Abstract
Hypertension frequently remains uncontrolled despite pharmacological therapy, supporting interest in complementary nutritional strategies. This narrative review evaluates human clinical evidence and mechanistic pathways for minerals, polyphenols, omega-3 fatty acids, probiotics, coenzyme Q10, and L-arginine in blood pressure regulation. Across these categories, antihypertensive effects appear to depend largely on post-ingestion metabolic biotransformation into bioactive metabolites that influence endothelial nitric oxide availability, vascular inflammation, renal sodium handling, and renin–angiotensin system activity. Randomized controlled trials and meta-analyses consistently demonstrate modest reductions in systolic blood pressure of approximately 2–8 mmHg, although most studies are short-term and frequently use supplementation models. The overall certainty of evidence is moderate due to consistent but heterogeneous randomized trials. Variability in response is partly explained by metabolic phenotype and gut microbiota composition, and combined dietary patterns targeting multiple mechanisms may produce additive effects. Overall, nutraceuticals function as adjunct physiological modulators that may contribute to cardiovascular risk reduction but are not intended to replace pharmacological therapy. The present review integrates post-ingestion metabolism, microbiota-derived mediators, and clinical trial evidence into a unified physiological framework explaining why consistent but modest blood pressure reductions occur across heterogeneous interventions. Nutritional strategies remain underutilized in routine clinical practice despite reproducible physiological effects. Incorporating evidence-based nutraceutical approaches alongside pharmacological management may facilitate patient engagement with lifestyle modification, as dietary interventions are often perceived as more achievable than isolated behavioral recommendations. A holistic management model integrating medical therapy, nutrition, and patient education may therefore enhance long-term adherence to cardiovascular prevention strategies and support sustained risk reduction.
1. Introduction
Hypertension is a major modifiable risk factor for cardiovascular morbidity and mortality, affecting approximately 1.3 billion adults worldwide according to the World Health Organization [1]. Despite the availability of effective pharmacological therapies, blood pressure control remains inadequate in a substantial proportion of patients. This gap is largely attributable to poor long-term adherence, adverse drug reactions, therapeutic inertia, and the multifactorial pathophysiology of hypertension, in which single-drug therapy often fails to sufficiently reduce residual cardiovascular risk [2]. Consequently, increasing attention has been directed toward complementary preventive strategies that can be integrated with standard treatment.
Current clinical guidelines emphasize lifestyle modification—particularly dietary patterns and physical activity—as first-line management [3,4]. However, lifestyle interventions alone often fail to achieve adequate blood pressure control, especially in individuals with metabolic dysfunction, endothelial impairment, or chronic low-grade inflammation. In this context, nutraceuticals, defined as food-derived compounds providing physiological benefits beyond basic nutrition, have emerged as potential adjunctive therapeutic strategies [5].
Accumulating evidence suggests that several nutraceutical classes influence key biological pathways involved in blood pressure regulation, including endothelial nitric oxide bioavailability, vascular smooth muscle tone, oxidative stress, inflammatory signaling, gut microbiota–host interactions, and the renin–angiotensin–aldosterone system [6]. Importantly, many of these effects depend not only on the ingested compound itself but also on its biotransformation after digestion. Following ingestion, nutrients undergo enzymatic metabolism and microbial bioconversion in the intestine and liver, generating bioactive metabolites—such as short-chain fatty acids, phenolic metabolites, and lipid mediators—that directly modulate vascular, renal, immune, and neurohormonal pathways. Therefore, understanding nutraceutical effects requires a systems perspective integrating digestion, host metabolism, and microbiota-derived metabolomics.
This narrative review evaluates human evidence for nutraceutical approaches to blood pressure control within an integrated mechanistic framework. Rather than examining isolated compounds independently, the review synthesizes findings across five biologically interconnected groups: (1) essential minerals, including magnesium, potassium, calcium, and iodine; (2) polyphenols from tea, cocoa, berries, and plant preparations such as Hibiscus sabdariffa; (3) omega-3 fatty acids; (4) probiotics influencing the gut–vascular axis; and (5) selected bioactive compounds, including coenzyme Q10 and L-arginine [6,7].
By linking molecular mechanisms, metabolic pathways, and clinical outcomes, this review aims to clarify how nutraceuticals may complement pharmacological therapy. Nutraceutical interventions should be regarded as supportive strategies capable of improving vascular physiology and cardiometabolic risk, but not as substitutes for antihypertensive medications. An additional perspective increasingly applied in nutrition science is food metabolomics, which examines small bioactive molecules generated after the digestion and microbial transformation of dietary compounds. Unlike classical nutrient composition analysis, metabolomics focuses on circulating metabolites that directly interact with physiological pathways regulating vascular tone, inflammation, and renal sodium handling. This approach is particularly relevant for nutraceutical research because many dietary compounds—especially polyphenols and microbiota-dependent substrates—exert biological activity primarily through secondary metabolites rather than their native structures. Consequently, variability in blood pressure response reflects differences in metabolic phenotype and gut microbiota composition rather than intake alone. Incorporating a metabolomics framework therefore provides a mechanistic bridge between dietary exposure and the vascular outcomes observed in human studies.
Despite growing interest in nutraceutical approaches, interpretation of the available evidence requires caution. Many clinical trials evaluating nutraceuticals for blood pressure control are relatively short in duration, involve small sample sizes, and frequently rely on supplementation models rather than habitual dietary intake. Differences in study design, dosing strategies, baseline blood pressure, and participant characteristics contribute to considerable heterogeneity across studies, which complicates direct comparison of outcomes. Furthermore, variability in gut microbiota composition, metabolic phenotype, and background diet likely influences the generation of bioactive metabolites and may partly explain inconsistent responses among individuals. Consequently, although mechanistic evidence is biologically plausible and randomized trials generally demonstrate modest blood pressure reductions, the clinical relevance of individual nutraceutical interventions remains context-dependent. Future research should therefore focus on longer-term trials, standardized intervention protocols, and identification of responder phenotypes integrating metabolomic and microbiome-based approaches.
Methods and Literature Search Strategy
This work was conducted as a structured narrative review aimed at integrating mechanistic and clinical evidence regarding nutraceutical interventions in blood pressure regulation.
- Search Strategy
A comprehensive literature search was performed in PubMed/MEDLINE, Web of Science, Scopus, and Food Science and Technology Abstracts (FSTA). Google Scholar was additionally used to identify recently published or in-press articles not yet indexed in primary databases. The search covered publications from January 1990 to December 2025, with greater emphasis placed on studies published after 2010 to ensure contemporary clinical relevance.
Search strategies combined Medical Subject Headings (MeSH) and free-text terms using Boolean operators. The core search terms included combinations of: “hypertension”, “blood pressure”, “nutraceuticals”, “dietary supplements”, “minerals”, “potassium”, “magnesium”, “calcium”, “iodine”, “polyphenols”, “flavonoids”, “omega-3 fatty acids”, “probiotics”, and “Hibiscus sabdariffa”. Additional targeted searches were performed for mechanistic pathways using terms such as “gut microbiota”, “metabolites”, “short-chain fatty acids”, “nitric oxide”, “endothelial function”, and “renin–angiotensin system”.
- Study Selection
Studies were initially screened based on titles and abstracts, followed by full-text evaluation of potentially relevant articles. The initial search yielded 1476 records across databases. After removal of duplicates, 1028 records remained for title and abstract screening. Following screening, 276 full-text articles were assessed for eligibility, of which 132 studies were included in the final synthesis. A summary of nutraceutical compounds and interventions evaluated in the included literature is provided in Supplementary Table S1.
- Inclusion and Exclusion Criteria
Priority was given to randomized controlled trials, systematic reviews, meta-analyses, prospective cohort studies, and clinical practice guidelines evaluating nutraceutical interventions in relation to blood pressure regulation. Mechanistic studies were included when they provided biologically plausible pathways relevant to human blood pressure physiology.
Exclusion criteria included non-human studies without clear translational relevance, conference abstracts without full data, duplicate datasets, publications lacking methodological transparency, and non-English or non-Croatian articles.
- Quality Assessment
Because of the narrative design, a formal quantitative risk-of-bias meta-analysis was not performed. Instead, study quality was assessed qualitatively based on study design hierarchy (randomized trials > observational studies > mechanistic studies), methodological transparency, consistency of findings across studies, and the magnitude and reproducibility of blood pressure effects. Mechanistic studies were used to support biological plausibility, whereas clinical interpretation relied primarily on randomized controlled trials and meta-analyses. Observational studies were considered supportive but not causal evidence.
GenAI tools, namely ChatGPT (GPT-5.5 Thinking, OpenAI) and Gemini 2.0 (Google), were used for manuscript drafting, language editing, and additional retrieval of relevant studies. The authors reviewed and edited all AI-generated output and take full responsibility for the content of the manuscript.
The nutraceutical categories, key compounds, mechanisms, evidence levels, typical blood pressure effects, and clinical considerations are summarized in Table 1.

Table 1.
Nutraceuticals identified to have a potential positive impact on blood pressure control in human studies. Source: Compiled by the authors based on the literature cited.
2. Essential Minerals and Blood Pressure Regulation
Dietary minerals are fundamental regulators of blood pressure homeostasis. Beyond maintaining electrolyte balance, they influence vascular tone, endothelial signaling, renal sodium handling, and neurohormonal control. Importantly, their physiological effects are interdependent rather than isolated; the dietary sodium-to-potassium ratio predicts cardiovascular risk more reliably than sodium intake alone [7]. This highlights that mineral balance, rather than single-nutrient intake, is a major determinant of long-term hemodynamic regulation.
Potassium, magnesium, calcium, and iodine modulate complementary biological pathways governing vascular resistance and fluid balance. These include regulation of the renin–angiotensin–aldosterone system, Na+/K+-ATPase activity, intracellular calcium signaling in vascular smooth muscle cells, and endocrine control mediated by thyroid hormones [8,9]. Through these mechanisms, minerals affect arterial stiffness, endothelial nitric oxide bioavailability, and renal pressure–natriuresis responses.
Unlike many bioactive nutraceuticals whose biological activity depends largely on metabolic derivatives, minerals exert their effects primarily through ionic transport processes and hormonal regulation. Nevertheless, they also interact indirectly with metabolic pathways related to insulin sensitivity, oxidative stress, and inflammatory signaling. Through these mechanisms, minerals influence vascular function and responsiveness to other dietary compounds.
Correction of mineral insufficiency therefore represents a low-risk population-level strategy for improving baseline blood pressure regulation and enhancing the effectiveness of pharmacological therapy. The principal biological pathways through which these minerals influence blood pressure are summarized in Figure 1.
