Abstract
Patients with diabetes and/or peripheral artery disease (PAD) are at risk for lower limb amputation and a subsequently higher mortality risk. Peer support interventions have been shown to increase diabetes self-management and glycemic control. This scoping review aims to synthesize the current literature on peer support interventions in reducing lower limb amputations. A PubMed search was conducted in June of 2023, excluding publications prior to 2000, focusing on two themes: (1) peer support and (2) the patient population of interest (i.e., individuals with diabetic foot disease and/or PAD). Studies were included if they addressed the population of interest, involved a peer support intervention to improve lower extremity health, and had outcomes pertaining to the health of the lower extremities or programmatic metrics such as participant satisfaction or program adherence. Out of 1730 publications initially identified, six met the inclusion criteria. These six studies were categorized as group foot care education studies (n = 4) or group cognitive behavioral studies (n = 2). The group foot care education studies showed mixed results, which varied from no effect to significant improvements in foot care, self-management, and complications. There was a trend of improvement in self-management behaviors and physical activity in cognitive behavioral interventions. Despite showing promise in other settings, there have been limited investigations of peer support interventions to improve lower extremity outcomes and avert amputations in persons with diabetes and/or PAD. Further studies are required to conclusively determine the efficacy of peer support interventions to reduce lower extremity amputation rates.
1. Introduction
Individuals diagnosed with diabetes mellitus and/or peripheral artery disease (PAD) are at an increased risk of lower extremity amputation. Unfortunately, the five-year mortality rate in persons with diabetes and PAD ranges from 53% to 100% for major and minor amputations combined, 52% to 80% for major amputations alone, and 29% to 69% for minor amputations alone [1]. Armstrong et al. determined a respective 46.2% and 56.6% five-year mortality rate after minor and major amputations in patients with diabetes, comparable to the five-year mortality rate of all cancers at 31% [2]. Despite a decline in the early 2000s, lower limb amputations in persons with diabetes in the US increased from 2010 to 2020 [3]. By 2020, there were 6.1 non-traumatic lower extremity amputation hospitalizations per 1000 adults living with diabetes [3]. The primary precursor to amputations in persons with diabetes is a diabetic foot ulcer (DFU), with 84% of such amputations being preceded by a DFU [4]. Within Medicare beneficiaries with concomitant diabetes and PAD, Fowler et al. reported a five-year lower extremity amputation rate of 3% [5]. Similarly, in a large-scale trial of individuals with PAD (13,385 participants) that received medication to prevent major adverse cardiovascular events, 2.9% of participants underwent at least one lower extremity amputation within the median follow-up time of 30 months [6]. Within the sizable proportion of participants with diabetes in the trial (38%), infection was the most frequent driver of amputation, with 58% of the amputations attributable to it [6]. Additionally, higher amputation rates are found in individuals with diabetes and PAD who are African American, Native American, or Hispanic [7,8]. This large-scale problem warrants additional efforts to limit amputations in persons with diabetes and/or PAD. It is possible peer support interventions could help to reduce the unacceptably high incidence of lower extremity amputations by helping at-risk individuals to learn and implement preventative behaviors in an understanding environment.
Peer support is defined as a reciprocal relationship based on mutual respect, responsibility, and agreement with a foundation of commonality, empathy, and trust with the aim of providing help to all parties involved [9]. Peer support refers to individuals who are considered equals and falls within the larger category of social support, which refers to a broader spectrum of relationships that provide support [10]. Social support affects psychosocial factors that influence the management of chronic disease. A recent meta-analysis consisting of 11 studies and 3151 participants with type 2 diabetes mellitus found an association between lower levels of social support and depression [11]. Comparably, a cross-sectional study conducted in South Africa determined that individuals with diabetes with a higher level of social support suffered less emotional distress [12]. In addition to emotional impact, peer support can lead to enhanced diabetes management. Two meta-analyses of randomized control trials (RCTs) illustrated a correlation between lower HbA1c scores and peer support intervention [13,14]. Song et al. found a medium-strength, positive association between social support and diabetes self-care, specifically with the greatest association with glucose monitoring [15]. Furthermore, in a systematic review of published systematic reviews and meta-analyses of peer support in diabetes care, Litchman et al. found social support led to significant improvements in HbA1c, systolic blood pressure, diabetes knowledge, and diabetes self-management [16].
