
Preoperative Serum Alkaline Phosphatase and Neurological Outcome of Cerebrovascular Surgery

 , ,
, ,
Abstract
:1. Introduction
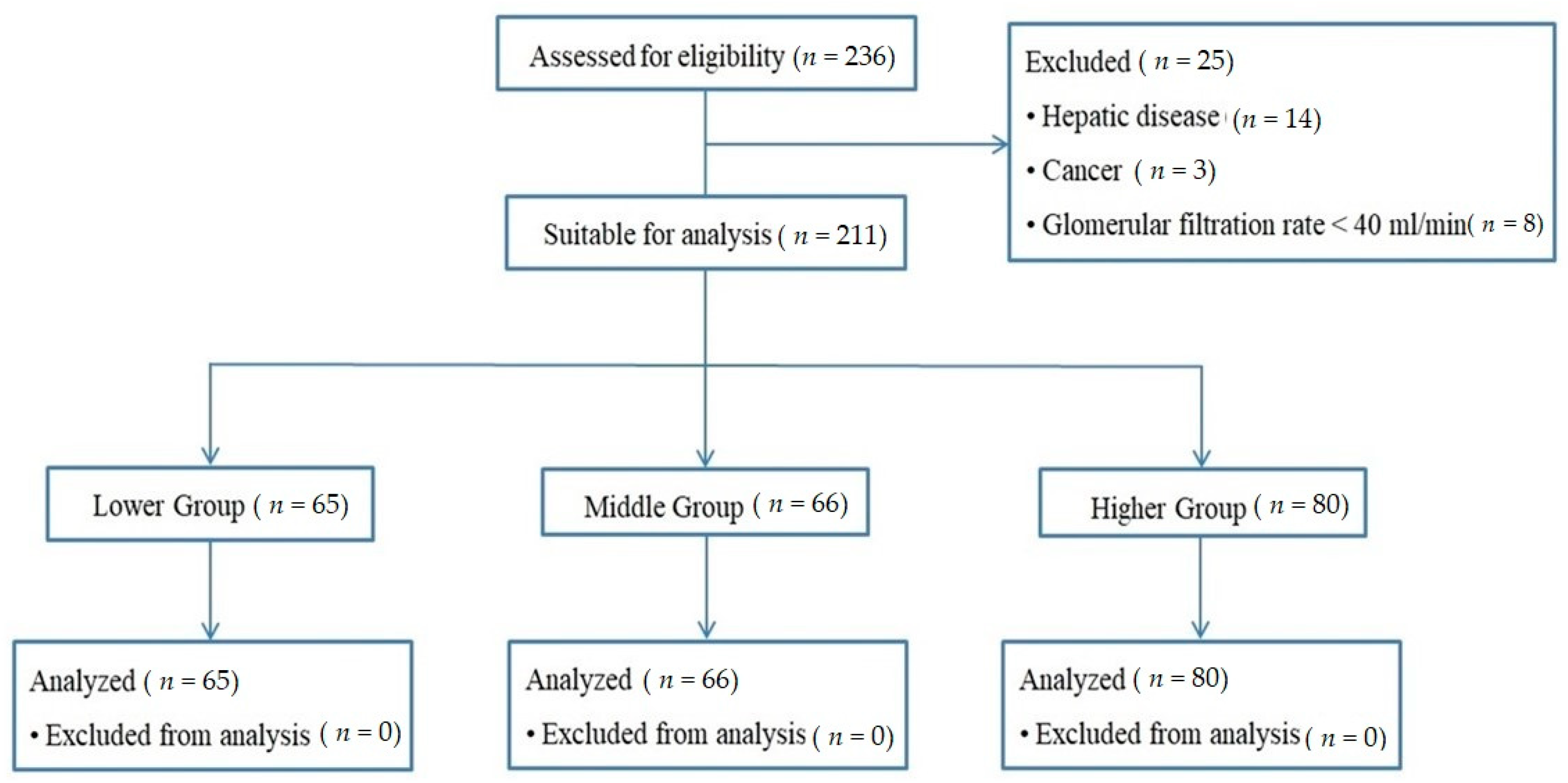
2. Materials and Methods
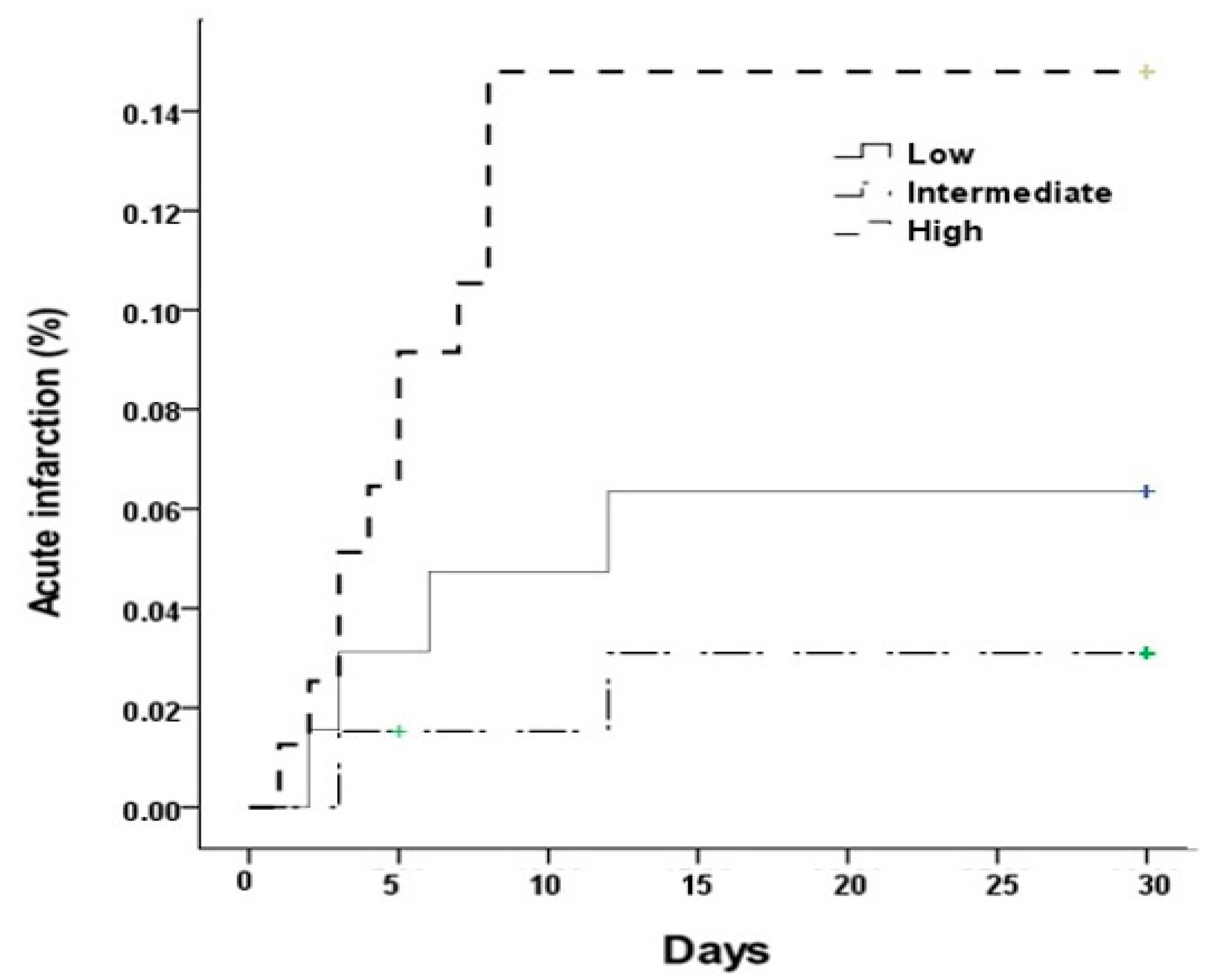
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Yoon, S.; Burkhardt, J.K.; Lawton, M.T. Long-term patency in cerebral revascularization surgery: An analysis of a consecutive series of 430 bypasses. J. Neurosurg. 2019, 131, 80–87. [Google Scholar] [CrossRef] [Green Version]
- Chen, X.; Lin, C.L.; Su, Y.C.; Chen, K.F.; Lai, S.W.; Wei, S.T.; Peng, C.T.; Chiu, C.D.; Shieh, S.H.; Chen, C.C. Risk of subsequent stroke, with or without extracranial-intracranial bypass surgery: A nationwide, retrospective, population-based study. J. Neurosurg. 2018, 130, 1906–1913. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schoppet, M.; Shanahan, C. Role for alkaline phosphatase as an inducer of vascular calcification in renal failure? Kidney Int. 2008, 73, 989–991. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abramowitz, M.; Muntner, P.; Coco, M.; William Southern, W.; Lotwin, I.; Hostetter, T.H.; Melamed, M.L. Serum alkaline phosphatase and phosphate and risk of mortality and hospitalization. Clin. J. Am. Soc. Nephrol. 2010, 5, 1064–1071. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beige, J.; Wendt, R.; Girndt, M.; Queck, K.-H.; Fiedler, R.; Jehle, P. Association of serum alkaline phosphatase with mortality in non-selected European patients with CKD5D: An observational, three-centre survival analysis. BMJ Open 2014, 4, e004275. [Google Scholar] [CrossRef] [Green Version]
- Stuto, S.; Chattopadhyay, J.; Avram, M.M. Relationship between alkaline phosphatase and all-cause mortality in peritoneal dialysis patients. Adv. Perit. Dial. 2013, 29, 61–63. [Google Scholar]
- Shimizu, Y.; Nakazato, M.; Sekita, T.; Kadota, K.; Yamasaki, H.; Takamura, N.; Aoyagi, K.; Kusano, Y.; Maeda, T. Association between alkaline phosphatase and hypertension in a rural Japanese population: The Nagasaki Islands study. J. Physiol. Anthropol. 2013, 32, 10. [Google Scholar] [CrossRef] [Green Version]
