
Propofol-Based Anesthesia Maintenance and/or Volatile Anesthetics during Intracranial Aneurysm Repair: A Comparative Analysis of Neurological Outcomes
 , , , , ,
, , , , , 
Abstract
:1. Introduction
2. Materials and Methods
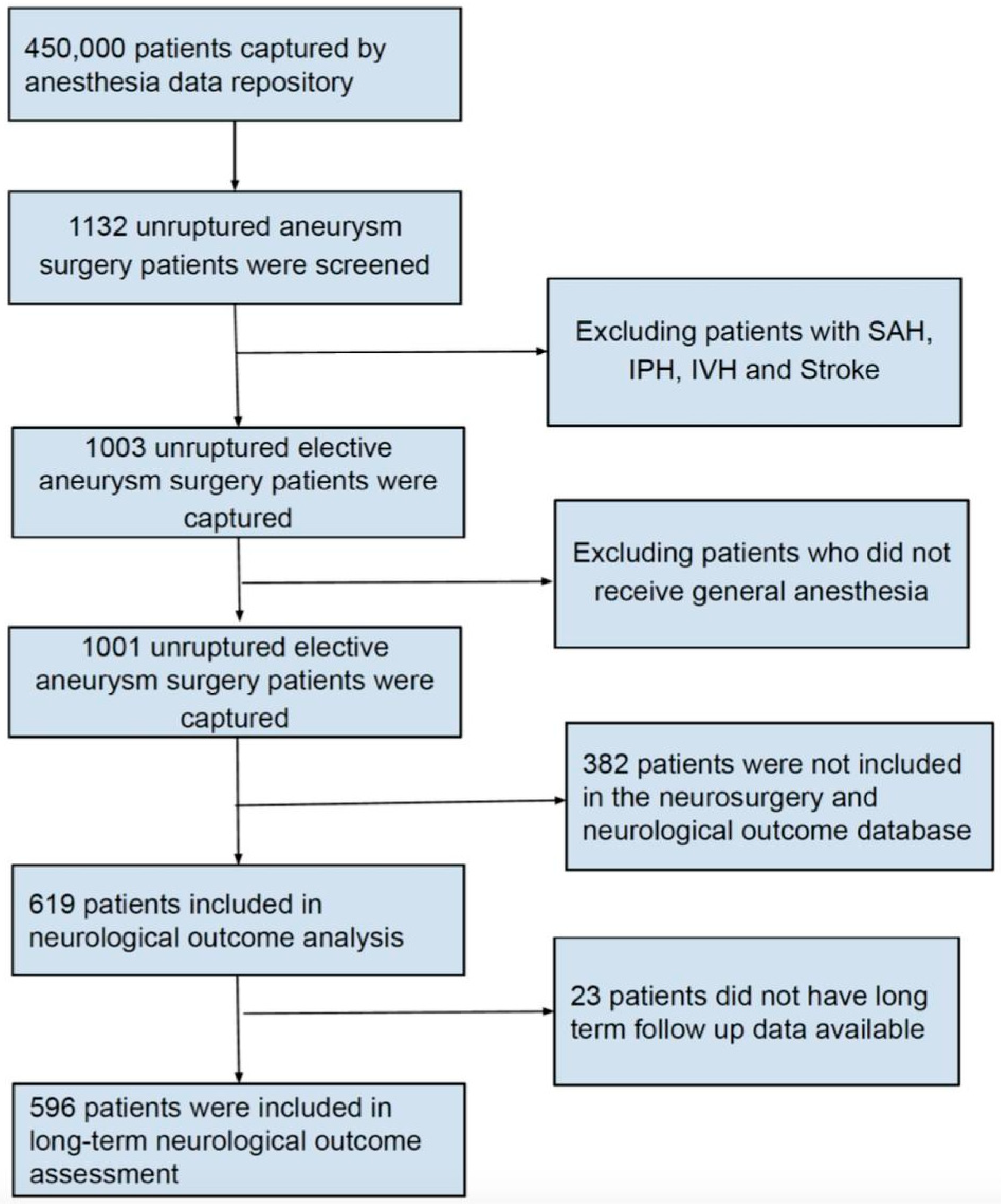
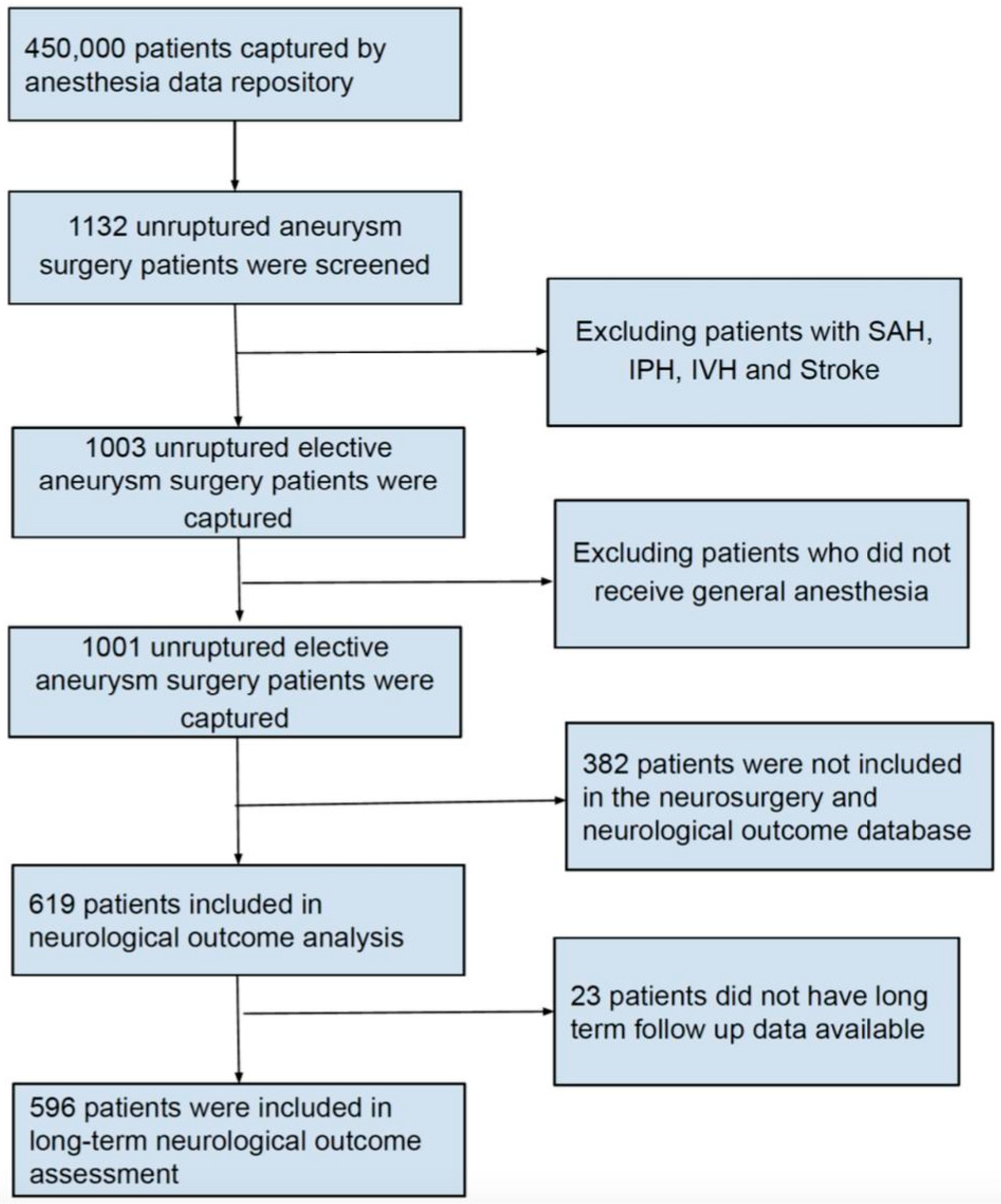
2.1. Study Population
2.2. Outcome Measures
2.3. Statistical Analysis
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviation List
| ASA | American Association of Anesthesiologists |
| BIDMC | Beth Israel Deaconess Medical Center |
| BMI | Body mass index |
| CI | Confidence interval |
| H-LOS | Hospital length of stay |
| ICU | Intensive care unit |
| ICU-LOS | Intensive care unit length of stay |
| IQR | Interquartile range |
| LOS | Length of stay |
| MAC | Minimum Alveolar Concentration |
| mRS | Modified Rankin Scale |
| OME | Oral Morphine Equivalents |
| OR | Odds ratio |
| SAH | Subarachnoid hemorrhage |
| TIVA | Total intravenous anesthesia |
| UIA | Unruptured intracranial aneurysm |
References
- Chalouhi, N.; Hoh, B.L.; Hasan, D. Review of cerebral aneurysm formation, growth, and rupture. Stroke 2013, 44, 3613–3622. [Google Scholar] [CrossRef]
- Benjamin, E.J.; Blaha, M.J.; Chiuve, S.E.; Cushman, M.; Das, S.R.; Deo, R.; De Ferranti, S.D.; Floyd, J.; Fornage, M.; Gillespie, C.; et al. Heart Disease and Stroke Statistics-2017 Update: A Report from the American Heart Association. Circulation 2017, 135, e146–e603. [Google Scholar] [CrossRef] [PubMed]
- Kochanek, K.D.; Murphy, S.L.; Xu, J.; Arias, E. Mortality in the United States, 2013. NCHS Data Brief. 2013, 178, 1–8. [Google Scholar]
- Go, A.S.; Mozaffarian, D.; Roger, V.L.; Benjamin, E.J.; Berry, J.D.; Borden, W.B.; Bravata, D.M.; Dai, S.; Ford, E.S.; Fox, C.S.; et al. Heart Disease and Stroke Statistics—2013 Update: A report from the American Heart Association. Circulation 2013, 127, e6–e245. [Google Scholar] [CrossRef] [PubMed]
- Kalani, M.Y.S.; Wanebo, J.E.; Martirosyan, N.L.; Nakaji, P.; Zabramski, J.M.; Spetzler, R.F. A raised bar for aneurysm surgery in the endovascular era. J. Neurosurg. 2017, 126, 1731–1739. [Google Scholar] [CrossRef] [PubMed]
