Abstract
This study investigates the emergence of psychosocial risks during the COVID-19 pandemic in the architecture, engineering, and construction (AEC) industry. It aims to enhance mental health outcomes for project professionals by identifying pandemic-related stressors, evaluating the role of organisational interventions, and developing a practical framework for psychosocial risk management. Guided by Job Demands–Resources (JDR) theory, the research involved a literature review, expert consultations, and a structured survey targeting AEC project managers. The findings reveal that COVID-19-related psychosocial risks such as work overload, isolation, job insecurity, and blurred work–life boundaries were negatively associated with mental health. Organisational interventions were positively associated with improved mental health. However, the moderating effect of organisational intervention on the relationship between psychosocial risks and mental health was not statistically significant. This study proposes a framework to guide AEC organisations in integrating proactive mental health strategies into everyday project practices. While the data are sector-specific and collected during a crisis period, the implications extend to broader project-based settings. This research offers practical insights for AEC firms, policymakers, and industry stakeholders on supporting workforce well-being through targeted interventions. It also contributes conceptually by linking pandemic-induced stressors to established theoretical models of occupational stress, highlighting the need for sector-specific strategies in promoting psychological safety in high-demand work environments.
1. Introduction
Architecture, engineering, and construction (AEC) project management is characterised by stringent budgets, unrealistic project deadlines, complex procurement systems and multiple project stakeholders. These features of project-based work expose project management (PM) practitioners to sustained work pressure, long working hours, role conflict and work–family imbalance, all of which have been associated with poor mental health [1,2,3]. Poor mental health among construction professionals is recognised as a significant occupational health concern that can lead to adverse organisational and economic consequences, including reduced productivity, increased absenteeism and increased turnover [4,5].
In response to these challenges, several studies were conducted to examine the issues of mental health risks and intervention strategies in the AEC industry [2,6,7]. While researchers and practitioners continue to explore innovative interventions, the coronavirus (COVID-19) has introduced new psychosocial risks like job insecurity, role ambiguity, working from home and unsafe project environments, limiting the potential of the existing mental health interventions [8,9]. The COVID-19 pandemic is a serious health problem that disrupted management practices by intensifying existing stressors and generating new psychosocial risks. COVID-19-related disruptions, such as job insecurity, rapid changes in work arrangements including working from home, and heightened concerns about health and site safety, altered the psychosocial conditions under which AEC projects were managed [10].
Few studies have examined how COVID-19 has impacted the mental health of PMPs. For instance, Pirzadeh and Lingard [11] confirmed the positive impact of working from home on the mental health of project-based construction workers during the COVID-19 pandemic. Liang, Liu, Yang and Xia [9] explored how coping behaviour moderates COVID-19-induced psychosocial risks and mental health. Complementing these studies, Adesi et al. [12] documented the extent of COVID-19-induced environmental turbulence in AEC project delivery, identifying severe disruptions related to scheduling, performance and productivity, worker anxiety, employee stress, and poor well-being. Despite increasing attention to mental health in construction during the COVID-19 pandemic, existing studies have predominantly focused on individual-level outcomes, general workforce populations, or isolated factors such as stressors or coping mechanisms. Limited research has simultaneously examined the holistic perspective of problems along with the solutions and outcomes and pandemic-induced psychosocial risks, organisational-level interventions, and mental health outcomes within project-based AEC environments. This study addresses these gaps by developing and empirically testing an integrated model that links COVID-19-related psychosocial risks, organisational interventions, and mental health among project management practitioners in AEC organisations. This study contributes by focusing on organisational-level mechanisms rather than individual coping strategies, applying JDR theory within a pandemic context, and providing sector-specific evidence from project-based work environments.
2. Review of Literature
2.1. Mental Health Among Project Management Practitioners
Mental health in occupational settings is commonly examined with regard to stress-related outcomes that reflect individuals’ psychological responses to work demands and organisational conditions [13]. In this study, mental health is conceptualised in terms of work-related stress and operationalised using the PSS-10 (Perceived Stress Scale-10) questionnaire.
Project management practitioners are professionals who are actively engaged in project management roles like the planning, execution, monitoring, maintenance and closing of projects across various sectors [14]. These positions are widely recognised as comparatively demanding and stress-intensive because they require the continuous coordination of teams, strict financial oversight, active stakeholder engagement, and tight schedule control [14]. Pressure arising from constrained budgets, ambitious timelines, and competing stakeholder priorities increases the psychological burden on project management professionals [15]. However, the mental health of PMPs in the AEC sector has always been overshadowed by the physical safety aspect, even at the cost of decreased productivity [16]. Previous studies have linked these project-related demands to increased levels of stress, burnout, and psychological strain among construction project managers, highlighting mental health as a critical occupational issue within project-based organisations [17]. Recognising the factors that contribute to mental stress is also crucial for devising effective preventative measures [18].
2.2. COVID-19-Induced Psychosocial Risks
Psychosocial risk in the workplace refers to different aspects in the design or management of work that lead to work-related stress [19]. They encompass aspects of job roles, work organisation, and the work environment that can adversely affect psychological and physical health. The COVID-19 pandemic introduced unprecedented disruptions to the AEC industry, including supply chain interruptions, regulatory uncertainty, remote working arrangements, and heightened health and safety concerns [20]. While these disruptions are not psychosocial risks in themselves, they intensified existing psychosocial risks by increasing uncertainty, work pressure, and job insecurity [21]. The pandemic substantially intensified such risks in the workplace by introducing prolonged uncertainty, rapid changes in work organisation, and heightened health-related concerns [22]. Unlike conventional project stressors, pandemic-related disruptions were largely external, uncontrollable, and persistent, thereby exacerbating existing psychosocial risks rather than creating entirely new ones [23]. Occupational health research indicates that such conditions increase the likelihood of psychological strain when job demands escalate while workers’ perceived control and predictability decline [12].
2.3. Organisational Interventions for Project Management Practitioners
Organisational interventions comprise structured, theory-informed, and behaviour-oriented initiatives aimed at modifying work design through adjustments in organisational structures, policies, managerial practices, culture, role allocation, and task arrangements in order to mitigate psychosocial risks and enhance employees’ mental health [24]. Such interventions adopt a preventive orientation and seek to enhance both individual psychological outcomes and organisational performance indicators, including staff retention, sickness absence, and productivity [25,26].
Unlike individual-level interventions that focus on personal coping or resilience, organisational interventions target upstream sources of work-related stress embedded within organisational systems, roles, and processes [27]. Prior research demonstrates that such interventions are effective in improving mental health outcomes and organisational performance indicators, including reduced turnover intentions, lower sickness absence, and enhanced productivity [28].