- Krishnamurthy, V.R.; Baird, B.C.; Wei, G.; Greene, T.; Raphael, K.; Beddhu, S. Associations of serum alkaline phosphatase with metabolic syndrome and mortality. Am. J. Med. 2011, 124, 566.e1–566.e7. [Google Scholar] [CrossRef] [Green Version]
- Oh, P.C.; Lee, K.; Kim, T.H.; Moon, J.G.; Park, H.W.; Jang, H.J.; Park, S.D.; Kwon, S.W.; Suh, J.; Kang, W.C. Prognostic impact of alkaline phosphatase measured at time of presentation in patients undergoing primary percutaneous coronary intervention for ST-segment elevation myocardial infarction. PLoS ONE 2017, 12, e0171914. [Google Scholar]
- Wannamethee, S.G.; Sattar, N.; Papcosta, O.; Lennon, L.; Whincup, P.H. Alkaline phosphatase, serum phosphate, and incident cardiovascular disease and total mortality in older men. Arterioscler. Thromb. Vasc. Biol. 2013, 33, 1070–1076. [Google Scholar] [CrossRef] [Green Version]
- Tonelli, M.; Curhan, G.; Pfeffer, M.; Sacks, F.; Thadhani, R.; Melamed, M.L.; Wiebe, N.; Muntner, P. Relation Between Alkaline Phosphatase, Serum Phosphate, and All-Cause or Cardiovascular Mortality. Circulation 2009, 120, 1784–1792. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ryu, W.S.; Lee, S.H.; Kim, C.; Kim, B.J.; Yoon, B.W. Increased serum alkaline phosphatase as a predictor of long-term mortality after stroke. Neurology 2010, 75, 1995–2002. [Google Scholar] [CrossRef] [PubMed]
- Shimizu, Y.; Imano, H.; Ohira, T.; Kitamura, A.; Kiyama, M.; Okada, T.; Ishikawa, Y.; Takashi Shimamoto, T.; Yamagishi, K.; Tanigawa, T.; et al. CIRCS Investigators. Alkaline phosphatase and risk of stroke among Japanese: The Circulatory Risk in Communities Study (CIRCS). J. Stroke Cerebrovasc. Dis. 2013, 22, 1046–1055. [Google Scholar] [CrossRef] [PubMed]
- Uehara, T.; Ohara, T.; Minematsu, K.; Nagatsuka, K.; Toyoda, K. Predictors of stroke events in patients with transient ischemic attack attributable to intracranial stenotic lesions. Intern. Med. 2018, 57, 295–300. [Google Scholar] [CrossRef] [Green Version]
- Pratibha, S.; Praveen-Kumar, S.; Agadi, J. Increased serum alkaline phosphatase and serum phosphate as predictors of mortality after stroke. J. Clin. Diag. Res. 2014, 8, CC01–CC03. [Google Scholar]
