
Spectral Entropy Monitoring Accelerates the Emergence from Sevoflurane Anesthesia in Thoracic Surgery: A Randomized Controlled Trial

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Clinical Settings
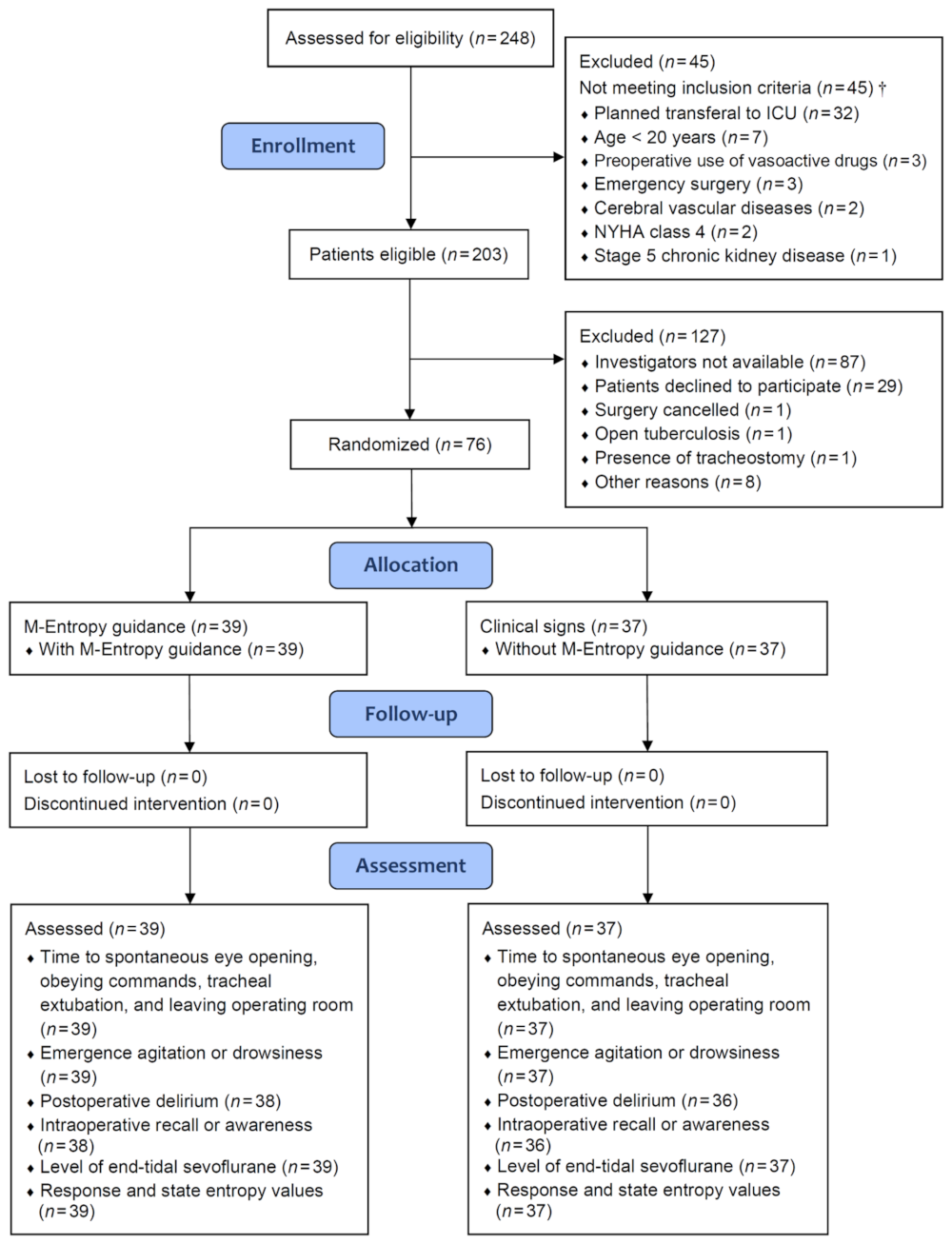
2.2. Randomization Process
2.3. Anesthesia Protocol
2.4. Spectral Entropy Monitoring and Guidance
2.5. Study Outcome
2.6. Statistical Analysis
3. Results
3.1. Baseline Characteristics of the Participants
3.2. Depth of Anesthesia
3.3. Recovery from Anesthesia and Postoperative Delirium
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lumb, A.B.; Slinger, P. Hypoxic pulmonary vasoconstriction: Physiology and anesthetic implications. Anesthesiology 2015, 122, 932–946. [Google Scholar] [CrossRef] [PubMed]
- Campos, J.H.; Feider, A. Hypoxia during one-lung ventilation: A review and update. J. Cardiothorac. Vasc. Anesth. 2018, 32, 2330–2338. [Google Scholar] [CrossRef] [PubMed]
- Dinu, A.R.; Rogobete, A.F.; Popovici, S.E.; Bedreag, O.H.; Papurica, M.; Dumbuleu, C.M.; Velovan, R.R.; Toma, D.; Georgescu, C.M.; Trache, L.I.; et al. Impact of general anesthesia guided by state entropy (SE) and response entropy (RE) on perioperative stability in elective laparoscopic cholecystectomy patients: A prospective observational randomized monocentric study. Entropy 2020, 22, 356. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thomas, E.; Martin, F.; Pollard, B. Delayed recovery of consciousness after general anaesthesia. BJA Educ. 2020, 20, 173–179. [Google Scholar] [CrossRef]
- Hung, M.H.; Chen, J.S.; Cheng, Y.J. Precise anesthesia in thoracoscopic operations. Curr. Opin. Anaesthesiol. 2019, 32, 39–43. [Google Scholar] [CrossRef]
- Pedoto, A.; Perrino, A.C., Jr. Delayed recovery following thoracic surgery: Persistent issues and potential interventions. Curr. Opin. Anaesthesiol. 2019, 32, 3–9. [Google Scholar] [CrossRef] [PubMed]
- Liang, Z.; Wang, Y.; Sun, X.; Li, D.; Voss, L.J.; Sleigh, J.W.; Hagihira, S.; Li, X. EEG entropy measures in anesthesia. Front. Comput. Neurosci. 2015, 9, 16. [Google Scholar] [CrossRef]
- Wu, Y.M.; Su, Y.H.; Huang, S.Y.; Lo, P.H.; Chen, J.T.; Chang, H.C.; Yang, Y.L.; Cherng, Y.G.; Wu, H.L.; Tai, Y.H. Recovery profiles of sevoflurane and desflurane with or without M-Entropy guidance in obese patients: A randomized controlled trial. J. Clin. Med. 2021, 11, 162. [Google Scholar] [CrossRef]
- Lewis, S.R.; Pritchard, M.W.; Fawcett, L.J.; Punjasawadwong, Y. Bispectral index for improving intraoperative awareness and early postoperative recovery in adults. Cochrane Database Syst. Rev. 2019, 9, CD003843. [Google Scholar]
