
Increased Circulating Malondialdehyde-Modified Low-Density Lipoprotein Level Is Associated with High-Risk Plaque in Coronary Computed Tomography Angiography in Patients Receiving Statin Therapy


Abstract
:1. Introduction
2. Materials and Methods
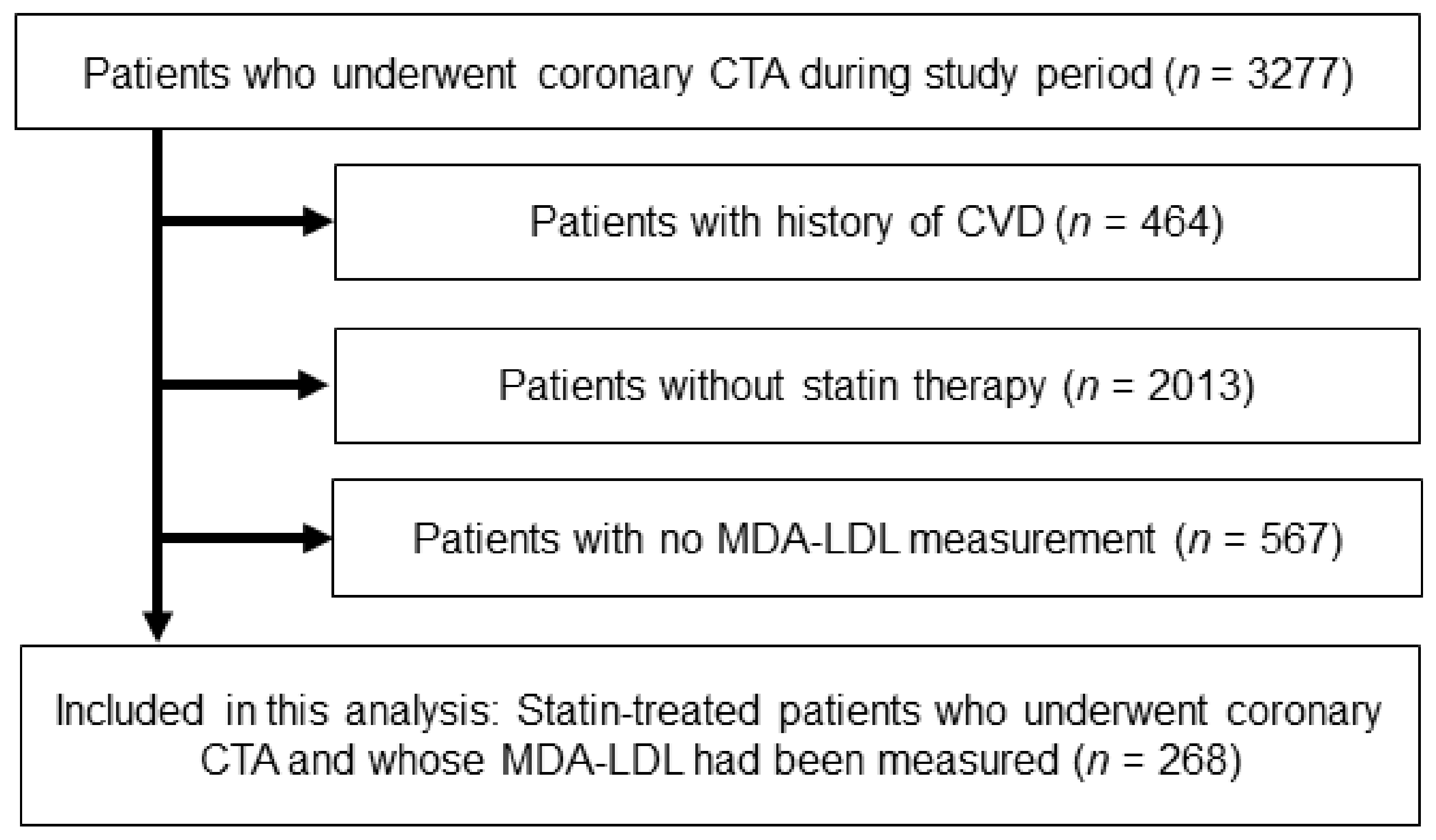
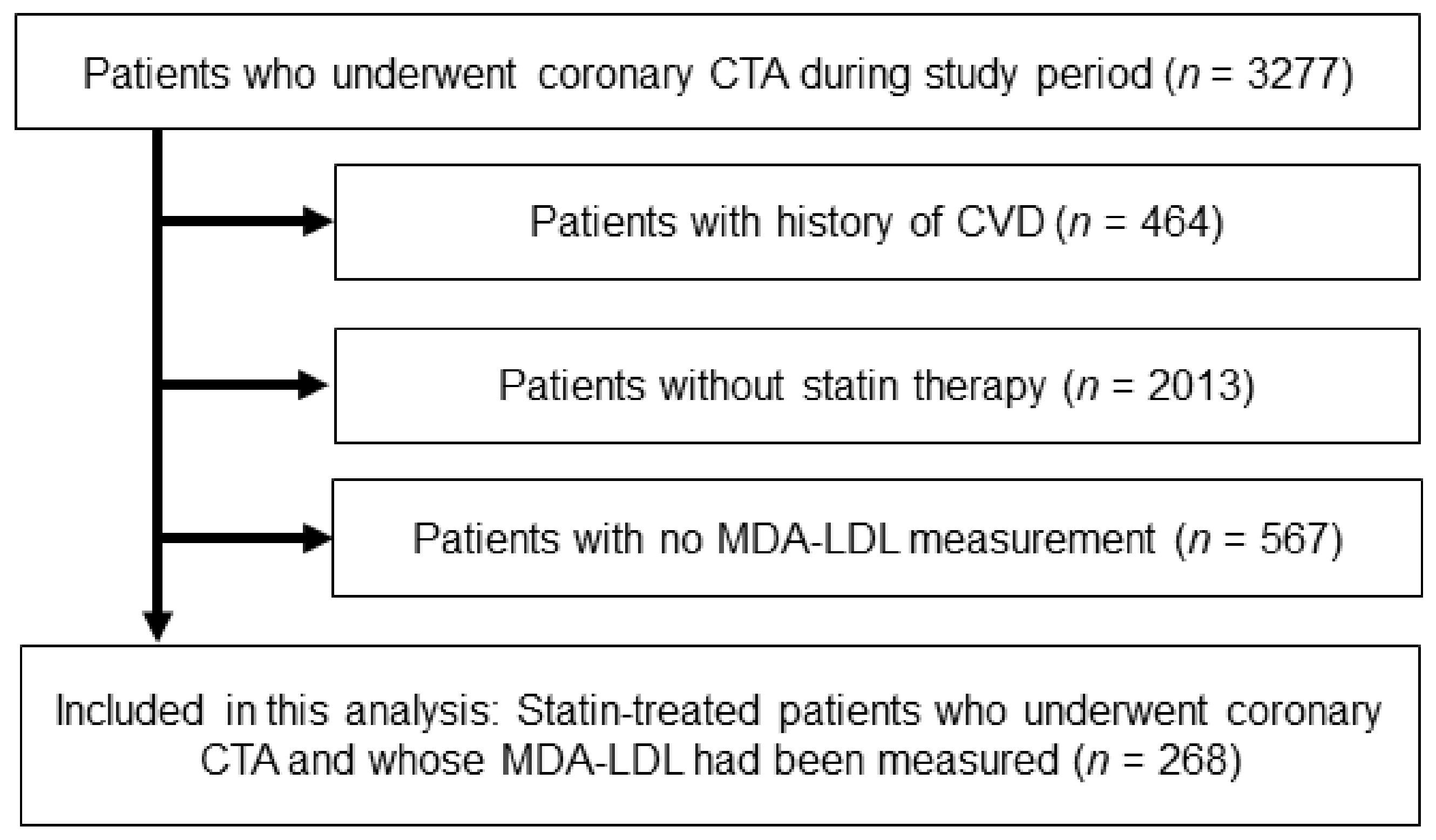
2.1. Study Population and Risk Assessment
2.2. Blood Sampling and the Measurement of MDA-LDL
2.3. Acquisition and Analyses of Coronary CTA Image
2.4. Outcome Data
2.5. Statistical Analysis
3. Results
3.1. Patient Characteristics
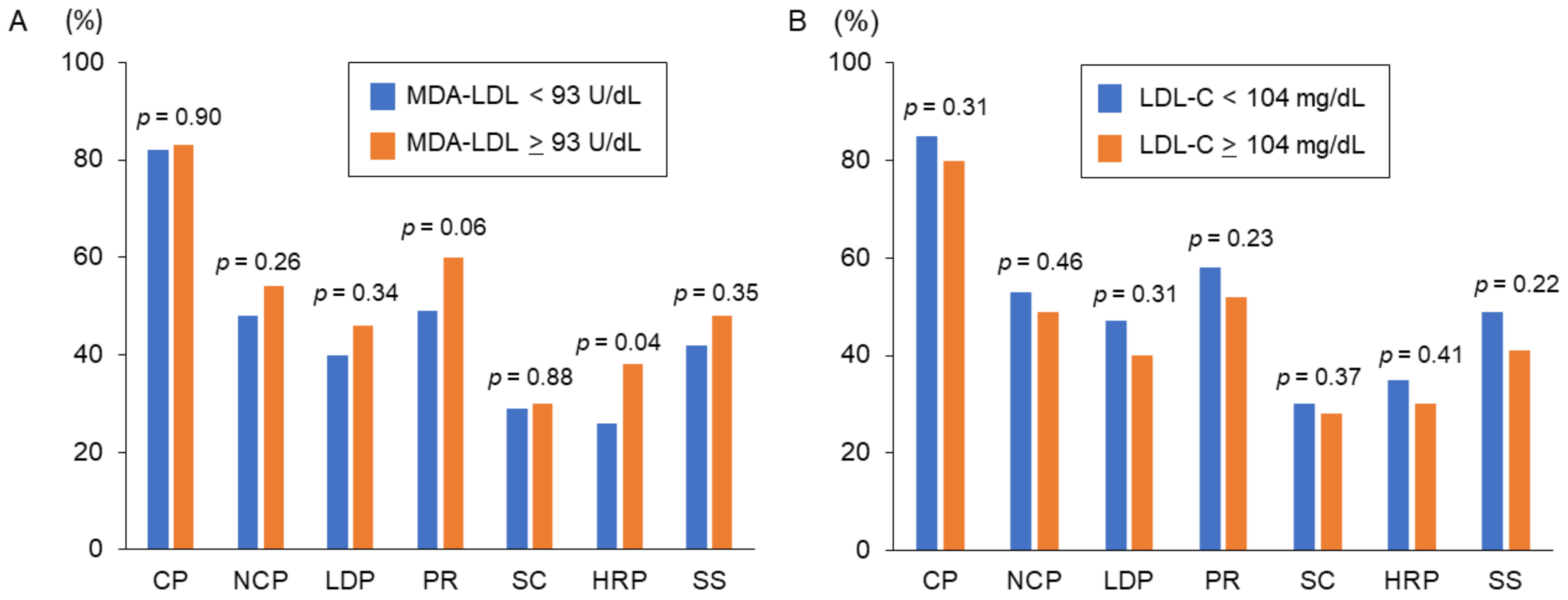
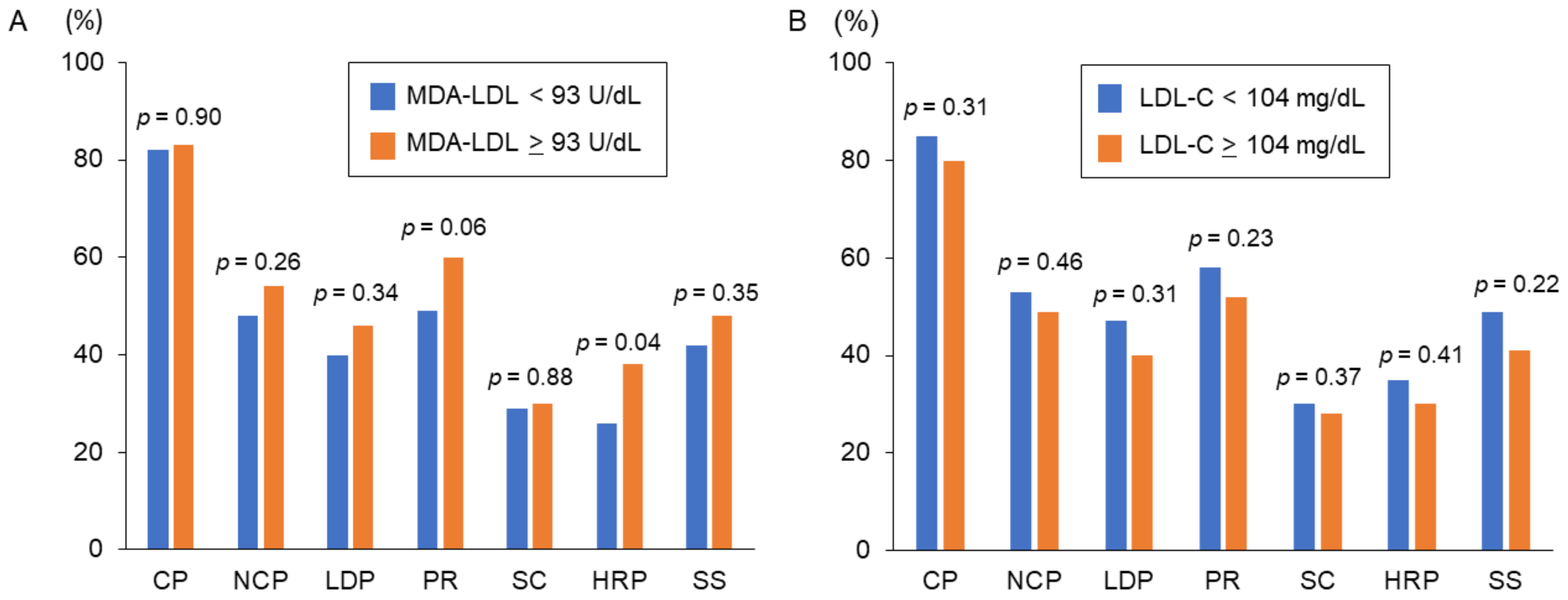
3.2. MDA-LDL and Coronary CTA Findings
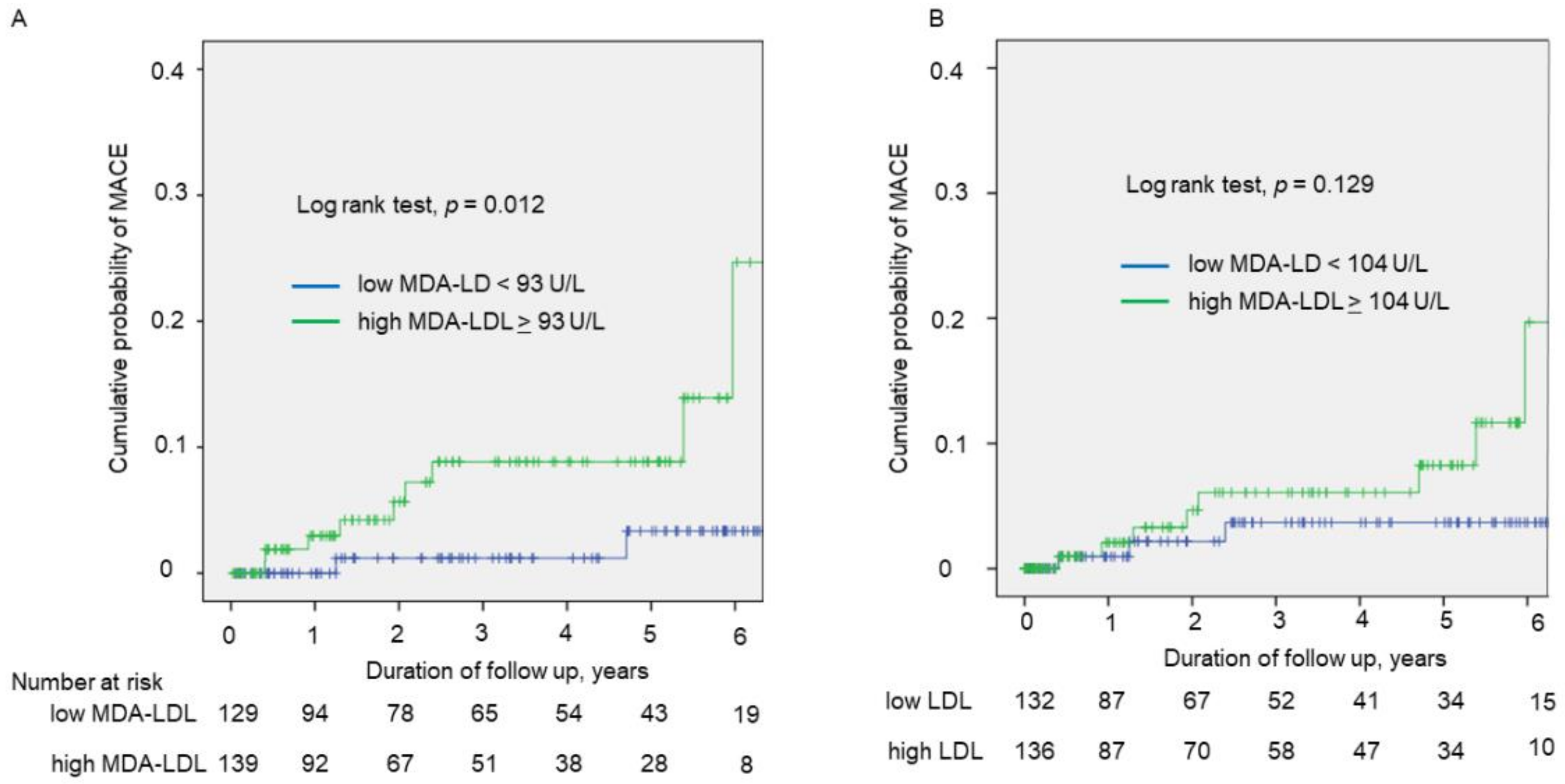
3.3. Prognostic Impact of HRP and MDA-LDL for Cardiovascular Events
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Timmis, A.; Townsend, N.; Gale, C.; Grobbee, R.; Maniadakis, N.; Flather, M.; Wilkins, E.; Wright, L.; Vos, R.; Bax, J.; et al. European Society of Cardiology: Cardiovascular Disease Statistics 2017. Eur. Heart J. 2018, 39, 508–579. [Google Scholar] [CrossRef] [Green Version]
- Ridker, P.M.; Pradhan, A.; MacFadyen, J.G.; Libby, P.; Glynn, R.J. Cardiovascular benefits and diabetes risks of statin therapy in primary prevention: An analysis from the JUPITER trial. Lancet 2012, 380, 565–571. [Google Scholar] [CrossRef] [Green Version]
- Mills, E.J.; Rachlis, B.; Wu, P.; Devereaux, P.J.; Arora, P.; Perri, D. Primary prevention of cardiovascular mortality and events with statin treatments: A network meta-analysis involving more than 65,000 patients. J. Am. Coll. Cardiol. 2008, 52, 1769–1781. [Google Scholar] [CrossRef] [Green Version]