- Zhong, C.; You, S.; Chen, J.; Zhai, G.; Du, H.; Luo, Y.; Dong, X.; Cao, Y.; Liu, C.F.; Zhang, Y. Serum alkaline phosphatase, phosphate, and in-‘hospital mortality in acute ischemic stroke patients. J. Stroke Cerebrovasc. Dis. 2018, 27, 257–266. [Google Scholar] [CrossRef]
- Liu, J.; Wang, D.; Li, J.; Xiong, Y.; Liu, B.; Wei, C.; Wu, S.; Liu, M. High serum alkaline phosphatase levels in relation to multi-cerebral microbleeds in acute ischemic stroke patients with atrial fibrillation and/or rheumatic heart disease. Curr. Neurovasc. Res. 2016, 13, 303–308. [Google Scholar] [CrossRef]
- Liu, J.; Wang, D.; Li, J.; Xiong, Y.; Liu, B.; Wei, C.; Wu, S.; Lin, J.; Liu, M. Increased serum alkaline phosphatase as a predictor of symptomatic hemorrhagic transformation in ischemic stroke patients with atrial fibrillation and/or rheumatic heart disease. J. Stroke Cerebrovasc. Dis. 2016, 25, 2448–2452. [Google Scholar] [CrossRef]
- Harmey, D.; Hessle, L.; Narisawa, S.; Johnson, K.A.; Terkeltaub, R.; Millán, J.L. Concerted regulation of inorganic pyrophosphate and osteopontin by akp2, enpp1, and ank: An integrated model of the pathogenesis of mineralization disorders. Am. J. Pathol. 2004, 164, 1199–1209. [Google Scholar] [CrossRef]
- Cheung, B.M.; Ong, K.L.; Wong, L.Y. Elevated serum alkaline phosphatase and peripheral arterial disease in the United States National Health and Nutrition Examination Survey 1999–2004. Int. J. Cardiol. 2009, 135, 156–161. [Google Scholar] [CrossRef]
- Schutte, R.; Huisman, H.; Malan, L.; van Rooyen, J.M.; Smith, W.; Glyn, M.C.P.; Mels, C.M.C.; Fourie, C.M.T.; Malan, N.T.; Schutte, A.E. Alkaline phosphatase and arterial structure and function in hypertensive African men: The SABPA study. Int. J. Cardiol. 2013, 167, 1995–2001. [Google Scholar] [CrossRef] [PubMed]
- Lomashvili, K.; Garg, P.; Narisawa, S.; Millan, J.; O’Neill, W. Upregulation of alkaline phosphatase and pyrophosphate hydrolysis: Potential mechanism for uremic vascular calcification. Kidney Int. 2008, 73, 1024–1030. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haarhaus, M.; Brandenburg, V.; Kalantar-Zadeh, K.; Stenvinkel, P.; Magnusson, P. Alkaline phosphatase: A novel treatment target for cardiovascular disease in CKD. Nat. Rev. Nephrol. 2017, 3, 429–442. [Google Scholar] [CrossRef] [PubMed]
