Neuroscience in Anesthesiology
Share This Topical Collection
Editor
 Prof. Dr. Young-Tae Jeon
Prof. Dr. Young-Tae Jeon
Prof. Dr. Young-Tae Jeon
E-Mail
Guest Editor
Department of Anaesthesiology and Pain Medicine, Seoul National University Bundang Hospital, Seongnam 13620, Republic of Korea
Interests: analgesia and anesthesia; anesthesia; brain tumor; cerebral aneurysm; neurosurgery; spine
Topical Collection Information
Dear Colleagues,
Numerous neurosurgical situations remain as problematic issues to anesthesiologists. An agreed understanding between surgeon and anesthesiologist should be established. Outstanding research ongoing at this time may provide window to the approaches to these problems and optimize outcomes for their patients.
Neuroscience in Anesthesiology includes many research areas that can be translated to clinical care of neurosurgical patients in the operating room and neurointensive care unit. Research areas extend to clinical neurosurgical anesthesia for brain and spine disease and neurocritical care, foundational neuroscience in anesthesiology, and neurologic outcomes after non-neurologic surgery, as well as systematic review of the studies in the literature.
Anesthesiologists’ efforts have led to significant advances in neuroanesthesia and neurocritical care.
Continuing this endeavor to develop neuroscience in anesthesiology, the Journal of Clinical Medicine will publish this Special Issue devoted to the topic of “Neuroscience in Anesthesiology”.
Prof. Dr. Young-Tae Jeon
Guest Editor
Manuscript Submission Information
Manuscripts should be submitted online at www.mdpi.com by registering and logging in to this website. Once you are registered, click here to go to the submission form. All submissions that pass pre-check are peer-reviewed. Accepted papers will be published continuously in the journal (as soon as accepted) and will be listed together on the collection website. Research articles, review articles as well as short communications are invited. For planned papers, a title and short abstract (about 250 words) can be sent to the Editorial Office for assessment.
Submitted manuscripts should not have been published previously, nor be under consideration for publication elsewhere (except conference proceedings papers). All manuscripts are thoroughly refereed through a single-blind peer-review process. A guide for authors and other relevant information for submission of manuscripts is available on the Instructions for Authors page. Journal of Clinical Medicine is an international peer-reviewed open access semimonthly journal published by MDPI.
Please visit the Instructions for Authors page before submitting a manuscript.
The Article Processing Charge (APC) for publication in this open access journal is 2600 CHF (Swiss Francs).
Submitted papers should be well formatted and use good English. Authors may use MDPI's
English editing service prior to publication or during author revisions.
Keywords
- anesthesia
- brain tumor
- cerebral aneurysm
- neuroanesthesia
- neurosurgery
- spine
Published Papers (10 papers)
Open AccessArticle
Propofol-Based Anesthesia Maintenance and/or Volatile Anesthetics during Intracranial Aneurysm Repair: A Comparative Analysis of Neurological Outcomes
by
Shooka Esmaeeli, Negar Motayagheni, Andres Brenes Bastos, Christopher S Ogilvy, Ajith J Thomas, Richard Pollard, Lauren K Buhl, Maxwell B Baker, Sheshanna Phan, Omron Hassan, Corey R Fehnel, Matthias Eikermann, Shahzad Shaefi and Ala Nozari
Cited by 4 | Viewed by 4234
Abstract
Background: Volatile and intravenous anesthetics have substantial effects on physiological functions, notably influencing neurological function and susceptibility to injury. Despite the importance of the anesthetic approach, data on its relative risks or benefits during surgical clipping or endovascular treatments for unruptured intracranial aneurysms
[...] Read more.