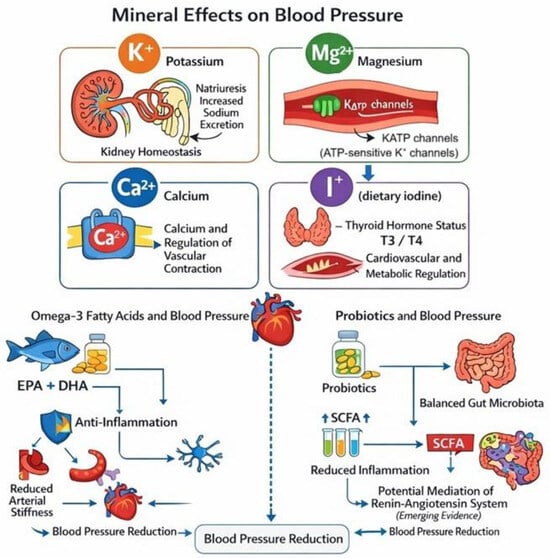
Figure 1.
Conceptual overview of nutritional mechanisms influencing blood pressure regulation. Arrows indicate proposed mechanistic pathways and the direction of physiological effects leading to blood pressure reduction. Dietary minerals such as potassium, magnesium, calcium, and iodine influence vascular tone, renal sodium handling, and endocrine regulation [7,8,9]. Omega-3 fatty acids (EPA and DHA) improve endothelial function, reduce inflammation, and decrease arterial stiffness [10,11,12]. Probiotics may influence blood pressure through modulation of the gut microbiota and production of short-chain fatty acids that affect vascular and inflammatory pathways [13,14,15,16,17]. The figure is an original illustration created by the authors based on mechanisms described in the cited literature.
2.1. Potassium: A Central Dietary Determinant of Blood Pressure
Potassium is one of the most important dietary determinants of blood pressure regulation. Epidemiological and intervention studies consistently show that populations with higher potassium intake—primarily from fruits, vegetables, legumes, and whole grains—have lower blood pressure and a reduced risk of stroke and cardiovascular disease [18,19].
The antihypertensive effects of potassium are mediated through several complementary mechanisms. At the renal level, increased potassium intake promotes natriuresis by suppressing activity of the sodium–chloride cotransporter in the distal convoluted tubule, thereby counteracting sodium-induced volume expansion [19,20]. In the vasculature, potassium stimulates Na+/K+-ATPase activity and activates ATP-sensitive potassium channels in vascular smooth muscle cells, leading to membrane hyperpolarization, reduced intracellular calcium concentration, and consequent vasodilation with decreased peripheral vascular resistance [21].
Clinical evidence supports these mechanisms. A meta-analysis of randomized controlled trials demonstrated significant reductions in both systolic and diastolic blood pressure, particularly in individuals with hypertension and high sodium intake [22]. These findings indicate that potassium primarily restores sodium–potassium balance rather than acting as an isolated pharmacological antihypertensive intervention [23]. However, most intervention trials are relatively short and frequently performed under controlled dietary sodium intake, which limits extrapolation to long-term free-living populations where adherence and baseline diet vary substantially.
Adequate dietary potassium intake is safe and recommended for most individuals; however, supplementation should be used cautiously in patients with advanced chronic kidney disease or in those receiving potassium-sparing diuretics because of the risk of hyperkalemia [24]. Overall, the strength of evidence supporting potassium intake in blood pressure reduction is moderate to high, with consistent findings across randomized trials despite heterogeneity in baseline sodium intake and dietary adherence.
2.2. Magnesium: A Physiological Calcium Antagonist
Magnesium is a predominantly intracellular cation involved in more than 300 enzymatic reactions, including the regulation of vascular smooth muscle tone, endothelial function, and electrolyte homeostasis [25]. Inadequate magnesium intake is common worldwide and has been associated with hypertension, insulin resistance, and metabolic syndrome [26,27].
Magnesium exerts antihypertensive effects primarily through its role as a physiological calcium antagonist. By competing with calcium at voltage-gated calcium channels, magnesium reduces calcium influx into vascular smooth muscle cells, thereby decreasing contractility and lowering peripheral vascular resistance [28,29]. In addition, intracellular magnesium enhances Na+/K+-ATPase activity, helping maintain electrochemical gradients required for vascular relaxation [30]. Beyond direct vascular effects, magnesium improves endothelial function by reducing oxidative stress, increasing nitric oxide bioavailability, and attenuating systemic inflammation, as reflected by reduced circulating C-reactive protein levels [31,32].
Clinical evidence supports these mechanisms. Meta-analyses of randomized controlled trials report modest but clinically meaningful reductions in blood pressure, with average decreases in systolic pressure of approximately 2–4 mmHg, particularly among individuals with hypertension or low baseline magnesium status [33,34]. The heterogeneity of baseline magnesium status across populations likely explains inconsistent responses, and benefits appear greatest in deficiency states rather than in normomagnesemic individuals.
Randomized clinical trials typically administer 240–600 mg/day of elemental magnesium, which appears to represent the most commonly effective dose range for improving blood pressure outcomes. The antihypertensive response also depends on the formulation used. Organic salts such as magnesium citrate, glycinate, or lactate demonstrate greater bioavailability than inorganic forms (e.g., magnesium oxide), which are less efficiently absorbed and more frequently associated with gastrointestinal adverse effects [35]. Overall, available randomized trials suggest consistent but modest blood pressure reductions, with clinical benefits influenced by baseline magnesium status, dose, and formulation.
2.3. Calcium: The Dietary Calcium Paradox
Calcium plays a central role in cardiovascular physiology. Intracellular calcium mediates vascular smooth muscle contraction and vasoconstriction, yet adequate dietary calcium intake has consistently been associated with lower blood pressure in both observational and interventional studies [36]. This apparent contradiction can be explained by endocrine regulation: low dietary calcium intake stimulates parathyroid hormone secretion and activation of the renin–angiotensin–aldosterone system, increasing intracellular calcium concentrations in vascular smooth muscle cells and promoting vasoconstriction [37,38].
Dietary intervention studies, including the DASH trial, demonstrate that calcium-rich dietary patterns significantly reduce blood pressure [18]. Meta-analyses of randomized trials also show modest but statistically significant reductions in blood pressure following calcium supplementation [39].
However, the effects of supplementation differ from those of dietary intake. High-dose calcium supplements, particularly when consumed without adequate vitamin D or magnesium, have been associated with increased vascular calcification and higher cardiovascular risk [40]. This phenomenon, often referred to as the “calcium paradox,” reflects the difference between physiological calcium intake within whole foods and pharmacological supplementation.
Accordingly, current evidence supports achieving recommended calcium intake (approximately 1000–1200 mg/day) primarily through dietary sources such as dairy products, leafy green vegetables, and fortified foods rather than routine high-dose supplementation [41].
2.4. Iodine: Thyroid-Mediated Blood Pressure Regulation
Unlike potassium and magnesium, iodine does not directly exert vasodilatory effects. Its influence on blood pressure occurs indirectly through its essential role in thyroid hormone synthesis. Triiodothyronine (T3) and thyroxine (T4) regulate metabolic rate, cardiac output, systemic vascular resistance, and endothelial function [42].
Both iodine deficiency and excess disrupt thyroid homeostasis and consequently alter blood pressure regulation. Hypothyroidism, commonly associated with inadequate iodine intake, increases peripheral vascular resistance and arterial stiffness, typically leading to diastolic hypertension. In contrast, hyperthyroidism—potentially triggered by excessive iodine exposure—elevates cardiac output and may result in systolic hypertension [43,44]. Thyroid hormones also directly affect vascular physiology, as T3 stimulates endothelial nitric oxide production and promotes vasodilation [45].
Although iodine is not an antihypertensive nutrient per se, maintaining euthyroid status is necessary for normal cardiovascular regulation. Epidemiological evidence suggests a U-shaped relationship between iodine intake and thyroid-related cardiovascular outcomes, with both deficiency and excess associated with adverse hemodynamic profiles [46]. Therefore, clinical recommendations emphasize adequate dietary intake through iodized salt and seafood while avoiding high-dose supplementation that may induce thyroid dysfunction [47,48]. Overall, the evidence is indirect but biologically consistent, indicating moderate certainty through thyroid-mediated hemodynamic regulation rather than direct antihypertensive action.
3. Polyphenols and Blood Pressure Regulation
Polyphenols are a diverse group of plant-derived bioactive compounds widely present in fruits, vegetables, tea, cocoa, and other plant foods. Epidemiological, clinical, and experimental evidence consistently link polyphenol-rich dietary patterns with improved vascular function and modest reductions in blood pressure, particularly in individuals with endothelial dysfunction or elevated cardiometabolic risk [49,50].
Importantly, the biological activity of polyphenols depends predominantly on post-ingestion metabolism rather than the native molecules themselves. After consumption, only a small fraction of intact compounds is absorbed in the small intestine; the majority undergoes intestinal and hepatic phase I/II metabolism followed by extensive microbial catabolism in the colon. This process generates circulating bioactive metabolites, including phenolic acids and other low-molecular-weight derivatives that interact with vascular and immune signaling pathways [51,52]. These metabolites enhance endothelial nitric oxide production, reduce oxidative stress, and attenuate inflammatory signaling, thereby influencing vascular tone and peripheral resistance.
Polyphenols therefore operate through a gut–vascular axis rather than acting solely as direct antioxidants. Microbiota-derived metabolites contribute to endothelial nitric oxide synthase activation, improvement of arterial compliance, and partial inhibition of the renin–angiotensin system [53,54]. Consequently, the magnitude of blood pressure reduction depends not only on intake but also on host metabolic phenotype and gut microbiota composition, explaining substantial interindividual variability in clinical response.
In the following sections, evidence is summarized across major dietary sources with the strongest human data: (1) cocoa flavanols, (2) tea catechins and theaflavins, (3) berry-derived anthocyanins, and (4) polyphenol-rich botanical preparations such as Hibiscus sabdariffa. For each subgroup, mechanistic pathways, randomized controlled trials, and meta-analyses are reviewed to contextualize their role as adjunctive nutraceutical strategies in blood pressure management.
3.1. General Mechanisms of Polyphenol Action in Blood Pressure Regulation
After ingestion, only a small proportion of intact polyphenols is absorbed in the small intestine. Most undergo extensive phase I/II metabolism and subsequent microbial catabolism in the colon, generating low-molecular-weight phenolic metabolites that circulate systemically and interact with vascular signaling pathways [51]. These metabolites function primarily as modulators of cell signaling rather than direct antioxidants.