- Kats, S.; Brands, R.; Seinen, W.; de Jager, W.; Bekker Margreet, W.A.; Soliman Hamad, M.A.; SH Tan, M.E.; Schönberger, J.P. Anti-inflammatory effects of alkaline phosphatase in coronary artery bypass surgery with cardiopulmonary bypass. Recent Pat. Inflamm. Allergy Drug Discov. 2009, 3, 214–220. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kats, S.; Schönberger, J.P.; Brands, R.; Seinen, W.; van Oeveren, W. Endotoxin release in cardiac surgery with cardiopulmonary bypass: Pathophysiology and possible therapeutic strategies. An update. Eur. J. Cardiothorac. Surg. 2011, 39, 451–458. [Google Scholar] [CrossRef] [Green Version]
- Verweij, W.R.; Bentala, H.; van der Vlag, A.H.; van Loenen-Weemaes, A.M.; Kooi, K.; Meijer, D.K.F.; Poelstra, K. Protection against an Escherichia coli-induced sepsis by alkaline phosphatase in mice. Shock 2004, 22, 174–179. [Google Scholar] [CrossRef]
- Maldonado, O.; Demasi, R.; Maldonado, Y.; Taylor, M.; Troncale, F.; Vender, R. Extremely high levels of alkaline phosphatase in hospitalized patients. J. Clin. Gastroenterol. 1998, 27, 342–345. [Google Scholar] [CrossRef]
- Webber, M.; Krishnan, A.; Thomas, N.G.; Cheung, B.M. Association between serum alkaline phosphatase and C-reactive protein in the United States National Health and Nutrition Examination Survey 2005–2006. Clin. Chem. Lab. Med. 2010, 48, 167–173. [Google Scholar] [CrossRef]
- Dziedzic, T. Changes of Bone Formation Markers Osteocalcin and Bone-Specific Alkaline Phosphatase in Postmenopausal Women with Osteoporosis. Expert Rev. Neurother. 2015, 15, 523–531. [Google Scholar] [CrossRef]
- Lumachi, F.; Ermani, M.; Camozzi, V.; Tombolan, V.; Luisetto, G. Changes of Bone Formation Markers Osteocalcin and Bone-Specific Alkaline Phosphatase in Postmenopausal Women with Osteoporosis. Ann. N. Y. Acad. Sci. 2009, 1173, E60–E63. [Google Scholar] [CrossRef]
- Takakura, N.; Watanabe, T.; Suenobu, S.; Yamada, Y.; Noda, T.; Ito, Y.; Satake, M.; Suda, T. A role for hematopoietic stem cells in promoting angiogenesis. Cell 2000, 102, 199–209. [Google Scholar] [CrossRef] [Green Version]