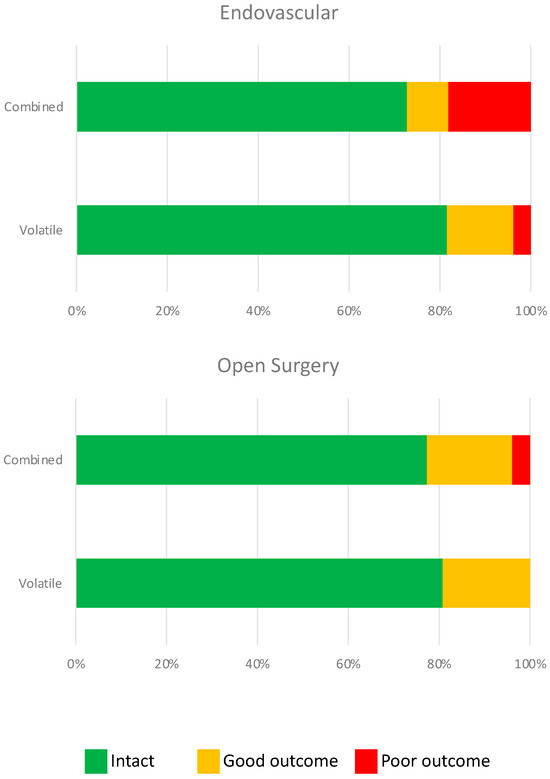
Background: Volatile and intravenous anesthetics have substantial effects on physiological functions, notably influencing neurological function and susceptibility to injury. Despite the importance of the anesthetic approach, data on its relative risks or benefits during surgical clipping or endovascular treatments for unruptured intracranial aneurysms (UIAs) remains scant. We investigated whether using volatile anesthetics alone or in combination with propofol infusion yields superior neurological outcomes following UIA obliteration. Methods: We retrospectively reviewed 1001 patients who underwent open or endovascular treatment for UIA, of whom 596 had short- and long-term neurological outcome data (modified Rankin Scale) recorded. Multivariable ordinal regression analysis was performed to examine the association between the anesthetic approach and outcomes. Results: Of 1001 patients, 765 received volatile anesthetics alone, while 236 received propofol infusion and volatile anesthetics (combined anesthetic group). Short-term neurological outcome data were available for 619 patients and long-term data for 596. No significant correlation was found between the anesthetic approach and neurologic outcomes, irrespective of the type of procedure (open craniotomy or endovascular treatment). The combined anesthetic group had a higher rate of ICU admission (
p < 0.001) and longer ICU and hospital length of stay (LOS,
p < 0.001). Similarly, a subgroup analysis revealed longer ICU and hospital LOS (
p < 0.0001 and
p < 0.001, respectively) in patients who underwent endovascular UIA obliteration under a combined anesthetic approach (n = 678). Conclusions: The addition of propofol to volatile anesthetics during UIA obliteration does not provide short- or long-term benefits to neurologic outcomes. Compared to volatile anesthetics alone, the combination of propofol and volatile anesthetics may be associated with an increased rate of ICU admission, as well as longer ICU and hospital LOS.
Full article
►▼
Show Figures
Open AccessArticle
Refraining from Packed Red Blood Cells in Cardiopulmonary Bypass Priming as a Method of Neuroprotection in Pediatric Cardiac Surgery
by
Artem A. Ivkin, Evgeny Grigoriev and Anna V. Sinitskaya
Cited by 4 | Viewed by 2698
Abstract
Congenital heart defect (CHD) surgeries are performed with cardiopulmonary bypass (CPB) and are complicated by several factors that affect the child’s brain. However, to date, the number of studies on brain protection in cardiac surgery remains small. The aim of this study was
[...] Read more.
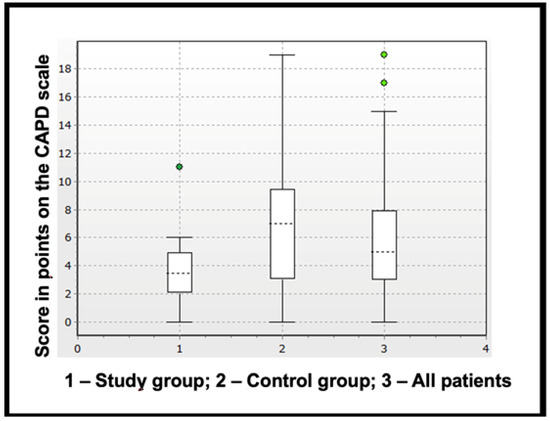
Congenital heart defect (CHD) surgeries are performed with cardiopulmonary bypass (CPB) and are complicated by several factors that affect the child’s brain. However, to date, the number of studies on brain protection in cardiac surgery remains small. The aim of this study was to assess the impact of refraining from using packed red blood cells (PRBCs) in priming solutions in children with congenital defects (CHDs) who require surgical interventions using CPB to prevent brain injury in the postoperative period. Material and methods: This study included 40 children, and the mean age was 14 (12–22.5) months and the mean weight was 8.8 (7.25–11) kg. All patients underwent CHD closure using CPB. The patients were divided into two groups depending on the use of PRBCs in the priming solution. Brain injury was assessed using three specific blood serum markers, namely S100 calcium-binding protein β (S100β), neuron-specific enolase (NSE) and glial fibrillary acidic protein (GFAP) before surgery, after the completion of CPB and 16 h after surgery (first, second and third control points). Markers of systemic inflammatory response were also analyzed, including interleukin-1, -6, -10 and tumor necrosis factor alpha (TNF-α). A clinical assessment of brain injury was carried out using a valid, rapid, observational tool for screening delirium in children of this age group, i.e., “Cornell Assessment of Pediatric Delirium”. Results: Factors of the intra- and postoperative period were analyzed, such as hemoglobin levels, oxygen delivery (cerebral tissue oxygenation, blood lactate level and venous oxygen saturation) and indicators of organ dysfunction (creatinine, urea, bilirubin levels, duration of CPB and length of stay in the ICU). Following the procedure, there were no significant differences between the groups and all indicators were within the reference values, thus demonstrating the safety of CHD closure without transfusion. Moreover, the highest level of specific markers of brain injury were noted immediately after the completion of CPB in both groups. The concentration of all three markers was significantly higher in the group with transfusion after the completion of CPB. Moreover, GFAP levels were higher in the transfusion group and 16 h after surgery. Conclusions: The results of the study show the safety and effectiveness of brain injury prevention strategies that consist of not conducting PRBC transfusion.