A central mechanism involves enhancement of endothelial nitric oxide (NO) bioavailability. Polyphenol metabolites activate endothelial nitric oxide synthase through phosphorylation-dependent pathways, improving endothelium-dependent vasodilation and reducing peripheral vascular resistance [55,56]. Because impaired NO signaling is a hallmark of hypertension, restoration of NO homeostasis represents a major pathway linking polyphenol intake to blood pressure reduction.
Polyphenols also influence oxidative balance by inhibiting enzymatic sources of reactive oxygen species, particularly NADPH oxidase, thereby preserving NO from oxidative degradation rather than acting primarily as radical scavengers [50,54]. In parallel, they attenuate vascular inflammation through modulation of nuclear factor κB signaling and cytokine expression [57].
Additional mechanisms contributing to blood pressure control include partial inhibition of angiotensin-converting enzyme activity, modulation of endothelin-1 production, and improvement of insulin sensitivity [54]. Collectively, these pathways indicate that polyphenols influence vascular homeostasis through integrated metabolic and signaling effects mediated by host–microbiota interactions rather than isolated antioxidant activity.
Interindividual variability in the blood pressure response to polyphenol intake is increasingly explained by differences in metabolic phenotype rather than intake alone. Following consumption, gut microbiota convert polyphenols into specific circulating metabolites such as phenyl-γ-valerolactones, urolithins, and various phenolic acids, which correlate more closely with vascular effects than the parent molecules [58]. Individuals differ markedly in their capacity to generate these metabolites due to variation in microbial composition and enzymatic activity. Consequently, dietary polyphenols act as precursor compounds whose antihypertensive efficacy depends on host–microbiome metabolism, providing a mechanistic explanation for heterogeneous outcomes observed across clinical intervention studies [58].
3.2. Cocoa and Flavanols
Cocoa flavanols are among the most extensively studied polyphenols in relation to vascular function and blood pressure regulation. The principal bioactive constituents include (−)-epicatechin, catechin, and oligomeric procyanidins, which after ingestion are metabolized into circulating phenolic metabolites responsible for most vascular effects [59,60].
Mechanistic studies show that cocoa flavanol metabolites enhance nitric oxide bioavailability by activating endothelial nitric oxide synthase and reducing nitric oxide degradation [61]. Both acute and chronic intake of flavanol-rich cocoa improves flow-mediated dilation, a validated non-invasive measure of endothelial function, reflecting increased vasodilatory capacity [62]. Cocoa consumption additionally reduces arterial stiffness and wave reflection, improving central hemodynamics [63].
Randomized controlled trials and meta-analyses consistently demonstrate modest but significant reductions in blood pressure following regular consumption of flavanol-rich cocoa products, particularly in individuals with hypertension or endothelial dysfunction [64,65]. Average reductions in systolic blood pressure of approximately 3–5 mmHg have been reported, a magnitude considered clinically relevant at the population level [66].
The magnitude of benefit depends strongly on flavanol content and processing methods. Many commercial chocolate products contain relatively low flavanol concentrations and high amounts of sugar and saturated fat, which may attenuate potential vascular benefits [67]. Consequently, standardized high-flavanol cocoa preparations are more appropriate when evaluating therapeutic outcomes. Overall, the evidence is moderate-to-high, supported by multiple randomized trials with consistent vascular outcomes.
The chemical structure of (−)-catechin, a representative flavan-3-ol found in cocoa and tea, is shown in Figure 2.
Figure 2.
Chemical structure of (−)-catechin (a flavan-3-ol polyphenol found in cocoa and tea). Source: Catechin.png, public domain, Wikimedia Commons.
3.3. Tea Polyphenols: Green and Black Tea
Tea is one of the most widely consumed beverages worldwide and represents one of the major dietary sources of flavonoids. Green tea is rich in catechins, particularly epigallocatechin gallate (EGCG), whereas black tea contains theaflavins and thearubigins formed through enzymatic oxidation of catechins during processing [68,69]. Despite compositional differences, both green and black tea are associated with improved vascular function and modest reductions in blood pressure.
After ingestion, tea polyphenols undergo extensive intestinal and microbial metabolism, generating circulating phenolic metabolites that mediate much of their biological activity. These metabolites enhance endothelial nitric oxide availability, reduce oxidative stress, and modulate signaling pathways involved in vascular regulation [56,70,71]. EGCG and related metabolites activate endothelial nitric oxide synthase and influence inflammatory signaling, contributing to improved vascular responsiveness.
Observational studies and randomized controlled trials indicate that habitual tea consumption is associated with modest reductions in both systolic and diastolic blood pressure [72]. Meta-analyses of intervention studies report average systolic blood pressure reductions of approximately 2–3 mmHg following regular intake of green or black tea for at least 8–12 weeks [73]. Although modest at the individual level, these reductions may be clinically meaningful at the population level due to the widespread consumption of tea. Overall, the certainty of evidence is moderate due to consistent but modest reductions across heterogeneous populations.
3.4. Berries and Anthocyanins
Berries are a major dietary source of anthocyanins, flavonoids responsible for the red, blue, and purple pigmentation of fruits such as blueberries, strawberries, blackberries, and cherries. Growing evidence links anthocyanin intake with vascular protection [74,75].
Following ingestion, intact anthocyanins display low systemic bioavailability and undergo extensive microbial metabolism into phenolic acids and related metabolites that mediate most biological effects. These metabolites enhance endothelial nitric oxide availability, reduce oxidative stress, and modulate inflammatory signaling pathways involved in vascular dysfunction [52]. In addition to functional changes, anthocyanin-rich interventions are associated with reductions in arterial stiffness and improvements in microvascular function [52].
Randomized controlled trials evaluating whole-berry consumption or anthocyanin supplementation demonstrate modest reductions in blood pressure, particularly in individuals with hypertension or elevated cardiovascular risk [76]. Meta-analyses report average decreases in systolic blood pressure of approximately 2–4 mmHg, with variability depending on dose, duration, and berry source [77]. Collectively, these findings support inclusion of anthocyanin-rich foods within polyphenol-rich dietary patterns aimed at improving vascular health and supporting blood pressure control. The evidence is moderate, with variability largely explained by dose and baseline cardiometabolic risk.
3.5. Hibiscus sabdariffa (Sour Tea): A Polyphenol-Rich Botanical Intervention
Hibiscus sabdariffa is a polyphenol-rich botanical preparation commonly consumed as a herbal infusion (“sour tea”). Similar to other polyphenols, its antihypertensive activity appears to be mediated largely by microbiota-derived phenolic metabolites rather than intact anthocyanins [78]. The plant contains anthocyanins and related phenolic compounds that undergo intestinal and microbial biotransformation to circulating metabolites contributing to vascular effects.
Proposed mechanisms include inhibition of angiotensin-converting enzyme activity, enhancement of endothelial nitric oxide bioavailability, and mild diuretic effects mediated by organic acids and phenolic metabolites. Through these pathways, H. sabdariffa may reduce peripheral vascular resistance and support vascular relaxation.
Human clinical evidence suggests a clinically relevant antihypertensive effect. Meta-analysis of randomized controlled trials demonstrates significant reductions in both systolic and diastolic blood pressure, with systolic reductions commonly in the range of approximately 5–8 mmHg, particularly among individuals with higher baseline blood pressure [79].
4. Omega-3 Fatty Acids
Omega-3 polyunsaturated fatty acids (PUFAs) are dietary lipids with well-established roles in cardiovascular prevention and have been extensively investigated for blood pressure regulation. The principal biologically active omega-3 fatty acids include eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA), mainly derived from marine sources, and α-linolenic acid (ALA), a plant-derived precursor that undergoes limited conversion to long-chain omega-3 fatty acids in humans [80]. Among these, EPA and DHA demonstrate the most consistent antihypertensive effects across mechanistic and clinical studies [10,81].
4.1. Mechanisms Underlying the Antihypertensive Effects of Omega-3 Fatty Acids
Omega-3 fatty acids influence blood pressure through complementary effects on vascular function, inflammation, oxidative stress, and neurohormonal regulation.
A primary mechanism involves improvement of endothelial function through increased NO bioavailability. EPA and DHA incorporate into cell membranes, increasing membrane fluidity and stimulating endothelial nitric oxide synthase activity, thereby enhancing vasodilation and reducing peripheral vascular resistance [10,11].
Omega-3 fatty acids also exert anti-inflammatory actions by altering eicosanoid synthesis and generating specialized pro-resolving mediators such as resolvins and protectins [82]. These mediators attenuate vascular inflammation and endothelial activation, processes strongly linked to increased vascular resistance and hypertension [83]. Concurrently, omega-3 fatty acids reduce oxidative stress and preserve NO availability [84].
Additional hemodynamic effects include reduced arterial stiffness and improved arterial compliance, particularly in large elastic arteries [12,85]. Omega-3 fatty acids may further contribute to blood pressure control through reduced sympathetic activity and modulation of the renin–angiotensin–aldosterone system [10,11].
Following ingestion, omega-3 fatty acids are incorporated into plasma lipoproteins and cellular phospholipids, gradually replacing arachidonic acid and altering downstream signaling pathways. Their biological activity therefore depends on tissue incorporation and formation of lipid mediators rather than acute circulating concentrations. Variability in absorption, baseline fatty acid status, and enzymatic conversion partly explains heterogeneous responses across clinical trials.
4.2. Clinical Evidence for Blood Pressure Reduction
The antihypertensive effects of omega-3 fatty acids have been evaluated in numerous randomized controlled trials and meta-analyses. Early studies demonstrated that fish oil supplementation reduced both systolic and diastolic blood pressure, particularly in untreated hypertension [86].
Subsequent meta-analyses confirm a dose-dependent effect, with average reductions of approximately 4–5 mmHg systolic and 2–3 mmHg diastolic blood pressure among hypertensive participants [87,88]. A large contemporary meta-analysis further supports stronger reductions at higher intake levels [88].
Differences between individual fatty acids have also been observed. DHA appears to exert greater antihypertensive effects than EPA, likely due to stronger influences on arterial stiffness and endothelial function [83].
Observational studies additionally associate habitual fish consumption with lower blood pressure and reduced incidence of hypertension [89]. In contrast, plant-derived ALA demonstrates less consistent effects because conversion to EPA and DHA in humans is limited [80]. Long-term effects remain difficult to determine, as most studies are short-term and rely on supplement interventions rather than sustained dietary consumption. Collectively, randomized trials and meta-analyses indicate a relatively robust level of evidence, showing reproducible dose-related reductions of roughly 4–5 mmHg systolic and 2–3 mmHg diastolic pressure across diverse study populations.