Instilling peer support interventions with diabetes self-management behaviors, such as foot care, could potentially reduce the occurrence of amputations. In a 2013 investigation of peer support for persons with type 2 diabetes, Whitford et al. generated 21 frequently asked questions regarding foot care over eight meetings from 29 peer support groups, demonstrating the relatively recent need and desire for diabetic foot care education, particularly in a peer support setting [17]. The aim of this scoping review was to identify and examine the available recent literature regarding peer support interventions with a lower extremity component and their influence on populations at risk for lower extremity amputations with the purpose of summarizing the structure, dynamics, and findings of these studies.
2. Methods
An advanced search on PubMed was conducted for articles published in the 2000s that reported on subjective and clinical outcome measures related to amputation prevention in patients with diabetes and/or PAD at risk of loss of the lower limb. The following search string was used to retrieve relevant articles from the database in June of 2023: ((social support) OR (“peer support”) OR (“group visits”) OR (peer groups) OR (“group education”) OR (“foot care education”) OR (“psychoeducation”) OR (“cognitive behavioral”)) AND ((diabetic foot[MeSH Terms]) OR (peripheral arterial disease [MeSH Terms]) OR (foot health) OR (“foot care”) OR (“diabetes self-management”) NOT (arm OR hand)).
Publications were included if a peer support intervention was conducted with adults at risk for lower extremity amputations. At-risk adults were individuals with one or more of the following: type 1 or type 2 diabetes mellitus with a foot ulcer or at a risk level 1–3 for ulceration according to the International Working Group on the Diabetic Foot or PAD in the absence of diabetes. Studies required an aspect of peer support in their intervention such as the establishment of virtual or in-person peer support groups or the provision of education and/or treatment to patients in a group setting. One or more outcome measures pertaining to clinical (e.g., amputations, ulcerations, or physical activity), behavioral (e.g., self-care activities), or programmatic (e.g., participant satisfaction or adherence) outcomes were needed for inclusion. Review articles and studies published prior to 2000 were excluded from this review.
Eligibility assessment (Figure 1) was performed by two independent reviewers using the Rayyan software (https://www.rayyan.ai/) (Cambridge, MA, USA) in three stages: abstract and title, full-text screening, and data abstraction. Disputed articles were analyzed by a third reviewer, acting as a tie breaker. A consensus was reached by all reviewers on the included articles. Data was then abstracted from the included articles and compiled into tables. Outcome measures not directly related to lower extremity health, programmatic or behavioral adherence, or social support are not reported in Table 1 or Table 2. A completed Preferred Reporting Items for Systematic reviews and Meta-Analyses extension for Scoping Reviews checklist for this project is available in this publication’s Supplementary Materials.
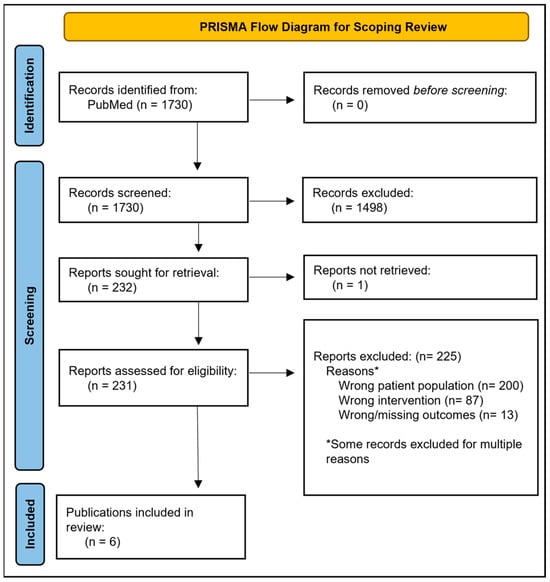
Figure 1.
PRISMA Flow Diagram for Scoping Review.