Full article
►▼
Show Figures
Open AccessArticle
Preoperative Serum Alkaline Phosphatase and Neurological Outcome of Cerebrovascular Surgery
by
Seongjoo Park, Eun-Su Choi, Hee-Won Jung, Ji-Youn Lee, Jin-Woo Park, Jae-Seung Bang and Yeong-Tae Jeon
Cited by 2 | Viewed by 2610
Abstract
This study evaluated the relationship between the preoperative alkaline phosphatase (ALP) level and major postoperative neurological complications in patients undergoing cerebral bypass surgery. This was a retrospective analysis of a prospective database of all patients undergoing cerebral bypass surgery after a diagnosis of
[...] Read more.
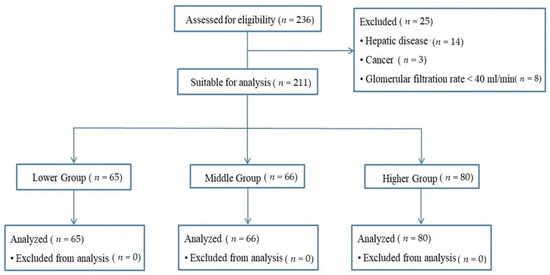
This study evaluated the relationship between the preoperative alkaline phosphatase (ALP) level and major postoperative neurological complications in patients undergoing cerebral bypass surgery. This was a retrospective analysis of a prospective database of all patients undergoing cerebral bypass surgery after a diagnosis of cerebrovascular stenosis or occlusion between May 2003 and August 2017. The patients were divided into tertiles based on serum alkaline phosphatase (ALP) levels (low: <63, intermediate: 63~79, and high: ALP > 79 IU/mL). The incidence of neurological events according to ALP level was analyzed. The study analyzed 211 cases. The incidence of acute infarction was highest in the third serum ALP tertile (5.7% vs. 2.9% vs. 16.9% in the first, second, and third tertile, respectively,
p = 0.007). Logistic regression analysis showed that the third tertile of serum ALP was an independent predictor of acute cerebral infarction (odds ratio 3.346, 95% confidence interval 1.026–10.984,
p = 0.045). On Kaplan–Meier time-to-event curves, the incidence of acute infarction increased significantly with ALP (log rank = 0.048). Preoperative serum ALP level can be used as a biomarker to predict acute cerebral infarction in patients undergoing cerebral bypass surgery for vascular stenosis or occlusion.
Full article
►▼
Show Figures
Open AccessArticle
Effect of Dexmedetomidine on Early Postoperative Cognitive Function in Patients Undergoing Arthroscopic Shoulder Surgery in Beach Chair Position: A Randomized Double-Blind Study
by
Namo Kim, Kwan Hyung Kim, Yong Seon Choi, Sei Han Song and Seung Ho Choi
Cited by 7 | Viewed by 2493
Abstract
This study sought to determine whether intraoperative dexmedetomidine infusion might reduce the incidence of postoperative cognitive dysfunction (POCD) and alleviate the neuroinflammatory response in patients who have undergone arthroscopic shoulder surgery. A total of 80 patients over 60 years of age who had
[...] Read more.