- Vakkuri, A.; Yli-Hankala, A.; Sandin, R.; Mustola, S.; Høymork, S.; Nyblom, S.; Talja, P.; Sampson, T.; van Gils, M.; Viertiö-Oja, H. Spectral entropy monitoring is associated with reduced propofol use and faster emergence in propofol-nitrous oxide-alfentanil anesthesia. Anesthesiology 2005, 103, 274–279. [Google Scholar] [CrossRef]
- Aimé, I.; Verroust, N.; Masson-Lefoll, C.; Taylor, G.; Laloë, P.A.; Liu, N.; Fischler, M. Does monitoring bispectral index or spectral entropy reduce sevoflurane use? Anesth. Analg. 2006, 103, 1469–1477. [Google Scholar] [CrossRef]
- Gruenewald, M.; Zhou, J.; Schloemerkemper, N.; Meybohm, P.; Weiler, N.; Tonner, P.H.; Scholz, J.; Bein, B. M-Entropy guidance vs standard practice during propofol-remifentanil anaesthesia: A randomised controlled trial. Anaesthesia 2007, 62, 1224–1229. [Google Scholar] [CrossRef]
- Ellerkmann, R.K.; Soehle, M.; Riese, G.; Zinserling, J.; Wirz, S.; Hoeft, A.; Bruhn, J. The Entropy Module and Bispectral Index as guidance for propofol-remifentanil anaesthesia in combination with regional anaesthesia compared with a standard clinical practice group. Anaesth. Intensive Care 2010, 38, 159–166. [Google Scholar] [CrossRef] [Green Version]
- Jiahai, M.; Xueyan, W.; Yonggang, X.; Jianhong, Y.; Qunhui, H.; Zhi, L.; Juan, D.; Xiuliang, J. Spectral entropy monitoring reduces anesthetic dosage for patients undergoing off-pump coronary artery bypass graft surgery. J. Cardiothorac. Vasc. Anesth. 2012, 26, 818–821. [Google Scholar] [CrossRef]
- El Hor, T.; Van Der Linden, P.; De Hert, S.; Mélot, C.; Bidgoli, J. Impact of entropy monitoring on volatile anesthetic uptake. Anesthesiology 2013, 118, 868–873. [Google Scholar] [CrossRef] [Green Version]
- Gruenewald, M.; Harju, J.; Preckel, B.; Molnár, Z.; Yli-Hankala, A.; Rosskopf, F.; Koers, L.; Orban, A.; Bein, B.; AoA Study Group. Comparison of adequacy of anaesthesia monitoring with standard clinical practice monitoring during routine general anaesthesia: An international, multicentre, single-blinded randomised controlled trial. Eur. J. Anaesthesiol. 2021, 38, 73–81. [Google Scholar] [CrossRef]
- Boutron, I.; Altman, D.G.; Moher, D.; Schulz, K.F.; Ravaud, P.; CONSORT NPT Group. CONSORT Statement for randomized trials of nonpharmacologic treatments: A 2017 update and a CONSORT extension for nonpharmacologic trial abstracts. Ann. Intern. Med. 2017, 167, 40–47. [Google Scholar] [CrossRef]
- Ling, Y.H.; Tai, Y.H.; Wu, H.L.; Fu, W.L.; Tsou, M.Y.; Chang, K.Y. Evaluating the association of preoperative parecoxib with acute pain trajectories after video-assisted thoracoscopic surgery: A single-centre cohort study in Taiwan. BMJ Open 2021, 11, e038985. [Google Scholar] [CrossRef]
- Ely, E.W.; Truman, B.; Shintani, A.; Thomason, J.W.; Wheeler, A.P.; Gordon, S.; Francis, J.; Speroff, T.; Gautam, S.; Margolin, R.; et al. Monitoring sedation status over time in ICU patients: Reliability and validity of the Richmond Agitation-Sedation Scale (RASS). JAMA 2003, 289, 2983–2991. [Google Scholar] [CrossRef] [Green Version]