- Reith, C.; Armitage, J. Management of residual risk after statin therapy. Atherosclerosis 2016, 245, 161–170. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matsuo, Y.; Kubo, T.; Okumoto, Y.; Ishibashi, K.; Komukai, K.; Tanimoto, T.; Ino, Y.; Kitabata, H.; Hirata, K.; Imanishi, T.; et al. Circulating malondialdehyde-modified low-density lipoprotein levels are associated with the presence of thin-cap fibroatheromas determined by optical coherence tomography in coronary artery disease. Eur. Heart J. Cardiovasc. Imaging 2013, 14, 43–50. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ito, T.; Fujita, H.; Tani, T.; Ohte, N. Malondialdehyde-modified low-density lipoprotein is a predictor of cardiac events in patients with stable angina on lipid-lowering therapy after percutaneous coronary intervention using drug-eluting stent. Atherosclerosis 2015, 239, 311–317. [Google Scholar] [CrossRef] [PubMed]
- Holvoet, P.; Collen, D.; Van de Werf, F. Malondialdehyde-modified LDL as a marker of acute coronary syndromes. JAMA 1999, 281, 1718–1721. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xie, J.X.; Cury, R.C.; Leipsic, J.; Crim, M.T.; Berman, D.S.; Gransar, H.; Budoff, M.J.; Achenbach, S.; Hartaigh, B.O.; Callister, T.Q.; et al. The Coronary Artery Disease-Reporting and Data System (CAD-RADS): Prognostic and Clinical Implications Associated With Standardized Coronary Computed Tomography Angiography Reporting. JACC Cardiovasc. Imaging 2018, 11, 78–89. [Google Scholar] [CrossRef] [PubMed]
- Bamberg, F.; Sommer, W.H.; Hoffmann, V.; Achenbach, S.; Nikolaou, K.; Conen, D.; Reiser, M.F.; Hoffmann, U.; Becker, C.R. Meta-analysis and systematic review of the long-term predictive value of assessment of coronary atherosclerosis by contrast-enhanced coronary computed tomography angiography. J. Am. Coll. Cardiol. 2011, 57, 2426–2436. [Google Scholar] [CrossRef] [Green Version]
