incidence of occurrence and severity of complications and to improve future patient outcomes through increased understanding of factors for re-presentation, enabling early recognition and timely intervention.
2. Materials and Methods
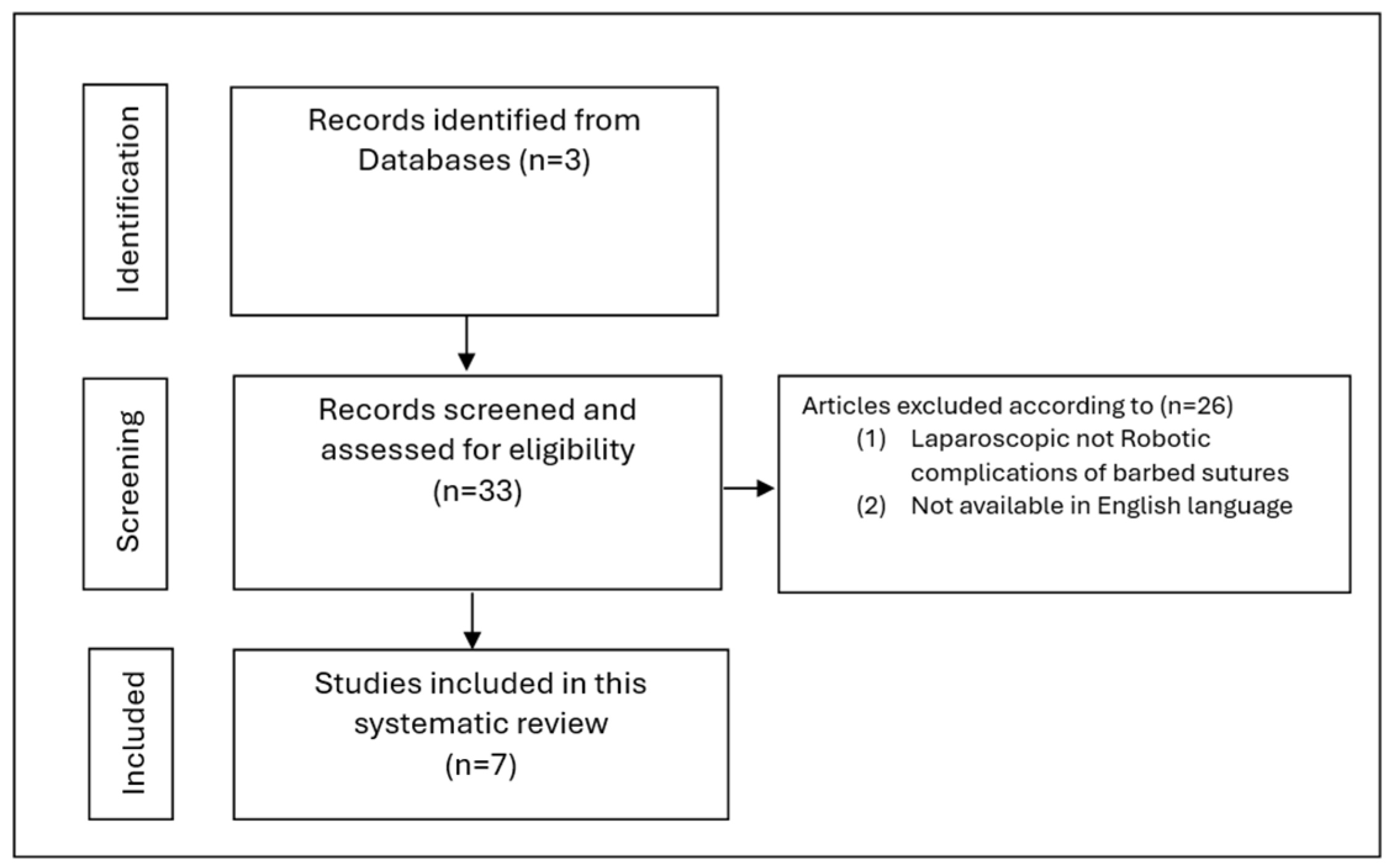
A systematic review of the literature was performed by searching the PubMed, Ovoid Medline and Cochrane Databases over an unlimited period. A protocol was not prepared; however, this systematic review adheres to Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA). To conduct our search, we utilised broad search terms as well as mesh terms including intestinal obstruction, volvulus, barbed sutures, V-Loc, robotic surgical procedures, bowel occlusion, ileus and strangulation. A total of 33 articles were found in this search. Abstracts or articles not published in English were excluded. After applying our exclusion criteria, we were left with seven relevant articles depicting a total of eight patients (Figure 1).
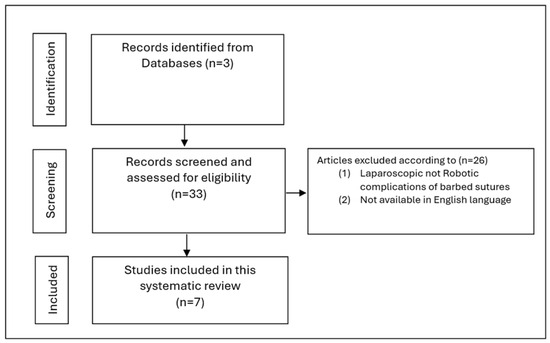
Figure 1.
Flow chart of the systematic review procedure.
The seven articles included were either case series or case reports with accompanying literature reviews. We used the JBI critical appraisal checklist for case reports and case series as an independent tool to assess the inclusion of these articles in our systematic review. ROBINS-1 was utilised to assess the risk of bias, which may be due to reporting bias.
Each article was carefully analysed, and data were collected. The mean and median were calculated on qualitative data pertaining to the initial surgical procedure, type of barbed suture used, time to complication, presenting symptoms, type of complication, type of operative interventions required for treatment and length of hospital stay following re-admission. Due to the novel nature of the study resulting in a small sample size, further statistical analyses including standard deviation and confidence interval were not calculated to avoid the risk of overestimation of the significance of each parameter.