4.3. Safety, Dosage, and Clinical Considerations
Omega-3 fatty acid supplementation is generally well tolerated within recommended intake ranges. Reported adverse effects are typically mild and include gastrointestinal discomfort and a fishy aftertaste. At higher doses, a modest increase in bleeding tendency may occur in susceptible individuals, although clinically significant complications are uncommon [89,90].
Clinical evidence suggests that daily intake of approximately 2–3 g of combined EPA and DHA is most consistently associated with blood pressure reduction, while lower habitual intakes may provide smaller long-term benefits [89]. The response varies according to baseline blood pressure, background diet, genetics, and EPA:DHA ratio [10,11].
The magnitude of blood pressure reduction is also influenced by the underlying dietary context, including sodium intake and baseline cardiometabolic profile. Accordingly, omega-3 fatty acids should be considered an adjunctive nutraceutical strategy that supports vascular health and complements pharmacological therapy rather than replacing antihypertensive medication in established hypertension.
5. Probiotics and the Gut–Vascular Axis
The gut microbiota is increasingly recognized as an important regulator of cardiovascular physiology, influencing blood pressure through interactions among microbial metabolites, host metabolism, immune signaling, and vascular function [13,14]. Growing evidence suggests the existence of a gut–vascular axis, whereby alterations in microbial composition and metabolic activity contribute to the development and progression of hypertension [13,14].
Probiotics—defined as live microorganisms that confer health benefits when administered in adequate amounts—have emerged as potential adjunctive nutraceutical strategies for blood pressure control [15,16]. Their effects are mediated primarily through the production of short-chain fatty acids, modulation of systemic inflammation, and interaction with neurohormonal pathways involved in vascular regulation [17,91].
5.1. Gut Microbiota Dysbiosis and Hypertension
Hypertension is consistently associated with gut microbiota dysbiosis, characterized by reduced microbial diversity and shifts in metabolically relevant bacterial taxa. This includes depletion of short-chain fatty acid (SCFA)–producing genera such as Faecalibacterium, Roseburia, and Bifidobacterium, accompanied by enrichment of potentially pro-inflammatory organisms, including Prevotella, Desulfovibrio, and members of the Enterobacteriaceae family [13]. Observational human studies demonstrate that hypertensive individuals exhibit microbial and inflammatory metabolic profiles distinct from normotensive populations [14].
SCFAs—particularly acetate, propionate, and butyrate—interact with host receptors involved in vascular tone regulation, immune signaling, and renal sodium handling, thereby influencing blood pressure homeostasis [17]. Experimental evidence further supports a causal relationship: transplantation of microbiota from hypertensive donors into normotensive animals increases blood pressure, whereas transfer from normotensive donors exerts protective effects [15].
Collectively, these findings indicate that microbiota alterations are not merely associated with hypertension but may actively contribute to its pathogenesis through metabolite-mediated host–vascular signaling pathways.
5.2. Mechanisms Linking Probiotics to Blood Pressure Regulation
Probiotics may influence blood pressure primarily through the production of short-chain fatty acids (SCFAs), including acetate, propionate, and butyrate, generated during the fermentation of dietary fiber. These metabolites interact with host G-protein–coupled receptors (GPR41 and GPR43) expressed in vascular, renal, and immune tissues, promoting vasodilation and modulating autonomic regulation of vascular tone [14].
A second mechanism involves restoration of intestinal barrier integrity and attenuation of systemic inflammation. Gut dysbiosis increases intestinal permeability, allowing translocation of pro-inflammatory bacterial components such as lipopolysaccharides into the circulation, thereby contributing to endothelial dysfunction and hypertension. Probiotic supplementation has been shown to improve epithelial barrier function, reduce circulating inflammatory markers, and enhance endothelial function [15].
Responses to probiotic supplementation vary among individuals because administered strains interact with an existing microbial ecosystem rather than acting independently. Colonization success, metabolite production, and downstream vascular effects depend on baseline microbiota composition and substrate availability. Consequently, probiotics act as modulators of metabolic networks rather than isolated pharmacological agents, which may explain heterogeneous blood pressure responses observed across clinical trials [17].
Probiotics may also influence neurohormonal regulation. Certain strains generate bioactive peptides capable of inhibiting angiotensin-converting enzyme activity, producing effects comparable to mild dietary ACE inhibition [92]. In addition, modulation of bile acid metabolism and improvements in insulin sensitivity may indirectly support vascular homeostasis and blood pressure regulation [91]. Because these metabolic pathways rely on bacterial fermentation, their vascular effects are influenced by the availability of fermentable dietary substrates, linking probiotic efficacy to concurrent dietary fiber intake.
5.3. Clinical Evidence for Probiotic Interventions
Meta-analyses of randomized controlled trials demonstrate that probiotic supplementation produces modest but statistically significant reductions in blood pressure, averaging approximately 2–4 mmHg systolic and 1–2 mmHg diastolic, with larger effects observed in hypertensive populations [15]. The magnitude of response depends on formulation characteristics, including strain selection, dose, treatment duration, and baseline blood pressure. Multistrain preparations administered for at least 8–12 weeks generally provide more consistent reductions than short-term or single-strain interventions [15].
Clinical efficacy appears to be strain-specific and linked to defined metabolic functions. Lactobacillus helveticus has demonstrated antihypertensive effects attributed to the production of angiotensin-converting enzyme inhibitory peptides [92]. In contrast, Lactobacillus plantarum and Bifidobacterium longum are primarily associated with improved endothelial function and reduced inflammation through enhanced short-chain fatty acid production and restoration of intestinal barrier integrity [17]. Other strains, including Lactobacillus casei and Bifidobacterium breve, may exert indirect metabolic effects such as improved insulin sensitivity and attenuation of systemic inflammatory signaling.
Overall, probiotics appear to act through strain-specific metabolic pathways rather than as interchangeable agents, with efficacy determined by the functional properties of the administered microorganisms. Current data support a contributory role of microbiota-derived metabolites in hypertension pathophysiology, although causality in humans remains uncertain. Consistent but modest blood pressure reductions across heterogeneous trials indicate a moderate level of evidence.
5.4. Limitations and Future Perspectives
Despite encouraging findings, interpretation of current evidence remains limited by substantial heterogeneity in probiotic strains, dosing regimens, treatment duration, participant characteristics, and outcome assessment across studies [93]. In addition, interindividual variability in gut microbiota composition influences treatment response, supporting a potential role for personalized nutritional approaches [17].
Future research should identify specific microbial strains and metabolites most relevant to blood pressure regulation and clarify interactions among probiotics, diet, and host factors. Well-designed long-term randomized controlled trials are required to determine optimal formulations and to define the role of probiotics as adjunctive therapy in hypertension management. Most available trials remain short-term, limiting conclusions regarding sustained blood pressure control.
6. Coenzyme Q10 and L-Arginine
Coenzyme Q10 (CoQ10) and L-arginine are nutraceutical compounds investigated for their potential effects on cardiovascular physiology, particularly endothelial function and oxidative stress regulation [94,95,96]. Although both influence pathways also targeted by antihypertensive medications, they are classified as dietary supplements rather than antihypertensive drugs because they function primarily as endogenous cofactors or metabolic substrates rather than receptor-specific pharmacological agents [5,94].
Mechanistically, both compounds influence blood pressure regulation through mitochondrial function, oxidative stress modulation, and NO signaling. CoQ10 supports mitochondrial electron transport and ATP production and acts as a membrane antioxidant [95,97]. L-arginine is the physiological substrate for endothelial nitric oxide synthase (eNOS), directly supporting NO synthesis and endothelium-dependent vasodilation [94]. Accordingly, these interventions may be particularly relevant in clinical conditions characterized by endothelial dysfunction and oxidative stress, including hypertension [96].
6.1. Coenzyme Q10
Coenzyme Q10 (ubiquinone) is a lipid-soluble component of the mitochondrial electron transport chain essential for oxidative phosphorylation and cellular ATP generation [97,98]. Beyond its bioenergetic role, CoQ10 acts as an endogenous antioxidant, limiting oxidative damage in membranes and lipoproteins and participating in redox cycling with vitamin E [95]. Reduced circulating or tissue CoQ10 concentrations have been described in cardiovascular disease states, including hypertension, suggesting a relationship with endothelial dysfunction and oxidative stress [97].
The antihypertensive effect of CoQ10 is mainly attributed to improved endothelial function and restoration of NO bioavailability. By reducing lipid peroxidation and reactive oxygen species production, CoQ10 preserves NO signaling and enhances endothelium-dependent vasodilation, lowering peripheral vascular resistance [97,99]. Improvements in vascular compliance and myocardial efficiency may further contribute to blood pressure reduction [99].
The highest standard for evidence quality (Cochrane methodology) and systematic reviews report modest but clinically relevant reductions in blood pressure. Meta-analyses typically demonstrate decreases higher effect on systolic blood pressure, especially at lower doses and for prolonged periods [99,100,101]. Earlier small studies reported larger effects, although these findings were not consistently reproduced in more rigorous trials [101]. Overall, current evidence supports CoQ10 as an adjunctive rather than primary antihypertensive therapy.
CoQ10 is generally well tolerated at doses of 100–300 mg/day. Reported adverse effects are mild and typically limited to gastrointestinal discomfort, nausea, and headache, with no consistent evidence of clinically significant hypotension or electrolyte disturbances [102,103]. However, differences in formulation bioavailability and limited long-term outcome data indicate the need for further well-designed trials [100,104]. Overall, the available randomized trials consistently show modest blood pressure reductions compatible with improved endothelial function and oxidative balance, but variability in formulations, baseline cardiovascular status, and study duration limits the strength of inference to a moderate level.
6.2. L-Arginine
L-arginine is a semi-essential amino acid that serves as the primary substrate for endothelial nitric oxide synthase (eNOS) and therefore plays a central role in NO production and vascular homeostasis [94]. Reduced L-arginine availability and impaired NO synthesis are characteristic features of endothelial dysfunction and hypertension, providing a mechanistic rationale for supplementation [94].
Oral L-arginine administration increases NO bioavailability, resulting in improved endothelium-dependent vasodilation, enhanced arterial compliance, and reduced peripheral vascular resistance [105]. In addition to its direct effect on NO synthesis, L-arginine may modulate oxidative stress and inflammatory pathways, thereby supporting endothelial function [106]. It has also been suggested in a systematic review and meta-analysis of randomized controlled trials to influence insulin sensitivity and autonomic regulation, which may indirectly contribute to blood pressure control [106].