- Versteylen, M.O.; Kietselaer, B.L.; Dagnelie, P.C.; Joosen, I.A.; Dedic, A.; Raaijmakers, R.H.; Wildberger, J.E.; Nieman, K.; Crijns, H.J.; Niessen, W.J.; et al. Additive value of semiautomated quantification of coronary artery disease using cardiac computed tomographic angiography to predict future acute coronary syndrome. J. Am. Coll. Cardiol. 2013, 61, 2296–2305. [Google Scholar] [CrossRef]
- Puri, R.; Nicholls, S.J.; Shao, M.; Kataoka, Y.; Uno, K.; Kapadia, S.R.; Tuzcu, E.M.; Nissen, S.E. Impact of statins on serial coronary calcification during atheroma progression and regression. J. Am. Coll. Cardiol. 2015, 65, 1273–1282. [Google Scholar] [CrossRef] [PubMed]
- Amioka, N.; Miyoshi, T.; Otsuka, H.; Yamada, D.; Takaishi, A.; Ueeda, M.; Hirohata, S.; Ito, H. Serum malondialdehyde-modified low-density lipoprotein levels on admission predict prognosis in patients with acute coronary syndrome undergoing percutaneous coronary intervention. J. Cardiol. 2019, 74, 258–266. [Google Scholar] [CrossRef] [PubMed]
- Osawa, K.; Miyoshi, T.; Yamauchi, K.; Koyama, Y.; Nakamura, K.; Sato, S.; Kanazawa, S.; Ito, H. Nonalcoholic Hepatic Steatosis Is a Strong Predictor of High-Risk Coronary-Artery Plaques as Determined by Multidetector CT. PLoS ONE 2015, 10, e0131138. [Google Scholar] [CrossRef] [PubMed]
- Ichikawa, K.; Miyoshi, T.; Osawa, K.; Miki, T.; Nakamura, K.; Ito, H. Prognostic Value of Coronary Computed Tomographic Angiography in Patients With Nonalcoholic Fatty Liver Disease. JACC Cardiovasc. Imaging 2020, 13, 1628–1630. [Google Scholar] [CrossRef]