Before the COVID-19 pandemic, organisational interventions in construction and project-based environments involved aspects like managing workload, enhancing supervisory support, and promoting work–life balance, etc. [29]. The COVID-19 pandemic significantly altered work conditions and intensified psychosocial risks [22], necessitating the adaptation and expansion of organisational interventions. Pandemic-related interventions extended beyond traditional work design measures to include flexible and remote working arrangements, revised health and safety protocols, enhanced organisational communication, mental health support initiatives, and adjustments to project delivery processes [22]. These interventions are aimed at mitigating heightened job insecurity, uncertainty, work–life boundary blurring, and health-related anxiety experienced by workers during prolonged crisis conditions [27,30]. The resurgence of psychosocial hazards associated with COVID-19 necessitates adjustments in work design through modifications to organisational processes, structures, and programmes to support employees’ mental health [25,31]. Such organisational responses aim to mitigate pandemic-related psychosocial risks and foster positive psychological well-being among workers [32].
3. Theoretical Framework
Job Demands–Resources Theory
This investigation is grounded in the Job Demands–Resources (JDR) theory, which is widely applied in occupational health and safety research. The theory asserts that psychological strain arises when job demands exceed the resources available to manage them and that insufficient resources are associated with adverse mental health outcomes among employees [33]. Guided by this framework, organisational interventions are conceptualised as mechanisms that can reduce COVID-19-related psychosocial risks by strengthening resources within AEC project-based organisations. On this basis, three hypotheses were formulated. Figure 1 illustrates the conceptual model that informs this study.
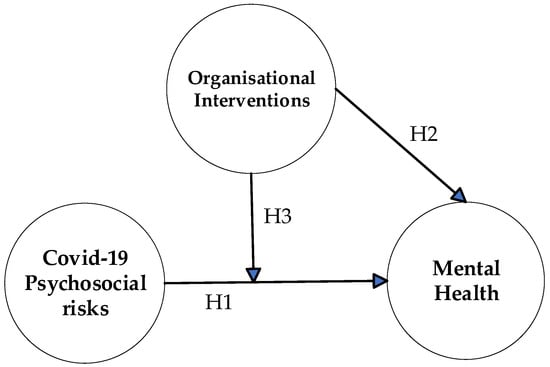
Figure 1.
Theoretical Model.
4. Hypotheses Formulation
4.1. COVID-19-Induced Psychosocial Risks on Mental Health
Past research has documented that work-related hazards contribute to adverse mental health outcomes among project management practitioners, arguing for the development of targeted interventions. Commonly reported risks include prolonged working hours, elevated workload, insufficient recovery time, and work–family conflict. The onset of COVID-19 generated additional stressors, such as social isolation, remote working arrangements, employment insecurity, revenue decline, fear of infection, and disruptions to procurement processes as well as project planning and control practices. These pandemic-related factors have intensified the psychological strain among project managers within project-based AEC organisations.
The systematic identification of COVID-19-related psychosocial risks in project environments is a necessary step in refining management practices aimed at strengthening positive mental health among project management practitioners. Prior research underscores the importance of accurately identifying psychosocial hazards when designing preventive workplace interventions. Given the limited empirical evidence on pandemic-related mental health challenges within AEC project settings, this study draws on the broader workplace literature and incorporates expert consultation to determine context-specific psychosocial risks. Accordingly, the following hypothesis is proposed:
H1.
COVID-19-related psychosocial risks have a negative effect on mental health.
4.2. Impacts of Organisational Interventions on Mental Health
Organisational interventions function as workplace resources that support positive mental health by reducing psychosocial hazards and strengthening employees’ cognitive and emotional capacity. Evidence indicates that such interventions can enhance psychological well-being and job satisfaction, particularly when they target the underlying sources of psychosocial risk and expand access to supportive resources [34]. Through adjustments to organisational design, operational procedures, and project management practices, these interventions can contribute to improved mental health outcomes among project managers in AEC settings [1,2]. Accordingly, the following hypothesis is proposed:
H2.
Organisational interventions have a positive effect on mental health.
4.3. Moderating Effect of Organisational Interventions
In line with Job Demands–Resources theory, organisational resources can buffer the adverse consequences of job demands on employees’ mental health [33]. When adequate resources are unavailable, sustained job demands may lead to burnout and psychological strain. On this basis, organisational interventions are expected to attenuate the negative association between COVID-19-related psychosocial risks and mental health. Therefore, the following hypothesis is advanced:
H3.
Organisational interventions have a moderating effect on the relation between COVID-19 psychosocial risk and mental health.
Figure 1 illustrates the theoretical framework underpinning this study, grounded in the Job Demands–Resources (JDR) theory. The model conceptualises COVID-19-related psychosocial risks as job demands that exert a direct negative influence on the mental health of project management practitioners. Organisational interventions are positioned as job resources that directly promote positive mental health and are hypothesised to have a moderating relation between COVID-19-induced risks and mental health outcomes. In line with JDR theory, the framework reflects the assumption that heightened job demands in the form of pandemic-related psychosocial risks impair mental health, while organisational resources can both enhance mental health directly and buffer, to varying degrees, the adverse effects of excessive demands. The proposed relationships are operationalised through three hypotheses, capturing the direct effect of psychosocial risks on mental health, the direct effect of organisational interventions on mental health, and the moderating role of organisational interventions.
5. Operationalisation of Constructs
The questionnaire consisted of three construct groups: COVID-19 psychosocial risks, organisational interventions, and mental health. Measurement items for COVID-19 psychosocial risks and organisational interventions were initially identified through an extensive review of prior studies and subsequently refined through expert consultation to ensure contextual relevance to AEC project environments during the COVID-19 pandemic. The mental health construct was measured using the established Perceived Stress Scale-10 (PSS-10). Table 1, Table 2 and Table 3 summarise the final measurement items included in the questionnaire.
5.1. COVID-19 Psychosocial Risks
Table 1 presents the final COVID-19 psychosocial risk items included in the questionnaire. The references associated with each item indicate the principal studies and literature sources that informed the development and adaptation of the measurement indicators. After the literature review, the questionnaire was subjected to consultation through expert forums to ensure clarity and contexualisation. The combined use of these approaches enabled the identification of context-specific indicators relevant to AEC project-based organisations. Drawing on this evidence, COVID-19 psychosocial risk was operationalised using nineteen items. These indicators were labelled CO-RISK-1 to CO-RISK-19, and responses were recorded on a five-point Likert scale.

Table 1.
Operationalisation of COVID-19-induced psychosocial risk.
5.2. Organisational Interventions
Careful operationalisation of the construct is essential to ensure that measurement items are appropriate for questionnaire development. A comprehensive review of prior studies combined with insights from expert consultations identified multiple indicators relevant to organisational interventions. Based on this process, the construct was defined using twenty measurement items, as outlined in Table 2. These indicators were labelled CO-OPM-1 to CO-OPM-20, and responses were captured using a five-point Likert scale.
Table 2.
Operationalisation of organisational interventions.