- Yamada, Y.; Takakura, N. Physiological pathway of differentiation of hematopoietic stem cell population into mural cells. J. Exp. Med. 2006, 203, 1055–1065. [Google Scholar] [CrossRef] [PubMed]
- Shi, Q.; Rafii, S.; Wu, M.H.D.; Wijelath, E.S.; Yu, C.; Ishida, A.; Fujita, Y.; Kothari, S.; Mohle, R.; Sauvage, L.R.; et al. Evidence for circulating bone marrow-derived endothelial cells. Blood 1998, 92, 362–367. [Google Scholar] [CrossRef] [PubMed]
- Sata, M.; Saiura, A.; Kunisato, A.; Tojo, A.; Okada, S.; Tokuhisa, T.; Hirai, H.; Makuuchi, M.; Hirata, Y.; Nagai, R. Hematopoietic stem cells differentiate into vascular cells that participate in the pathogenesis of atherosclerosis. Nat. Med. 2002, 8, 403–409. [Google Scholar] [CrossRef]
- Lomashvili, K.; Garg, P.; O’Neill, W. Chemical and hormonal determinants of vascular calcification in vitro. Kidney Int. 2006, 69, 1464–1470. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chang, J.F.; Feng, Y.F.; Peng, Y.S.; Hsu, S.P.; Pai, M.F.; Chen, H.Y.; Wu, H.Y.; Yang, J.Y. Combined alkaline phosphatase and phosphorus levels as a predictor of mortality in maintenance hemodialysis patients. Medicine 2014, 93, e106. [Google Scholar] [CrossRef]
- Larsson, T.E.; Olauson, H.; Hagström, E.; Ingelsson, E.; Arnlöv, J.; Lind, L.; Sundström, J. Conjoint effects of serum calcium and phosphate on risk of total, cardiovascular, and noncardiovascular mortality in the community. Arterioscler. Thromb. Vasc. Biol. 2010, 30, 333–339. [Google Scholar] [CrossRef]
- Foley, R.N.; Collins, A.J.; Ishani, A.; Kalra, P.A. Calcium-phosphate levels and cardiovascular disease in community-dwelling adults: The Atherosclerosis Risk in Communities (ARIC) Study. Am. Heart J. 2008, 156, 556–563. [Google Scholar] [CrossRef]
- Park, W.; Kim, B.S.; Lee, J.E.; Huh, J.K.; Kim, B.J.; Sung, K.C.; Kang, J.H.; Lee, M.H.; Park, J.R.; Eun Jung Rhee, E.J.; et al. Serum phosphate levels and the risk of cardiovascular disease and metabolic syndrome: A double-edged sword. Diabetes Res. Clin. Pract. 2009, 83, 119–125. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Lower Group (n = 70) | Middle Group (n = 70) | Higher Group (n = 71) | p Value | |