3. Results
The PubMed search identified 1730 articles (Figure 1). After title and abstract screening, 232 articles were identified for full-text review. One publication could not be retrieved (Qian et al.). Six articles were ultimately found to meet the inclusion criteria. Studies originated from multiple countries with a range of start dates from 2005 to 2016 (Table 1 and Table 2). Study duration ranged from a singular but repeated 2.5 h workshop to 24 months. Four studies were RCTs [18,19,20,21]. The number of patients enrolled varied between studies. Five articles [18,19,20,22,23] focused on populations of patients with diabetes, while McDermott et al. [21]. focused on patients with PAD. The Annersten Gershater et al. [19]. and Vedhara et al. [20]. publications explicitly focused on individuals with a history of prior diabetic foot ulceration. Although not limited to participants with diabetes, the program evaluated by Woodbury et al. [23]. was a peer education program focused on foot health in persons with diabetes. The two remaining publications [18,22] focused on diabetes, studying broader populations of persons with diabetes without specifications of amputation risk factors.

Table 1.
Group foot care education studies.
Table 2.
Group cognitive behavioral studies.
For analysis purposes, the studies were further categorized into two groups based off the method of conduction of the intervention: group foot care education (Table 1) and group cognitive behavioral therapy (Table 2). Four studies utilized group foot care education as an intervention. Utz et al. [22]. and Ahmad Sharoni et al. [18]. provided culturally tailored group sessions. Vedhara et al. [20]. and McDermott et al. [21]. utilized a group cognitive behavioral intervention in populations with diabetes and PAD, respectively. The control groups commonly received only standard care or were provided with educational materials in addition to the original care they were receiving.
3.1. Group Foot Care Education Studies
Outcomes reported included foot care/self-management behaviors and foot complications such as ulceration and amputation (Table 1). Results of the studies varied. Statistically significant and non-statistically significant increases in foot care related outcomes were found by Ahmad Sharoni et al. [18]. and Utz et al. [22], respectively. Annersten Gershater et al. [19]. reported no prevention of ulceration occurrence or significant difference in self-care behaviors with group foot care education in an underpowered study. Increased self-management with limited foot complications was reported by Woodbury et al. [23] in a non-statistical analysis.
3.2. Group Cognitive Behavioral Intervention Studies
Outcomes reported included ulceration, social support, self-care behaviors, qualitative feedback, and physical activity (Table 2). Based on the results of the two studies, group cognitive behavioral intervention can lead to improvement in outcomes such as social support and self-care behaviors in diabetes populations and physical activity in PAD populations at risk of lower limb amputations. Vedhara et al. [20]. reported an equal occurrence of ulceration between groups and did not conduct a statistical analysis.
4. Discussion
This scoping review indicates that there is varying evidence regarding peer support interventions in patients with diabetes or PAD at risk for lower limb amputation. The current literature represents a diverse range of studies analyzing a variety of peer support intervention methods and limb preservation-related outcomes. No conclusions can be drawn from the available evidence published due to the heterogeneity in peer support definitions, study designs, reported outcome measures, and inclusion/exclusion criteria. The population of interest in Utz et al. [22]. was African Americans with type 2 diabetes mellitus, a patient demographic with an increased risk for amputations. Outcome measures are often collected through subjective tools such as questionnaires and interviews, and many studies do not statistically analyze their data. In this review, two out of six studies did not include statistical analysis. Additionally, difficulty with recruiting patients or study volunteers was common in the studies. Annersten Gershater et al. [19]. reported a statistically higher ulceration rate at 12 months in the intervention group but cautioned that this was likely due to their smaller sample size. More objective, clinical outcome measures in higher-powered studies are needed to deduce the influence of peer support interventions on amputation prevention.