5.3. Mental Health
This study operationalised mental health using the Perceived Stress Scale-10 item version, PSS-10, developed by Cohen, Kamarck and Mermelstein [57]. The PSS-10 is a self-administered psychological instrument that assesses the extent to which individuals perceive their life circumstances as stressful [57,58]. The scale has been applied in previous Australian research contexts [59,60] and has also been validated and utilised in studies conducted in the United Kingdom by Denovan, Dagnall, Dhingra and Grogan [61] and in the United States [62]. Table 3 outlines the operational definition and measurement items for the mental health construct.
Table 3.
Operationalisation of stress-induced mental health.
6. Materials and Methods
Based on the aim of this research, a deductive approach was selected for the research design based on the recommendation of Creswell [63] and Kumar [64]. Furthermore, a survey was carried out to collect quantitative data from PM practitioners in Australia to ensure a wider coverage among PM practitioners.
6.1. Questionnaire Survey Development
A structured questionnaire survey was developed to collect data from project management practitioners in the AEC sector. The questionnaire was developed after an extensive review of the literature and a formal expert consultation process to ensure contextual relevance to project-based work during the COVID-19 pandemic. An initial pool of psychosocial risk and organisational intervention items was identified from prior studies in construction management, occupational health, and work stress research. These items were then refined through an expert consultation involving nine professionals with backgrounds in engineering, construction, architecture, and project management. The selection of experts followed a structured two-step process adapted from established expert opinion methodologies. In the first step, nine project management professionals were identified through the researchers’ professional network using convenience sampling. In the second step, these experts were formally invited and screened based on their qualifications, education, project management experience, and professional affiliations to ensure their suitability for contributing to this study. All experts had a minimum of six years of project management-oriented experience, with six experts having more than fifteen years of experience and holding senior managerial or professional roles during the COVID-19 period. The consultation was conducted through an online expert forum, where experts evaluated the relevance, clarity, and applicability of each item to AEC project organisations operating under pandemic conditions. Experts were also invited to propose additional factors not captured in the initial item pool. Items endorsed by the majority of experts were retained, while overlapping or less relevant items were revised or removed based on qualitative feedback. This process resulted in a final set of 19 COVID-19-related psychosocial risk items and 20 organisational intervention items.
Accordingly, the final questionnaire comprised a single integrated survey instrument containing four sections: demographic information, COVID-19 psychosocial risk items, organisational intervention items, and mental health items adapted from the PSS-10 scale. The COVID-19 psychosocial risk construct contained 19 items, organisational interventions contained 20 items, and mental health was measured using the 10-item PSS-10 scale.
6.2. Validity and Reliability of the Survey
The content validity of the questionnaire was established through the combined use of an extensive literature review and expert consultation. Prior to full-scale data collection, a pilot survey was conducted with a small group of project management practitioners to assess face validity, clarity of wording, and overall survey structure. The pilot study was conducted with four participants, including two academics and two industry professionals who were not part of the expert panel. Three of the experts had 5 years of experience in project management, and one associate professor from academia had 5 publications in studies related to mental health. Feedback from the pilot survey was used to refine item phrasing, improve readability, and confirm the suitability of the questionnaire length and response format.
Following data collection, the reliability and construct validity of the measurement model were evaluated using partial least squares structural equation modelling (PLS-SEM). Internal consistency reliability was assessed using Cronbach’s alpha and composite reliability. Convergent validity was examined using average variance extracted, while discriminant validity was assessed using cross-loading criteria. These procedures ensured that the measurement model met established reliability and validity requirements prior to structural model analysis.
6.3. Sampling and Data Collection
A non-probability convenience sampling strategy was employed to recruit project management practitioners capable of providing informed insights into mental health conditions within AEC project organisations during the COVID-19 period. This approach was adopted due to the limited timeframe of the study and the practical accessibility of potential respondents. In addition, the absence of a comprehensive registry detailing the total number of AEC firms in Australia constrained the feasibility of probability-based sampling, thereby supporting the suitability of convenience sampling for this investigation.
A total of 200 online questionnaires were circulated to AEC organisations across Australia, yielding 58 usable responses and a response rate of 29 percent. The adequacy of the sample size was assessed using the ten times rule, which recommends that the minimum sample should be ten times the maximum number of structural paths directed toward any endogenous construct in the model [65]. The structural model in this study contained three such paths, resulting in a minimum required sample of 30 observations. The final dataset comprised 58 responses, exceeding this threshold and indicating sufficient sample size for analysis.
7. Results and Analysis
The survey data were analysed using SPSS version 27 and structural equation modelling. The internal reliability of the measurement scales was evaluated using Cronbach’s alpha to assess the consistency of the items within each construct [66]. Mean score analysis was also performed to identify the relative significance of the indicators related to mental health, COVID-19 psychosocial risks, and organisational interventions.
Structural equation modelling enables the simultaneous estimation of multiple interrelated relationships, incorporates latent constructs, and accounts for measurement error within the modelling process [67]. The method has been widely applied in mental health research to examine associations among unobserved variables. In this study, SEM was utilised to test the relationships between COVID-19-related psychosocial risks, organisational intervention practices, and mental health outcomes. Two principal SEM approaches exist: covariance-based SEM and partial least squares SEM. Partial least squares SEM was selected because of its suitability for non-normally distributed data and its appropriateness for studies with relatively small sample sizes [65,68]. The analysis was conducted using Smart-PLS version 3.2.8, which aligns with the methodological requirements of this study [65].
7.1. Respondents’ Profile
Table 4 summarises the demographic and professional characteristics of the 58 participants. With respect to project involvement during the COVID-19 period, just over half of the respondents, 51.7 percent, reported working on between one and five projects, while 34.5 percent were involved in six to ten projects. Only a small proportion, 6.9 percent each, indicated participation in eleven to fifteen projects and sixteen to twenty projects.
Table 4.
Respondents’ profile.
The sample was predominantly male, representing 77.6 percent of respondents, while females accounted for 22.4 percent. In terms of educational attainment, the largest group held postgraduate qualifications at 32.8 percent, followed by graduate-level degrees at 31.0 percent and doctoral degrees at 20.7 percent. A smaller proportion reported diploma-level education at 10.3 percent, high school education at 3.4 percent, and vocational certification at 1.7 percent.
Regarding professional experience in project management-oriented roles, nearly half of the participants, 48.3 percent, had sixteen years or more of experience. Respondents with six to ten years of experience comprised 20.7 percent, those with zero to five years accounted for 18.9 percent, and 12.1 percent reported eleven to fifteen years of experience. Overall, the profile indicates a sample with substantial professional experience and advanced educational backgrounds.
7.2. Measurement Model Evaluation
The measurement model was examined to determine the reliability and validity of the latent constructs. The indicators with outer loadings less than 0.4 were removed from the model for all three constructs of psychosocial risks, mental health and interventions [65]. While all of the indicators from organisational intervention were retained, as they satisfied the evaluation criteria, several criteria from the constructs ’Psychosocial Risk’ and ‘Mental Health’ were deleted to satisfy the model. The outcomes of this assessment are presented in Table 5, Table 6 and Table 7. Confirmatory factor analysis was applied to test internal consistency reliability, convergent validity, and discriminant validity, thereby evaluating the extent to which the observed indicators adequately represent their respective constructs [69].