- Inouye, S.K.; van Dyck, C.H.; Alessi, C.A.; Balkin, S.; Siegal, A.P.; Horwitz, R.I. Clarifying confusion: The confusion assessment method. A new method for detection of delirium. Ann. Intern. Med. 1990, 113, 941–948. [Google Scholar] [CrossRef]
- Brice, D.D.; Hetherington, R.R.; Utting, J.E. A simple study of awareness and dreaming during anaesthesia. Br. J. Anaesth. 1970, 42, 535–542. [Google Scholar] [CrossRef]
- Chhabra, A.; Subramaniam, R.; Srivastava, A.; Prabhakar, H.; Kalaivani, M.; Paranjape, S. Spectral entropy monitoring for adults and children undergoing general anaesthesia. Cochrane Database Syst. Rev. 2016, 3, CD010135. [Google Scholar] [CrossRef]
- Armitage, P.; Berry, G.; Matthews, J.N.S. Sample-Size Determination. In Statistical Methods in Medical Research; Armitage, P., Berry, G., Matthews, J.N.S., Eds.; Blackwell Science: Malden, MA, USA, 2002; pp. 137–146. [Google Scholar]
- Batchelor, T.J.P.; Rasburn, N.J.; Abdelnour-Berchtold, E.; Brunelli, A.; Cerfolio, R.J.; Gonzalez, M.; Ljungqvist, O.; Petersen, R.H.; Popescu, W.M.; Slinger, P.D.; et al. Guidelines for enhanced recovery after lung surgery: Recommendations of the Enhanced Recovery After Surgery (ERAS®) Society and the European Society of Thoracic Surgeons (ESTS). Eur. J. Cardiothorac. Surg. 2019, 55, 91–115. [Google Scholar] [CrossRef]
- Yildizeli, B.; Ozyurtkan, M.O.; Batirel, H.F.; Kuşcu, K.; Bekiroğlu, N.; Yüksel, M. Factors associated with postoperative delirium after thoracic surgery. Ann. Thorac. Surg. 2005, 79, 1004–1009. [Google Scholar] [CrossRef]
- Hayashi, K.; Motoishi, M.; Sawai, S.; Horimoto, K.; Hanaoka, J. Postoperative delirium after lung resection for primary lung cancer: Risk factors, risk scoring system, and prognosis. PLoS ONE 2019, 14, e0223917. [Google Scholar] [CrossRef]
- Shi, Z.; Mei, X.; Li, C.; Chen, Y.; Zheng, H.; Wu, Y.; Zheng, H.; Liu, L.; Marcantonio, E.R.; Xie, Z.; et al. Postoperative delirium is associated with long-term decline in activities of daily living. Anesthesiology 2019, 131, 492–500. [Google Scholar] [CrossRef] [Green Version]
- Goldberg, T.E.; Chen, C.; Wang, Y.; Jung, E.; Swanson, A.; Ing, C.; Garcia, P.S.; Whittington, R.A.; Moitra, V. Association of delirium with long-term cognitive decline: A meta-analysis. JAMA Neurol. 2020, 77, 1373–1381. [Google Scholar] [CrossRef]
- Fritz, B.A.; King, C.R.; Ben Abdallah, A.; Lin, N.; Mickle, A.M.; Budelier, T.P.; Oberhaus, J.; Park, D.; Maybrier, H.R.; Wildes, T.S.; et al. ENGAGES Research Group. Preoperative cognitive abnormality, intraoperative electroencephalogram suppression, and postoperative delirium: A mediation analysis. Anesthesiology 2020, 132, 1458–1468. [Google Scholar] [CrossRef]