Clinical evidence for the antihypertensive effect of L-arginine is heterogeneous but generally supportive. Several randomized controlled trials report reductions in blood pressure, particularly in individuals with hypertension, metabolic syndrome, or endothelial dysfunction [105]. Meta-analyses indicate average decreases of approximately 4–5 mmHg in systolic and 2–3 mmHg in diastolic blood pressure [106,107]. Short intervention duration and small sample sizes in many trials limit certainty regarding long-term clinical effectiveness.
The magnitude of response appears to depend on baseline NO status, administered dose, duration of treatment, and comorbid conditions [107]. Higher doses may cause gastrointestinal discomfort, hypotension in combination with antihypertensive therapy, and should be used cautiously in patients with severe cardiovascular disease or those receiving nitrates or phosphodiesterase-5 inhibitors [108]. Because oral bioavailability of L-arginine is limited by metabolism, alternative strategies targeting the same pathway, such as L-citrulline supplementation, have been proposed to provide more sustained increases in systemic arginine availability [109]. Overall, randomized trials suggest a reproducible but modest blood pressure reduction consistent with enhanced nitric oxide availability; however, differences in baseline endothelial function, dosing strategies, and short treatment durations limit confidence in sustained long-term benefit.
6.3. Summary
In summary, coenzyme Q10 and L-arginine represent complementary nutraceutical approaches targeting distinct physiological pathways involved in blood pressure regulation. Coenzyme Q10 primarily influences mitochondrial bioenergetics and cellular redox balance, thereby supporting endothelial function, whereas L-arginine serves as a substrate for nitric oxide synthesis and promotes endothelium-dependent vasodilation. Clinical studies suggest modest reductions in blood pressure, particularly in individuals with impaired endothelial function or increased oxidative stress. However, heterogeneity in study design, dosing regimens, and patient populations limits definitive conclusions. Larger, well-controlled, long-term randomized trials are required to clarify their durability of effect and their role as adjunctive strategies within evidence-based hypertension management.
7. Nutrients Influencing Endothelial Function and the Renin–Angiotensin System (RAS)
As discussed above, hypertension results from coordinated dysregulation of vascular, renal, inflammatory, and neurohormonal pathways rather than a single defect. Reduced NO bioavailability, increased oxidative stress, and chronic activation of the renin–angiotensin system (RAS) interact to maintain elevated vascular resistance. Angiotensin II promotes vasoconstriction, inflammation, and reactive oxygen species production, which further impairs endothelial signaling and perpetuates blood pressure elevation [110,111,112].
Across the nutraceutical categories discussed in this review, most compounds do not function as direct vasodilators but instead influence upstream regulatory pathways. Their activity commonly depends on metabolic transformation into secondary bioactive molecules—including phenolic metabolites, short-chain fatty acids, and lipid mediators—that simultaneously affect endothelial signaling, renal sodium handling, immune activation, and neurohormonal regulation [14,82]. This systems-level modulation provides a mechanistic basis for the small but consistent reductions in blood pressure observed across intervention studies.
7.1. Endothelial Function as a Target for Nutraceutical Intervention
Endothelial dysfunction, characterized by impaired NO signaling and increased oxidative stress, represents a central feature of hypertension [110,113]. Excess reactive oxygen species reduce NO availability and promote a pro-inflammatory vascular phenotype [114].
The nutraceutical groups reviewed converge on restoration of endothelial redox balance through complementary mechanisms. Minerals influence vascular smooth muscle excitability and intracellular calcium handling [113,115], polyphenol metabolites enhance endothelial signaling and limit oxidative nitric oxide degradation [51,116], and omega-3 fatty acids modify membrane lipid composition while generating anti-inflammatory lipid mediators [10,82]. In parallel, microbiota-derived metabolites modulate vascular tone and inflammatory activity [14,15], whereas coenzyme Q10 supports mitochondrial redox homeostasis [95]. Together, these mechanisms support improved endothelial function despite modest individual blood pressure reductions [117].
Accordingly, convergent improvement in endothelial function provides a plausible explanation for the reproducible, though limited, blood pressure reductions reported across randomized trials and meta-analyses.
7.2. Nutritional Modulation of the Renin–Angiotensin System
The RAS regulates vascular tone and extracellular fluid balance. Chronic overactivation contributes to vasoconstriction, sodium retention, oxidative stress, and vascular remodeling [111,117]. Nutraceuticals influence this system mainly through regulatory modulation rather than pharmacological blockade.
Potassium improves renal sodium handling and suppresses renin release [113].
Magnesium affects vascular tone and insulin signaling, indirectly influencing RAS activity [115].
Polyphenol metabolites and fermentation-derived peptides exhibit mild ACE-inhibitory activity [51,92].
Omega-3 fatty acids attenuate angiotensin II–associated inflammation and oxidative stress [10,83].
Together, these actions support attenuation of excessive RAS signaling rather than complete inhibition.
7.3. Integrated Effects on Vascular Remodeling and Blood Pressure
A common feature across nutraceutical interventions is dependence on metabolic activation. Many compounds exert biological effects through metabolites generated by host enzymes or gut microbiota rather than the ingested molecules themselves [51,90]. Consequently, identical intake may produce different circulating metabolite profiles among individuals, contributing to heterogeneous clinical responses.
This variability highlights the importance of metabolic phenotype and microbiota composition in determining treatment efficacy and supports integration of metabolomics- and microbiome-based approaches in future clinical research [118,119].
7.4. Clinical and Translational Implications
As stated already, lifestyle modification remains first-line therapy for hypertension, yet long-term control is frequently inadequate [120]. The mechanisms described above indicate that nutraceuticals are most relevant as adjunctive interventions in individuals with endothelial dysfunction, metabolic inflammation, or residual cardiovascular risk despite standard therapy [4].
Average reductions in blood pressure associated with nutraceutical intake are small at the individual level but may be clinically meaningful at the population level [117]. For that reason, future trials should focus on standardized formulations, longer follow-up, and identification of responder phenotypes [117,118].
7.5. Integrated Mechanistic Summary
Nutraceuticals influence blood pressure through coordinated modulation of endothelial signaling, oxidative stress, renal sodium handling, and RAS activity. Their effects depend largely on metabolic and microbiota-derived mediators, producing gradual improvements in vascular homeostasis rather than acute pharmacological vasodilation [14,110]. Accordingly, they should be considered complementary components of comprehensive cardiovascular risk management.
8. Conclusions
Hypertension remains insufficiently controlled in many patients despite effective pharmacological therapy, highlighting the importance of complementary preventive strategies. Evidence from randomized trials and meta-analyses indicates that several nutraceutical categories—including minerals, polyphenols, omega-3 fatty acids, probiotics, coenzyme Q10, and L-arginine—produce modest but consistent reductions in blood pressure, typically in the range of 2–8 mmHg. Although these effects are relatively small at the individual level, they may contribute to meaningful cardiovascular risk reduction at the population level when combined with established lifestyle interventions.
Current evidence suggests that nutraceuticals act primarily as physiological modulators influencing endothelial function, inflammation, oxidative stress, and neurohormonal regulation rather than as direct pharmacological antihypertensive agents. However, heterogeneity in study design, dosing strategies, and formulations limits precise clinical recommendations. Future research should prioritize standardized intervention protocols, longer follow-up periods, and identification of responder phenotypes using microbiome and metabolomic approaches. Overall, nutraceuticals should be considered supportive components of comprehensive cardiovascular risk management alongside pharmacological therapy and lifestyle modification.
Supplementary Materials
The following supporting information can be downloaded at: https://www.mdpi.com/article/10.3390/nutraceuticals6020036/s1, Table S1. Summary of nutraceutical compounds and interventions with potential effects on blood pressure regulation, including mechanisms, typical doses, blood pressure effects, evidence level, microbiota involvement, and key clinical considerations.
Author Contributions
Conceptualization, T.V. and I.B.; methodology, T.V. and I.B.; validation, I.B., V.B.S., M.F.K. and V.Y.W.; investigation, T.V.; resources, T.V. and I.B.; data curation, T.V.; writing—original draft preparation, T.V.; writing—review and editing, T.V., V.B.S., M.F.K., V.Y.W. and I.B.; visualization, T.V.; supervision, I.B.; project administration, I.B. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
No new data were created or analyzed in this study. Data sharing is not applicable to this article.
Acknowledgments
During the preparation of this manuscript, the authors used ChatGPT (GPT-5.5 Thinking, OpenAI) and Gemini 2.0 (Google) for the purposes of manuscript drafting, language editing, and additional retrieval of relevant studies. The authors have reviewed and edited the output and take full responsibility for the content of this publication.
Conflicts of Interest
The authors declare no conflict of interest.
Abbreviations
| ACE | Angiotensin-converting enzyme |
| BP | Blood pressure |
| CoQ10 | Coenzyme Q10 |
| DASH | Dietary Approaches to Stop Hypertension |
| DHA | Docosahexaenoic acid |
| eNOS | Endothelial nitric oxide synthase |
| EPA | Eicosapentaenoic acid |
| NO | Nitric oxide |
| PUFA | Polyunsaturated fatty acid |
| RAAS | Renin–angiotensin–aldosterone system |
| RAS | Renin–angiotensin system |
| RCT | Randomized controlled trial |
| ROS | Reactive oxygen species |
| SCFA | Short-chain fatty acid |
| WHO | World Health Organization |
References
- World Health Organization. Global Report on Hypertension: The Race Against a Silent Killer; World Health Organization: Geneva, Switzerland, 2023; Available online: https://www.who.int/publications/i/item/9789240081062 (accessed on 14 December 2025).