Table 5.
Measurement model for mental health.
Table 6.
Measurement model for COVID-19 psychosocial risks.
Table 7.
Measurement model for organisational interventions.
The ranking column represents the relative contribution of each indicator to its respective latent construct based on the magnitude of the outer loading values obtained from the PLS-SEM measurement model. Indicators with higher outer loadings were assigned higher rankings, indicating a comparatively stronger representation of the construct.
7.2.1. Internal Consistency Reliability
Internal consistency was evaluated using Cronbach’s alpha and composite reliability [70]. Both indices range from 0 to 1, with higher values indicating stronger reliability. A minimum threshold of 0.7 was adopted for both measures in accordance with established guidelines [65].
7.2.2. Convergent Validity
Convergent validity was assessed by examining outer loadings and average variance extracted, AVE. As reported in Table 5, Table 6 and Table 7, the initial outer loading values ranged from −0.8 to 0.9. Following recommendations from Hair, Hult, Ringle and Sarstedt [65], those outer loadings with values below 0.4 were deleted. In addition, the AVE values for each construct were above the suggested benchmark of 0.50 [71]. These results confirm that the measurement model demonstrates adequate convergent validity.
7.2.3. Discriminant Validity
Discriminant validity was evaluated using cross-loadings and the heterotrait–monotrait ratio of correlations, HTMT [65]. Table 8 presents the cross-loading results. Each indicator demonstrated a higher loading on its intended construct relative to other constructs in the model, supporting discriminant validity. The HTMT criterion was also applied to further assess construct distinctiveness. A threshold of 0.9 was adopted for HTMT, for which correlations between latent variables should remain below this value to confirm adequate separation [72]. As reported in Table 9, all HTMT values were below 0.9, indicating that COVID-19 psychosocial risks, organisational interventions, and mental health represent empirically distinct constructs.
Table 8.
Cross-loading analysis of the constructs.
Table 9.
Heterotrait–monotrait ratio of correlations (HTMT).
7.3. Structural Model Evaluation
Path analysis was conducted to evaluate the structural model and estimate the associations among the latent variables. The figurative representation is shown in Figure 2. The model was formulated to assess the relationships linking COVID-19 psychosocial risks, organisational interventions, and mental health. The findings indicate that all three of the proposed hypotheses were statistically significant at p less than 0.01, as reported in Table 10. Predictive capability was evaluated using effect size, f squared, to determine the contribution of each exogenous construct to the endogenous variable. As shown in Table 11, all f squared values exceeded the recommended minimum threshold of 0.02 [65], indicating that the model demonstrates acceptable explanatory power. In addition, predictive relevance was assessed using the blindfolding procedure to compute Q squared, which reflects the model’s ability to predict observed values. The Q squared results are presented in Table 12.
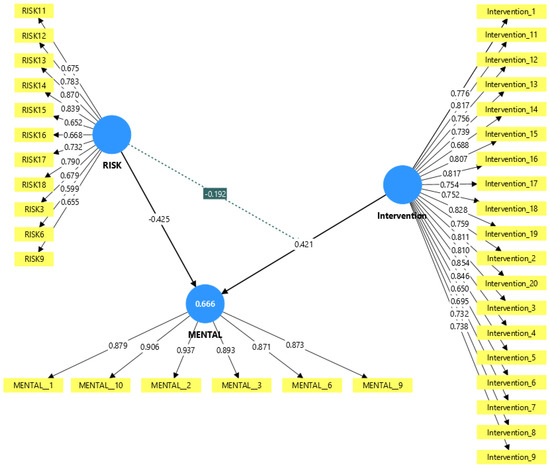
Figure 2.
Final SEM Model.
Table 10.
Summary of hypotheses for the model.
Table 11.
Summary of effect size.
Table 12.
Predictive power of dependent variables (Q2).
7.4. Relationship Between COVID-19 Psychosocial Risk and Mental Health
The linkage between COVID-19-related psychosocial risks and mental health was examined using structural equation modelling. The findings reveal a statistically significant negative association between these variables: β equals minus 0.425, t equals 4.80, and p equals 0.000. This indicates that higher levels of COVID-19 psychosocial risk are associated with poorer mental health outcomes, thereby supporting H1.
7.5. Relationship Between Organisational Interventions and Mental Health
The relation between organisational interventions and mental health was also assessed using the SEM framework. The results demonstrate a significant positive relationship: β equals 0.421, t equals 5.905, and p equals 0.000. This suggests that stronger organisational intervention practices are linked to better mental health, providing support for H2.
7.6. Moderating Role of Organisational Interventions
The structural model was used to examine whether organisational interventions moderated the association between COVID-19 psychosocial risks and mental health. The interaction term was negative and statistically significant: β equals minus 0.192, t equals 2.588, and p equals 0.01. These results indicate that organisational interventions significantly buffer the adverse effect of COVID-19 psychosocial risks on mental health, leading to the acceptance of H3.
8. Discussion
The objective of this study informed the application of Job Demands–Resources theory in formulating a conceptual model linking COVID-19-related psychosocial risks, organisational interventions, and mental health outcomes. The structural equation modelling results indicate that the JDR framework provides explanatory insight into how organisational interventions are associated with mental health in the presence of COVID-19-related stressors among project management practitioners.
8.1. Impact of Psychosocial Risks on Mental Health
In line with earlier research that identified an inverse relationship between psychosocial hazards and mental health [30], The present study identified a significant association between COVID-19-related psychosocial risks and elevated perceived work stress. The findings reinforce evidence that pandemic-related psychosocial pressures adversely affect the psychological well-being of project management professionals. Prior studies have shown that exposure to psychosocial hazards within project environments is linked to poorer mental health among construction professionals [30,73,74,75,76]. Such risks are often associated with an imbalance between job demands and available organisational resources [77,78]. The current results extend this body of evidence by empirically confirming the detrimental influence of COVID-19-related psychosocial risks on mental health within the AEC industry.
Further insight is obtained from the measurement model, where high-loading indicators such as difficulty with stakeholder management (CO-RISK-13), resource constraints (CO-RISK-14), and contract management challenges (CO-RISK-18) emerged as the most influential contributors to the risk construct. These factors reflect core project management functions that were disrupted during the pandemic, indicating that operational complexity rather than only health-related fear is a critical driver of stress in AEC project environments. The results extend prior research by demonstrating that pandemic-induced psychosocial risks are not isolated stressors but rather are embedded within project delivery processes. This aligns with findings reported by [30], who identified disruptions in scheduling, coordination, and performance as key stress amplifiers for construction workers. The current study contributes by quantifying these relationships within a structural model and confirming their substantial explanatory power (R2 = 0.666), indicating that psychosocial risks account for a large proportion of the variance in mental health outcomes.
