
Low-Dose Aspirin for Preterm Birth Prevention in Low- and Middle-Income Countries: A Systematic Review and Meta-Analysis


Abstract
1. Introduction
2. Materials and Methods
2.1. Information Sources and Search Strategies
2.2. Eligibility Criteria and Data Extraction
2.3. Risk of Bias Assessment
2.4. Statistical Analysis
3. Results
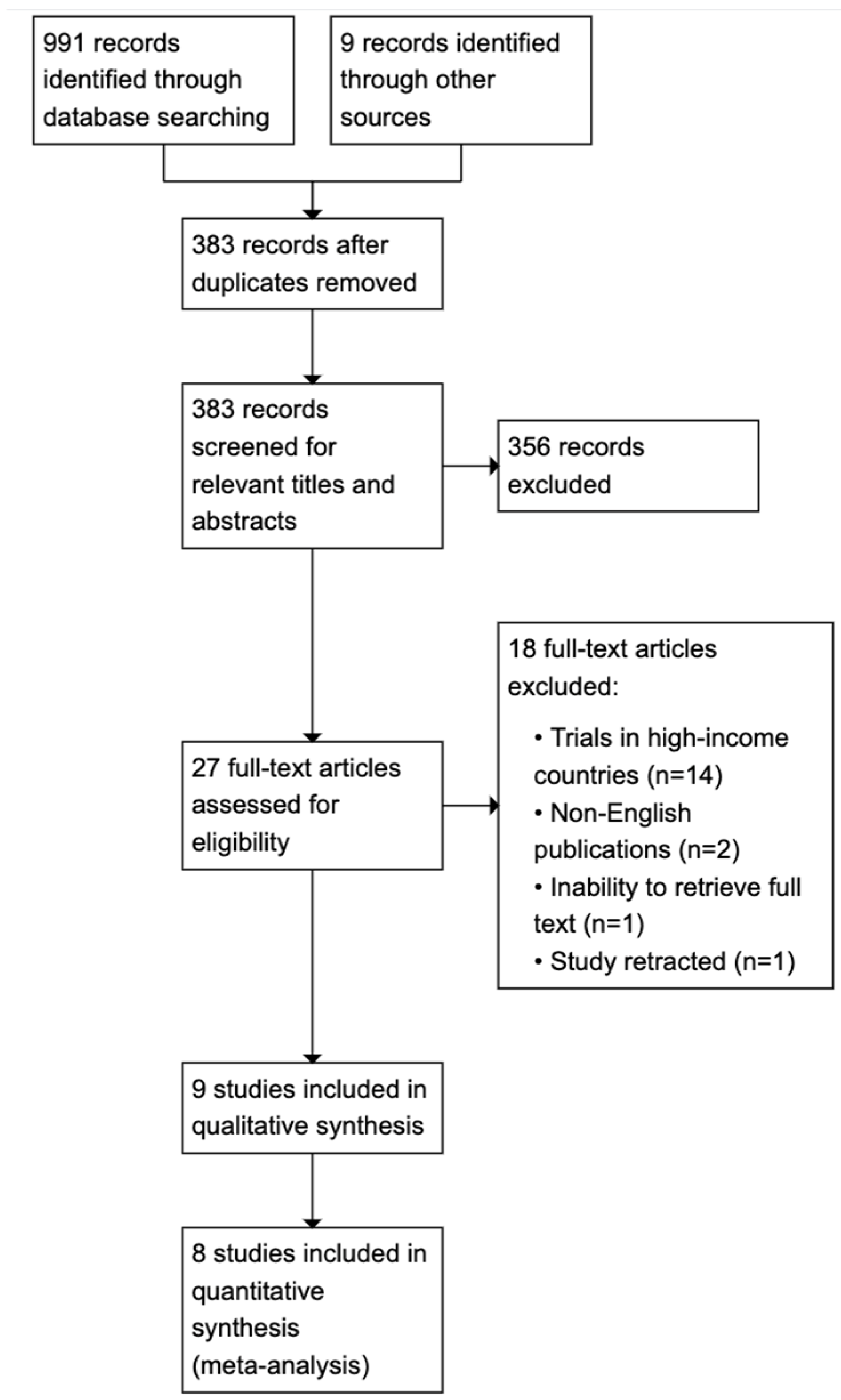
3.1. Search Process and Study Selection
3.2. Study Characteristics
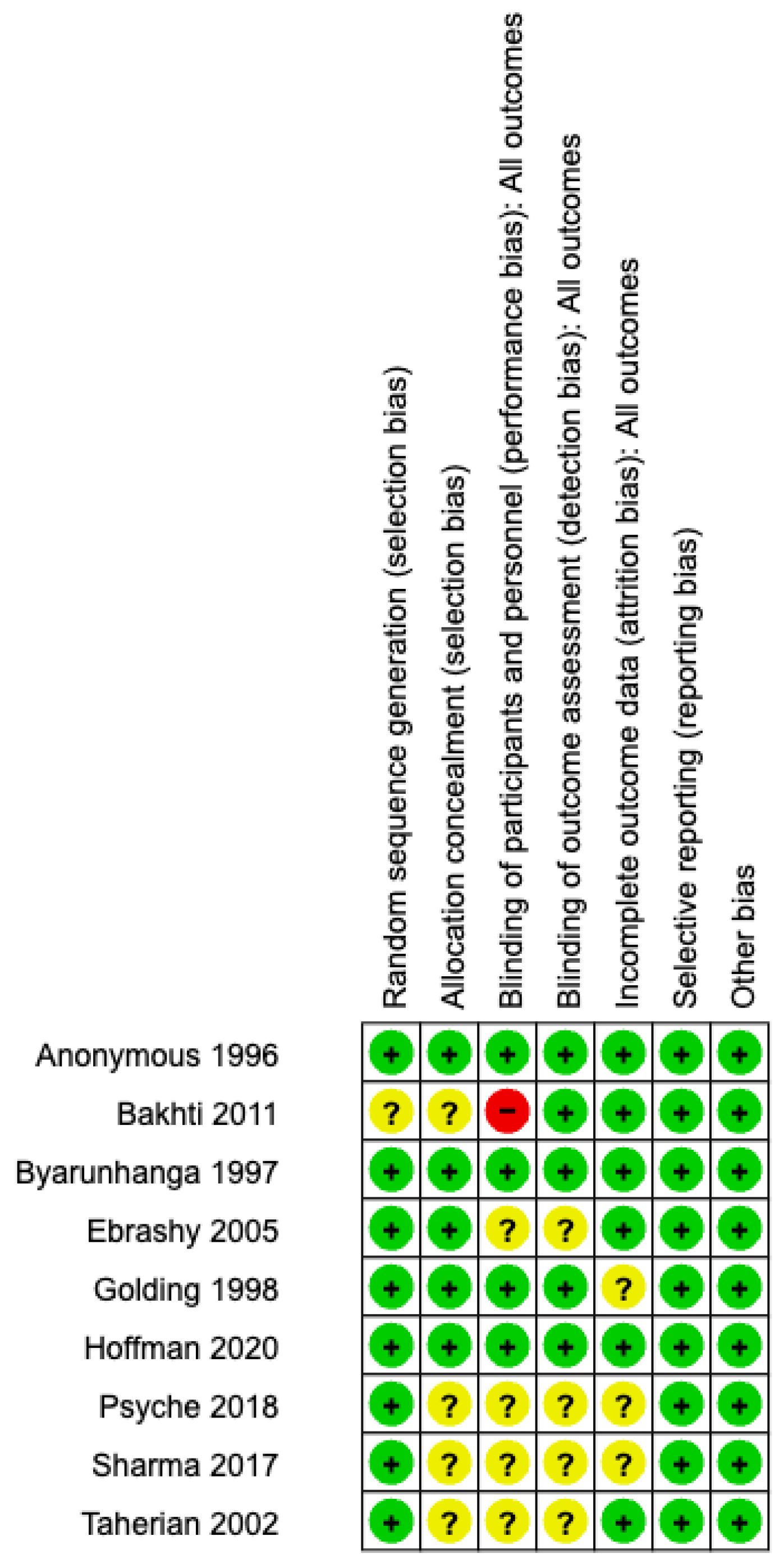
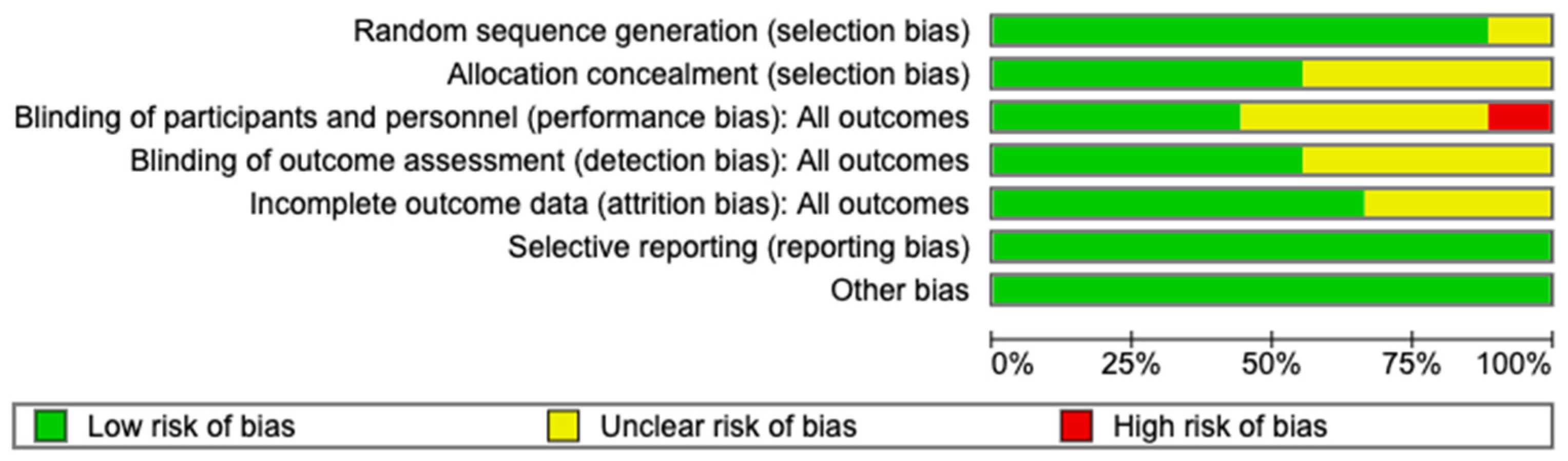
3.3. Risk of Bias Within Studies
3.4. Results of Individual Studies
3.5. Results of Synthesis
3.5.1. Primary Outcome
- ◆
- Preterm birth
3.5.2. Secondary Outcomes
- Low birthweight
- Perinatal mortality
- Antepartum hemorrhage
- Postpartum hemorrhage
3.6. Publication Bias and Quality of Evidence
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| EMBASE via Ovid–last searched 13 July 2023 @ 13:40 hrs. | ||
| Number | Searches | Results |
| 1 | exp acetylsalicylic acid/ | 209,695 |
| 2 | aspirin.tw. | 115,744 |
| 3 | asa.tw. | 47,971 |
| 4 | acetylsalicylic acid.tw. | 12,253 |
| 5 | acetylsalicylate.tw | 705 |
| 6 | antiplatelet agent.tw. | 2457 |
| 7 | 1 or 2 or 3 or 4 or 5 or 6 | 260,739 |
| 8 | exp premature labor/co, dm, dt, pc, th [complication, disease management, drug therapy, prevention therapy] | 7899 |
| 9 | prematur*.tw. | 189,215 |
| 10 | preterm birth.tw. | 24,283 |
| 11 | preterm delivery.tw. | 14,798 |
| 12 | (early labour or early labor).tw. | 729 |
| 13 | early delivery.tw. | 909 |
| 14 | 8 or 9 or 10 or 11 or 12 or 13 | 223,264 |
| 15 | randomized controlled trials/ | 181,727 |
| 16 | random$.mp. | 1,769,188 |
| 17 | controlled clinical trials/ | 10,828 |
| 18 | 15 or 16 or 17 | 1,774,717 |
| 19 | 7 and 14 and 18 | 473 |
| 20 | limit 19 to (human and english language) | 434 |
| MEDLINE via Ovid–last searched 3 July 2023 @ 12:28 hrs. | ||
| 1 | exp Premature Birth | 13,934 |
| 2 | Premature birth.tw. | 2801 |
| 3 | Exp Obstetric Labor, Premature/ | 26,461 |
| 4 | (premature labour or premature labor).tw. | 2824 |