- Ihn, Y.K.; Shin, S.H.; Baik, S.K.; Choi, I.S. Complications of endovascular treatment for intracranial aneurysms: Management and prevention. Interv. Neuroradiol. 2018, 24, 237–245. [Google Scholar] [CrossRef]
- Bruder, N.; Boussen, S.; Velly, L. Anesthesia for Aneurysmal Subarachnoid Hemorrhage. In Textbook of Neuroanesthesia and Neurocritical Care; Springer: Berlin/Heidelberg, Germany, 2019; pp. 115–130. [Google Scholar]
- Hunt, W.E.; Hess, R.M. Surgical Risk as Related to Time of Intervention in the Repair of Intracranial Aneurysms. J. Neurosurg. 1968, 28, 14–20. [Google Scholar] [CrossRef]
- Molyneux, A.J.; Kerr, R.S.; Yu, L.-M.; Clarke, M.; Sneade, M.; Yarnold, J.A.; Sandercock, P. International subarachnoid aneurysm trial (ISAT) of neurosurgical clipping versus endovascular coiling in 2143 patients with ruptured intracranial aneurysms: A randomised comparison of effects on survival, dependency, seizures, rebleeding, subgroups, and aneurysm occlusion. Lancet 2005, 366, 809–817. [Google Scholar] [CrossRef]
- Esmaeeli, S.; Valencia, J.; Buhl, L.K.; Bastos, A.B.; Goudarzi, S.; Eikermann, M.; Fehnel, C.; Pollard, R.; Thomas, A.; Ogilvy, C.S.; et al. Anesthetic management of unruptured intracranial aneurysms: A qualitative systematic review. Neurosurg. Rev. 2021, 44, 2477–2492. [Google Scholar] [CrossRef] [PubMed]
- Archer, D.P.; Walker, A.M.; McCann, S.K.; Moser, J.J.; Appireddy, R.M. Anesthetic Neuroprotection in Experimental Stroke in Rodents: A Systematic Review and Meta-analysis. Anesthesiology 2017, 126, 653–665. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Li, P.; Xu, N.; Zhu, L.; Cai, M.; Yu, W.; Gao, Y. Paradigms and mechanisms of inhalational anesthetics mediated neuroprotection against cerebral ischemic stroke. Med. Gas Res. 2016, 6, 194–205. [Google Scholar] [CrossRef] [PubMed]
- Adembri, C.; Venturi, L.; Pellegrini-Giampietro, D.E. Neuroprotective effects of propofol in acute cerebral injury. CNS Drug Rev. 2007, 13, 333–351. [Google Scholar] [CrossRef] [PubMed]