- Anderson, J.L.; Adams, C.D.; Antman, E.M.; Bridges, C.R.; Califf, R.M.; Casey, D.E., Jr.; Chavey, W.E., 2nd; Fesmire, F.M.; Hochman, J.S.; Levin, T.N.; et al. 2011 ACCF/AHA Focused Update Incorporated Into the ACC/AHA 2007 Guidelines for the Management of Patients With Unstable Angina/Non-ST-Elevation Myocardial Infarction: A report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. Circulation 2011, 123, e426–e579. [Google Scholar] [CrossRef]
- Gao, S.; Zhao, D.; Wang, M.; Zhao, F.; Han, X.; Qi, Y.; Liu, J. Association Between Circulating Oxidized LDL and Atherosclerotic Cardiovascular Disease: A Meta-analysis of Observational Studies. Can. J. Cardiol. 2017, 33, 1624–1632. [Google Scholar] [CrossRef] [PubMed]
- Matsuura, Y.; Kanter, J.E.; Bornfeldt, K.E. Highlighting Residual Atherosclerotic Cardiovascular Disease Risk. Arterioscler. Thromb. Vasc. Biol. 2019, 39, e1–e9. [Google Scholar] [CrossRef]
- Fan, J.; Liu, Y.; Yin, S.; Chen, N.; Bai, X.; Ke, Q.; Shen, J.; Xia, M. Small dense LDL cholesterol is associated with metabolic syndrome traits independently of obesity and inflammation. Nutr. Metab. 2019, 16, 7. [Google Scholar] [CrossRef]
- Hu, C.; Dandapat, A.; Sun, L.; Chen, J.; Marwali, M.R.; Romeo, F.; Sawamura, T.; Mehta, J.L. LOX-1 deletion decreases collagen accumulation in atherosclerotic plaque in low-density lipoprotein receptor knockout mice fed a high-cholesterol diet. Cardiovasc. Res. 2008, 79, 287–293. [Google Scholar] [CrossRef]
- Kume, N.; Kita, T. Apoptosis of vascular cells by oxidized LDL: Involvement of caspases and LOX-1 and its implication in atherosclerotic plaque rupture. Circ. Res. 2004, 94, 269–270. [Google Scholar] [CrossRef] [Green Version]
- Kattoor, A.J.; Pothineni, N.V.K.; Palagiri, D.; Mehta, J.L. Oxidative Stress in Atherosclerosis. Curr. Atheroscler. Rep. 2017, 19, 42. [Google Scholar] [CrossRef]