3. Results
3.1. Types of Index Operations
The systematic review yielded eight cases describing bowel obstruction secondary to the use of barbed sutures in robotic surgery. Robot-assisted sacrocolpopexy (RA-SCP) or procedures involving RA-SCP were the most reported procedure (50%) associated with post operative complications when barbed sutures were utilised intraoperatively (Table 1). The additional reported cases included a robot-assisted radical cystectomy, robot-assisted laparoscopic Roux-en-Y gastric bypass and robotic inguinal hernia repair. Six of the cases reported use of the V-LocTM suture, and two cases did not identify the barbed suture manufacturer. The majority utilised a size 3-0 V-LocTM suture (50%), followed by a size 2-00 V-LocTM suture (13%) and the remaining 25% had no identifiable suture size.

Table 1.
Systematic review of the literature.
3.2. Time to Presentation and Common Clinical Presentation
The average time for patients to re-present to hospital during the post operative course was 16 days (median of 14 days), with a range from 3 to 42 days (Table 1). Clinically, patients presented with vomiting (100%), nausea (63%), abdominal distension (38%), abdominal pain (50%) and obstipation (25%) (Table 1).
3.3. Intraoperative Findings and Treatments
The approach to suspected small bowel obstruction secondary to a barbed suture in most cases was a diagnostic laparoscopy (88%), with only one case describing a diagnostic laparotomy as initial treatment. Intraoperatively, all the cases involved the tail of the barbed suture being adhered to the small bowel, causing small bowel obstruction (Figure 2B). Two cases reported progression of the entangled bowel to the ischaemic bowel, requiring resection. The fatty appendages of the sigmoid colon were also found to be adherent to the barbed suture tail in 25% of cases. Most cases were resolved with truncation/removal of the implicated barbed suture tail (63%). Two cases required additional small bowel resection. The average length of stay during these cases was 6 days (median 4 days), with a range from 2 to 18 days (Table 1).
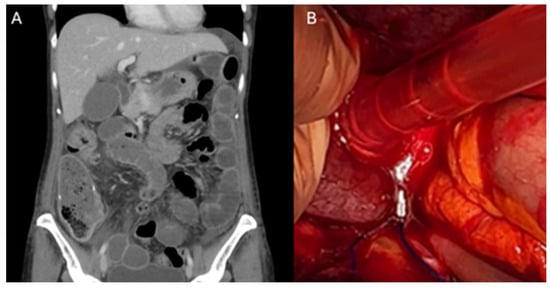
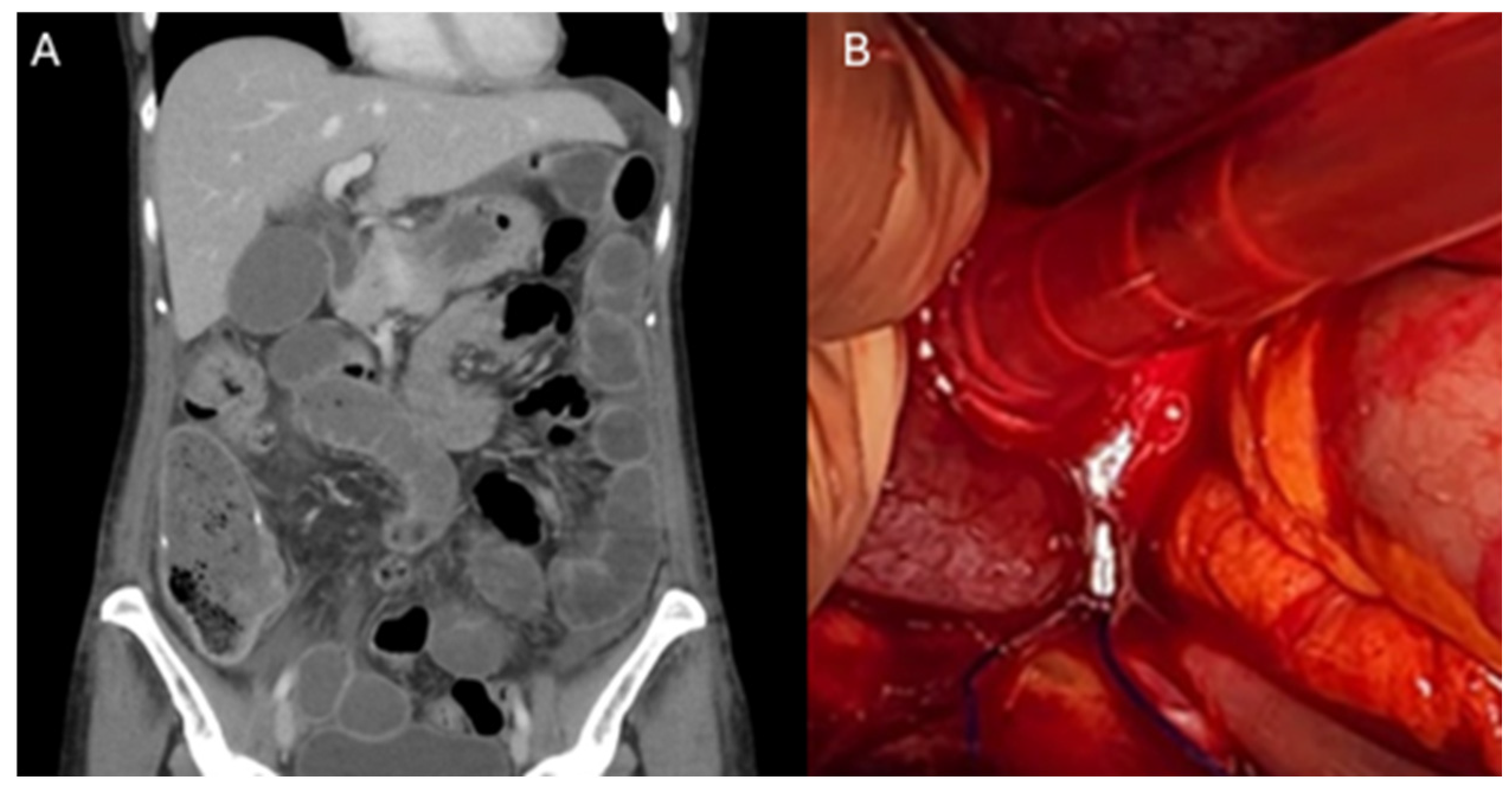
Figure 2.