8.2. Impact of Organisational Interventions and Mental Health
In line with hypothesis H2, the findings indicate that organisational interventions are consistent with the proposed hypothesis, i.e., organisational interventions were found to be positively associated with mental health. This suggests that structured organisational practices contribute to improved psychological outcomes among project managers exposed to pandemic-related stressors. Previous research has demonstrated that organisational systems and management practices can reduce burnout and psychological strain among project professionals [1,27]. Such systems function as preventive mechanisms that address psychosocial risks and support positive mental health [27]. According to Lamontagne, Keegel and Vallance [79], organisational-level interventions have been identified as primary strategies for mitigating work-related stress.
The measurement model further highlights the most influential organisational practices, including work–life management training (CO-OPM-10), technology adaptation training (CO-OPM-4), communication systems (CO-OPM-5), and stakeholder collaboration (CO-OPM-19). These high-loading indicators suggest that interventions targeting skills development, communication, and digital infrastructure are particularly effective in supporting mental health during crisis conditions. Importantly, lower-loading items such as health screening (CO-OPM-6) and workplace disinfection (CO-OPM-7) contributed less to the construct, which indicates that operational and managerial interventions have a stronger psychological impact than purely health-protective measures in project-based settings. This finding provides a nuanced understanding that organisational responses must extend beyond compliance-based safety measures to include structural and managerial support mechanisms. The results align with evidence from [27], who identified organisational-level interventions as primary strategies for mitigating work-related stress. However, the current study advances this literature by demonstrating their effectiveness specifically within pandemic-disrupted AEC project environments, where traditional interventions required adaptation to remote work, digital coordination, and uncertainty management.
8.3. Moderating Role of Organisational Interventions
The findings indicate that organisational interventions significantly moderate the relationship between COVID-19 psychosocial risks and mental health (β = −0.192, p < 0.01), supporting hypothesis H3. The negative interaction effect suggests that organisational interventions minimise the adverse impact of psychosocial risks, which is consistent with the buffering hypothesis of JDR theory. This result implies that when organisational resources are strengthened, the detrimental influence of high job demands on mental health is reduced. Although the moderating effect size is smaller (f2 = 0.117), it remains meaningful, indicating that interventions do not eliminate stressors but rather reduce their intensity and impact on psychological outcomes. This finding aligns with prior studies that highlight the protective role of organisational support in high-demand work environments [13,73]. However, the present study extends this evidence by demonstrating the buffering effect within a pandemic context, where uncertainty, disruption, and complexity are elevated. The results suggest that organisational interventions are not only directly beneficial but also function as risk-mitigating mechanisms that enhance resilience among project management practitioners.
8.4. Comparative Contribution of Indicators
Additional insight is provided through the indicator ranking analysis presented in Table 5, Table 6 and Table 7, where rankings were assigned based on descending outer loading values to reflect the relative contribution of each indicator to its respective construct. Among the COVID-19 psychosocial risk indicators, project-related stressors such as stakeholder management challenges, resource constraints, and contract management issues demonstrated comparatively higher outer loading values, which indicates a stronger contribution to the psychosocial risk construct. Organisational interventions related to work–life management training, technology adaptation support, communication systems, and stakeholder collaboration similarly exhibited stronger contributions, which suggests greater relevance for supporting mental health outcomes within project-based work environments. By contrast, compliance-oriented measures such as workplace screening and disinfection procedures demonstrated a comparatively lower contribution to the construct. The mental health indicators further revealed that perceived stress associated with a loss of control and an inability to manage work demands represented dominant dimensions of psychological strain among respondents. Collectively, these findings extend the contribution of this study by identifying the relative importance of specific psychosocial risks and organisational interventions that influenced mental health within the AEC industry during the COVID-19 pandemic.
9. Conclusions
Mental health among project management practitioners in AEC firms represents a substantial concern, attracting increasing attention from industry stakeholders, scholars, and policymakers. The onset of COVID-19 introduced new, unanticipated stressors that intensified psychological strain, underscoring the need to examine pandemic-related risks within project environments. Organisational interventions were, therefore, considered as mechanisms for addressing emerging psychosocial challenges and informing risk management strategies aimed at protecting mental health. Guided by Job Demands–Resources theory, this study investigated the hypothesised relationships among COVID-19-induced psychosocial risks, organisational interventions, and mental health, with the objective of enhancing psychological well-being among PM practitioners during the pandemic period.
The results demonstrate a significant negative association between the two constructs of COVID-19 psychosocial risks and mental health, indicating that increased exposure to such risks is linked to poorer psychological outcomes. The strength of this relationship highlights the influence of pandemic-related stressors on PM practitioners in AEC projects. In addition, organisational interventions were found to exert a positive effect on mental health, consistent with the JDR proposition that organisational resources support employee well-being. The analysis also revealed a moderating interaction, indicating that the moderating role of organisational preventive measures on the relation between psychosocial risks and mental health was also statistically significant.
10. Limitation
This study has several limitations that should be acknowledged when interpreting the findings. First, this study employed convenience sampling to recruit project management practitioners, which may introduce selection bias. Participants were more likely to be individuals with access to professional networks, an interest in mental health topics, or availability during the COVID-19 period, which may not fully reflect the broader population of AEC project management practitioners. Second, the use of a non-probability sampling approach limits the generalisability of the findings, and caution needs to be maintained when interpreting the results in different socio-economic contexts. Third, this study is based on a relatively small sample size (n = 58), which may affect the stability of the parameter estimates and reduce statistical power, thereby limiting the robustness of the findings. In addition, the cross-sectional design of this study restricts causal inference; therefore, the observed relationships among psychosocial risks, organisational interventions, and mental health should be interpreted as statistical associations rather than causal effects. Furthermore, this study relies on self-reported measures, which may introduce response biases such as social desirability and the subjective interpretation of workplace conditions. The use of a single data source also raises the possibility of common method bias, which may inflate observed relationships despite procedural controls being applied during survey design. In addition, the adaptation of the PSS-10 scale to a work-oriented project context may affect comparability with studies using the original instrument, although acceptable reliability and validity were observed.
Author Contributions
Conceptualization, X.J. and R.O.-K.; methodology: X.J. and R.O.-K.; software, B.T.; validation, X.J., J.B., P.P. and S.P.; formal analysis, B.T., X.J. and P.P.; investigation, X.J. and J.B.; resources, X.J.; data curation, X.J. and R.O.-K.; writing—original draft preparation, B.T. and X.J.; writing—review and editing, P.P., R.O.-K., S.P. and J.B.; visualization, X.J., P.P. and S.P.; supervision, X.J.; project administration, X.J.; funding acquisition, X.J. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by Project Governance and Controls Symposium (PGCS) Ltd. (PGCS GRANT 2021), Australia.
Institutional Review Board Statement
Ethical approval for this research was obtained from the Human Research Ethics Committee of Western Sydney University (Ethics Approval ID: H14637) on 12 November 2021.
Informed Consent Statement
All participants were provided informed consent before their participation, and their confidentiality and anonymity were maintained throughout the research process.