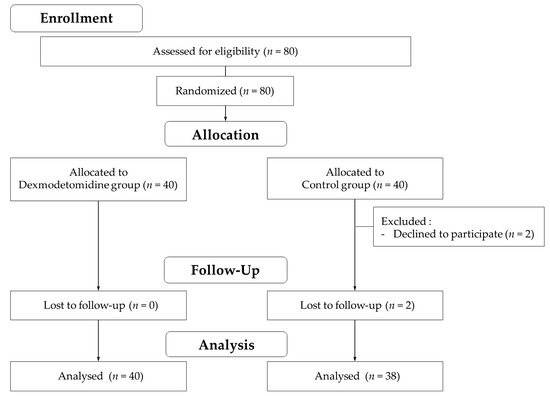
This study sought to determine whether intraoperative dexmedetomidine infusion might reduce the incidence of postoperative cognitive dysfunction (POCD) and alleviate the neuroinflammatory response in patients who have undergone arthroscopic shoulder surgery. A total of 80 patients over 60 years of age who had undergone arthroscopic shoulder surgery in the beach chair position were randomly allocated to either the dexmedetomidine group (Group D) or the control group (Group C). Dexmedetomidine (0.6 μg/kg/h) or a comparable amount of normal saline was infused into each group during the surgery. The early incidence of POCD was assessed by comparing cognitive tests on the day before and 1 d after surgery. The neuroinflammatory response with the S100 calcium-binding protein B (S100β) assay was compared prior to anesthetic induction and 1 h following surgery. The incidence of POCD was comparable between groups D (
n = 9, 22.5%) and C (
n = 9, 23.7%) (
p = 0.901). However, the results of the cognitive test revealed a significant difference between the groups after surgery (
p = 0.004). Although the S100β levels measured at the end of surgery were significantly higher than those at baseline in both groups (
p < 0.001), there was no difference between the groups after the surgery (
p = 0.236). Our results suggest that intraoperative dexmedetomidine infusion neither reduce the incidence of early POCD nor alleviated the neuroinflammatory response in patients undergoing arthroscopic shoulder surgery.
Full article
►▼
Show Figures
Open AccessArticle
Spectral Entropy Monitoring Accelerates the Emergence from Sevoflurane Anesthesia in Thoracic Surgery: A Randomized Controlled Trial
by
Jui-Tai Chen, Yu-Ming Wu, Tung-Yu Tiong, Juan P. Cata, Kuang-Tai Kuo, Chun-Cheng Li, Hsin-Yi Liu, Yih-Giun Cherng, Hsiang-Ling Wu and Ying-Hsuan Tai
Cited by 7 | Viewed by 4219
Abstract
The clinical efficacy of spectral entropy monitoring in improving postoperative recovery remains unclear. This trial aimed to investigate the impact of M-Entropy (GE Healthcare, Helsinki, Finland) guidance on emergence from anesthesia and postoperative delirium in thoracic surgery. Adult patients undergoing video-assisted thoracoscopic surgery
[...] Read more.
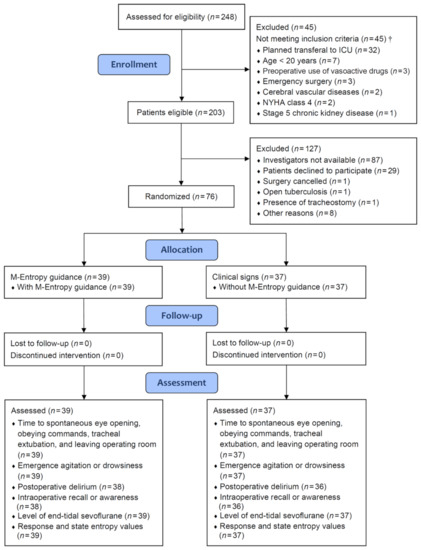
The clinical efficacy of spectral entropy monitoring in improving postoperative recovery remains unclear. This trial aimed to investigate the impact of M-Entropy (GE Healthcare, Helsinki, Finland) guidance on emergence from anesthesia and postoperative delirium in thoracic surgery. Adult patients undergoing video-assisted thoracoscopic surgery for lung resection at a medical center were randomly allocated into the M-Entropy guidance group (
n = 39) and the control group (
n = 37). In the M-Entropy guidance group, sevoflurane anesthesia was titrated to maintain response and state entropy values between 40 and 60 intraoperatively. In the control group, the dosing of sevoflurane was adjusted based on clinical judgment and vital signs. The primary outcome was time to spontaneous eye opening. M-Entropy guidance significantly reduced the time proportion of deep anesthesia (entropy value <40) during surgery, mean difference: −21.5% (95% confidence interval (CI): −32.7 to −10.3) for response entropy and −24.2% (−36.3 to −12.2) for state entropy. M-Entropy guidance significantly shortened time to spontaneous eye opening compared to clinical signs, mean difference: −154 s (95% CI: −259 to −49). In addition, patients of the M-Entropy group had a lower rate of emergence agitation (absolute risk reduction: 0.166, 95% CI: 0.005–0.328) and delirium (0.245, 0.093–0.396) at the postanesthesia care unit. M-Entropy-guided anesthesia hastened awakening and potentially prevented emergence agitation and delirium after thoracic surgery. These results may provide an implication for facilitating postoperative recovery and reducing the complications associated with delayed emergence and delirium.