| 5 | Prematur*.tw. | 130,587 |
| 6 | exp Infant, Premature/ | 56,053 |
| 7 | premature delivery.tw. | 2415 |
| 8 | preterm birth.tw. | 13,975 |
| 9 | (early labour or early labor).tw. | 503 |
| 10 | early delivery.tw. | 536 |
| 11 | 1 or 2 or 3 or 4 or 5 or 6 or 7 or 8 or 9 or 10 | 183,708 |
| 12 | exp Aspirin/ | 44,985 |
| 13 | aspirin.tw. | 43,625 |
| 14 | acetylsalicylic acid.tw. | 8308 |
| 15 | antiplatelet therapy.tw. | 9167 |
| 16 | ASA.tw. | 22,425 |
| 17 | 12 or 13 or 14 or 15 or 16 | 87,918 |
| 18 | Randomized Controlled Trials/ | 135,465 |
| 19 | Randomized Controlled Trial.pt. | 511,314 |
| 20 | controlled clinical trial.pt. | 93,789 |
| 21 | 18 or 19 or 20 | 729,828 |
| 22 | 11 and 17 and 21 | 192 |
| 23 | limit 22 to (english language and humans) | 183 |
| CENTRAL via Cochrane Library—last searched 8 July 2023 @ 18:37 hrs. | ||
| ||
| ||
| ||
| ||
| ||
| ||
| ||
| ||
| ||
| Author (Year) | Country | Study Design | Participant Assignment | Population | Intervention | Comparator | Outcomes Reported | |
|---|---|---|---|---|---|---|---|---|
| LDA | Placebo | |||||||
| Anonymous (1996) [25] | Brazil | RCT | 498 | 511 | Women between 12 and 32 weeks of gestation with chronic HTN, primigravidity, DM, renal disease, history of PEC or IUGR | 60 mg ASA daily until delivery | Placebo | Proteinuric PEC, preterm delivery, IUGR, stillbirths and neonatal deaths, BW, delivery type. Bleeding, fetal loss |
| Byaruhanga et al. (1997) [26] | Zimbabwe | RCT | 125 | 125 | Women between 20 and 28 weeks of gestation, previous history of PIH, PEC or eclampsia, chronic HTN | 75 mg ASA daily until 38 weeks of gestation | Placebo | Pre-eclampsia, pregnancy duration, BW and perinatal deaths, type of delivery, outcome of pregnancy, post-dates, blood loss |
| Golding (1998) [27] | Jamaica | RCT | 3023 | 3026 | Primiparae between 12 and 32 weeks of gestation | 60 mg ASA until delivery | Placebo | Proteinuria, proteinuric PEC, eclampsia, edema at delivery, onset of labor, type of delivery, GA at delivery, BW, perinatal death, 5-min APGAR, baby admitted to SCBU, maternal bleeding, wheezing or asthma, stomach pains, skin rash |