- Bayona, N.A.; Gelb, A.W.; Jiang, Z.; Wilson, J.X.; Urquhart, B.L.; Cechetto, D.F. Propofol neuroprotection in cerebral ischemia and its effects on low-molecular-weight antioxidants and skilled motor tasks. Anesthesiology 2004, 100, 1151–1159. [Google Scholar] [CrossRef]
- Raub, D.; Platzbecker, K.; Grabitz, S.D.; Xu, X.; Wongtangman, K.; Pham, S.B.; Murugappan, K.R.; Hanafy, K.A.; Nozari, A.; Houle, T.T.; et al. Effects of Volatile Anesthetics on Postoperative Ischemic Stroke Incidence. J. Am. Heart Assoc. 2021, 10, e018952. [Google Scholar] [CrossRef] [PubMed]
- Sivasankar, C.; Stiefel, M.; Miano, T.A.; Kositratna, G.; Yandrawatthana, S.; Hurst, R.; Kofke, W.A. Anesthetic variation and potential impact of anesthetics used during endovascular management of acute ischemic stroke. J. Neurointerv. Surg. 2016, 8, 1101–1106. [Google Scholar] [CrossRef] [PubMed]
- Lecours, M.; Gelb, A.W. Anesthesia for the surgical treatment of cerebral aneurysms. Colomb. J. Anesthesiol. 2015, 43, 45–51. [Google Scholar] [CrossRef]
- Chowdhury, T.; Petropolis, A.; Wilkinson, M.; Schaller, B.; Sandu, N.; Cappellani, R.B. Controversies in the anesthetic management of intraoperative rupture of intracranial aneurysm. Anesthesiol. Res. Pract. 2014, 2014, 595837. [Google Scholar] [CrossRef]
- Guo, D.; Li, Y.; Wang, H.; Wang, X.; Hua, W.; Tang, Q.; Miao, L.; Wang, G. Propofol post-conditioning after temporary clipping reverses oxidative stress in aneurysm surgery. Int. J. Neurosci. 2019, 129, 157–166. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing; R Core Team: Vienna, Austria, 2018. [Google Scholar]
- Wolf, A.; Selpien, H.; Haberl, H.; Unterberg, M. Does a combined intravenous-volatile anesthesia offer advantages compared to an intravenous or volatile anesthesia alone: A systematic review and meta-analysis. BMC Anesthesiol. 2021, 21, 52. [Google Scholar] [CrossRef]