Data Availability Statement
The data that support the findings of this study are available from the authors, upon reasonable request.
Acknowledgments
The authors acknowledge the financial support received through the PGCS Research Grant awarded by PGCS Ltd., Sydney, Australia. Appreciation is extended to the anonymous project management professionals who contributed to this study, as well as to Western Sydney University and PMLogic for their in-kind assistance. The authors also recognise the support provided by the Australian Institute of Project Management, the International Centre for Complex Project Management, the Chartered Institute of Building, the Cooperative Network of Building Researchers, and the Mosaic Project Blog.
Conflicts of Interest
The authors declare that this study received funding from PGCS Ltd. The funder was not involved in the study design, collection, analysis, interpretation of data, the writing of this article or the decision to submit it for publication. Author James Bawtree was employed by the company PMLogic. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
- Yang, F.; Li, X.; Zhu, Y.; Li, Y.; Wu, C. Job burnout of construction project managers in China: A cross-sectional analysis. Int. J. Proj. Manag. 2017, 35, 1272–1287. [Google Scholar] [CrossRef]
- Tijani, B.; Jin, X.; Osei-Kyei, R. Effect of project organization elements on the mental health of project management practitioner in AEC projects. Eng. Constr. Archit. Manag. 2024, 31, 73–114. [Google Scholar] [CrossRef]
- Pinto, J. Project management, governance, and the normalization of deviance. Int. J. Proj. Manag. 2014, 32, 376–387. [Google Scholar] [CrossRef]
- Ajayi, S.O.; Jones, W.; Unuigbe, M. Occupational stress management for UK construction professionals: Understanding the causes and strategies for improvement. J. Eng. Des. Technol. 2019, 17, 819–832. [Google Scholar] [CrossRef]
- Tijani, B.; Jin, X.; Osei-Kyei, R. Critical analysis of mental health research among construction project professionals. J. Eng. Des. Technol. 2020, 19, 467–496. [Google Scholar] [CrossRef]
- Tijani, B.; Jin, X.-H.; Osei-Kyei, R. PESTEL analysis of mental health management of project management practitioners (PMPs) in architecture, engineering and construction (AEC) project organization. Smart Sustain. Built Environ. 2023, 12, 1002–1030. [Google Scholar] [CrossRef]
- Cheung, C.; Chih, Y.-Y.; Bowen, P.; Liao, P.-C. Leadership and Employee Well-Being in the Architecture, Engineering, and Construction (AEC) Industry. J. Manag. Eng. 2023, 39, 02023001. [Google Scholar] [CrossRef]
- Wu, T.-L.; Liu, H.-T. Causal Model Analysis of the Effect of Policy Formalism, COVID-19 Fear, Social Support and Work Stress on Construction Workers’ Anxiety during the Epidemic. Buildings 2022, 13, 10. [Google Scholar] [CrossRef]
- Liang, H.; Liu, T.; Yang, W.; Xia, F. Impact of COVID-19 Pandemic Perception on Job Stress of Construction Workers. Int. J. Environ. Res. Public Health 2022, 19, 10169. [Google Scholar] [CrossRef]
- Hamouche, S. COVID-19 and employees’ mental health: Stressors, moderators and agenda for organizational actions. Emerald Open Res. 2020, 2. [Google Scholar] [CrossRef]
- Pirzadeh, P.; Lingard, H. Working from home during the COVID-19 pandemic: Health and well-being of project-based construction workers. J. Constr. Eng. Manag. 2021, 147, 04021048. [Google Scholar] [CrossRef]
- Adesi, M.; Ewuga, D.; Owusu-Manu, D.-G.; Boateng, F.; Kissi, E. COVID-19 pandemic disruptions and environmental turbulence in architectural, engineering and construction project delivery space. Int. J. Build. Pathol. Adapt. 2025, 43, 977–992. [Google Scholar] [CrossRef]
- Pokhrel, P.; Jin, X.; Osei-Kyei, R.; Al-Ashwal, A. Well-being and productivity in construction industry through gendered lens: A conceptual framework. In Australasian Universities Building Education Association Conference; Victoria University: Melbourne, Australia, 2024. [Google Scholar]
- Fu, Y.; Jin, X.; Perera, S.; Tijani, B.; Pokhrel, P. Tuning out tension: Influence of music on stress level among project management practitioners. Eng. Constr. Archit. Manag. 2025, 1–19. [Google Scholar] [CrossRef]
- Jin, X.-H.; Senaratne, S.; Fu, Y.; Tijani, B. Tackling stress of project management practitioners in the Australian construction industry: The causes, effects and alleviation. Eng. Constr. Archit. Manag. 2024, 31, 4016–4041. [Google Scholar] [CrossRef]
- Powell, A.; Galea, N.; Salignac, F.; Loosemore, M.; Chappell, L. Masculinity and workplace wellbeing in the Australian construction industry. In Proceedings of the 34th Annual Association of Researchers in Construction Management (ARCOM) Conference, Belfast, UK, 3–5 September 2018; Volume 1, pp. 321–330. [Google Scholar]
- Tijani, B.; Jin, X.; Osei-Kyei, R. Theoretical model for mental health management of project management practitioners in architecture, engineering and construction (AEC) project organizations. Eng. Constr. Archit. Manag. 2023, 30, 914–943. [Google Scholar] [CrossRef]
- Kamardeen, I.; Hasan, A. Analysis of Work-Related Psychological Injury Severity among Construction Trades Workers. J. Manag. Eng. 2023, 39, 04023001. [Google Scholar] [CrossRef]
- International Labour Organisation. Psychosocial Risks and Stress at Work. 2022. Available online: https://www.ilo.org/resource/psychosocial-risks-and-stress-work (accessed on 15 March 2023).