| Taherian et al. (2002) [28] | Iran | RCT | 330 | 330 | Nulliparity, single gestation, first prenatal visit before 20 weeks of gestation, BP < 130/80, no proteinuria on urine dipstick | 75 mg ASA daily until delivery | No treatment | PEC, BP, BW, IUGR, preterm delivery, fetal and newborn morbidity (anomaly, RDS, sepsis, jaundice, death) |
| Ebrashy et al. (2005) [29] | Egypt | RCT | 74 | 65 | Women between 14 and 16 weeks of gestation, high risk for PEC or IUGR | 75 mg ASA daily until 37 weeks of gestation | No treatment | PEC, IUGR, preterm delivery, 1-min and 5-min APGAR, maternal and neonatal bleeding |
| Bakhti et al. (2011) [30] | Algeria | RCT | 82 | 82 | Primigravid women consulting before 10th week of amenorrhea without previous vasculo-renal pathology | 100 mg ASA until 36 weeks of gestation | No treatment | Gravidic hypertensive disorders, BW, gestational age at delivery, prematurity, perinatal mortality |
| Sharma et al. (2017) [31] | India | RCT | 34 | 31 | Women between 12 and 20 weeks of gestation, age > 34 years, chronic HTN, twins gestation, gestational diabetes, previous PEC, high uterine artery pulsatility index | 75 mg ASA until 34 weeks of gestation | Placebo | PEC, PPH, abruption placentae, preterm delivery, IUGR |
| Psyche et al. (2018) [32] | India | RCT | 1300 | 1300 | Women between 13 and 24 weeks of gestation with high-risk of PEC (pregestational insulin-treated DM, chronic HTN, multifetal gestations, history of PEC) | 75 mg ASA until delivery | Placebo | PEC, PPH, abruptio placentae, preterm delivery, SGA, perinatal death, neonatal IVH |
| Hoffman et al. (2020) [18] | Congo, Zambia, India etc. | RCT | 5787 | 5771 | Nulliparous pregnant women between 18 and 40 years, gestational age between 6 weeks + 0 days and 13 weeks + 6 days by USG. | 81 mg ASA daily until delivery or 36 weeks + 7 days of gestation | Placebo | Preterm birth, maternal morbidities (hypertensive disorders, PPH, APH etc.), fetal morbidities (SGA, perinatal mortality, BW etc.) |