|---|---|---|---|---|
| Demographic data | ||||
| Age (year) | 61.8 ± 11.3 | 64.2 ± 11.4 | 64.6 ± 11.7 | 0.285 |
| Body-mass index | 24.0 ± 3.4 | 24.2 ± 2.6 | 24.4 ± 3.6 | 0.783 |
| Male | 47 (72.3%) | 46 (69.7%) | 58 (72.5%) | 0.073 |
| Past history | ||||
| Smoking | 29 (44.6%) | 23 (34.8%) | 36 (45.0%) | 0.371 |
| Diabetes mellitus | 25 (38.5%) | 28 (42.4%) | 22 (27.5%) | 0.162 |
| Hypertension | 44 (67.7%) | 45 (68.2%) | 50 (62.5%) | 0.787 |
| Stroke | 25 (38.5%) | 25 (37.9%) | 35 (43.8%) | 0.723 |
| Myocardial infarction | 7 (10.8%) | 6 (9.1%) | 10 (12.5%) | 0.805 |
| Laboratory variables | ||||
| CRP (mg/L) | 0.1 ± 0.2 | 0.3 ± 1.3 | 0.5 ± 1.9 | 0.114 |
| Hemoglobin (g/dL) | 13.5 ± 1.5 | 14.4 ± 7.4 | 13.6 ± 1.6 | 0.438 |
| Cholesterol (mg/dL) | 150.3 ± 44.5 | 158.9 ± 44.9 | 158.3 ± 40.1 | 0.427 |
| Calcium (mg/dL) | 8.7 ± 0.8 | 8.9 ± 0.5 | 8.8 ± 0.7 | 0.475 |
| Phosphorus (mg/dL) | 44.7 ± 17.3 | 60.6 ± 23.9 | 89.2 ± 45.0 | <0.001 |
| Creatinine | 0.9 ± 0.3 | 1.0 ± 0.3 | 0.9 ± 0.3 | 0.273 |
| Albumin (g/dL) | 4.0 ± 0.6 | 4.2 ± 0.5 | 4.1 ± 0.4 | 0.238 |
| Bilirubin (mg/dL) | 0.7 ± 0.2 | 0.7 ± 0.3 | 0.6 ± 0.3 | 0.651 |
| AST (IU/dL) | 24.8 ± 19.1 | 25.5 ± 23.6 | 28.1 ± 14.7 | 0.583 |
| ALT (IU/dL) | 26.7 ± 22.8 | 30.8 ± 33.0 | 35.0 ± 25.0 | 0.193 |
| ALP (IU/dL) | 49.4 ± 10.6 | 70.2 ± 4.8 | 102.7 ± 30.1 | <0.001 |
| Lower Group (n = 70) | Middle Group (n = 70) | Higher Group (n = 71) | p Value | |
|---|---|---|---|---|
| Acute infarction | 4 (5.7%) | 2 (2.9%) | 12 (16.9%) | 0.007 |
| No Infarction (n = 193) | Infarction (n = 18) | p Value | |
|---|---|---|---|
| Demographic data | |||
| Age (year) | 63.7 ± 11.4 | 61.8 ± 12.5 | 0.497 |
| Body-mass index | 24.2 ± 3.3 | 24.1 ± 2.3 | 0.836 |
| Male | 136 (70%) | 15(83%) | 0.290 |
| Past history | |||
| Smoking | 80 (41%) | 8 (44%) | 0.799 |
| Diabetes mellitus | 71 (37%) | 4 (22%) | 0.307 |
| Hypertension | 129 (67%) | 10 (56%) | 0.503 |
| Stroke | 48 (25%) | 3 (17%) | 0.575 |
| Myocardial infarction | 21 (11%) | 2 (11%) | 1.000 |
| Laboratory variables | |||