The idea of using peer support to prevent gangrene and associated amputations in persons with diabetes was proposed by Joslin almost a century ago [24]. With respect to diabetic gangrene, he noted, “Perhaps the best preventative measure of all which we have at the hospital is the exhibition to new-comers of a few patients who have had gangrene and amputations of a leg or a toe… Visiting diabetics cannot help drawing useful lessons from the causes of their gangrene but also from the good spirits which they show (p. 18).” This historic perspective underscores the long-recognized importance of social support in managing diabetes-related complications. However, our review reveals mixed evidence regarding the effectiveness of peer support interventions on amputation prevention. Furthermore, the degree of social support involved in each intervention varied. Social support post-intervention was only measured by Vedhara et al. [20]. The method of delivery of the intervention should be analyzed for its effectiveness in providing patient-perceived social support, which may have an impact on the study’s outcomes.
A limitation of publications identified in this review include the lack of thorough documentation of participants’ risk for ulceration/amputation in three [18,22,23] out of six studies. Some enrolled participants in those studies were likely at the lowest level of risk, and study results were not reported according to risk level. Notably, Woodbury et al. [23]. collected data and reported outcome measures from their participants, which included patients with diabetes, family members, and healthcare professionals. Only outcomes from the patients with diabetes in the Woodbury et al. study are reported in this scoping review. Ahmad Sharoni et al. [18]. included patients with or without diabetic foot problems, and Utz et al. [22]. reported neuropathic symptoms in 23.8% of their patients with diabetes. Both studies did not further specify risk. Additionally, all studies focused on lower extremity health education or outcomes with the exception of Utz et al. [22], which was a general diabetes management study with two foot care-related outcomes but no specific emphasis on the lower extremity.
Further studies are needed to draw direct conclusions on the effects of peer support intervention on lower limb preservation. Quantitative outcomes with statistical analysis are important to form a consensus; however, qualitative feedback from participants is necessary to ensure that the intervention provided produces the desired peer support. Future research should focus on the development of a standardized protocol to deliver peer support interventions to individuals at risk for an amputation. A standardized intervention will allow for easier implementation for clinical use and can help create a better understanding of the role peer support can play in amputation prevention. Limb preservation requires a holistic approach; a patient’s psychological, social, and physical needs should all be addressed.
5. Conclusions
The six articles included in this review were categorized based on intervention as either a group foot care education study or group cognitive behavioral study. Results from the group foot care education varied, ranging from no effect to significant improvements in foot care, self-management, and complications. Group cognitive behavioral studies showed improvements in outcomes that reduce the likelihood of limb amputation such as self-care behaviors and physical activity. Given the heterogeneity of study design and outcome measures, further randomized controlled trials focusing on peer support interventions and limb preservation outcomes are needed to establish their efficacy compared with standard foot education.
Supplementary Materials
The following supporting information can be downloaded at https://www.mdpi.com/article/10.3390/japma116030039/s1, PRISMA-ScR Checklist [25].
Author Contributions
Conceptualization, S.A.S. and R.T.C.; methodology, R.T.C.; validation of search string, S.A.S., R.T.C., T.-W.T. and D.G.A.; literature screening, S.A.S., B.M.C., S.N.J., M.S.J. and R.T.C.; data extraction, S.A.S., B.M.C. and S.N.J.; writing—original draft preparation, S.A.S.; writing—review and editing, B.M.C., S.N.J., M.S.J., T.-W.T., D.G.A. and R.T.C. All authors have read and agreed to the published version of the manuscript.