| Study ID | PREGNANCY OUTCOMES | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Pre-Term birth | Low-Birth weight | Perinatal Mortality | Antepartum Hemorrhage | Post-Partum Hemorrhage | |||||||||||
| IG | CG | RR [95% CI; p] | IG | CG | RR [95% CI; p] | IG | CG | RR [95% CI; p] | IG | CG | RR [95% CI; p] | IG | CG | RR [95% CI; p] | |
| +(n) | +(n) | +(n) | +(n) | +(n) | +(n) | +(n) | +(n) | +(n) | +(n) | ||||||
| Anonymous 1996 [25] | 106 (476) | 129 (494) | 0.85 [0.68–1.07; 0.16] | NR | NR | - | NR | NR | - | 11 (476) | 15 (494) | 0.76 [0.35–1.64; 0.49] | 3 (476) | 6 (494) | 0.52 [0.13–2.06; 0.35] |
| Bakhti 2011 [30] | 34 (84) | 75 (84) | 0.45 [0.35–0.59; 0.00] * | 0 (84) | 1 (84) | 0.33 [0.01–8.07; 0.50] | 0 (84) | 7 (84) | 0.07 [0.00–1.15; 0.06] | NR | NR | - | NR | NR | - |
| Byaruhanga 1997 [26] | 21 (113) | 30 (117) | 0.72 [0.44–1.19; 0.20] | NR | NR | - | 5 (114) | 13 (122) | 0.41 [0.15–1.12; 0.08] | NR | NR | - | 11 (113) | 10 (117) | 1.04 [0.46–2.35; 0.92] |
| Ebrashy 2005 [29] | 3 (74) | 9 (65) | 0.29 [0.08–1.04; 0.06] | NR | NR | - | NR | NR | - | NR | NR | - | NR | NR | - |
| Golding 1998 [27] | 447 (3023) | 463 (3026) | 0.97 [0.86–1.09; 0.58] | 303 (3023) | 325 (3026) | 0.93 [0.80–1.08; 0.36] | 86 (3023) | 103 (3026) | 0.84 [0.63–1.10; 0.21] | 75 (3023) | 67 (3026) | 1.12 [0.81–1.55; 0.49] | 213 (3023) | 135 (3026) | 1.58 [1.28–1.95; 0.00] * |
| Hoffman 2020 [18] | 668 (5780) | 754 (5764) | 0.89 [0.80–0.99; 0.02] * | 1078 (5628) | 1153 (5624) | 0.93 [0.87–1.01; 0.07] | 264 (5779) | 309 (5763) | 0.86 [0.73–1.00; 0.05] | 26 (5761) | 25 (5746) | 1.03 [0.60–1.79; 0.90] | 54 (5928) | 43 (5907) | 1.25 [0.84–1.86; 0.27] |
| Psyche 2018 [32] | 390 (1300) | 429 (1300) | 0.91 [0.81–1.01; 0.10] | NR | NR | - | 39 (1300) | 52 (1300) | 0.75 [0.50–1.13; 0.17] | 26 (1300) | 39 (1300) | 0.67 [0.41–1.09; 0.11] | 104 (1300) | 104 (1300) | 1.00 [0.78–1.30; 1.00] |
| Sharma 2017 [31] | 31 (97) | 34 (92) | 0.86 [0.58–1.28; 0.47] | NR | NR | - | NR | NR | - | 1 (97) | 2 (92) | 0.47 [0.04–5.14; 0.54] | 4 (97) | 5 (92) | 0.76 [0.21–2.74; 0.67] |