| CRP (mg/L) | 0.3 ± 1.4 | 0.3 ± 0.7 | 0.960 |
| Hemoglobin (g/dL) | 13.9 ± 4.6 | 13.5 ± 2.0 | 0.689 |
| Cholesterol (mg/dL) | 156.7 ± 43.1 | 147.2 ± 44.4 | 0.374 |
| Calcium (mg/dL) | 8.8 ± 0.7 | 8.8 ± 4.8 | 0.969 |
| Phosphorus (mg/dL) | 64.1 ± 34.2 | 73.8 ± 53.3 | 0.280 |
| Creatinine | 0.9 ± 0.3 | 0.9 ± 0.2 | 0.775 |
| Albumin (g/dL) | 4.1 ± 0.5 | 4.2 ± 0.4 | 0.615 |
| Bilirubin (mg/dL) | 0.7 ± 0.3 | 0.7 ± 0.3 | 0.757 |
| AST (IU/dL) | 26.4 ± 20.1 | 23.1 ± 9.5 | 0.488 |
| ALT (IU/dL) | 30.8 ± 27.5 | 31.7 ± 27.3 | 0.897 |
| AST/ALT ratio | 1.0 ± 0.5 | 1.0 ± 0.7 | 0.972 |
| ALP (IU/dL) | 72.5 ± 27.9 | 92.5 ± 33.3 | 0.005 |
| OR (95% CI) | p Value | |
|---|---|---|
| ALP third tertile | 3.356 (1.026–10.974) | 0.045 |
| Cholesterol | 0.995 (0.983–1.006) | 0.372 |
| AST/ALT ratio | 0.983 (0.377–2.560) | 0.971 |
| ALP third tertile | 3.356 (1.026–10.974) | 0.045 |
| Event Number | Hazard Ratio | 95% CI of Hazard Ratio | p Value | |
|---|---|---|---|---|
| Acute infarction | 18 | 1.013 | 1.004–1.022 | 0.007 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Park, S.; Choi, E.-S.; Jung, H.-W.; Lee, J.-Y.; Park, J.-W.; Bang, J.-S.; Jeon, Y.-T. Preoperative Serum Alkaline Phosphatase and Neurological Outcome of Cerebrovascular Surgery. J. Clin. Med. 2022, 11, 2981. https://doi.org/10.3390/jcm11112981
Park S, Choi E-S, Jung H-W, Lee J-Y, Park J-W, Bang J-S, Jeon Y-T. Preoperative Serum Alkaline Phosphatase and Neurological Outcome of Cerebrovascular Surgery. Journal of Clinical Medicine. 2022; 11(11):2981. https://doi.org/10.3390/jcm11112981
Chicago/Turabian StylePark, Seongjoo, Eun-Su Choi, Hee-Won Jung, Ji-Youn Lee, Jin-Woo Park, Jae-Seung Bang, and Yeong-Tae Jeon. 2022. "Preoperative Serum Alkaline Phosphatase and Neurological Outcome of Cerebrovascular Surgery" Journal of Clinical Medicine 11, no. 11: 2981. https://doi.org/10.3390/jcm11112981
APA StylePark, S., Choi, E.-S., Jung, H.-W., Lee, J.-Y., Park, J.-W., Bang, J.-S., & Jeon, Y.-T. (2022). Preoperative Serum Alkaline Phosphatase and Neurological Outcome of Cerebrovascular Surgery. Journal of Clinical Medicine, 11(11), 2981. https://doi.org/10.3390/jcm11112981