Small bowel obstruction secondary to entanglement in a barbed suture tail. (A) Coronal section of Computed Tomography scan of the Abdomen and Pelvis (CTAP), demonstrating distended loops of small bowel secondary to entanglement in a barbed suture tail in the pelvis. (B) Intraoperative finding of distended loops of small bowel anchored in the pelvis secondary to entanglement with a barbed suture tail.
4. Discussion
Herein, we present the first systematic review of complications resulting from barbed suture use in robotic surgery. Worldwide, common laparoscopic procedures have been replaced by robot-assisted surgery (RAS) including hysterectomies [26], closure of uterine wall defects [27], colectomies [28] and Roux-en-Y bypass surgeries [1]. Studies comparing traditional sutures to V-Loc barbed sutures in laparoscopic surgery and RAS noted decreasing surgical operative times, ischaemic time, post operative complications and transfusion rates [27,29]. Johnson et al. reported a single-centre study of 15,875 patients undergoing robotic colorectal surgery where 668 cases used barbed sutures, and 175,963 patients undergoing total hysterectomies, where 15,075 cases used barbed sutures. In this study, compared to conventional sutures, barbed sutures showed significantly shorter operating theatre times [30].
4.1. The Use of Barbed Sutures in Robotic Surgery
The V-Loc has several features that make its use desirable during robotic surgery. Firstly, the unidirectional barbed thread fixates itself in tissue, removing the need for an assistant to provide constant tension (Figure 3) [31]. Additionally, it features a loop at the end of the suture (Figure 3B); thus, to secure an anchoring knot, the surgeon simply passes the needle through the loop to secure the suture, which removes one of the most complex and time-consuming robotic skill tasks of knot tying [32]. When asking why surgeons continue to opt for a barbed suture in robotic surgery, it is important to recognise the role of robotic arms.
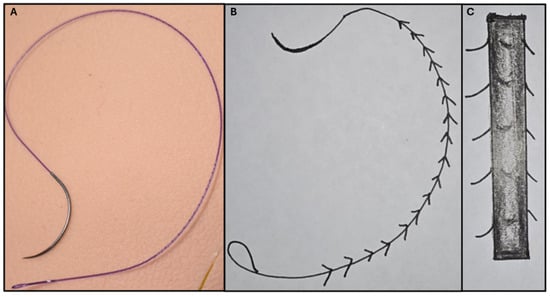
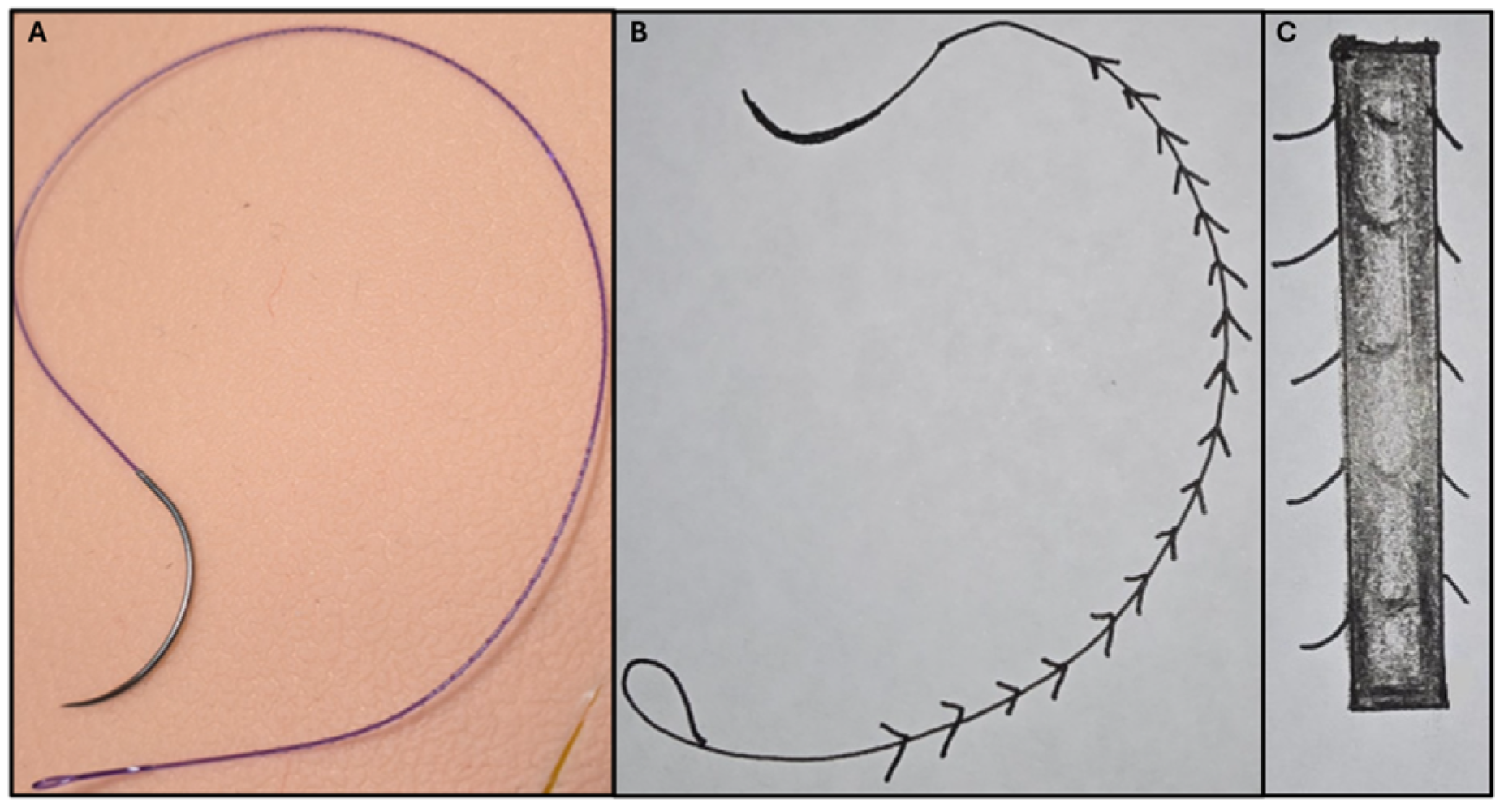
Figure 3.