| Taherian 2002 [28] | 39 (330) | 29 (330) | 1.34 [0.85–2.12; 0.20] | NR | NR | - | NR | NR | - | NR | NR | - | NR | NR | - |
| Summary of Findings: | ||||||
|---|---|---|---|---|---|---|
| Low-dose aspirin compared to placebo for preterm birth prevention | ||||||
| Patient or population: preterm birth prevention Setting: LMICs Intervention: Low-dose aspirin Comparison: placebo | ||||||
| Outcomes | Anticipated absolute effects * (95% CI) | Relative effect (95% CI) | № of participants (studies) | Certainty of the evidence (GRADE) | Comments | |
| Risk with placebo | Risk with Low-dose aspirin | |||||
| Preterm birth | 168 per 1000 | 151 per 1000 (138 to 164) | RR 0.90 (0.82 to 0.98) | 22,381 (8 RCTs) | ⨁⨁◯◯ Low a,b,c | |
| Low birthweight | 171 per 1000 | 159 per 1000 (149 to 171) | RR 0.93 (0.87 to 1.00) | 17,301 (2 RCTs) | ⨁⨁⨁◯ Moderate d | |
| Perinatal mortality | 47 per 1000 | 39 per 1000 (34 to 44) | RR 0.83 (0.73 to 0.94) | 20,427 (4 RCTs) | ⨁⨁⨁⨁ High | |
| Antepartum hemorrhage | 14 per 1000 | 13 per 1000 (10 to 16) | RR 0.91 (0.70 to 1.18) | 21,315 (5 RCTs) | ⨁⨁◯◯ Low e | |
| Post-partum hemorrhage | 28 per 1000 | 29 per 1000 (21 to 40) | RR 1.05 (0.77 to 1.43) | 21,873 (6 RCTs) | ⨁⨁◯◯ Low f,g | |
| * The risk in the intervention group (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: confidence interval; RR: risk ratio | ||||||
| GRADE working group grades of evidence High certainty: We are very confident that the true effect lies close to that of the estimate of the effect. Moderate certainty: We are moderately confident in the effect estimate: the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different. Low certainty: Our confidence in the effect estimate is limited: the true effect may be substantially different from the estimate of the effect. Very low certainty: We have very little confidence in the effect estimate: the true effect is likely to be substantially different from the estimate of effect. | ||||||
References
- Preterm Birth. Available online: https://www.who.int/news-room/fact-sheets/detail/preterm-birth (accessed on 12 October 2023).