- Ikenaga, H.; Kurisu, S.; Kono, S.; Sumimoto, Y.; Watanabe, N.; Shimonaga, T.; Higaki, T.; Iwasaki, T.; Mitsuba, N.; Ishibashi, K.; et al. Impact of Malondialdehyde-Modified Low-Density Lipoprotein on Tissue Characteristics in Patients With Stable Coronary Artery Disease- Integrated Backscatter-Intravascular Ultrasound Study. Circ. J. 2016, 80, 2173–2182. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Duran, E.K.; Aday, A.W.; Cook, N.R.; Buring, J.E.; Ridker, P.M.; Pradhan, A.D. Triglyceride-Rich Lipoprotein Cholesterol, Small Dense LDL Cholesterol, and Incident Cardiovascular Disease. J. Am. Coll. Cardiol. 2020, 75, 2122–2135. [Google Scholar] [CrossRef] [PubMed]
- Marwali, M.R.; Hu, C.P.; Mohandas, B.; Dandapat, A.; Deonikar, P.; Chen, J.; Cawich, I.; Sawamura, T.; Kavdia, M.; Mehta, J.L. Modulation of ADP-induced platelet activation by aspirin and pravastatin: Role of lectin-like oxidized low-density lipoprotein receptor-1, nitric oxide, oxidative stress, and inside-out integrin signaling. J. Pharmacol. Exp. Ther. 2007, 322, 1324–1332. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nishikido, T.; Oyama, J.; Keida, T.; Ohira, H.; Node, K. High-dose statin therapy with rosuvastatin reduces small dense LDL and MDA-LDL: The Standard versus high-dose therApy with Rosuvastatin for lipiD lowering (SARD) trial. J. Cardiol. 2016, 67, 340–346. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, W.; Yin, Y.; Zhou, Z.; He, M.; Dai, Y. OxLDL-induced IL-1 beta secretion promoting foam cells formation was mainly via CD36 mediated ROS production leading to NLRP3 inflammasome activation. Inflamm. Res. 2014, 63, 33–43. [Google Scholar] [CrossRef]
- Ridker, P.M.; Everett, B.M.; Thuren, T.; MacFadyen, J.G.; Chang, W.H.; Ballantyne, C.; Fonseca, F.; Nicolau, J.; Koenig, W.; Anker, S.D.; et al. Antiinflammatory Therapy with Canakinumab for Atherosclerotic Disease. N. Engl. J. Med. 2017, 377, 1119–1131. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| All Patients | High MDA-LDL (≥93 U/L) | Low MDA-LDL (<93 U/L) | p-Value | |