- Ghansah, F.A.; Lu, W. Responses to the COVID-19 pandemic in the construction industry: A literature review of academic research. Constr. Manag. Econ. 2023, 41, 781–803. [Google Scholar] [CrossRef]
- Xiao, J.; Zhao, J.; Luo, Z.; Liu, F.; Greenwood, D. The impact of built environment on mental health: A COVID-19 lockdown perspective. Health Place 2022, 77, 102889. [Google Scholar] [CrossRef]
- Musonda, I.; Onososen, A.; Moyo, T.; Tjebane, M.M. COVID-19 and shock events in the AEC sector: Perspectives on mitigating measures. In Construction Safety, Health and Well-Being in the COVID-19 Era; Routledge: Oxfordshire, UK, 2023; pp. 271–286. [Google Scholar]
- Hayes, S.W.; Priestley, J.L.; Ishmakhametov, N.; Ray, H.E. “I’m not Working from Home, I’m Living at Work”: Perceived Stress and Work-Related Burnout before and during COVID-19. PsyArXiv 2020, 103, 2391–2399. [Google Scholar]
- Naghieh, A.; Montgomery, P.; Bonell, C.P.; Thompson, M.; Aber, J.L. Organisational interventions for improving wellbeing and reducing work-related stress in teachers. Cochrane Database Syst. Rev. 2015, 2015, CD010306. [Google Scholar] [CrossRef]
- Mousa, M.; Boyle, J.; Skouteris, H.; Mullins, A.K.; Currie, G.; Riach, K.; Teede, H.J. Advancing women in healthcare leadership: A systematic review and meta-synthesis of multi-sector evidence on organisational interventions. eClinicalMedicine 2021, 39, 101084. [Google Scholar] [CrossRef]
- Rickard, G.; Lenthall, S.; Dollard, M.; Opie, T.; Knight, S.; Dunn, S.; Wakerman, J.; MacLeod, M.; Seiler, J.; Brewster-Webb, D. Organisational intervention to reduce occupational stress and turnover in hospital nurses in the Northern Territory, Australia. Collegian 2012, 19, 211–221. [Google Scholar] [CrossRef]
- Pokhrel, P.; Jin, X.; Osei-Kyei, R.; Alashwal, A. Primary Preventive Strategies for White-collar Women in Nepal’s Construction Industry: Factor analysis and Demographic Comparison. Eng. Constr. Archit. Manag. 2025, 33, 225–248. [Google Scholar] [CrossRef]
- Bhui, K.; Dinos, S.; Galant-Miecznikowska, M.; de Jongh, B.; Stansfeldand, S. Perceptions of work stress causes and effective interventions in employees working in public, private and non-governmental organisations: A qualitative study. BJPsych Bull. 2016, 40, 318–325. [Google Scholar] [CrossRef]
- Tijani, B. Developing a Framework for Mental Health Management of Project Management Practitioners in Architecture, Engineering and Construction Project Organizations; Western Sydney University: Sydney, NSW, Australia, 2020. [Google Scholar]
- Pokhrel, P.; Jin, X.; Osei-Kyei, R.; Alashwal, A. Deconstructing Disparities: Analysis of Occupational Hazards for Women in Construction. Int. J. Occup. Saf. Ergon. JOSE, 2026; in press. [CrossRef]
- Giménez-Espert, M.d.C.; Prado-Gascó, V.; Soto-Rubio, A. Psychosocial risks, work engagement, and job satisfaction of nurses during COVID-19 pandemic. Front. Public Health 2020, 8, 566896. [Google Scholar] [CrossRef]
- Chirico, F.; Ferrari, G. Role of the workplace in implementing mental health interventions for high-risk groups among the working age population after the COVID-19 pandemic. J. Health Soc. Sci. 2021, 6, 145–150. [Google Scholar]
- Demerouti, E.; Bakker, A.B.; Nachreiner, F.; Schaufeli, W. The job demandsresources model of burnout. J. Appl. Psychol. 2001, 86, 499. [Google Scholar] [CrossRef]
- Gray, P.; Senabe, S.; Naicker, N.; Kgalamono, S.; Yassi, A.; Spiegel, J.M. Workplace-based organizational interventions promoting mental health and happiness among healthcare workers: A realist review. Int. J. Environ. Res. Public Health 2019, 16, 4396. [Google Scholar] [CrossRef]
- Ho, C.S.; Chee, C.Y.; Ho, R.C. Mental health strategies to combat the psychological impact of COVID-19 beyond paranoia and panic. Ann. Acad. Med. Singap. 2020, 49, 1–3. [Google Scholar]
- Xiang, Y.-T.; Yang, Y.; Li, W.; Zhang, L.; Zhang, Q.; Cheung, T.; Ng, C.H. Timely mental health care for the 2019 novel coronavirus outbreak is urgently needed. Lancet Psychiatry 2020, 7, 228–229. [Google Scholar] [CrossRef] [PubMed]
- Alsharef, A.; Banerjee, S.; Uddin, S.; Albert, A.; Jaselskis, E. Early impacts of the COVID-19 pandemic on the United States construction industry. Int. J. Environ. Res. Public Health 2021, 18, 1559. [Google Scholar]
- Sonta, E. How COVID-19 Changes Project Management? 27 May 2020. Available online: https://www.linkedin.com/pulse/how-covid-19-changes-project-management-ewa-so%C5%84ta/?articleId=6671305950122541056 (accessed on 15 March 2023).
- Ramarajan, L.; Reid, E. Shattering the myth of separate worlds: Negotiating nonwork identities at work. Acad. Manag. Rev. 2013, 38, 621–644. [Google Scholar] [CrossRef]
- Kniffin, K.M.; Narayanan, J.; Anseel, F.; Antonakis, J.; Ashford, S.P.; Bakker, A.B.; Bamberger, P.; Bapuji, H.; Bhave, D.P.; Choi, V.K. COVID-19 and the workplace: Implications, issues, and insights for future research and action. Am. Psychol. 2021, 76, 63. [Google Scholar] [CrossRef]
- Dirani, K.M.; Abadi, M.; Alizadeh, A.; Barhate, B.; Garza, R.C.; Gunasekara, N.; Ibrahim, G.; Majzun, Z. Leadership competencies and the essential role of human resource development in times of crisis: A response to COVID-19 pandemic. Hum. Resour. Dev. Int. 2020, 23, 380–394. [Google Scholar] [CrossRef]
- Stiles, S.; Golightly, D.; Ryan, B. Impact of COVID-19 on health and safety in the construction sector. Hum. Factors Ergon. Manuf. Serv. Ind. 2021, 31, 425–437. [Google Scholar]
- CDCgov. How to Cope with Job Stress and Build Resilience During the COVID-19 Pandemic. 2020. Available online: https://stacks.cdc.gov/view/cdc/99349 (accessed on 18 November 2021).