- Chawanpaiboon, S.; Vogel, J.P.; Moller, A.-B.; Lumbiganon, P.; Petzold, M.; Hogan, D.; Landoulsi, S.; Jampathong, N.; Kongwattanakul, K.; Laopaiboon, M.; et al. Global, regional, and national estimates of levels of preterm birth in 2014: A systematic review and modelling analysis. Lancet Glob. Health 2019, 7, e37–e46. [Google Scholar] [CrossRef]
- Kleinhout, M.Y.; Stevens, M.M.; Osman, K.A.; Adu-Bonsaffoh, K.; Groenendaal, F.; Zepro, N.B.; Rijken, M.J.; Browne, J.L. Evidence-based interventions to reduce mortality among preterm and low-birthweight neonates in low-income and middle-income countries: A systematic review and meta-analysis. BMJ Glob. Health 2021, 6, e003618. [Google Scholar] [CrossRef] [PubMed]
- Laelago, T.; Yohannes, T.; Tsige, G. Determinants of preterm birth among mothers who gave birth in East Africa: Systematic review and meta-analysis. Ital. J. Pediatr. 2020, 46, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Respiratory Morbidity in Late Preterm Births. Available online: www.jama.com (accessed on 25 August 2023).
- Patel, R.M. Short and Long-Term Outcomes for Extremely Preterm Infants. Am. J. Perinatol. 2016, 33, 318. [Google Scholar] [CrossRef] [PubMed]
- Camerota, M.; Graw, S.; Everson, T.M.; McGowan, E.C.; Hofheimer, J.A.; O’shea, T.M.; Carter, B.S.; Helderman, J.B.; Check, J.; Neal, C.R.; et al. Prenatal risk factors and neonatal DNA methylation in very preterm infants. Clin. Epigenetics 2021, 13, 171. [Google Scholar] [CrossRef]
- Mangham, L.J.; Petrou, S.; Doyle, L.W.; Draper, E.S.; Marlow, N. The cost of preterm birth throughout childhood in England and Wales. Pediatrics 2009, 123, e312–e327. [Google Scholar] [CrossRef]
- Raju, T.N.K.; Pemberton, V.L.; Saigal, S.; Blaisdell, C.J.; Moxey-Mims, M.; Buist, S. Long-Term Healthcare Outcomes of Preterm Birth: An Executive Summary of a Conference Sponsored by the National Institutes of Health Other Research Approaches in Preterm Born Individuals. J. Pediatr. 2016, 181, 309–318.e1. [Google Scholar] [CrossRef]
- Ganpat, Y. Low-dose aspirin for pre-term birth prevention in LMICs: A systematic review and meta-analysis. BMC Pregnancy Childbirth 2024, 24, 260. [Google Scholar]
- Van Vliet, E.O.G.; Askie, L.A.; Mol, B.W.J.; Oudijk, M.A. Antiplatelet agents and the prevention of spontaneous preterm birth: A systematic review and meta-analysis. Obstet. Gynecol. 2017, 129, 327–336. [Google Scholar] [CrossRef]
- Nadeau-Vallée, M.; Obari, D.; Palacios, J.; Brien, M.; Duval, C.; Chemtob, S.; Girard, S. Sterile inflammation and pregnancy complications: A review. Reproduction 2016, 152, R277–R292. [Google Scholar] [CrossRef]
- Atallah, M.; Yamashita, T.; Abe, K. Effect of edaravone on pregnant mice and their developing fetuses subjected to placental ischemia. Reprod. Biol. Endocrinol. 2021, 19, 19. [Google Scholar]
- Klumper, J.; Ravelli, A.C.J.; Roos, C.; Abu-Hanna, A.; Oudijk, M.A. Deprived neighborhoods and spontaneous preterm birth: A national cohort study. Eur. J. Obstet. Gynecol. Reprod. Biol. 2022, 274, 88–95. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.; Zhang, X.; Li, W.; Li, W.; Wang, Y.; Zhang, S.; Zhu, C. Iatrogenic vs. Spontaneous Preterm Birth: A Retrospective Study of Neonatal Outcome Among Very Preterm Infants. Front. Neurol. 2021, 12, 649749. [Google Scholar]
- Kamphuis, E.I.; Ravelli, A.C.J.; Koullali, B.; Kazemier, B.; de Groot, C.J.M.; Mol, B.W.J. Spontaneous and iatrogenic preterm birth rates among unselected women in three consecutive pregnancies. Eur. J. Obstet. Gynecol. Reprod. Biol. 2018, 228, 92–97. [Google Scholar] [CrossRef]
- Duley, L.; Meher, S.; Hunter, K.E.; Seidler, A.L.; Askie, L.M. Antiplatelet agents for preventing pre-eclampsia and its complications. Cochrane Database Syst. Rev. 2019, 2019, CD004659. [Google Scholar] [CrossRef]
- Hoffman, M.K.; Goudar, S.S.; Kodkany, B.S.; Metgud, M.; Somannavar, M.; Okitawutshu, J.; Lokangaka, A.; Tshefu, A.; Bose, C.L.; Mwapule, A.; et al. Low-dose aspirin for the prevention of preterm delivery in nulliparous women with a singleton pregnancy (ASPIRIN): A randomised, double-blind, placebo-controlled trial. Lancet 2020, 395, 285–293. [Google Scholar]
- Campbell, F.; Salam, S.; Sutton, A.; Jayasooriya, S.M.; Mitchell, C.; Amabebe, E.; Balen, J.; Gillespie, B.M.; Parris, K.; Soma-Pillay, P.; et al. Interventions for the prevention of spontaneous preterm birth: A scoping review of systematic reviews. BMJ Open 2022, 12, e052576. [Google Scholar]
- ROSPERO. International Prospective Register of Systematic Reviews. Available online: https://www.crd.york.ac.uk/prospero/display_record.php?ID=CRD42020212385 (accessed on 20 October 2023).