Funding
This project was partially supported by grant number T35DK074390 from the National Institute of Diabetes and Digestive and Kidney Disease. The content is solely the responsibility of the authors and does not represent the official views of the National Institute of Diabetes and Digestive and Kidney Diseases of the National Institutes of Health.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
No new data were created or analyzed in this study. Data sharing is not applicable to this article.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Thorud, J.C.; Plemmons, B.; Buckley, C.J.; Shibuya, N.; Jupiter, D.C. Mortality After Nontraumatic Major Amputation Among Patients With Diabetes and Peripheral Vascular Disease: A Systematic Review. J. Foot Ankle Surg. 2016, 55, 591–599. [Google Scholar] [CrossRef] [PubMed]
- Armstrong, D.G.; Swerdlow, M.A.; Armstrong, A.A.; Conte, M.S.; Padula, W.V.; Bus, S.A. Five year mortality and direct costs of care for people with diabetic foot complications are comparable to cancer. J. Foot Ankle Res. 2020, 13, 16. [Google Scholar] [CrossRef] [PubMed]
- Saelee, R.; Bullard, K.M.; Hora, I.A.; Pavkov, M.E.; Pasquel, F.J.; Holliday, C.S.; Benoit, S.R. Trends and Inequalities in Diabetes-Related Complications Among U.S. Adults, 2000–2020. Diabetes Care 2024, 48, 18–28. [Google Scholar] [CrossRef] [PubMed]
- Pecoraro, R.E.; Reiber, G.E.; Burgess, E.M. Pathways to diabetic limb amputation. Basis for prevention. Diabetes Care 1990, 13, 513–521. [Google Scholar] [CrossRef] [PubMed]
- Fowler, X.P.; Eid, M.A.; Barnes, J.A.; Gladders, B.; Austin, A.M.; Goodney, E.J.; Moore, K.O.; Kearing, S.; Feinberg, M.W.; Bonaca, M.P.; et al. Trends of Concomitant Diabetes and Peripheral Artery Disease and Lower Extremity Amputation in US Medicare Patients, 2007 to 2019. Circ. Cardiovasc. Qual. Outcomes 2023, 16, e009531. [Google Scholar] [CrossRef] [PubMed]
- Govsyeyev, N.; Nehler, M.R.; Low Wang, C.C.; Kavanagh, S.; Hiatt, W.R.; Long, C.; Jones, W.S.; Fowkes, F.G.R.; Berger, J.S.; Baumgartner, I.; et al. Etiology and outcomes of amputation in patients with peripheral artery disease in the EUCLID trial. J. Vasc. Surg. 2022, 75, 660–670.e663. [Google Scholar] [CrossRef] [PubMed]
- Allison, M.A.; Armstrong, D.G.; Goodney, P.P.; Hamburg, N.M.; Kirksey, L.; Lancaster, K.J.; Mena-Hurtado, C.I.; Misra, S.; Treat-Jacobson, D.J.; White Solaru, K.T.; et al. Health Disparities in Peripheral Artery Disease: A Scientific Statement From the American Heart Association. Circulation 2023, 148, 286–296. [Google Scholar] [CrossRef] [PubMed]
- Armstrong, D.G.; Tan, T.W.; Boulton, A.J.M.; Bus, S.A. Diabetic Foot Ulcers: A Review. JAMA 2023, 330, 62–75. [Google Scholar] [CrossRef] [PubMed]
- Mead, S.; Hilton, D.; Curtis, L. Peer support: A theoretical perspective. Psychiatr. Rehabil. J. 2001, 25, 134–141. [Google Scholar] [CrossRef] [PubMed]
- Dennis, C.L. Peer support within a health care context: A concept analysis. Int. J. Nurs. Stud. 2003, 40, 321–332. [Google Scholar] [CrossRef] [PubMed]
- Azmiardi, A.; Murti, B.; Febrinasari, R.P.; Tamtomo, D.G. Low Social Support and Risk for Depression in People With Type 2 Diabetes Mellitus: A Systematic Review and Meta-analysis. J. Prev. Med. Public. Health 2022, 55, 37–48. [Google Scholar] [CrossRef] [PubMed]
- Ramkisson, S.; Pillay, B.J.; Sibanda, W. Social support and coping in adults with type 2 diabetes. Afr. J. Prim. Health Care Fam. Med. 2017, 9, e1–e8. [Google Scholar] [CrossRef] [PubMed]