Full article
►▼
Show Figures
Open AccessArticle
Recovery Profiles of Sevoflurane and Desflurane with or without M-Entropy Guidance in Obese Patients: A Randomized Controlled Trial
by
Yu-Ming Wu, Yen-Hao Su, Shih-Yu Huang, Po-Han Lo, Jui-Tai Chen, Hung-Chi Chang, Yun-Ling Yang, Yih-Giun Cherng, Hsiang-Ling Wu and Ying-Hsuan Tai
Cited by 7 | Viewed by 3884
Abstract
Obesity increases the risk of prolonged emergence from general anesthesia due to the delayed release of anesthetic agents from body fat. This trial aimed to evaluate the effects of sevoflurane and desflurane along with anesthetic depth monitoring on emergence time from anesthesia in
[...] Read more.
Obesity increases the risk of prolonged emergence from general anesthesia due to the delayed release of anesthetic agents from body fat. This trial aimed to evaluate the effects of sevoflurane and desflurane along with anesthetic depth monitoring on emergence time from anesthesia in obese patients. Adults with a body mass index ≥ 30 kg·m
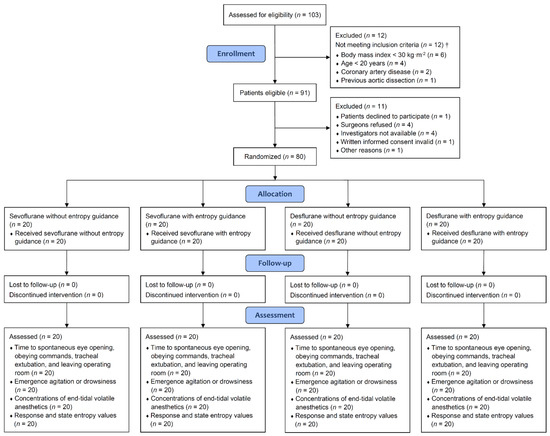
−2 undergoing laparoscopic sleeve gastrectomy at a medical center were randomized into four groups: sevoflurane or desflurane anesthesia with or without M-Entropy guidance on anesthetic depth in a ratio of 1:1:1:1. In the M-Entropy guidance groups, the dosage of sevoflurane and desflurane was adjusted to achieve response and state entropy values between 40 and 60 during surgery. In the non-M-Entropy guidance groups, the dosage of anesthetics was titrated according to clinical signs. Primary outcome was time to spontaneous eye opening. A total of 80 participants were randomized. Compared to sevoflurane, desflurane anesthesia significantly reduced the time to spontaneous eye opening [mean difference (MD): −129 s; 95% confidence interval (CI): −211, −46], obeying commands (−160; −243, −77), tracheal extubation (−172; −266, −78), and leaving operating room (−148; −243, −54). M-Entropy guidance further reduced time to eye opening (MD: −142 s; 99.2% CI: −276, −8), tracheal extubation (−199; −379, −19), and leaving operating room (−190; −358, −23) in the desflurane but not the sevoflurane group. M-Entropy guidance significantly reduced the risk of agitation during emergence, i.e., risk difference: −0.275 (95% CI: −0.464, −0.086); and number needed to treat: 4. Compared to sevoflurane, using desflurane to maintain general anesthesia accelerated the return of consciousness in obese patients. M-Entropy guidance further hastened awakening in patients using desflurane and prevented emergence agitation.