The barbed suture (A) 3-0 V-LocTM (CovidienTM, Mansfield, MA, USA). (B) Schematic drawing of the barbed suture, demonstrating the advantageous unidirectional barbs and easy anchoring knot technology. (C) Magnified schematic drawing of the barbed suture, demonstrating the advantageous unidirectional barbs.
In theory, the third or fourth arms in robotic surgery could replace the role of the assistant in laparoscopic surgery. The assistant provides constant tension on a traditional suture to prevent it from sliding back during the procedure and leading to laxity in the wound. However, in practice, the fourth arm is typically used for static activities, and if the third instrument was to take over the fourth arm, it would prolong intraoperative time and disrupt the course of the operation because of frequent changes in the two instruments, both of which are controlled by the surgeon’s dominant hand [1]. The use of a second console surgeon on the fourth arm can also be used for dynamic assistance, but this is subject to availability. Given the lack of haptic feedback, a non-barbed thread is often released and gripped more frequently, adding to operating time. These issues are all solved by the use of a barbed suture material in robotic surgery [1]. However, the adhesive properties of the barbed suture cannot be denied, and the potential disadvantage of the barbed suture in the entangling of the adjacent small bowel, mesentery or omentum, leading to serosal injury, obstruction or volvulus remains a serious risk.
4.2. Small Bowel Obstructions Caused by Barbed Sutures
Our systematic review identified eight cases of small bowel obstruction secondary to barbed sutures in robotic surgery. Patients undergoing robot-assisted sacrocolpopexy (RA-SCP) or procedures involving RA-SCP where barbed sutures were utilised intraoperatively had the highest rates of complications in the post operative period (50%). The additional cases reviewed were a robot-assisted radical cystectomy, robot-assisted laparoscopic Roux-en-Y gastric bypass and robotic inguinal hernia repair. RA-SCP has a very long intraoperative time that has been shown to be significantly reduced by using a barbed suture [33]. All eight of the cases reported use of the V-LocTM suture, and the majority utilised a size 3-0 V-LocTM. The V-Loc consists of unidirectional barbs with a unique dual-angle cut and an anchor loop at the other end. It is the dual-angle cut that gives a higher anchoring force compared to a single-angle cut. This unique property may also be contributing to the increased adhesive properties to bowels [18]. Intraoperatively, all cases involved the tail of the barbed suture being adhered to the small bowel, causing obstruction (Figure 2B). This is thought to be either due to most surgeons being accustomed to leaving ~1 cm of suture tail length at the end of a wound because of fear of a non-barbed suture unraveling when cut flush or not accounting for the degree of tissue shrinkage upon healing and/or developing scar tissue leading to greater exposure of the tail of the barbed suture [21].
After discharge post an operation, we found the average time to re-presentation of patient to the hospital emergency department was 16 days (median of 14 days), with a range from 3 to 42 days. Clinically, patients presented with vomiting (100%), nausea (63%) abdominal distension (38%), abdominal pain (50%) and obstipation (25%). Less frequent symptoms reported in the literature include shock, decreased appetite, peritonitis and cervical motion tenderness [11]. Gee et al. described a patient who presented three times within a one-week period. Whilst her symptoms were managed conservatively with bowel rest and nasogastric suction, they did recur [24].
Post operative small bowel obstructions may occur early and be treated less conservatively. To prevent more serious complications including progression to ischaemic bowel, all referred surgical registrars, fellows and consultants alike should have a high index of suspicion for patient’s presenting with abdominal pain. They should talk to the patient’s primary operating surgeon and ask if a barbed suture was utilised, and when revising the operative note, pay special attention to the type of suture utilised. If a barbed suture was utilised, a low threshold for emergent surgical re-exploration should be adopted.
Imaging in this subgroup of patients with Computed Tomography scans of the Abdomen and Pelvis (CTAP) typically demonstrates distension of the small bowel (Figure 2A); however, this may also appear as a volvulus. The barbed suture tail can act as a fixed point for the bowel to rotate around, creating a volvulus and potentially leading to ischaemia. CT scan findings in these cases have been found to often accurately correlate with intraoperative findings.
The most common approach to treatment was surgical intervention. Diagnostic laparoscopy was the predominant initial operation (88%), with a low threshold to convert to a laparotomy if required. This is congruent with the wider literature, which recognises that the laparoscopic approach is safe and effective for division of barbed suture tails causing obstruction [24]. Most cases were resolved with truncation/removal of the implicated barbed suture tail (63%). However, two cases required additional small bowel resection secondary to ischaemia at the time of operation, once again highlighting the need for prompt recognition of patient symptoms, review of imaging, review of operative notes for barbed sutures and expedition to a diagnostic laparoscopy if there are concerns.