- Spencer-Bonilla, G.; Ponce, O.J.; Rodriguez-Gutierrez, R.; Alvarez-Villalobos, N.; Erwin, P.J.; Larrea-Mantilla, L.; Rogers, A.; Montori, V.M. A systematic review and meta-analysis of trials of social network interventions in type 2 diabetes. BMJ Open 2017, 7, e016506. [Google Scholar] [CrossRef] [PubMed]
- Patil, S.J.; Ruppar, T.; Koopman, R.J.; Lindbloom, E.J.; Elliott, S.G.; Mehr, D.R.; Conn, V.S. Peer Support Interventions for Adults With Diabetes: A Meta-Analysis of Hemoglobin A(1c) Outcomes. Ann. Fam. Med. 2016, 14, 540–551. [Google Scholar] [CrossRef] [PubMed]
- Song, Y.; Nam, S.; Park, S.; Shin, I.S.; Ku, B.J. The Impact of Social Support on Self-care of Patients With Diabetes: What Is the Effect of Diabetes Type? Systematic Review and Meta-analysis. Diabetes Educ. 2017, 43, 396–412. [Google Scholar] [CrossRef] [PubMed]
- Litchman, M.L.; Oser, T.K.; Hodgson, L.; Heyman, M.; Walker, H.R.; Deroze, P.; Rinker, J.; Warshaw, H. In-Person and Technology-Mediated Peer Support in Diabetes Care: A Systematic Review of Reviews and Gap Analysis. Diabetes Educ. 2020, 46, 230–241. [Google Scholar] [CrossRef] [PubMed]
- Whitford, D.L.; Paul, G.; Smith, S.M. Patient generated "frequently asked questions": Identifying informational needs in a RCT of peer support in type 2 diabetes. Prim. Care Diabetes 2013, 7, 103–109. [Google Scholar] [CrossRef] [PubMed]
- Ahmad Sharoni, S.K.; Abdul Rahman, H.; Minhat, H.S.; Shariff-Ghazali, S.; Azman Ong, M.H. The effects of self-efficacy enhancing program on foot self-care behaviour of older adults with diabetes: A randomised controlled trial in elderly care facility, Peninsular Malaysia. PLoS ONE 2018, 13, e0192417. [Google Scholar] [CrossRef] [PubMed]
- Annersten Gershater, M.; Apelqvist, J.; Alm Roijer, C. Re-Ulceration Is Common in Persons with Diabetes and Healed Foot Ulcer After Participant-Driven Education in Group: A Randomized Controlled Trial. Adv. Wound Care 2023, 12, 117–126. [Google Scholar] [CrossRef] [PubMed]
- Vedhara, K.; Beattie, A.; Metcalfe, C.; Roche, S.; Weinman, J.; Cullum, N.; Price, P.; Dayan, C.; Cooper, A.R.; Campbell, R.; et al. Development and preliminary evaluation of a psychosocial intervention for modifying psychosocial risk factors associated with foot re-ulceration in diabetes. Behav. Res. Ther. 2012, 50, 323–332. [Google Scholar] [CrossRef] [PubMed]
- McDermott, M.M.; Guralnik, J.M.; Criqui, M.H.; Ferrucci, L.; Zhao, L.; Liu, K.; Domanchuk, K.; Spring, B.; Tian, L.; Kibbe, M.; et al. Home-based walking exercise in peripheral artery disease: 12-month follow-up of the GOALS randomized trial. J. Am. Heart Assoc. 2014, 3, e000711. [Google Scholar] [CrossRef] [PubMed]
- Utz, S.W.; Williams, I.C.; Jones, R.; Hinton, I.; Alexander, G.; Yan, G.; Moore, C.; Blankenship, J.; Steeves, R.; Oliver, M.N. Culturally tailored intervention for rural African Americans with type 2 diabetes. Diabetes Educ. 2008, 34, 854–865. [Google Scholar] [CrossRef] [PubMed]
- Woodbury, M.G.; Botros, M.; Kuhnke, J.L.; Greene, J. Evaluation of a peer-led self-management education programme PEP Talk: Diabetes, Healthy Feet and You. Int. Wound J. 2013, 10, 703–711. [Google Scholar] [CrossRef] [PubMed]
- Joslin, E.P. The menace of diabetic gangrene. N. Engl. J. Med. 1934, 211, 16–20. [Google Scholar] [CrossRef]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.; Horsley, T.; Weeks, L.; et al. PRISMA Extension for Scoping Reviews (PRISMAScR): Checklist and Explanation. Ann. Intern Med. 2018, 169, 467–473. [Google Scholar] [CrossRef] [PubMed]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Published by MDPI on behalf of the American Podiatric Medical Association (APMA). Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license.