- Higashida, R.T.; Lahue, B.J.; Torbey, M.T.; Hopkins, L.N.; Leip, E.; Hanley, D.F. Treatment of unruptured intracranial aneurysms: A nationwide assessment of effectiveness. AJNR Am. J. Neuroradiol. 2007, 28, 146–151. [Google Scholar]
- Badenes, R.; Nato, C.G.; Peña, J.D.; Bilotta, F. Inhaled anesthesia in neurosurgery: Still a role? Best Pract. Res. Clin. Anaesthesiol. 2021, 35, 231–240. [Google Scholar] [CrossRef]
- Bilotta, F.; Guerra, C.; Rosa, G. Update on anesthesia for craniotomy. Curr. Opin. Anaesthesiol. 2013, 26, 517–522. [Google Scholar] [CrossRef]
- Chen, R.M.; Chen, T.G.; Chen, T.L.; Lin, L.L.; Chang, C.C.; Chang, H.C.; Wu, C.H. Anti-inflammatory and antioxidative effects of propofol on lipopolysaccharide-activated macrophages. Ann. N. Y. Acad. Sci. 2005, 1042, 262–271. [Google Scholar] [CrossRef]
- Oshima, T.; Karasawa, F.; Satoh, T. Effects of propofol on cerebral blood flow and the metabolic rate of oxygen in humans. Acta Anaesthesiol. Scand. 2002, 46, 831–835. [Google Scholar] [CrossRef] [PubMed]
- Kaisti, K.K.; Metsähonkala, L.; Teräs, M.; Oikonen, V.; Aalto, S.; Jääskeläinen, S.; Hinkka, S.; Scheinin, H. Effects of Surgical Levels of Propofol and Sevoflurane Anesthesia on Cerebral Blood Flow in Healthy Subjects Studied with Positron Emission Tomography. Anesthesiology 2002, 96, 1358–1370. [Google Scholar] [CrossRef] [PubMed]
- Chui, J.; Mariappan, R.; Mehta, J.; Manninen, P.; Venkatraghavan, L. Comparison of propofol and volatile agents for maintenance of anesthesia during elective craniotomy procedures: Systematic review and meta-analysis. Can. J. Anaesth. 2014, 61, 347–356. [Google Scholar] [CrossRef]
- Kitahara, Y.; Taga, K.; Abe, H.; Shimoji, K. The effects of anesthetics on cortical spreading depression elicitation and c-fos expression in rats. J. Neurosurg. Anesthesiol. 2001, 13, 26–32. [Google Scholar] [CrossRef] [PubMed]
- Chung, D.Y.; Oka, F.; Ayata, C. Spreading Depolarizations: A Therapeutic Target Against Delayed Cerebral Ischemia After Subarachnoid Hemorrhage. J. Clin. Neurophysiol. 2016, 33, 196–202. [Google Scholar] [CrossRef]
