- Review

The Aging Skin–Psoriasis Interface: Could Cellular Senescence and Immunosenescence Slow Therapeutic Response?
- Umberto Santaniello,
- François Rosset and
- Simone Ribero
- + 3 authors
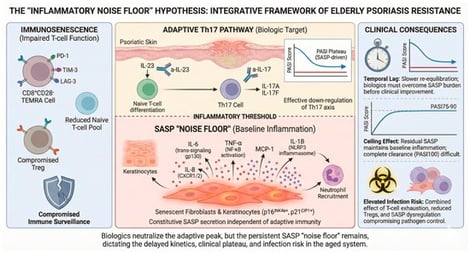
Elderly psoriasis patients (≥65 years) demonstrate mainly preserved but substantially delayed therapeutic responses to IL-17 and IL-23 inhibitors, achieving lower PASI90 rates at early time-points with eventual “catch-up” by week 52, alongside increased adverse-event-driven discontinuation. This review synthesizes clinical efficacy data from real-world studies with emerging mechanistic evidence on immunosenescence and cellular senescence to propose the “Inflammatory Noise Floor” hypothesis. We postulate that senescent keratinocytes and fibroblasts constitutively secrete SASP cytokines (IL-6, IL-8, TNF-α) through pathways partially independent of IL-23/IL-17, potentially establishing a persistent baseline inflammation that IL-23/IL-17 blockade might not suppress. Concurrently, immunosenescence, characterized by CD8+CD28− T-cell accumulation, exhaustion marker upregulation, and Treg dysfunction, is hypothesized to impair adaptive immune re-equilibration. This dual mechanism represents one plausible, albeit theoretical, explanatory framework for the temporal lag, PASI plateau effects, and infection risk observed in elderly patients. Optimizing outcomes in the elderly may require a pragmatic approach: accepting stable PASI 75-90 as a successful endpoint and prospectively validating extended assessment timelines. While a direct correlation remains to be proven, this framework identifies cellular and immunosenescence as potential targets for future senotherapeutic interventions.
8 May 2026