A study conducted by Bosma et al. demonstrated that patients who suffer severe complications Clavien–Dindo (CD) (III, IV and V), such as return to theatre (III), have a more pronounced decrease in overall quality of life in both physical and psychological domains, which may last for a further six weeks post operatively [34]. A study investigating the correlation between CD complication grade and severity identified a strong correlation between CD grade and increased direct medical cost during the first 90 days after surgery [35]. Data regarding costs specific to our area of interest were scarce. However, a systematic review incorporating data from Europe, the USA, New Zealand and Nigeria on patients who present with small bowel obstructions secondary to post operative adhesions requiring surgical management was reported to range between $4914 and $25,321 AUD for patients with a median length of stay of 4 days [36]. We found the average length of stay during patient re-admission to be 6 days (median 4 days), with a range from 2 to 18 days (Table 1), inferring a similar cost range to the healthcare system for the patients re-admitted with small bowel obstructions secondary to barbed sutures [37]. This further supports the need for prompt recognition of patient presentation and early intervention as well as learning strategies to prevent the rate of occurrence of the complication.
4.3. Practical Solutions to Prevent SBOs Secondary to Barbed Sutures
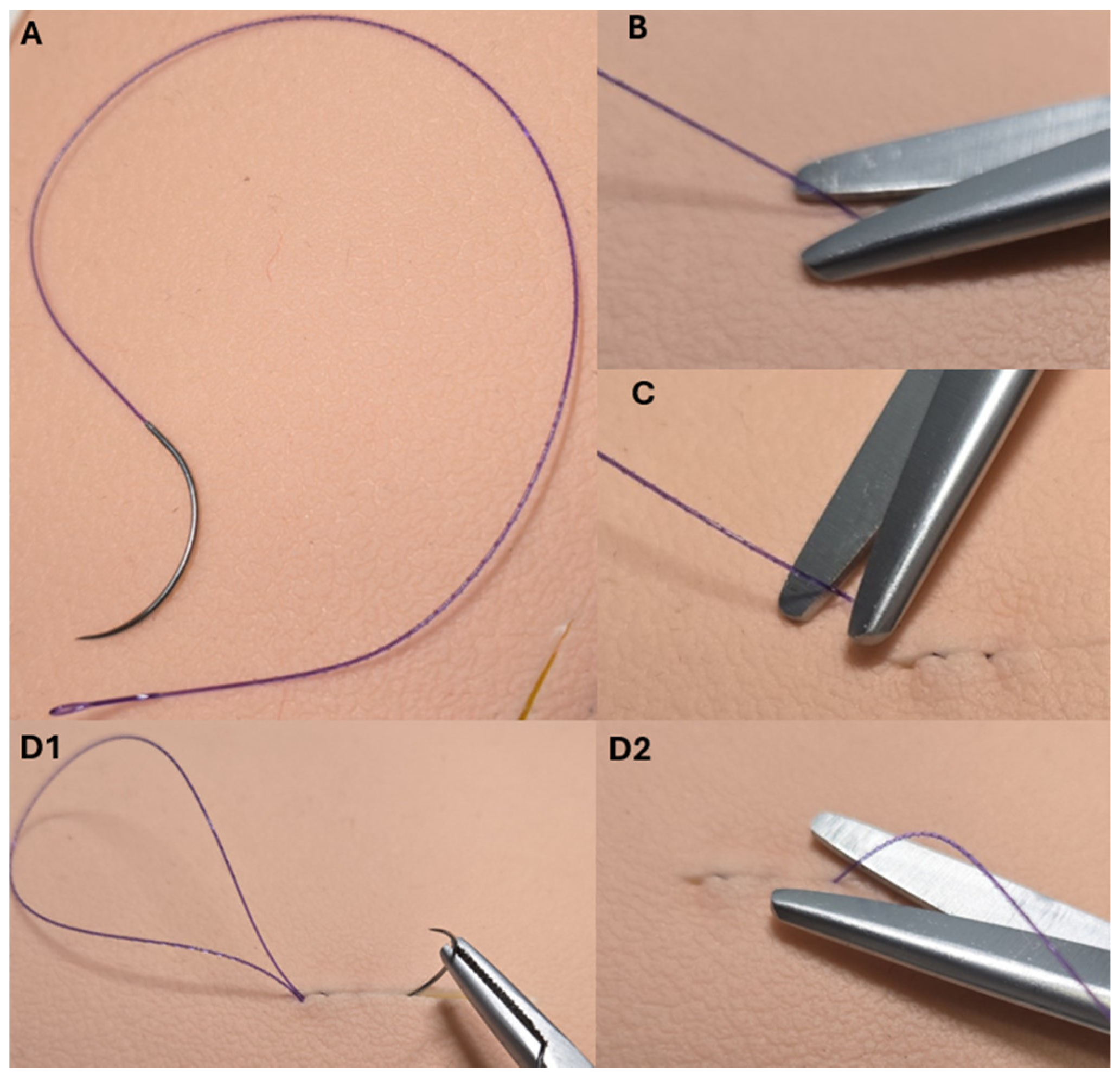
Current recommendations in the literature advise that the risk of SBOs secondary to barbed suture use can be reduced by ensuring the tail of the suture is cut as short as possible. Barbed sutures (Figure 3A) are capable of grasping surrounding tissues, and their product insert recommends cutting the suture flush with the peritoneum (Figure 4B) [38]. The instructions for StratafxTM also suggest suturing one to two stitches back along the suture line, and then cutting the suture flush (Figure 4D1,D2) [39]. We suggest that one buried suture away from the midline prior to cutting flush may also be a useful strategy (Figure 4C).