- Burnier, M.; Egan, B.M. Adherence in hypertension: A review of prevalence, risk factors, impact and management. Circ. Res. 2019, 124, 1124–1140. [Google Scholar] [CrossRef]
- Williams, B.; Mancia, G.; Spiering, W.; Agabiti Rosei, E.; Azizi, M.; Burnier, M.; Clement, D.L.; Coca, A.; de Simone, G.; Dominiczak, A.; et al. 2018 ESC/ESH Guidelines for the management of arterial hypertension. Eur. Heart J. 2018, 39, 3021–3104. [Google Scholar] [CrossRef] [PubMed]
- Whelton, P.K.; Carey, R.M.; Aronow, W.S.; Casey, D.E., Jr.; Collins, K.J.; Dennison Himmelfarb, C.; DePalma, S.M.; Gidding, S.; Jamerson, K.A.; Jones, D.W.; et al. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Hypertension 2018, 71, 1269–1324. [Google Scholar] [CrossRef]
- Kalra, E.K. Nutraceutical—Definition and introduction. AAPS PharmSci 2003, 5, E25. [Google Scholar] [CrossRef] [PubMed]
- Malinowski, B.; Fajardo Leighton, R.I.; Hill, C.G.; Szandorowski, P.; Wiciński, M. Bioactive Compounds and Their Effect on Blood Pressure—A Review. Nutrients 2020, 12, 1659. [Google Scholar] [CrossRef] [PubMed]
- Behers, B.J.; Melchor, J.; Behers, B.M.; Meng, Z.; Swanson, P.J.; Paterson, H.I.; Mendez Araque, S.J.; Davis, J.L.; Gerhold, C.J.; Shah, R.S.; et al. Vitamins and Minerals for Blood Pressure Reduction in the General, Normotensive Population: A Systematic Review and Meta-Analysis of Six Supplements. Nutrients 2023, 15, 4223. [Google Scholar] [CrossRef]
- Houston, M.C. The role of magnesium in hypertension and cardiovascular disease. J. Clin. Hypertens. 2011, 13, 843–847. [Google Scholar] [CrossRef]
- Weaver, C.M.; Heaney, R.P. Calcium in Human Health; Humana Press: Totowa, NJ, USA, 2006. [Google Scholar]
- Mozaffarian, D.; Wu, J.H.Y. Omega-3 fatty acids and cardiovascular disease: Effects on risk factors, molecular pathways, and clinical events. J. Am. Coll. Cardiol. 2011, 58, 2047–2067. [Google Scholar] [CrossRef]
- Calder, P.C. n-3 fatty acids and cardiovascular disease: Evidence explained and mechanisms explored. Clin. Sci. 2004, 107, 1–11. [Google Scholar] [CrossRef]
- Yates, C.M.; Calder, P.C.; Rainger, G.E. Pharmacology and therapeutics of omega-3 polyunsaturated fatty acids in chronic inflammatory disease. Pharmacol. Ther. 2014, 141, 272–282. [Google Scholar] [CrossRef]
- Gomes, A.C.; Hoffmann, C.; Mota, J.F. The human gut microbiota: Metabolism and perspective in obesity. Gut Microbes 2018, 9, 308–325. [Google Scholar] [CrossRef] [PubMed]
- Tilg, H.; Zmora, N.; Adolph, T.E.; Elinav, E. The intestinal microbiota fuelling metabolic inflammation. Nat. Rev. Immunol. 2020, 20, 40–54. [Google Scholar] [CrossRef] [PubMed]
- Khalesi, S.; Sun, J.; Buys, N.; Jayasinghe, R. Effect of probiotics on blood pressure: A systematic review and meta-analysis of randomized, controlled trials. Hypertension 2014, 64, 897–903. [Google Scholar] [CrossRef] [PubMed]
- O’Toole, P.W.; Marchesi, J.R.; Hill, C. Next-generation probiotics: From probiotics to live biotherapeutics. Nat. Microbiol. 2017, 2, 17057. [Google Scholar] [CrossRef]
- Zmora, N.; Suez, J.; Elinav, E. You are what you eat: Diet, health, and the gut microbiota. Nat. Rev. Gastroenterol. Hepatol. 2019, 16, 35–56. [Google Scholar] [CrossRef]
- Appel, L.J.; Moore, T.J.; Obarzanek, E.; Vollmer, W.M.; Svetkey, L.P.; Sacks, F.M.; Bray, G.A.; Vogt, T.M.; Cutler, J.A.; Windhauser, M.M.; et al. A clinical trial of the effects of dietary patterns on blood pressure. N. Engl. J. Med. 1997, 336, 1117–1124. [Google Scholar] [CrossRef]
- Mente, A.; O’Donnell, M.J.; Rangarajan, S.; McQueen, M.J.; Poirier, P.; Wielgosz, A.; Morrison, H.; Li, W.; Wang, X.; Di, C.; et al. Association of urinary sodium and potassium excretion with blood pressure. N. Engl. J. Med. 2014, 371, 601–611. [Google Scholar] [CrossRef]
- Hall, J.E. The kidney, hypertension, and obesity. Hypertension 2003, 41, 625–633. [Google Scholar] [CrossRef]
- Haddy, F.J.; Vanhoutte, P.M.; Feletou, M. Role of potassium in regulating blood flow and blood pressure. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2006, 290, R546–R552. [Google Scholar] [CrossRef]
- Filippini, T.; Violi, F.; D’Amico, R.; Vinceti, M. The effect of potassium supplementation on blood pressure in hypertensive subjects: A systematic review and meta-analysis. Int. J. Cardiol. 2017, 230, 127–135. [Google Scholar] [CrossRef]
- Aaron, K.J.; Sanders, P.W. Role of dietary salt and potassium intake in cardiovascular health and disease: A review of the evidence. Mayo Clin. Proc. 2013, 88, 987–995. [Google Scholar] [CrossRef]
- Palmer, B.F.; Clegg, D.J. Physiology and pathophysiology of potassium homeostasis. Adv. Physiol. Educ. 2016, 40, 480–490. [Google Scholar] [CrossRef]
- de Baaij, J.H.F.; Hoenderop, J.G.J.; Bindels, R.J.M. Magnesium in man: Implications for health and disease. Physiol. Rev. 2015, 95, 1–46. [Google Scholar] [CrossRef]
- Rosanoff, A.; Weaver, C.M.; Rude, R.K. Suboptimal magnesium status in the United States: Are the health consequences underestimated? Nutr. Rev. 2012, 70, 153–164. [Google Scholar] [CrossRef] [PubMed]
- Del Gobbo, L.C.; Imamura, F.; Wu, J.H.Y.; de Oliveira Otto, M.C.; Chiuve, S.E.; Mozaffarian, D. Circulating and dietary magnesium and risk of cardiovascular disease: A systematic review and meta-analysis of prospective studies. Am. J. Clin. Nutr. 2013, 98, 160–173. [Google Scholar] [CrossRef] [PubMed]
- Touyz, R.M. Role of magnesium in the pathogenesis of hypertension. Mol. Asp. Med. 2003, 24, 107–136. [Google Scholar] [CrossRef] [PubMed]
- Sontia, B.; Touyz, R.M. Role of magnesium in hypertension. Arch. Biochem. Biophys. 2007, 458, 33–39. [Google Scholar] [CrossRef]
- Altura, B.M.; Altura, B.T. Role of magnesium in patho-physiological processes and the clinical utility of magnesium ion selective electrodes. Scand. J. Clin. Lab. Invest. 1996, 56, 211–234. [Google Scholar] [CrossRef]
- Maier, J.A.M. Low magnesium and atherosclerosis: An evidence-based link. Mol. Asp. Med. 2003, 24, 137–146. [Google Scholar] [CrossRef]
- Dibaba, D.T.; Xun, P.; He, K. Dietary magnesium intake is inversely associated with serum C-reactive protein levels: Meta-analysis and systematic review. Eur. J. Clin. Nutr. 2014, 68, 510–516. [Google Scholar] [CrossRef]
- Zhang, X.; Li, Y.; Del Gobbo, L.C.; Rosanoff, A.; Wang, J.; Zhang, W.; Song, Y. Effects of magnesium supplementation on blood pressure: A meta-analysis of randomized double-blind placebo-controlled trials. Hypertension 2016, 68, 324–333. [Google Scholar] [CrossRef]
- Kass, L.; Weekes, J.; Carpenter, L. Effect of magnesium supplementation on blood pressure: A meta-analysis. Eur. J. Clin. Nutr. 2012, 66, 411–418. [Google Scholar] [CrossRef] [PubMed]
- Ranade, V.V.; Somberg, J.C. Bioavailability and pharmacokinetics of magnesium after administration of magnesium salts to humans. Am. J. Ther. 2001, 8, 345–357. [Google Scholar] [CrossRef]
- Jayedi, A.; Zargar, M.S. Dietary calcium intake and hypertension risk: A dose-response meta-analysis of prospective cohort studies. Eur. J. Clin. Nutr. 2019, 73, 969–978. [Google Scholar] [CrossRef] [PubMed]
- Blaustein, M.P.; Lederer, W.J. Sodium/calcium exchange: Its physiological implications. Physiol. Rev. 1999, 79, 763–854. [Google Scholar] [CrossRef]
- Resnick, L.M. Calcium metabolism in hypertension and allied metabolic disorders. Diabetes Care 1991, 14, 505–520. [Google Scholar] [CrossRef] [PubMed]
- van Mierlo, L.A.J.; Arends, L.R.; Streppel, M.T.; Zeegers, M.P.A.; Kok, F.J.; Grobbee, D.E.; Geleijnse, J.M. Blood pressure response to calcium supplementation: A meta-analysis of randomized controlled trials. J. Hum. Hypertens. 2006, 20, 571–580. [Google Scholar] [CrossRef]
- Bolland, M.J.; Grey, A.; Avenell, A.; Gamble, G.D.; Reid, I.R. Calcium supplements with or without vitamin D and risk of cardiovascular events: Reanalysis of the Women’s Health Initiative limited access dataset and meta-analysis. BMJ 2011, 342, d2040. [Google Scholar] [CrossRef]
- Dickinson, H.O.; Nicolson, D.J.; Cook, J.V.; Campbell, F.; Beyer, F.R.; Ford, G.A.; Mason, J. Calcium supplementation for the management of primary hypertension in adults. Cochrane Database Syst. Rev. 2006, CD004639. [Google Scholar] [CrossRef]
- Laurberg, P.; Cerqueira, C.; Ovesen, L.; Rasmussen, L.B.; Perrild, H.J.; Andersen, S.; Pedersen, I.B.; Carlé, A. Iodine intake as a determinant of thyroid disorders in populations. Best Pract. Res. Clin. Endocrinol. Metab. 2010, 24, 13–27. [Google Scholar] [CrossRef]