Full article
►▼
Show Figures
Open AccessArticle
Discrepant End-Tidal Concentrations of Sevoflurane at the Same A-Line Autoregressive Index Level during Induction of General Anesthesia: An Observational Study
by
Che-Hao Hsu, Shung-Tai Ho, Chih-Cherng Lu, Ju-O Wang, Te-Chun Yeh and Tso-Chou Lin
Cited by 2 | Viewed by 2956
Abstract
Background: The A-Line Autoregressive Index (AAI), which is derived from auditory evoked potentials, has been used for determining anesthetic depth. This study verified the correlation between AAI values and the corresponding end-tidal concentrations of sevoflurane during general anesthesia induction. Methods: Thirty young male
[...] Read more.
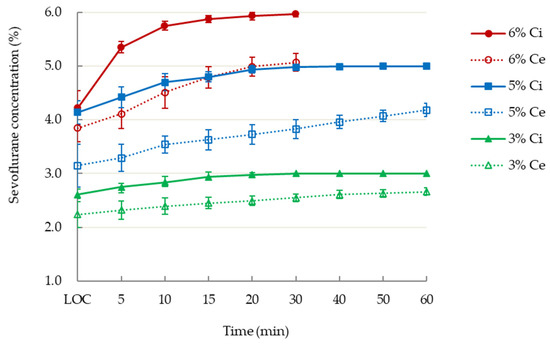
Background: The A-Line Autoregressive Index (AAI), which is derived from auditory evoked potentials, has been used for determining anesthetic depth. This study verified the correlation between AAI values and the corresponding end-tidal concentrations of sevoflurane during general anesthesia induction. Methods: Thirty young male adults undergoing elective minor orthopedic surgery were sequentially allocated to receive inspiratory 3%, 5%, or 6% sevoflurane for mask induction, followed by mechanical ventilation after tracheal intubation. The inspiratory, end-tidal and estimated jugular bulb concentrations of sevoflurane were recorded at three target AAI values: below 20, below 10, and at the start of burst suppression. Results: The mean time to loss of consciousness in the 6% sevoflurane group was shorter than that in the 5% and 3% groups; however, the groups had comparable AAI values (range: 16–45). The 6% group had a higher end-tidal concentration (4.5% ± 0.2% vs. 3.8% ± 0.2%,
p < 0.05) than did the 5% group, despite having the same target anesthetic levels by AAI score ≤10, whereas the estimated jugular bulb concentrations were comparable (1.9% vs. 1.9%) in both groups. Conclusions: Following mechanical ventilation with inspiratory 3%, 5%, or 6% sevoflurane, the end-tidal concentrations were discrepant at the same end points of AAI levels, despite similar estimated jugular bulb concentrations of sevoflurane. Thus, conventional alveolar concentration may overestimate anesthesia depth during rapid wash-in of sevoflurane.
Full article
►▼
Show Figures
Open AccessArticle
Blood Pressure and Transient Postoperative Neurologic Deterioration, Following Superficial Temporal-to-Middle Cerebral Artery Anastomosis in Adult Patients with Moyamoya Disease: A Retrospective Cohort Study
by
Tak-Kyu Oh, Ji-Hyeon Kim, Ho-Young Lee, Seong-Eun Kim, Tac-Keun Kim, Jae-Seung Bang, Moon-Ku Han, Chang-Wan Oh, Hee-Joon Bae and Young-Tae Jeon
Cited by 3 | Viewed by 2712
Abstract
We investigated whether intraoperative systolic blood pressure (ISBP) is associated with the risk of transient neurologic deficits (TND) following superficial temporal-to-middle cerebral artery (STA-MCA) anastomosis in adult patients with moyamoya disease (MMD). In this retrospective observational study, data from adult patients with MMD
[...] Read more.