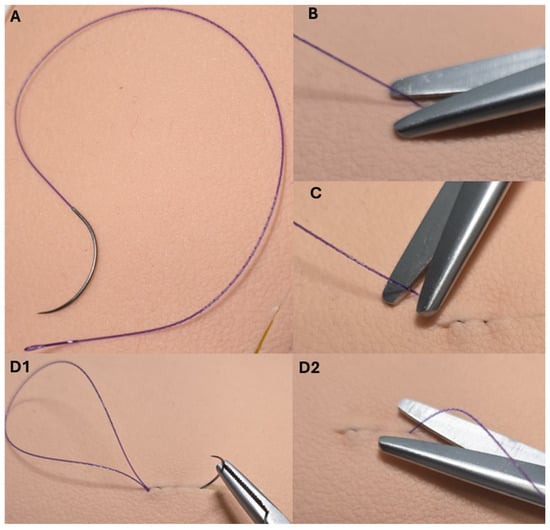
Figure 4.
Practical suture line finishing techniques to minimise small bowel obstructions secondary to entanglement in barbed suture tails. (A) 3-0 V-LocTM (CovidienTM, Mansfield, MA, USA); (B) recommendation to cut the suture flush with the wound; (C) alternative recommendation to place a final suture to the side of the wound and then to cut flush; and (D1) recommendation to suture one to two stitches back along the suture line and then to cut flush (D2).
Alternatively, some studies advocate for the use of adhesion barriers to avoid direct bowel contact with the barbed suture [2]. Anti-adhesive material (INTERCEED®; Johnson & Johnson, New Brunswick, NJ, USA) can be applied to the peritoneal closure line and the trimmed tail of V-LocTM [22]. Others propose a cellulose sheath such as Surgicel [40] or a laparoscopic clip such as the LAPRA-TY® device [2] be applied to the tail of the barbed suture to offer additional cover.
Stabile et al. recommended in procedures requiring two layers of sutures, e.g., uterine myomectomies, that only the first layer be closed with a barbed suture, and the second superficial layer be closed with a monofilament [33]. The safest course is to continue to use a classic suture whenever repair of the serosa or peritoneum is required [33]. Future prospective studies investigating which technique is best for preventing these catastrophic complications are needed.
Potential future directions include encouragement of case reporting globally so that the true extent of the impact of barbed sutures in robotic surgery can be evaluated. Prospective trials to assess the ideal operative technique/suture placement of barbed sutures to decrease the rate of SBOs should be conducted and adopted for patient safety. Finally, further research into non-adhesive materials, which may be used to evolve the barbed suture or its tail, should be conducted.
4.4. Limitations of the Study
This is the largest review published to date regarding the incidence of SBO secondary to barbed suture use in robotic surgery. Due to the novelty of robotic surgery and its use of barbed sutures, the search yielded only seven articles after our exclusion criterion of articles not published in English was applied. The exclusion of studies not published in English introduced a language bias. The inclusion of further analysis including standard deviation, etc., would have produced an overestimation in such a small sample size. Thus, we only reported the mean and median values, definitive conclusions cannot be drawn and further research is required before the significance of our results and proposed strategies for prevention can be applied to the general population.
Of the seven articles, one was a case series, and the others were case reports, which are identified as level 5 evidence. Thus, this review may also be subject to reporting as incidence rates of complication are subject to surgeons in practice publishing the complications they encounter. However, awareness of the complication to facilitate discussion about features for early recognition and prompt intervention is imperative to prevent severe complications in patients. Furthermore, education on strategies to reduce the incidence is imperative for improved future patient outcomes.
5. Conclusions
Barbed sutures have a role in expediting intraoperative time, reducing hospital length of stay and haemostasis in robotic surgery. However, due to their adhesive properties, the risk of small bowel obstruction remains. Surgeons should have a high index of suspicion for mechanical small bowel obstruction after any surgery in which a barbed suture has been utilised. These presentations will require prompt operative exploration, with laparoscopy and truncation of the barbed suture tail being successful in most cases. Furthermore, surgeons should implore techniques, such as burying the barbed suture and cutting it flush, to minimise the rate of occurrence, minimise future complications and reduce healthcare costs. Further research involving prospective investigation of new materials and operative techniques to improve the safety and efficacy of barbed sutures is needed.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
The data presented in this study are available through PubMed, Cochrane and Ovoid Medline Databases.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Beckmann, J.H.; Kersebaum, J.-N.; von Schönfels, W.; Becker, T.; Schafmayer, C.; Egberts, J.H. Use of barbed sutures in robotic bariatric bypass surgery: A single-center case series. BMC Surg. 2019, 19, 97. [Google Scholar] [CrossRef] [PubMed]
- Stabile, G.; Romano, F.; De Santo, D.; Sorrentino, F.; Nappi, L.; Cracco, F.; Ricci, G. Case Report: Bowel Occlusion Following the Use of Barbed Sutures in Abdominal Surgery. A Single-Center Experience and Literature Review. Front. Surg. 2021, 8, 626505. [Google Scholar] [CrossRef]