- Search|Mendeley. Available online: https://www.mendeley.com/search/ (accessed on 19 August 2022).
- 8 Assessing Risk of Bias in Included Studies. Available online: https://handbook-5-1.cochrane.org/chapter_8/8_assessing_risk_of_bias_in_included_studies.htm (accessed on 19 August 2022).
- The Cochrane Collaboration. Review Manager (RevMan) [Computer Program], Version 5.4, The Cochrane Collaboration: London, UK, 2020.
- Guyatt, G.H.; Oxman, A.D.; Vist, G.E.; Kunz, R.; Falck-Ytter, Y.; Alonso-Coello, P.; Schünemann, H.J. GRADE: An emerging consensus on rating quality of evidence and strength of recommendations. BMJ 2008, 336, 924–926. [Google Scholar] [PubMed]
- Anonymous. ECPPA: Randomised trial of low dose aspirin for the prevention of maternal and fetal complications in pregnancy. Br. J. Obstet. Gynaecol. 1996, 103, 39–47. [Google Scholar]
- Byaruhanga, R.N.; Chipato, T.; Rusakaniko, S. A randomized controlled trial of low-dose aspirin in women at risk from pre-eclampsia. Int. J. Gynecol. Obstet. 1998, 60, 129–135. [Google Scholar]
- Golding, J. A randomised trial of low dose aspirin for primiparae in pregnancy. Br. J. Obstet. Gynaecol. 1998, 105, 293–299. [Google Scholar]
- Taherian, A.A.; Taherian, A.; Shirvani, A. Prevention of preeclampsia with low-dose aspirin or calcium supplementation. Arch. Iran. Med. 2002, 5, 151–156. [Google Scholar]
- Ebrashy, A.; Ibrahim, M.; Marzook, A.; Yousef, D. Usefulness of Aspirin Therapy in High-risk Pregnant Women with Abnormal Uterine Artery Doppler Ultrasound at 14–16 Weeks Pregnancy: Randomized Controlled Clinical Trial. Croat. Med. J. 2005, 46, 826–831. [Google Scholar] [PubMed]
- Bakhti, A.; Vaiman, D. Prevention of gravidic endothelial hypertension by aspirin treatment administered from the 8th week of gestation. Hypertens. Res. 2011, 34, 1116–1120. [Google Scholar]
- Sharma, N.; Srinivasan, S.; Srinivasan, K.J.; Nadhamuni, K. Role of Aspirin in High Pulsatility Index of Uterine Artery: A Consort Study. J. Obstet. Gynecol. India 2018, 68, 382–388. [Google Scholar]
- Psyche, V. Effect of Early Administration of Low Dose Aspirin to Prevent Preeclampsia in Women at High Risk. J. Med. Sci. Clin. Res. 2018, 6, 32461–32469. [Google Scholar] [CrossRef]
- Di Renzo, G.C.; Fonseca, E.; Gratacos, E.; Hassan, S.; Kurtser, M.; Malone, F.; Nambiar, S.; Nicolaides, K.; Sierra, N.; Yang, H. Good clinical practice advice: First trimester screening and prevention of pre-eclampsia in singleton pregnancy. Int. J. Gynecol. Obstet. 2019, 144, 325–329. [Google Scholar]
- Ncc-wch. Hypertension in Pregnancy. 2011. Available online: www.cla.co.uk (accessed on 18 August 2023).
- ACOG Committee. Low-dose Aspirin Use During Pregnancy. Opinion Number 473. Obstet. Gynecol. 2018, 132, e44–e52. [Google Scholar]
- Moungmaithong, S.; Wang, X.; Tai, A.S.; Feng, Q.; Sahota, D.; Leung, T.Y.; Poon, L.C. First trimester screening for preeclampsia: An asian perspective. Matern. Med. 2021, 3, 116–123. [Google Scholar]
- Low Dose Aspirin (150 mg) in Pregnancy. Available online: www.esht.nhs.uk (accessed on 12 August 2023).