- Sieber, F.E.; Zakriya, K.J.; Gottschalk, A.; Blute, M.R.; Lee, H.B.; Rosenberg, P.B.; Mears, S.C. Sedation depth during spinal anesthesia and the development of postoperative delirium in elderly patients undergoing hip fracture repair. Mayo Clin. Proc. 2010, 85, 18–26. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weinstein, S.M.; Poultsides, L.; Baaklini, L.R.; Mörwald, E.E.; Cozowicz, C.; Saleh, J.N.; Arrington, M.B.; Poeran, J.; Zubizarreta, N.; Memtsoudis, S.G. Postoperative delirium in total knee and hip arthroplasty patients: A study of perioperative modifiable risk factors. Br. J. Anaesth. 2018, 120, 999–1008. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Evered, L.A.; Chan, M.T.V.; Han, R.; Chu, M.H.M.; Cheng, B.P.; Scott, D.A.; Pryor, K.O.; Sessler, D.I.; Veselis, R.; Frampton, C.; et al. Anaesthetic depth and delirium after major surgery: A randomised clinical trial. Br. J. Anaesth. 2021, 127, 704–712. [Google Scholar] [CrossRef] [PubMed]
- Wildes, T.S.; Mickle, A.M.; Ben Abdallah, A.; Maybrier, H.R.; Oberhaus, J.; Budelier, T.P.; Kronzer, A.; McKinnon, S.L.; Park, D.; Torres, B.A.; et al. ENGAGES Research Group. Effect of electroencephalography-guided anesthetic administration on postoperative delirium among older adults undergoing major surgery: The ENGAGES randomized clinical trial. JAMA 2019, 321, 473–483. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tang, C.J.; Jin, Z.; Sands, L.P.; Pleasants, D.; Tabatabai, S.; Hong, Y.; Leung, J.M. ADAPT-2: A randomized clinical trial to reduce intraoperative EEG suppression in older surgical patients undergoing major noncardiac surgery. Anesth. Analg. 2020, 131, 1228–1236. [Google Scholar] [CrossRef] [PubMed]
- Duning, T.; Ilting-Reuke, K.; Beckhuis, M.; Oswald, D. Postoperative delirium: Treatment and prevention. Curr. Opin. Anaesthesiol. 2021, 34, 27–32. [Google Scholar] [CrossRef]


{kind=link}
| Entropy Guidance n = 39 | Clinical Signs n = 37 | p | |||
|---|---|---|---|---|---|
| Age, year | 59.8 | 15.7 | 60.2 | 15.6 | 0.9122 |
| Sex, male | 18 | 46.2 | 19 | 51.4 | 0.6505 |
| Body mass index, kg·m−2 | 23.9 | 22.4–26.2 (16.6–35.6) | 23.0 | 21.3–25.2 (17.6–39.2) | 0.2797 |
| ASA physical status | >0.9999 | ||||
| I | 3 | 7.7 | 3 | 7.7 | |
| II | 36 | 92.3 | 34 | 91.9 | |
| Current cigarette smoking | 11 | 28.2 | 10 | 27.0 | 0.9086 |
| Current alcohol drinking | 4 | 10.3 | 2 | 5.4 | 0.6752 |
| Lung malignancy | 14 | 35.9 | 12 | 32.4 | 0.7503 |
| Coexisting disease | |||||
| Hypertension | 9 | 23.1 | 16 | 43.2 | 0.0614 |
| Diabetes mellitus | 5 | 12.8 | 4 | 10.8 | >0.9999 |
| Ischemic heart disease | 3 | 7.7 | 5 | 13.5 | 0.4747 |
| COPD | 0 | 0 | 4 | 10.8 | 0.0515 |