- Fouda, U.M.; Elsetohy, K.A.; Elshaer, H.S. Barbed Versus Conventional Suture: A Randomized Trial for Suturing the Endometrioma Bed After Laparoscopic Excision of Ovarian Endometrioma. J. Minim. Invasive Gynecol. 2016, 23, 962–968. [Google Scholar] [CrossRef]
- Hafermann, J.; Silas, U.; Saunders, R. Efficacy and safety of V-LocTM barbed sutures versus conventional suture techniques in gynecological surgery: A systematic review and meta-analysis. Arch. Gynecol. Obstet. 2024, 309, 1249–1265. [Google Scholar] [CrossRef]
- Angioli, R.; Plotti, F.; Montera, R.; Damiani, P.; Terranova, C.; Oronzi, I.; Luvero, D.; Scaletta, G.; Muzii, L.; Panici, P.B. A new type of absorbable barbed suture for use in laparoscopic myomectomy. Int. J. Gynaecol. Obstet. 2012, 117, 220–223. [Google Scholar] [CrossRef]
- Mikhail, E.; Wyman, A.; Hahn, L.; Hart, S. Barbed Sutures in Minimally Invasive Gynecologic Surgery. Surg. Technol. Int. 2016, 28, 185–191. [Google Scholar]
- Uccella, S.; Ceccaroni, M.; Cromi, A.; Malzoni, M.; Berretta, R.; De Iaco, P.; Roviglione, G.; Bogani, G.; Minelli, L.; Ghezzi, F. Vaginal cuff dehiscence in a series of 12,398 hysterectomies: Effect of different types of colpotomy and vaginal closure. Obstet. Gynecol. 2012, 120, 516–523. [Google Scholar] [CrossRef] [PubMed]
- Takayama, S.; Nakai, N.; Shiozaki, M.; Ogawa, R.; Sakamoto, M.; Takeyama, H. Use of barbed suture for peritoneal closure in transabdominal preperitoneal hernia repair. World J. Gastrointest. Surg. 2012, 4, 177–179. [Google Scholar] [CrossRef] [PubMed]
- Yokoyama, K.; Tanigawa, N.; Ogata, A.; Nagai, T.; Higashino, M. Laparoscopic Technique and Initial Experiences of Choledocholithotomy Closure With Knotless Unidirectional Barbed Sutures After Surgery for Biliary Stone Disease. Surg. Laparosc. Endosc. Percutaneous Tech. 2015, 25, e129–e133. [Google Scholar] [CrossRef]
- Vidarsson, B.; Sundbom, M.; Edholm, D. Shorter overall operative time when barbed suture is used in primary laparoscopic gastric bypass: A cohort study of 25,006 cases. Surg. Obes. Relat. Dis. 2017, 13, 1484–1488. [Google Scholar] [CrossRef]
- Clapp, B.; Klingsporn, W.; Lodeiro, C.; Wicker, E.; Christensen, L.; Jones, R.; Tyroch, A. Small bowel obstructions following the use of barbed suture: A review of the literature and analysis of the MAUDE database. Surg. Endosc. 2020, 34, 1261–1269. [Google Scholar] [CrossRef]
- Segura-Sampedro, J.J.; Ashrafian, H.; Navarro-Sánchez, A.; Jenkins, J.T.; Morales-Conde, S.; Martínez-Isla, A. Small bowel obstruction due to laparoscopic barbed sutures: An unknown complication? Rev. Esp. Enfermedades Dig. 2015, 107, 677–680. [Google Scholar] [CrossRef]
- Picozzi, P.; Nocco, U.; Labate, C.; Gambini, I.; Puleo, G.; Silvi, F.; Pezzillo, A.; Mantione, R.; Cimolin, V. Advances in Robotic Surgery: A Review of New Surgical Platforms. Electronics 2024, 13, 4675. [Google Scholar] [CrossRef]
- Nawfal, A.K.; Eisenstein, D.; Theoharis, E.; Dahlman, M.; Wegienka, G. Vaginal cuff closure during robotic-assisted total laparoscopic hysterectomy: Comparing vicryl to barbed sutures. J. Soc. Laparoendosc. Surg. 2012, 16, 525–529. [Google Scholar] [CrossRef] [PubMed]
- Kakiashvili, E.; Bez, M.; Abu Shakra, I.; Ganam, S.; Bickel, A.; Merei, F.; Drobot, A.; Bogouslavski, G.; Kassis, W.; Khatib, K.; et al. Robotic inguinal hernia repair: Is it a new era in the management of inguinal hernia? Asian J. Surg. 2021, 44, 93–98. [Google Scholar] [CrossRef] [PubMed]
- Chapman, S.; Turo, R.; Cross, W. Vesicourethral anastomosis using V-LocTM barbed suture during robot-assisted radical prostatectomy. Cent. Eur. J. Urol. 2011, 64, 236. [Google Scholar] [CrossRef]
- Zhou, Y.; Guthrie, G.; Chuang, A.; Faro, J.P.; Ali, V. Unidirectional barbed suture versus interrupted vicryl suture in vaginal cuff healing during robotic-assisted laparoscopic hysterectomy. J. Robot. Surg. 2014, 8, 201–205. [Google Scholar] [CrossRef]
- Nambi Gowri, K.; King, M.W. A Review of Barbed Sutures-Evolution, Applications and Clinical Significance. Bioengineering 2023, 10, 419. [Google Scholar] [CrossRef]
- Pajtak, R.; Ibraheem, C.; Mori, K. Catastrophic complications of a robot-assisted laparoscopic sacrocolpopexy with a barbed suture: Ischaemic bowel. J. Surg. Case Rep. 2024, 2024, rjae145. [Google Scholar] [CrossRef]
- Yajima, S.; Nakanishi, Y.; Matsumoto, S.; Ookubo, N.; Tanabe, K.; Masuda, H. Strangulated ileus from barbed suture following robot-assisted radical cystectomy: A case report. Urol. Case Rep. 2022, 40, 101916. [Google Scholar] [CrossRef]
- Vahanian, S.A.; Finamore, P.S.; Lazarou, G. Delayed small bowel obstruction after robotic-assisted sacrocolpopexy. Female Pelvic Med. Reconstr. Surg. 2015, 21, e11–e13. [Google Scholar] [CrossRef]