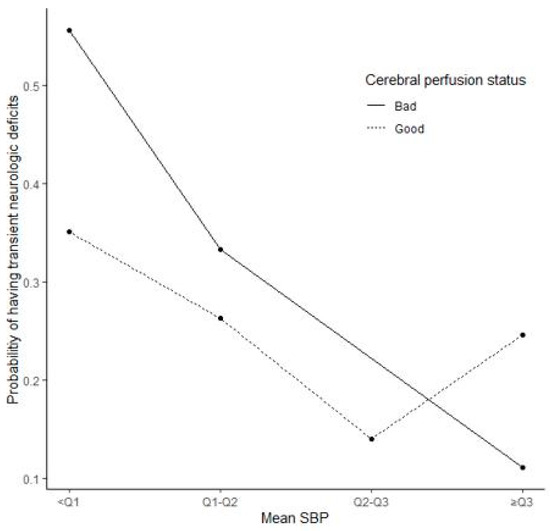
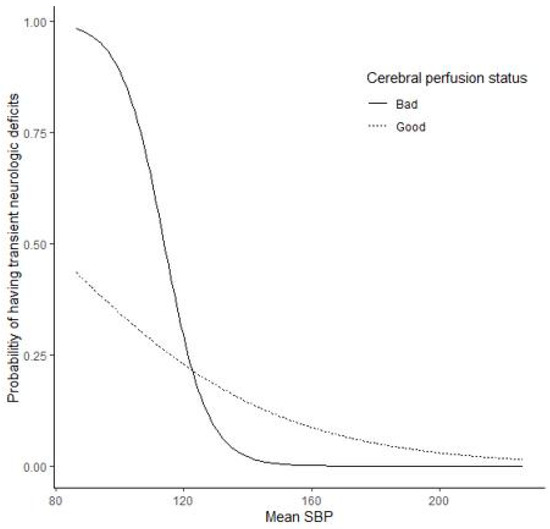
We investigated whether intraoperative systolic blood pressure (ISBP) is associated with the risk of transient neurologic deficits (TND) following superficial temporal-to-middle cerebral artery (STA-MCA) anastomosis in adult patients with moyamoya disease (MMD). In this retrospective observational study, data from adult patients with MMD who had undergone STA-MCA anastomosis at a single tertiary academic hospital during May 2003–April 2014 were examined. Data on patient characteristics were obtained from electronic medical records, including the details of comorbidities and laboratory findings. TND was the primary outcome of interest. Out of 192 patients (228 hemispheres), 66 (29%) hemispheres had TND after surgery. There were significant differences in ISBP between patients with and without TND. The lowest ISBP quartile was independently associated with TND (odds ratio: 5.50; 95% confidence interval: 1.96–15.46). Low ISBP might lead to TND after STA-MCA anastomosis in adult patients with MMD. In patients with poor perfusion status, low ISBP was associated with an increased risk of TND. Our findings suggest that strict ISBP control might be required to prevent TND after anastomosis in patients with MMD, in particular, in patients with poor perfusion status. Given limitations due to the retrospective design, further studies are needed to clarify these findings.
Full article
►▼
Show Figures
Open AccessArticle
Platelet Receptor Activity for Predicting Survival in Patients with Intracranial Bleeding
by
Barbara Dragan, Barbara Adamik, Malgorzata Burzynska, Szymon Lukasz Dragan and Waldemar Gozdzik
Cited by 4 | Viewed by 3255
Abstract
Blood coagulation disorders in patients with intracranial bleeding as a result of head injuries or ruptured aneurysms are a diagnostic and therapeutic problem and appropriate assessments are needed to limit CNS damage and to implement preventive measures. The aim of the study was
[...] Read more.
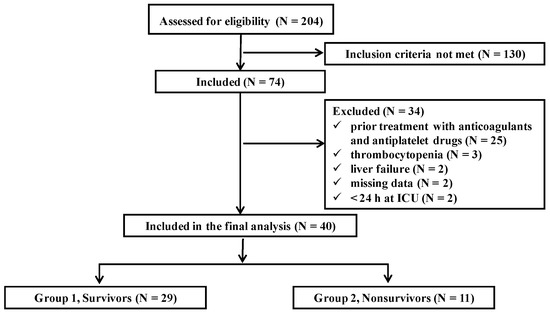
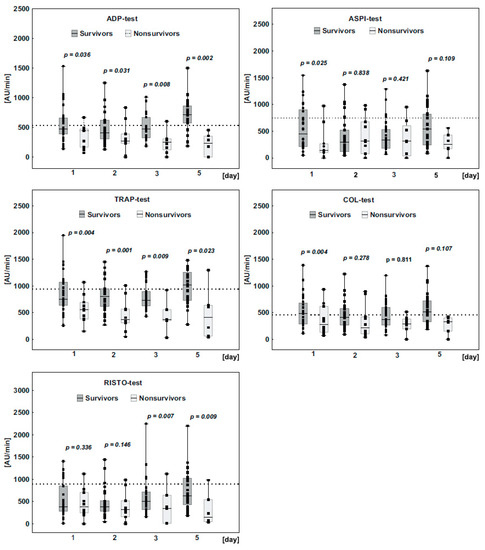
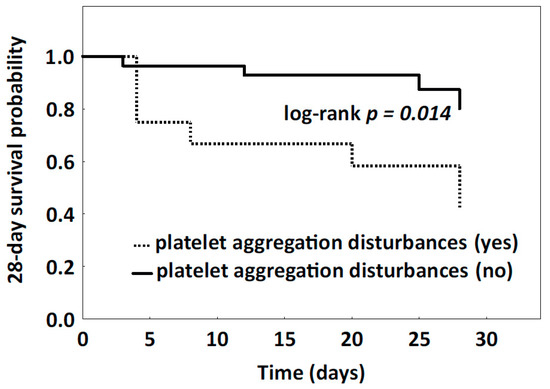
Blood coagulation disorders in patients with intracranial bleeding as a result of head injuries or ruptured aneurysms are a diagnostic and therapeutic problem and appropriate assessments are needed to limit CNS damage and to implement preventive measures. The aim of the study was to monitor changes in platelet aggregation and to assess the importance of platelet dysfunction for predicting survival. Platelet receptor function analysis was performed using the agonists arachidonic acid (ASPI), adenosine diphosphate (ADP), collagen (COL), thrombin receptor activating protein (TRAP), ristocetin (RISTO) upon admission to the ICU and on days 2, 3, and 5. On admission, the ASPI, ADP, COL, TRAP, and RISTO tests indicated there was reduced platelet aggregation, despite there being a normal platelet count. In ‘Non-survivors’, the platelet response to all agonists was suppressed throughout the study period, while in ‘Survivors’ it improved. Measuring platelet function in ICU patients with intracranial bleeding is a strong predictor related to outcome: patients with impaired platelet aggregation had a lower 28-day survival rate compared to patients with normal platelet aggregation (log-rank test