| Chronic kidney disease | 1 | 2.6 | 1 | 2.7 | >0.9999 |
| Liver disease | 4 | 10.3 | 1 | 2.7 | 0.3589 |
| Carotid arterial disease | 0 | 0 | 1 | 2.7 | 0.4868 |
| Pulmonary function test | |||||
| FVC, % predicted | 88.0 | 78.2–103.9 (56.3–127.3) | 81.3 | 76.8–93.0 (54.2–158.4) | 0.3501 |
| FEV1, % predicted | 87.5 | 73.5–95.9 (49.0–131.1) | 84.5 | 71.6–93.7 (40.3–162.3) | 0.6979 |
| Left ventricular ejection fraction, % | 67 | 7 | 70 | 8 | 0.1341 |
| Preoperative blood test | |||||
| Hemoglobin, g·dL−1 | 13.9 | 13.0–14.5 (9.0–15.8) | 13.1 | 11.7–14.4 (10.6–17.2) | 0.0553 |
| Creatinine, mg·dL−1 | 0.80 | 0.64–0.94 (0.36–1.35) | 0.86 | 0.79–1.08 (0.51–1.80) | 0.0762 |
| eGFR, mL·min·1.73 m−2 | 90.1 | 77.0–108.8 (53.2–198.9) | 80.0 | 65.8–103.0 (37.0–130.7) | 0.1515 |
| Urea nitrogen, mg·dL−1 | 14 | 12–18 (6–27) | 15 | 13–19 (9–23) | 0.4323 |
| Sodium, mmol·L−1 | 139 | 138–141 (135–143) | 139 | 138–140 (129–145) | 0.3705 |
| Potassium, mmol·L−1 | 3.8 | 3.6–4.0 (3.1–4.4) | 3.8 | 3.6–4.1 (2.8–4.9) | 0.7575 |
| Alanine aminotransferase, U·L−1 | 22 | 17–28 (12–53) | 22 | 17–27 (11–59) | 0.9202 |
| Aspartate aminotransferase, U·L−1 | 22 | 20–24 (11–80) | 21 | 18–27 (11–95) | 0.9349 |
| Entropy Guidance n = 39 | Clinical Signs n = 37 | p | |||
|---|---|---|---|---|---|
| Surgical procedures | 0.9642 | ||||
| Wedge resection | 22 | 56.4 | 22 | 59.5 | |
| Segmentectomy | 9 | 23.1 | 8 | 21.6 | |
| Lobectomy | 8 | 20.5 | 7 | 18.9 | |
| RE value before induction | 98 | 95–99 (71–100) | 97 | 96–98 (90–100) | 0.8004 |
| SE value before induction | 87 | 86–89 (70–91) | 88 | 86–89 (79–91) | 0.5127 |
| Intravenous anesthetics | |||||
| Fentanyl, μg | 150 | 125–175 (50–250) | 125 | 100–150 (50–200) | 0.0320 |
| Propofol, mg | 120 | 110–150 (70–200) | 105 | 100–140 (60–300) | 0.1327 |
| Rocuronium, mg | 90 | 60–110 (40–140) | 80 | 70–100 (40–140) | 0.7226 |
| Sugammadex, mg | 130 | 120–160 (100–200) | 130 | 120–150 (90–200) | 0.7810 |
| Amount of crystalloid fluids, mL | 700 | 500–900 (350–1500) | 800 | 600–1000 (400–1400) | 0.1754 |
| Amount of colloid fluids, mL | 0 | 0–0 (0–500) | 0 | 0–0 (0–500) | 0.2584 |
| Surgical blood loss, mL | 10 | 10–50 (10–350) | 10 | 10–100 (10–500) | 0.1641 |
| Duration of anesthesia, min | 190 | 135–285 (75–400) | 210 | 145–247 (80–505) | 0.9917 |
| Entropy Guidance n = 39 | Clinical Signs n = 37 | p | |||
|---|---|---|---|---|---|
| Average level of end-tidal sevoflurane, % | 1.49 | 1.19–1.72 (0.72–2.08) | 1.58 | 1.45–1.68 (1.10–2.06) | 0.2660 |
| Average level of end-tidal sevoflurane, aaMAC | 0.78 | 0.61–0.92 (0.43–1.17) | 0.86 | 0.73–0.95 (0.58–1.19) | 0.1499 |
| Time percentage of RE > 60, % | 14.5 | 6.7–30.0 (2.7–73.1) | 11.3 | 5.8–23.1 (1.8–75.0) | 0.3496 |