|---|---|---|---|---|
| n | 268 | 139 | 129 | |
| Age, year | 67 ± 11 | 67 ± 11 | 68 ± 11 | 0.521 |
| Male sex | 154 (58) | 76 (55) | 78 (61) | 0.338 |
| Body mass index, kg/m2 | 24.6 ± 4.1 | 25.2 ± 3.9 | 24.0 ± 4.2 | 0.016 |
| Hypertension | 203 (76) | 109 (78) | 94 (73) | 0.290 |
| Diabetes mellitus | 122 (46) | 59 (42) | 63 (49) | 0.294 |
| Current Smoker | 70 (26) | 36 (26) | 34 (26) | 0.932 |
| Medications | ||||
| Beta blockers | 71 (27) | 37 (27) | 34 (26) | 0.933 |
| CCBs | 122 (46) | 70 (50) | 52 (40) | 0.099 |
| ACE-Is or ARBs | 135 (50) | 73 (53) | 62 (48) | 0.466 |
| Oral antihyperglycemic drugs | 86 (32) | 45 (32) | 41 (32) | 0.918 |
| Ezetimibe | 15 (6) | 10 (7) | 5 (4) | 0.293 |
| Statin intensity, low/moderate * | 160 (60)/108 (40) | 76 (55)/63 (45) | 84 (65)/45 (35) | 0.082 |
| Statin type, dosage | ||||
| Atorvastatin, 5 mg/10 mg | 18/49 | 5/26 | 13/23 | |
| Fluvastatin, 20 mg/40 mg | 4/1 | 3/1 | 1/0 | |
| Pitavastatin, 1 mg/2 mg/4 mg | 14/28/4 | 6/13/3 | 8/15/1 | |
| Pravastatin, 5 mg/10 mg | 9/36 | 5/21 | 4/15 | |
| Rosuvastatin, 2.5 mg/5 mg/10 mg | 68/24/2 | 30/19/2 | 38/5/0 | |
| Simvastatin, 5 mg/10 mg | 8/3 | 4/1 | 4/2 | |
| Laboratory findings | ||||
| Creatinine, mg/dL | 0.89 ± 0.78 | 0.85 ± 0.64 | 0.93 ± 0.92 | 0.397 |
| eGFR, mL/min/1.73 m2 | 68 ± 18 | 68 ± 17 | 69 ± 19 | 0.665 |
| Total cholesterol, mg/dL | 186 ± 40 | 203 ± 40 | 168 ± 31 | <0.001 |
| LDL cholesterol, mg/dL | 107 ± 32 | 122 ± 33 | 90 ± 22 | <0.001 |
| HDL cholesterol, mg/dL | 58 ± 17 | 57 ± 17 | 60 ± 17 | 0.080 |
| Triglyceride, mg/dL | 121 (88, 171) | 150 (104, 198) | 101 (76, 130) | <0.001 |
| MDA-LDL, U/L | 96 ± 35 | 122 ± 28 | 69 ± 15 | <0.001 |