p = 0.014). The results indicated that measuring platelet aggregation can be helpful in the early detection, diagnosis, and treatment of bleeding disorders.
Full article
►▼
Show Figures
Open AccessArticle
Impact of Procedural Sedation on the Clinical Outcome of Microelectrode Recording Guided Deep Brain Stimulation in Patients with Parkinson’s Disease
by
Michael J. Bos, Dianne de Korte-de Boer, Ana Maria Alzate Sanchez, Annelien Duits, Linda Ackermans, Yasin Temel, Anthony R. Absalom, Wolfgang F. Buhre, Mark J. Roberts and Marcus L. F. Janssen
Cited by 9 | Viewed by 3333
Abstract
Background: Subthalamic nucleus (STN) deep brain stimulation (DBS) has become a routine treatment of advanced Parkinson’s disease (PD). DBS surgery is commonly performed under local anesthesia (LA) to obtain reliable microelectrode recordings. However, procedural sedation and/or analgesia (PSA) is often desirable to improve
[...] Read more.
Background: Subthalamic nucleus (STN) deep brain stimulation (DBS) has become a routine treatment of advanced Parkinson’s disease (PD). DBS surgery is commonly performed under local anesthesia (LA) to obtain reliable microelectrode recordings. However, procedural sedation and/or analgesia (PSA) is often desirable to improve patient comfort. The impact of PSA in addition to LA on outcome is largely unknown. Therefore, we performed an observational study to assess the effect of PSA compared to LA alone during STN DBS surgery on outcome in PD patients. Methods: Seventy PD patients (22 under LA, 48 under LA + PSA) scheduled for STN DBS implantation were included. Dexmedetomidine, clonidine or remifentanil were used for PSA. The primary outcome was the change in Movement Disorders Society Unified Parkinson’s Disease Rating Score III (MDS-UPDRS III) and levodopa equivalent daily dosage (LEDD) between baseline, one month before surgery, and twelve months postoperatively. Secondary outcome measures were motor function during activities of daily living (MDS-UPDRS II), cognitive alterations and surgical adverse events. Postoperative assessment was conducted in “on” stimulation and “on” medication conditions. Results: At twelve months follow-up, UPDRS III and UPDRS II scores in “on” medication conditions were similar between the LA and PSA groups. The two groups showed a similar LEDD reduction and an equivalent decline in executive function measured by the Stroop Color-Word Test, Trail Making Test-B, and verbal fluency. The incidence of perioperative and postoperative adverse events was similar between groups. Conclusion: This study demonstrates that PSA during STN DBS implantation surgery in PD patients was not associated with differences in motor and non-motor outcome after twelve months compared with LA only.
Full article




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}