- Takagi, H.; Wada, N.; Morishita, S.; Ohtani, M.; Kitta, T.; Kakizaki, H.; Kohro, D.; Shonaka, T. Postoperative small intestinal obstruction caused by barbed suture after robot-assisted laparoscopic sacrocolpopexy. IJU Case Rep. 2024, 7, 105–109. [Google Scholar] [CrossRef]
- Khan, F.A.; Hashmi, A.; Edelman, D.A. Small bowel obstruction caused by self-anchoring suture used for peritoneal closure following robotic inguinal hernia repair. J. Surg. Case Rep. 2016, 2016, rjw117. [Google Scholar] [CrossRef] [PubMed]
- Gee, K.N.; Many, H.R.; Foulke, E.; Smith, L.M. Early Post-operative Mechanical Small Bowel Obstruction Induced by Unidirectional Barbed Suture. Am. Surg. 2023, 89, 3937–3938. [Google Scholar] [CrossRef] [PubMed]
- Mourad, M.; Avedikian, J.; Kim, J.; Haskins, I.; Kothari, V. A295 Beware the Barbs! A Rare Case of Early Small Bowel Obstruction Due to Barbed Suture After Roux-en-Y Gastric Bypass. Surg. Obes. Relat. Dis. 2024, 20, S93. [Google Scholar] [CrossRef]
- Shin, S.-J.; Chung, H.; Kwon, S.-H.; Cha, S.-D.; Cho, C.-H. New suturing technique for robotic-assisted vaginal cuff closure during single-site hysterectomy. J. Robot. Surg. 2017, 11, 139–143. [Google Scholar] [CrossRef]
- Alessandri, F.; Remorgida, V.; Venturini, P.L.; Ferrero, S. Unidirectional Barbed Suture versus Continuous Suture with Intracorporeal Knots in Laparoscopic Myomectomy: A Randomized Study. J. Minim. Invasive Gynecol. 2010, 17, 725–729. [Google Scholar] [CrossRef]
- Ward, H.; Hosseini, O.; Taylor, B.R.; Opoku, K.; Dharmarpandi, J.; Dharmarpandi, G.; Obokhare, I. The Effect of Barbed Sutures on Complication Rates Post Colectomy: A Retrospective Case-Matched Review. Cureus 2022, 14, e29484. [Google Scholar] [CrossRef]
- Bertolo, R.; Campi, R.; Klatte, T.; Kriegmair, M.C.; Mir, M.C.; Ouzaid, I.; Salagierski, M.; Bhayani, S.; Gill, I.; Kaouk, J.; et al. Suture techniques during laparoscopic and robot-assisted partial nephrectomy: A systematic review and quantitative synthesis of peri-operative outcomes. BJU Int. 2019, 123, 923–946. [Google Scholar] [CrossRef]
- Johnson, B.H.; Sinchana, T.; Johnston, S.S.; Gunja, N. Trends in adoption of knotless tissue control devices in robotic surgery. J. Comp. Eff. Res. 2025, 14, e240229. [Google Scholar] [CrossRef]
- Oor, J.; de Castro, S.; van Wagensveld, B. V-locTM capable of grasping surrounding tissue causes obstruction at the jejunojejunostomy after Roux-en-Y laparoscopic gastric bypass. Asian J. Endosc. Surg. 2015, 8, 209–211. [Google Scholar] [CrossRef]
- Thubert, T.; Pourcher, G.; Deffieux, X. Small bowel volvulus following peritoneal closure using absorbable knotless device during laparoscopic sacral colpopexy. Int. Urogynecol. J. 2011, 22, 761–763. [Google Scholar] [CrossRef] [PubMed]
- Stabile, G.; Vona, L.; Carlucci, S.; Nappi, L. Small bowel obstruction secondary to barbed sutures: A few more tricks to have fewer complications. ANZ J. Surg. 2024, 95, 264. [Google Scholar] [CrossRef] [PubMed]
- Bosma, E.; Pullens, M.J.; de Vries, J.; Roukema, J.A. The impact of complications on quality of life following colorectal surgery: A prospective cohort study to evaluate the Clavien-Dindo classification system. Color. Dis. 2016, 18, 594–602. [Google Scholar] [CrossRef] [PubMed]
- Widmar, M.; Keskin, M.; Strombom, P.D.; Gennarelli, R.L.; Szeglin, B.C.; Smith, J.J.; Nash, G.M.; Weiser, M.R.; Paty, P.B.; Russell, D.; et al. Evaluating the Validity of the Clavien-Dindo Classification in Colectomy Studies: A 90-Day Cost of Care Analysis. Dis. Colon Rectum 2021, 64, 1426–1434. [Google Scholar] [CrossRef]
- Garoufalia, Z.; Gefen, R.; Emile, S.H.; Zhou, P.; Silva-Alvarenga, E.; Wexner, S.D. Financial and Inpatient Burden of Adhesion-Related Small Bowel Obstruction: A Systematic Review of the Literature. Am. Surg. 2023, 89, 2693–2700. [Google Scholar] [CrossRef]
- Oyasiji, T.; Angelo, S.; Kyriakides, T.C.; Helton, S.W. Small Bowel Obstruction: Outcome and Cost Implications of Admitting Service. Am. Surg. 2010, 76, 687–691. [Google Scholar] [CrossRef]
- Filser, J.; Reibetanz, J.; Krajinovic, K.; Germer, C.-T.; Dietz, U.A.; Seyfried, F. Small bowel volvulus after transabdominal preperitoneal hernia repair due to improper use of V-LocTM barbed absorbable wire—Do we always “read the instructions first”? Int. J. Surg. Case Rep. 2015, 8, 193–195. [Google Scholar] [CrossRef]
- MedTech, J.J. STRATAFIX Sprial Knotless Tissue Control Devices. Availabe online: https://www.jnjmedtech.com/en-US/product/stratafix-spiral-knotless-tissue-control-device (accessed on 10 November 2024).
- Bassi, A.; Tulandi, T. Evaluation of total laparoscopic hysterectomy with and without the use of barbed suture. J. Obstet. Gynaecol. Can. 2013, 35, 718–722. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).