- Danzi, S.; Klein, I. Thyroid hormone and the cardiovascular system. Med. Clin. N. Am. 2012, 96, 203–218. [Google Scholar] [CrossRef]
- Biondi, B.; Cooper, D.S. The clinical significance of subclinical thyroid dysfunction. Endocr. Rev. 2008, 29, 76–131. [Google Scholar] [CrossRef]
- Napoli, R.; Guardasole, V.; Angelini, V.; Zarra, E.; Terracciano, D.; D’Anna, C.; Matarazzo, M.; Oliviero, U.; Macchia, V.; Saccà, L. Acute effects of triiodothyronine on endothelial function in human subjects. J. Clin. Endocrinol. Metab. 2007, 92, 250–254. [Google Scholar] [CrossRef] [PubMed]
- Taylor, P.N.; Albrecht, D.; Scholz, A.; Gutierrez-Buey, G.; Lazarus, J.H.; Dayan, C.M.; Okosieme, O.E. Global epidemiology of hyperthyroidism and hypothyroidism. Nat. Rev. Endocrinol. 2018, 14, 301–316. [Google Scholar] [CrossRef] [PubMed]
- Leung, A.M.; Braverman, L.E. Consequences of excess iodine. Nat. Rev. Endocrinol. 2014, 10, 136–142. [Google Scholar] [CrossRef] [PubMed]
- Zimmermann, M.B.; Boelaert, K. Iodine deficiency and thyroid disorders. Lancet Diabetes Endocrinol. 2015, 3, 286–295. [Google Scholar] [CrossRef]
- Del Rio, D.; Rodriguez-Mateos, A.; Spencer, J.P.E.; Tognolini, M.; Borges, G.; Crozier, A. Dietary polyphenolics in human health: Structures, bioavailability, and evidence of protective effects. Antioxid. Redox Signal. 2013, 18, 1818–1892. [Google Scholar] [CrossRef]
- Vauzour, D.; Rodriguez-Mateos, A.; Corona, G.; Oruna-Concha, M.J.; Spencer, J.P.E. Polyphenols and human health: Prevention of disease and mechanisms of action. Nutrients 2010, 2, 1106–1131. [Google Scholar] [CrossRef]
- Williamson, G.; Clifford, M.N. Role of the small intestine, colon and microbiota in determining the metabolic fate of polyphenols. Biochem. Pharmacol. 2017, 139, 24–39. [Google Scholar] [CrossRef]
- Rodriguez-Mateos, A.; Rendeiro, C.; Bergillos-Meca, T.; Tabatabaee, S.; George, T.W.; Heiss, C.; Spencer, J.P.E. Intake and time dependence of blueberry flavonoid-induced improvements in vascular function: A randomized, controlled, double-blind, crossover intervention study with mechanistic insights into biological activity. Am. J. Clin. Nutr. 2013, 98, 1179–1191. [Google Scholar] [CrossRef]
- Actis-Goretta, L.; Ottaviani, J.I.; Fraga, C.G. Inhibition of angiotensin-converting enzyme activity by flavanol-rich foods. J. Agric. Food Chem. 2006, 54, 229–234. [Google Scholar] [CrossRef]
- Förstermann, U.; Xia, N.; Li, H. Roles of vascular oxidative stress and nitric oxide in the pathogenesis of atherosclerosis. Circ. Res. 2017, 120, 713–735. [Google Scholar] [CrossRef] [PubMed]
- Heiss, C.; Kleinbongard, P.; Dejam, A.; Perré, S.; Schroeter, H.; Sies, H.; Kelm, M. Acute consumption of flavanol-rich cocoa and the reversal of endothelial dysfunction in smokers. J. Am. Coll. Cardiol. 2005, 46, 1277–1283. [Google Scholar] [CrossRef] [PubMed]
- Schroeter, H.; Heiss, C.; Balzer, J.; Kleinbongard, P.; Keen, C.L.; Hollenberg, N.K.; Sies, H.; Kwik-Uribe, C.; Schmitz, H.H.; Kelm, M. (–)-Epicatechin mediates beneficial effects of flavanol-rich cocoa on vascular function in humans. Proc. Natl. Acad. Sci. USA 2006, 103, 1024–1029. [Google Scholar] [CrossRef] [PubMed]
- González-Gallego, J.; García-Mediavilla, M.V.; Sánchez-Campos, S.; Tuñón, M.J. Fruit polyphenols, immunity and inflammation. Br. J. Nutr. 2010, 104, S15–S27. [Google Scholar] [CrossRef]
- Rodriguez-Mateos, A.; Vauzour, D.; Krueger, C.G.; Shanmuganayagam, D.; Reed, J.; Calani, L.; Mena, P.; Del Rio, D.; Crozier, A. Bioavailability, bioactivity and impact on health of dietary flavonoids and related compounds: An update. Arch. Toxicol. 2014, 88, 1803–1853. [Google Scholar] [CrossRef]
- Katz, D.L.; Doughty, K.; Ali, A. Cocoa and chocolate in human health and disease. Antioxid. Redox Signal. 2011, 15, 2779–2811. [Google Scholar] [CrossRef]
- Fraga, C.G.; Oteiza, P.I. Dietary flavonoids: Role of (–)-epicatechin and related procyanidins in cell signaling. Free Radic. Biol. Med. 2011, 51, 813–823. [Google Scholar] [CrossRef]
- Heiss, C.; Dejam, A.; Kleinbongard, P.; Schewe, T.; Sies, H.; Kelm, M. Vascular effects of cocoa rich in flavan-3-ols. JAMA 2003, 290, 1030–1031. [Google Scholar] [CrossRef]
- Grassi, D.; Necozione, S.; Lippi, C.; Croce, G.; Valeri, L.; Pasqualetti, P.; Desideri, G.; Blumberg, J.B.; Ferri, C. Cocoa reduces blood pressure and insulin resistance and improves endothelium-dependent vasodilation in hypertensives. Hypertension 2005, 46, 398–405. [Google Scholar] [CrossRef]
- Vlachopoulos, C.; Aznaouridis, K.; Alexopoulos, N.; Economou, E.; Andreadou, I.; Stefanadis, C. Effect of dark chocolate on arterial function in healthy individuals. Am. J. Hypertens. 2005, 18, 785–791. [Google Scholar] [CrossRef] [PubMed]
- Ried, K.; Fakler, P.; Stocks, N.P. Effect of cocoa on blood pressure. Cochrane Database Syst. Rev. 2017, 4, CD008893. [Google Scholar] [CrossRef]
- Hooper, L.; Kay, C.; Abdelhamid, A.; Kroon, P.A.; Cohn, J.S.; Rimm, E.B.; Cassidy, A. Effects of chocolate, cocoa, and flavan-3-ols on cardiovascular health: A systematic review and meta-analysis of randomized trials. Am. J. Clin. Nutr. 2012, 95, 740–751. [Google Scholar] [CrossRef]
- Ried, K.; Sullivan, T.; Fakler, P.; Frank, O.R.; Stocks, N.P. Does chocolate reduce blood pressure? A meta-analysis. BMC Med. 2010, 8, 39. [Google Scholar] [CrossRef]
- Cooper, K.A.; Donovan, J.L.; Waterhouse, A.L.; Williamson, G. Cocoa and health: A decade of research. Br. J. Nutr. 2008, 99, 1–11. [Google Scholar] [CrossRef]
- Cabrera, C.; Artacho, R.; Giménez, R. Beneficial effects of green tea—A review. J. Am. Coll. Nutr. 2006, 25, 79–99. [Google Scholar] [CrossRef]
- Deka, A.; Vita, J.A. Tea and cardiovascular disease. Pharmacol. Res. 2011, 64, 136–145. [Google Scholar] [CrossRef]
- Lorenz, M. Cellular targets for the beneficial action of tea polyphenols. Am. J. Clin. Nutr. 2013, 98, 1642S–1650S. [Google Scholar] [CrossRef]
- Kim, W.; Jeong, M.H.; Cho, S.H.; Yun, K.H.; Chae, H.J.; Ahn, Y.; Lee, M.C.; Cheng, X.; Kondo, T.; Murohara, T.; et al. Effect of green tea consumption on endothelial function and circulating endothelial progenitor cells in chronic smokers. Circ. J. 2006, 70, 1052–1057. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.; Lu, F.H.; Wu, J.S.; Wu, C.H.; Chang, C.J. The protective effect of habitual tea consumption on hypertension. Arch. Intern. Med. 2004, 164, 1534–1540. [Google Scholar] [CrossRef] [PubMed]
- Liu, G.; Mi, X.N.; Zheng, X.X.; Xu, Y.L.; Lu, J.; Huang, X.H. Effects of tea intake on blood pressure: A meta-analysis of randomised controlled trials. Br. J. Nutr. 2014, 112, 1043–1054. [Google Scholar] [CrossRef]
- He, J.; Giusti, M.M. Anthocyanins: Natural colorants with health-promoting properties. Annu. Rev. Food Sci. Technol. 2010, 1, 163–187. [Google Scholar] [CrossRef]
- Wallace, T.C. Anthocyanins in cardiovascular disease. Adv. Nutr. 2011, 2, 1–7. [Google Scholar] [CrossRef]
- Curtis, P.J.; van der Velpen, V.; Berends, L.; Jennings, A.; Haag, L.; Chandra, P.; Kay, C.D.; Rimm, E.B.; Cassidy, A. Blueberries improve biomarkers of cardiometabolic function in participants with metabolic syndrome—Results from a 6-month, double-blind, randomized controlled trial. Am. J. Clin. Nutr. 2019, 109, 1535–1545. [Google Scholar] [CrossRef]
- Zhu, Y.; Bo, Y.; Wang, X.; Lu, W.; Wang, X.; Han, Z.; Qiu, C. The effect of anthocyanins on blood pressure: A PRISMA-compliant meta-analysis of randomized clinical trials. Medicine 2016, 95, e3380. [Google Scholar] [CrossRef]
- Hopkins, A.L.; Lamm, M.G.; Funk, J.L.; Ritenbaugh, C. Hibiscus sabdariffa L. in the treatment of hypertension and hyperlipidemia: A comprehensive review of animal and human studies. Fitoterapia 2013, 85, 84–94. [Google Scholar] [CrossRef] [PubMed]
- Serban, C.; Sahebkar, A.; Ursoniu, S.; Andrica, F.; Banach, M. Effect of sour tea (Hibiscus sabdariffa L.) on arterial hypertension: A systematic review and meta-analysis of randomized controlled trials. J. Hypertens. 2015, 33, 1119–1127. [Google Scholar] [CrossRef] [PubMed]
- Burdge, G.C.; Calder, P.C. Conversion of α-linolenic acid to longer-chain polyunsaturated fatty acids in human adults. Reprod. Nutr. Dev. 2005, 45, 581–597. [Google Scholar] [CrossRef]
