- Systematic Review

Diagnosis and Treatment of Nontraumatic Osteonecrosis of the Femoral Head: A Systematic Review and Meta-Analyses for the ARCO Clinical Practice Guideline Development Workgroup
- Romil R. Parikh,
- Alireza Mirzaei and
- Edward Y. Cheng
- + 10 authors
Background/Objectives: Diagnostic evaluation and management of nontraumatic osteonecrosis of the femoral head (ONFH) vary substantially. This systematic review was conducted to inform development of the Association Research Circulation Osseous (ARCO) clinical practice guideline for diagnosis and treatment of ARCO stages I to III ONFH. Methods: We searched MEDLINE, EMBASE, Web of Science, SCOPUS, Global Index Medicus, and the Cochrane Library for studies evaluating imaging modalities and treatments for adult ONFH. We assessed risk of bias using the QUADAS-2, the ROB-2, and the ROBINS-I tools; conducted meta-analyses using random-effects regression; and evaluated certainty of evidence using GRADE methodology. Results: Among 36 included studies, 18 addressed diagnostic test accuracy and 18 addressed comparative effectiveness of treatments. Magnetic resonance imaging (MRI) demonstrated the highest pooled sensitivity (0.91; 95% confidence interval (CI), 0.87 to 0.94) and specificity (0.96; 95% CI, 0.87 to 0.99) for ONFH diagnosis. Bone marrow edema and grade 2+ joint effusion on MRI differentiated symptomatic versus asymptomatic disease. Computed tomography and MRI better detected subchondral fractures than plain radiography. Very low-grade evidence suggested lower rates of femoral head collapse with core decompression plus bone marrow concentrate compared with core decompression alone (pooled relative risk [RR], 0.55; 95% CI, 0.36 to 0.83), and with vascularized versus non-vascularized bone grafting (RR, 0.35; 95% CI, 0.14 to 0.84) over a ≤5-year follow-up. Based on three non-comparative case series, osteotomies might have a lower risk of collapse over a 10- to 20-year follow-up, but this needs to be evaluated in future comparative research. Inconsistent outcome reporting hindered treatment outcome pooling. There were no comparative studies that evaluated observation only versus intervention in asymptomatic disease or strategies for monitoring treatment response. Conclusions: Evidence supporting optimal imaging modalities and early joint-preserving interventions remains limited and predominantly observational, underscoring the need for high-quality comparative studies with consistently defined core outcomes to guide clinical decision-making.
23 February 2026
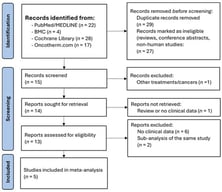
![PRISMA Flow Diagram for Study Selection for Systematic Review: Diagnosis and Treatment of Osteonecrosis of Femoral Head. KQ: Key Question; Source: Page et al. [10]. This work is licensed under CC BY 4.0. To view a copy of this license, visit https://creativecommons.org/licenses/by/4.0/ (accessed on 17 February 2026).](https://mdpi-res.com/cdn-cgi/image/w=470,h=317/https://mdpi-res.com/medsci/medsci-14-00107/article_deploy/html/images/medsci-14-00107-g001-550.jpg)