| HbA1c, % | 6.6 ± 1.3 | 6.6 ± 1.4 | 6.6 ± 1.3 | 0.968 |
| hsCRP, mg/dL | 0.08 (0.05, 0.18) | 0.08 (0.04, 0.16) | 0.08 (0.05, 0.20) | 0.608 |
| Patients achieving LDLcholesterol <70 mg/dL | 24 (9) | 1 (1) | 23 (18) | <0.001 |
| Variables | High-Risk Plaque | Significant Stenosis | ||||
|---|---|---|---|---|---|---|
| Present | Absent | p Value | Present | Absent | p Value | |
| n | 87 | 181 | 119 | 148 | ||
| Age, year | 68 ± 10 | 67 ± 12 | 0.747 | 68 ± 11 | 67 ± 12 | 0.489 |
| Male sex | 64 (74) | 90 (50) | <0.001 | 84 (70) | 70 (47) | <0.001 |
| Body mass index, kg/m2 | 24.7 ± 3.4 | 24.5 ± 4.4 | 0.718 | 24.4 ± 4.1 | 24.7 ± 4.1 | 0.450 |
| Hypertension | 73 (84) | 130 (76) | 0.031 | 93 (78) | 110 (74) | 0.546 |
| Diabetes mellitus | 48 (55) | 74 (41) | 0.028 | 63 (53) | 59 (40) | 0.039 |
| Current smoker | 29 (33) | 41 (23) | 0.062 | 32 (27) | 38 (25) | 0.854 |
| Oral antihyperglycemic drugs | 32 (37) | 54 (30) | 0.254 | 42 (35) | 44 (30) | 0.333 |
| Creatinine, mg/dL | 1.00 ± 0.99 | 0.83 ± 0.65 | 0.087 | 0.91 ± 0.71 | 0.88 ± 0.83 | 0.066 |
| Total cholesterol, mg/dL | 186 ± 45 | 187 ± 38 | 0.834 | 183 ± 41 | 188 ± 38 | 0.300 |
| LDL cholesterol, mg/dL | 107 ± 37 | 107 ± 30 | 0.867 | 106 ± 34 | 107 ± 31 | 0.728 |
| HDL cholesterol, mg/dL | 55 ± 16 | 60 ± 17 | 0.014 | 58 ± 18 | 58 ± 16 | 0.905 |
| Triglyceride, mg/dL | 130 (90, 182) | 117 (85, 170) | 0.206 | 118 (86, 158) | 122 (89, 183) | 0.155 |
| MDA-LDL, U/L | 105 ± 40 | 92 ± 32 | 0.011 | 96 ± 33 | 96 ± 36 | 0.979 |
| HbA1c, % | 6.7 ± 1.3 | 6.5 ± 1.4 | 0.347 | 6.6 ± 1.3 | 6.5 ± 1.4 | 0.122 |
| hsCRP, mg/dL | 0.08 (0.05, 0.16) | 0.08 (0.04, 0.19) | 0.907 | 0.09 (0.05, 0.200) | 0.07 (0.040, 0.160) | 0.132 |
| Univariate | Multivariate | |||
|---|---|---|---|---|
| Odds Ratio (95%CI) | p Value | Odds Ratio (95%CI) | p Value | |