- Zhang, X.; Ritonja, J.A.; Zhou, N.; Chen, B.E.; Li, X. Omega-3 Polyunsaturated Fatty Acids Intake and Blood Pressure: A Dose-Response Meta-Analysis of Randomized Controlled Trials. J. Am. Heart Assoc. 2022, 11, e025071. [Google Scholar] [CrossRef] [PubMed]
- Calder, P.C. Omega-3 fatty acids and inflammatory processes. Nutrients 2010, 2, 355–374. [Google Scholar] [CrossRef]
- Choi, G.Y.; Calder, P.C. The differential effects of eicosapentaenoic acid and docosahexaenoic acid on cardiovascular risk factors: An updated systematic review of randomized controlled trials. Front. Nutr. 2024, 11, 1423228. [Google Scholar] [CrossRef] [PubMed]
- Harris, W.S.; Dayspring, T.D.; Moran, T.J. Omega-3 fatty acids and cardiovascular disease: New developments and applications. Postgrad. Med. 2013, 125, 100–113. [Google Scholar] [CrossRef] [PubMed]
- Nestel, P.J.; Shige, H.; Pomeroy, S.; Cehun, M.; Abbey, M.; Raederstorff, D. The n−3 fatty acids eicosapentaenoic acid and docosahexaenoic acid increase systemic arterial compliance in humans. Am. J. Clin. Nutr. 2002, 76, 326–330. [Google Scholar] [CrossRef]
- Geleijnse, J.M.; Giltay, E.J.; Grobbee, D.E.; Donders, A.R.T.; Kok, F.J. Blood pressure response to fish oil supplementation: Metaregression analysis of randomized trials. J. Hypertens. 2002, 20, 1493–1499. [Google Scholar] [CrossRef] [PubMed]
- Knapp, H.R.; FitzGerald, G.A. The antihypertensive effects of fish oil. N. Engl. J. Med. 1989, 320, 1037–1043. [Google Scholar] [CrossRef]
- Miller, P.E.; Van Elswyk, M.; Alexander, D.D. Long-chain omega-3 fatty acids eicosapentaenoic acid and docosahexaenoic acid and docosahexaenoic acid and blood pressure: A meta-analysis of randomized controlled trials. Am. J. Hypertens. 2014, 27, 885–896. [Google Scholar] [CrossRef]
- Mozaffarian, D.; Lemaitre, R.N.; Kuller, L.H.; Burke, G.L.; Tracy, R.P.; Siscovick, D.S. Cardiac benefits of fish consumption may depend on the type of fish meal consumed: The Cardiovascular Health Study. Circulation 2003, 107, 1372–1377. [Google Scholar] [CrossRef]
- Kris-Etherton, P.M.; Harris, W.S.; Appel, L.J.; American Heart Association. Nutrition Committee. Fish consumption, fish oil, omega-3 fatty acids, and cardiovascular disease. Circulation 2002, 106, 2747–2757. [Google Scholar] [CrossRef]
- Joyce, S.A.; Gahan, C.G.M. Bile acid modifications at the microbe–host interface: Potential for nutraceutical and pharmaceutical interventions in host health. Annu. Rev. Food Sci. Technol. 2016, 7, 313–333. [Google Scholar] [CrossRef]
- Ahtesh, F.B.; Stojanovska, L.; Apostolopoulos, V. Anti-hypertensive peptides derived from milk proteins by probiotics. Maturitas 2018, 115, 103–109. [Google Scholar] [CrossRef]
- Didari, T.; Solki, S.; Mozaffari, S.; Nikfar, S.; Abdollahi, M. A systematic review of the safety of probiotics. Expert Opin. Drug Saf. 2014, 13, 227–239. [Google Scholar] [CrossRef]
- Böger, R.H. The pharmacodynamics of L-arginine. J. Nutr. 2007, 137, 1650S–1655S. [Google Scholar] [CrossRef] [PubMed]
- Littarru, G.P.; Tiano, L. Bioenergetic and antioxidant properties of coenzyme Q10: Recent developments. Mol. Biotechnol. 2007, 37, 31–37. [Google Scholar] [CrossRef] [PubMed]
- Zuchi, C.; Ambrosio, G.; Lüscher, T.F.; Landmesser, U. Nutraceuticals in cardiovascular prevention: Lessons from studies on endothelial function. Cardiovasc. Ther. 2010, 28, 187–201. [Google Scholar] [CrossRef] [PubMed]
- Ernster, L.; Dallner, G. Biochemical, physiological and medical aspects of ubiquinone function. Biochim. Biophys. Acta 1995, 1271, 195–204. [Google Scholar] [CrossRef]
- Crane, F.L. Biochemical functions of coenzyme Q10. J. Am. Coll. Nutr. 2001, 20, 591–598. [Google Scholar] [CrossRef]
- Rabanal-Ruiz, Y.; Llanos-González, E.; Alcain, F.J. The Use of Coenzyme Q10 in Cardiovascular Diseases. Antioxidants 2021, 10, 755. [Google Scholar] [CrossRef]
- Singh, R.B.; Niaz, M.A.; Rastogi, S.S.; Shukla, P.K.; Thakur, A.S. Effect of hydrosoluble coenzyme Q10 on blood pressures and insulin resistance in hypertensive patients with coronary artery disease. J. Hum. Hypertens. 1999, 13, 203–208. [Google Scholar] [CrossRef]
- Karimi, M.; Pirzad, S.; Hooshmand, F.; Shirsalimi, N.; Pourfaraji, S.M.A. Effects of coenzyme Q10 administration on blood pressure and heart rate in adults: A systematic review and meta-analysis of randomized controlled trials. Int. J. Cardiol. Cardiovasc. Risk Prev. 2025, 26, 200424. [Google Scholar] [CrossRef]
- Rosenfeldt, F.L.; Haas, S.J.; Krum, H.; Hadj, A.; Ng, K.; Leong, J.Y.; Watts, G.F. Coenzyme Q10 in the treatment of hypertension: A meta-analysis of the clinical trials. J. Hum. Hypertens. 2007, 21, 297–306. [Google Scholar] [CrossRef]
- Hidaka, T.; Fujii, K.; Funahashi, I.; Fukutomi, N.; Hosoe, K. Safety assessment of coenzyme Q10 (CoQ10). BioFactors 2008, 32, 199–208. [Google Scholar] [CrossRef]
- Garrido-Maraver, J.; Cordero, M.D.; Oropesa-Ávila, M.; Fernández Vega, A.; de la Mata, M.; Delgado Pavón, A.; de Miguel, M.; Pérez Calero, C.; Villanueva Paz, M.; Cotán, D.; et al. Coenzyme Q10 therapy. Mol. Syndromol. 2014, 5, 187–197. [Google Scholar] [CrossRef]
- Abukhodair, A.W.; Abukhudair, W.; Alqarni, M.S. The Effects of L-Arginine in Hypertensive Patients: A Literature Review. Cureus 2021, 13, e20485. [Google Scholar] [CrossRef]
- McRae, M.P. Therapeutic benefits of L-arginine: An umbrella review of meta-analyses. J. Chiropr. Med. 2016, 15, 184–189. [Google Scholar] [CrossRef]
- Dong, J.Y.; Qin, L.Q.; Zhang, Z.; Zhao, Y.; Wang, J.; Arigoni, F.; Zhang, W. Effect of oral L-arginine supplementation on blood pressure: A meta-analysis of randomized, double-blind, placebo-controlled trials. Am. Heart J. 2011, 162, 959–965. [Google Scholar] [CrossRef]
- Shiraseb, F.; Gholami, F.; Mohammadi, H.; Asbaghi, O.; Niktab, I.; Mirzababaei, A.; Clark, C.C.T.; Mirzaei, K. Effect of L-arginine supplementation on blood pressure in adults: A systematic review and dose-response meta-analysis of randomized clinical trials. Adv. Nutr. 2022, 13, 1226–1242. [Google Scholar] [CrossRef]
- Grimble, G.K. Adverse gastrointestinal effects of arginine and related amino acids. J. Nutr. 2007, 137, 1693S–1701S. [Google Scholar] [CrossRef]
- Allerton, T.D.; Proctor, D.N.; Stephens, J.M.; Dugas, T.R.; Spielmann, G.; Irving, B.A. L-Citrulline supplementation: Impact on cardiometabolic health. Nutrients 2018, 10, 921. [Google Scholar] [CrossRef]
- Förstermann, U.; Sessa, W.C. Nitric oxide synthases: Regulation and function. Eur. Heart J. 2012, 33, 829–837. [Google Scholar] [CrossRef]
- Fyhrquist, F.; Saijonmaa, O. Renin–angiotensin system revisited. J. Intern. Med. 2008, 264, 224–236. [Google Scholar] [CrossRef]
- Montezano, A.C.; Touyz, R.M. Reactive oxygen species, vascular Noxs, and hypertension: Focus on translational and clinical research. Antioxid. Redox Signal. 2014, 20, 164–182. [Google Scholar] [CrossRef]
- Higashi, Y.; Noma, K.; Yoshizumi, M.; Kihara, Y. Endothelial function and oxidative stress in cardiovascular diseases. Circ. J. 2009, 73, 411–418. [Google Scholar] [CrossRef]
- Dickinson, H.O.; Nicolson, D.J.; Campbell, F.; Beyer, F.R.; Mason, J. Potassium supplementation for the management of primary hypertension in adults. Cochrane Database Syst. Rev. 2006, 3, CD004641. [Google Scholar] [CrossRef]
- Argeros, Z.; Xu, X.; Bhandari, B.; Harris, K.; Touyz, R.M.; Schutte, A.E. Magnesium supplementation and blood pressure: A systematic review and meta-analysis of randomized controlled trials. Hypertension 2025, 82, 1844–1856. [Google Scholar] [CrossRef]
- Heiss, C.; Keen, C.L.; Kelm, M. Flavanols and cardiovascular disease prevention. Eur. Heart J. 2010, 31, 2583–2592. [Google Scholar] [CrossRef]
- Schiffrin, E.L. Vascular remodeling in hypertension: Mechanisms and treatment. Hypertension 2012, 59, 367–374. [Google Scholar] [CrossRef]
- Ordovás, J.M.; Ferguson, L.R.; Tai, E.S.; Mathers, J.C. Personalized nutrition and health. BMJ 2018, 361, bmj.k2173. [Google Scholar] [CrossRef]
- Zeevi, D.; Korem, T.; Zmora, N.; Israeli, D.; Rothschild, D.; Weinberger, A.; Ben-Yacov, O.; Lador, D.; Avnit-Sagi, T.; Lotan-Pompan, M.; et al. Personalized nutrition by prediction of glycemic responses. Cell 2015, 163, 1079–1094. [Google Scholar] [CrossRef]


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license.