| Time percentage of RE 40–60, % | 77.8 | 65.5–88.2 (26.9–96.1) | 71.1 | 29.1–76.9 (0–90.9) | 0.0056 |
| Time percentage of RE < 40, % | 1.9 | 0–6.0 (0–29.2) | 10.0 | 3.6–40.6 (0–97.4) | 0.0002 |
| Average RE value | 55 | 51–59 (44–69) | 51 | 44–57 (26–68) | 0.0117 |
| Time percentage of SE > 60, % | 13.8 | 4.7–18.5 (0–65.4) | 9.4 | 4.3–14.3 (0–66.7) | 0.2142 |
| Time percentage of SE 40–60, % | 81.5 | 72.3–90.0 (34.6–96.1) | 71.8 | 35.4–82.2 (0–90.9) | 0.0020 |
| Time percentage of SE < 40, % | 2.3 | 0–7.5 (0–46.2) | 13.2 | 4.2–46.9 (0–97.4) | 0.0001 |
| Average SE value | 52 | 49–57 (41–65) | 49 | 42–54 (26–65) | 0.0093 |
| Entropy Guidance n = 39 | Clinical Signs n = 37 | p | |||
|---|---|---|---|---|---|
| Time to spontaneous eye opening, s | 427 | 270–530 (56–830) | 505 | 395–736 (209–1226) | 0.0155 |
| Time to obeying commands, s | 506 | 388–644 (95–1201) | 550 | 445–823 (215–1310) | 0.1006 |
| Time to tracheal extubation, s | 565 | 420–840 (135–7116) | 595 | 504–863 (256–11,927) | 0.1685 |
| Time to leaving operating room, s | 885 | 804–1103 (450–1744) | 1030 | 882–1200 (575–1590) | 0.1178 |
| Emergence agitation | 3 | 7.7 | 9 | 24.3 | 0.0469 |
| Drowsiness during tracheal extubation | 2 | 5.1 | 6 | 16.2 | 0.1481 |
| Postoperative delirium | 1 | 2.6 | 10 | 27.0 | 0.0024 |
| Intraoperative awareness or recall | 0 | 0 | 0 | 0 | NA |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, J.-T.; Wu, Y.-M.; Tiong, T.-Y.; Cata, J.P.; Kuo, K.-T.; Li, C.-C.; Liu, H.-Y.; Cherng, Y.-G.; Wu, H.-L.; Tai, Y.-H. Spectral Entropy Monitoring Accelerates the Emergence from Sevoflurane Anesthesia in Thoracic Surgery: A Randomized Controlled Trial. J. Clin. Med. 2022, 11, 1631. https://doi.org/10.3390/jcm11061631
Chen J-T, Wu Y-M, Tiong T-Y, Cata JP, Kuo K-T, Li C-C, Liu H-Y, Cherng Y-G, Wu H-L, Tai Y-H. Spectral Entropy Monitoring Accelerates the Emergence from Sevoflurane Anesthesia in Thoracic Surgery: A Randomized Controlled Trial. Journal of Clinical Medicine. 2022; 11(6):1631. https://doi.org/10.3390/jcm11061631
Chicago/Turabian StyleChen, Jui-Tai, Yu-Ming Wu, Tung-Yu Tiong, Juan P. Cata, Kuang-Tai Kuo, Chun-Cheng Li, Hsin-Yi Liu, Yih-Giun Cherng, Hsiang-Ling Wu, and Ying-Hsuan Tai. 2022. "Spectral Entropy Monitoring Accelerates the Emergence from Sevoflurane Anesthesia in Thoracic Surgery: A Randomized Controlled Trial" Journal of Clinical Medicine 11, no. 6: 1631. https://doi.org/10.3390/jcm11061631
APA StyleChen, J.-T., Wu, Y.-M., Tiong, T.-Y., Cata, J. P., Kuo, K.-T., Li, C.-C., Liu, H.-Y., Cherng, Y.-G., Wu, H.-L., & Tai, Y.-H. (2022). Spectral Entropy Monitoring Accelerates the Emergence from Sevoflurane Anesthesia in Thoracic Surgery: A Randomized Controlled Trial. Journal of Clinical Medicine, 11(6), 1631. https://doi.org/10.3390/jcm11061631