- Raoufi, M.; Fayek, A.R. Identifying actions to control and mitigate the effects of the COVID-19 Pandemic on construction Organizations: Preliminary Findings. Public Work. Manag. Policy 2021, 26, 47–55. [Google Scholar] [CrossRef]
- Brooks, S.K.; Dunn, R.; Amlôt, R.; Rubin, G.J.; Greenberg, N. A systematic, thematic review of social and occupational factors associated with psychological outcomes in healthcare employees during an infectious disease outbreak. J. Occup. Environ. Med. 2018, 60, 248–257. [Google Scholar] [CrossRef]
- Tavares, A.I. Telework and health effects review. Int. J. Healthc. 2017, 3, 30. [Google Scholar]
- World Health Organization and International Labour Organisation Office (Ed.) Preventing and Mitigating COVID-19 at Work; World Health Organization and International Labour Organisation Office: Geneva, Switzerland, 2021. [Google Scholar]
- van der Molen, H.F.; Basnet, P.; Hoonakker, P.L.; Lehtola, M.M.; Lappalainen, J.; Frings-Dresen, M.H.; Haslam, R.; Verbeek, J.H. Interventions to prevent injuries in construction workers. Cochrane Database Syst. Rev. 2018, 2018, CD006251. [Google Scholar] [CrossRef]
- Pamidimukkala, A.; Kermanshachi, S. Impact of COVID-19 on field and office workforce in construction industry. Proj. Leadersh. Soc. 2021, 2, 100018. [Google Scholar] [CrossRef]
- International Labour Organisation Office. Managing Work-Related Psychosocial Risks During the COVID-19 Pandemic; International Labour Organisation Office: Geneva, Switzerland, 2020. [Google Scholar]
- Koch, J.; Schermuly, C.C. Managing the Crisis: How COVID-19 Demands Interact with Agile Project Management in Predicting Employee Exhaustion. Br. J. Manag. 2021, 32, 1265–1283. [Google Scholar] [CrossRef]
- Deloite. COVID-19 Workforce Strategies for a Post-COVID-19 Recovery Workbook; Deloitee Development LLC: Toronto, ON, Canada, 2020. [Google Scholar]
- Safapour, E.; Kermanshachi, S.; Kamalirad, S. Analysis of effective project-based communication components within primary stakeholders in construction industry. Built Environ. Proj. Asset Manag. 2020, 11, 157–173. [Google Scholar] [CrossRef]
- McKinsey & Company. Reopening Workplaces: A Collection of Workforce-Protection Interventions; McKinsey & Company: New York, NY, USA, 2020. [Google Scholar]
- Sharma, K.; Deng, L.; Noguez, C.C. Field investigation on the performance of building structures during the April 25, 2015, Gorkha earthquake in Nepal. Eng. Struct. 2016, 121, 61–74. [Google Scholar] [CrossRef]
- Stephany, F.; Stoehr, N.; Darius, P.; Neuhäuser, L.; Teutloff, O.; Braesemann, F. The CoRisk-Index: A data-mining approach to identify industry-specific risk assessments related to COVID-19 in real-time. arXiv 2020, arXiv:2003.12432. [Google Scholar] [CrossRef]
- Cohen, S.; Kamarck, T.; Mermelstein, R. A global measure of perceived stress. J. Health Soc. Behav. 1983, 24, 385–396. [Google Scholar] [CrossRef]
- Remor, E. Psychometric properties of a European Spanish version of the Perceived Stress Scale (PSS). Span. J. Psychol. 2006, 9, 86–93. [Google Scholar] [CrossRef]
- Ribeiro Santiago, P.H.; Nielsen, T.; Smithers, L.G.; Roberts, R.; Jamieson, L. Measuring stress in Australia: Validation of the perceived stress scale (PSS-14) in a national sample. Health Qual. Life Outcomes 2020, 18, 100. [Google Scholar] [CrossRef]
- Foster, K.; Fethney, J.; Kozlowski, D.; Fois, R.; Reza, F.; McCloughen, A. Emotional intelligence and perceived stress of Australian pre-registration healthcare students: A multi-disciplinary cross-sectional study. Nurse Educ. Today 2018, 66, 51–56. [Google Scholar] [CrossRef]
- Denovan, A.; Dagnall, N.; Dhingra, K.; Grogan, S. Evaluating the Perceived Stress Scale among UK university students: Implications for stress measurement and management. Stud. High. Educ. 2019, 44, 120–133. [Google Scholar] [CrossRef]
- Smith, K.J.; Emerson, D.J. An assessment of the psychometric properties of the Perceived Stress Scale-10 (PSS10) with a US public accounting sample. Adv. Account. 2014, 30, 309–314. [Google Scholar] [CrossRef]
- Creswell, J.W. Research Design: Qualitative, Quantitative and Mixed Methods Approaches, 4th ed.; Sage Publications: Atlanta, GA, USA, 2014. [Google Scholar]
- Kumar, R. Research Methodology: A Step-by-Step Guide for Beginners; Sage Publications Limited: London, UK, 2019. [Google Scholar]
- Hair, J.; Hult, T.; Ringle, C.; Sarstedt, M. A Primer on Partial Least Squares Structural Equation Modeling (PLS-SEM); Sage publications: London, UK, 2022. [Google Scholar]
- Cronbach, L. Coefficient alpha and the internal structure of tests. Psychometrika 1951, 16, 297–334. [Google Scholar] [CrossRef]
- DiLalla, L.; Tinsley, H.; Brown, S. Structural Equation Modeling: Uses and Issues’, Handbook of Applied Multivariate Statistics and Mathematical Modeling; Academic Press: Cambridge, MA, USA, 2000. [Google Scholar] [CrossRef]
- Falk, R.F.; Miller, N.B. A Primer for Soft Modeling; University of Akron Press: Akron, OH, USA, 1992. [Google Scholar]
- Anderson, J.; Gerbing, D. Structural equation modeling in practice: A review and recommended two-step approach. Psychol. Bull. 1988, 103, 411. [Google Scholar] [CrossRef]
- Werts, C.; Linn, R.; Jöreskog, K. Intraclass reliability estimates: Testing structural assumptions. Educ. Psychol. Meas. 1974, 34, 25–33. [Google Scholar] [CrossRef]
- Kline, R.B. Principles and Practices of Structural Equation Modeling; Guilford Publications: New York, NY, USA, 2015. [Google Scholar]
- Henseler, J.; Ringle, C.M.; Sarstedt, M. A new criterion for assessing discriminant validity in variance-based structural equation modeling. J. Acad. Mark. Sci. 2015, 43, 115–135. [Google Scholar] [CrossRef]
- Pokhrel, P.; Jin, X.; Osei-Kyei, R.; Alashwal, A. Women’s well-being in construction: A systematic review of hazards and primary preventive measures. Int. J. Constr. Manag. 2026, 1–21. [Google Scholar] [CrossRef]
- Tijani, B.; Jin, X.; Osei-kyei, R. A systematic review of mental stressors in the construction industry. Int. J. Build. Pathol. Adapt. 2020, 39, 433–460. [Google Scholar] [CrossRef]
- Leung, M.Y.; Chan, I.Y. Exploring stressors of Hong Kong expatriate construction professionals in Mainland China: Focus group study. J. Constr. Eng. Manag. 2012, 138, 78–88. [Google Scholar] [CrossRef]
- Bowen, P.; Edwards, P.; Lingard, H.; Cattell, K. Occupational stress and job demand, control and support factors among construction project consultants. Int. J. Proj. Manag. 2014, 32, 1273–1284. [Google Scholar] [CrossRef]
- Love, P.E.; Edwards, D.J. Taking the pulse of UK construction project managers’ health: Influence of job demands, job control and social support on psychological wellbeing. Eng. Constr. Archit. Manag. 2005, 12, 88–101. [Google Scholar] [CrossRef]
- Senaratne, S.; Rasagopalasingam, V. The causes and effects of work stress in construction project managers: The case in Sri Lanka. Int. J. Constr. Manag. 2017, 17, 65–75. [Google Scholar] [CrossRef]
- Lamontagne, A.; Keegel, T.; Vallance, D. Protecting and promoting mental health in the workplace: Developing a systems approach to job stress. Health Promot. J. Aust. 2007, 18, 221–228. [Google Scholar] [CrossRef]


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license.