| Age, per 1 year | 1.004 (0.981–1.028) | 0.746 | ||
| Male | 2.814 (1.609–4.918) | <0.001 | 2.749 (1.502–1.502) | 0.001 |
| Hypertension | 2.046 (1.060–3.947) | 0.033 | 2.027 (1.022–4.019) | 0.049 |
| Diabetes Mellitus | 1.780 (1.062–2.982) | 0.029 | 1.630 (0.941–2.824) | 0.081 |
| Current smoker | 1.707 (0.970–3.006) | 0.064 | ||
| HDL cholesterol, per 1 mg/dL | 0.980 (0.964–0.996) | 0.015 | 0.994 (0.977–1.012) | 0.531 |
| LDL cholesterol, >104 mg/dL | 0.807 (0.483–1.347) | 0.412 | ||
| Triglyceride *, per 1 index | 1.454 (0.854–2.475) | 0.168 | ||
| MDA-LDL, >93 U/L | 1.722 (1.024–2.897) | 0.041 | 1.883 (1.082–3.279) | 0.025 |
| hsCRP *, per 1 index | 0.983 (0.793–1.219) | 0.878 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ichikawa, K.; Miyoshi, T.; Osawa, K.; Miki, T.; Ito, H. Increased Circulating Malondialdehyde-Modified Low-Density Lipoprotein Level Is Associated with High-Risk Plaque in Coronary Computed Tomography Angiography in Patients Receiving Statin Therapy. J. Clin. Med. 2021, 10, 1480. https://doi.org/10.3390/jcm10071480
Ichikawa K, Miyoshi T, Osawa K, Miki T, Ito H. Increased Circulating Malondialdehyde-Modified Low-Density Lipoprotein Level Is Associated with High-Risk Plaque in Coronary Computed Tomography Angiography in Patients Receiving Statin Therapy. Journal of Clinical Medicine. 2021; 10(7):1480. https://doi.org/10.3390/jcm10071480
Chicago/Turabian StyleIchikawa, Keishi, Toru Miyoshi, Kazuhiro Osawa, Takashi Miki, and Hiroshi Ito. 2021. "Increased Circulating Malondialdehyde-Modified Low-Density Lipoprotein Level Is Associated with High-Risk Plaque in Coronary Computed Tomography Angiography in Patients Receiving Statin Therapy" Journal of Clinical Medicine 10, no. 7: 1480. https://doi.org/10.3390/jcm10071480