- Kozer, E.; Nikfar, S.; Costei, A.; Boskovic, R.; Nulman, I.; Koren, G. Aspirin consumption during the first trimester of pregnancy and congenital anomalies: A meta-analysis. Am. J. Obstet. Gynecol. 2002, 187, 1623–1630. [Google Scholar]
- Levin, D.L.; Mills, L.J.; Parkey, M.; Garriott, J.; Campbell, W. Constriction of the fetal ductus arteriosus after administration of indomethacin to the pregnant ewe. J. Pediatr. 1979, 94, 647–650. [Google Scholar] [PubMed]
- Morton, V.H.; Stock, S.J. Low-dose aspirin for the prevention of preterm birth: More questions than answers. PLoS Med. 2022, 19, e1003908. [Google Scholar]
- van Doorn, R.; Mukhtarova, N.; Flyke, I.P.; Lasarev, M.; Kim, K.; Hennekens, C.H.; Hoppe, K.K. Dose of aspirin to prevent preterm preeclampsia in women with moderate or high-risk factors: A systematic review and meta-analysis. PLoS ONE 2021, 16, e0247782. [Google Scholar]
- Mirabito Colafella, K.M.; Neuman, R.I.; Visser, W.; Danser, A.H.J.; Versmissen, J. Aspirin for the prevention and treatment of pre-eclampsia: A matter of COX-1 and/or COX-2 inhibition? Basic Clin. Pharmacol. Toxicol. 2020, 127, 132–141. [Google Scholar]
- Choi, Y.J.; Shin, S. Aspirin Prophylaxis During Pregnancy: A Systematic Review and Meta-Analysis. Am. J. Prev. Med. 2021, 61, e31–e45. [Google Scholar]
- Man, R.; Hodgetts Morton, V.; Devani, P.; Morris, R.K. Aspirin for preventing adverse outcomes in low-risk nulliparous women with singleton pregnancies: A systematic review and meta-analysis. Eur. J. Obstet. Gynecol. Reprod. Biol. 2021, 262, 105–112. [Google Scholar]
- Nieves, C.; Victoria da Costa Ghignatti, P.; Aji, N.; Bertagnolli, M. Immune Cells and Infectious Diseases in Preeclampsia Susceptibility. Can. J. Cardiol. 2024, 40, 2340–2355. [Google Scholar] [CrossRef]
- CDC. About Zika|Zika Virus|. Available online: https://www.cdc.gov/zika/about/index.html (accessed on 26 February 2025).
- Bauserman, M.; Leuba, S.I.; Hemingway-Foday, J.; Nolen, T.L.; Moore, J.; McClure, E.M.; Lokangaka, A.; Tsehfu, A.; Patterson, J.; Liechty, E.A.; et al. The efficacy of low-dose aspirin in pregnancy among women in malaria-endemic countries. BMC Pregnancy Childbirth 2022, 22, 303. [Google Scholar] [CrossRef]


| Secondary Outcomes | Trials (n) | Participants (n) | Random Effect, Relative Risk (95% CI) | p-Value | I2 (%) |
|---|---|---|---|---|---|
| Low birthweight | 2 | 17,301 | 0.93 (0.87 to 1.00) | 0.04 | 0 |
| Perinatal mortality | 4 | 20,427 | 0.83 (0.73 to 0.94) | <0.01 | 0 |
| Antepartum hemorrhage | 5 | 21,315 | 0.92 (0.66 to 1.27) | 0.51 | 19 |
| Post-partum hemorrhage | 6 | 21,873 | 1.20 (0.89 to 1.61) | 0.18 | 47 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ganpat, Y.; Campbell, F. Low-Dose Aspirin for Preterm Birth Prevention in Low- and Middle-Income Countries: A Systematic Review and Meta-Analysis. Reprod. Med. 2025, 6, 8. https://doi.org/10.3390/reprodmed6020008
Ganpat Y, Campbell F. Low-Dose Aspirin for Preterm Birth Prevention in Low- and Middle-Income Countries: A Systematic Review and Meta-Analysis. Reproductive Medicine. 2025; 6(2):8. https://doi.org/10.3390/reprodmed6020008
Chicago/Turabian StyleGanpat, Yeeshana, and Fiona Campbell. 2025. "Low-Dose Aspirin for Preterm Birth Prevention in Low- and Middle-Income Countries: A Systematic Review and Meta-Analysis" Reproductive Medicine 6, no. 2: 8. https://doi.org/10.3390/reprodmed6020008
APA StyleGanpat, Y., & Campbell, F. (2025). Low-Dose Aspirin for Preterm Birth Prevention in Low- and Middle-Income Countries: A Systematic Review and Meta-Analysis. Reproductive Medicine, 6(2), 8. https://doi.org/10.3390/reprodmed6020008