- Kuzkov, V.V.; Obraztsov, M.Y.; Ivashchenko, O.Y.; Ivashchenko, N.Y.; Gorenkov, V.M.; Kirov, M.Y. Total Intravenous Versus Volatile Induction and Maintenance of Anesthesia in Elective Carotid Endarterectomy: Effects on Cerebral Oxygenation and Cognitive Functions. J. Cardiothorac. Vasc. Anesth. 2018, 32, 1701–1708. [Google Scholar] [CrossRef]
- Schoen, J.; Husemann, L.; Tiemeyer, C.; Lueloh, A.; Sedemund-Adib, B.; Berger, K.U.; Hueppe, M.; Heringlake, M. Cognitive function after sevoflurane- vs propofol-based anaesthesia for on-pump cardiac surgery: A randomized controlled trial. Br. J. Anaesth. 2011, 106, 840–850. [Google Scholar] [CrossRef]
- Banks, J.L.; Marotta, C.A. Outcomes validity and reliability of the modified Rankin scale: Implications for stroke clinical trials: A literature review and synthesis. Stroke 2007, 38, 1091–1096. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| (Total N = 1001) | Combined * (N = 236) | Inhalational † (N = 765) | p Value |
|---|---|---|---|
| Age (years) | 57 ± 11 | 59 ± 12 | 0.01 |
| Sex | |||
| Female | 170 (72%) | 587 (76%) | 0.1 |
| Male | 66 (28%) | 178 (24%) | |
| BMI | 28 ± 6 | 27± 5 | 0.3 |
| ASA Status | |||
| I | 0 (0%) | 11 (1%) | 0.1 |
| II | 76 (26%) | 257 (33%) | |
| III | 141 (65%) | 467 (61%) | |
| IV | 18 (6%) | 30 (4%) | |
| V | 1 (0.4%) | 0 (0%) | |
| Anesthetic agents | |||
| N2O | 17 (8%) | 58 (7%) | 0.9 |
| Sevoflurane | 215 (91%) | 695 (90%) | 1 |
| Desflurane | 28 (11%) | 82 (10%) | 0.7 |
| Isoflurane | 10 (5%) | 13 (1%) | 0.04 |
| Opioids | 230 (97%) | 756 (99%) | 0.2 |
| Treatment | |||
| Endovascular management | 53 (22%) | 625 (81%) | <0.001 |
| Open craniotomy | 183 (78%) | 140 (19%) | |
| Duration of procedure (min) | 210 ± 10 | 162 ± 3 | <0.001 |
| (Total N = 1001) | Endovascular * (N = 678) | † Open Craniotomy (N = 323) | p Value |
|---|---|---|---|
| Age (years) | 60 ± 12 | 56 ± 11 | <0.0001 |
| Sex | |||
| Female | 520 (77%) | 237 (73%) | 0.2 |
| Male | 158 (23%) | 86 (27%) | |
| BMI | 28 ± 6 | 27 ± 5 | 0.1 |
| ASA Status | |||
| I | 10 (1%) | 1 (0.5%) | 0.8 |
| II | 223 (33%) | 110 (34%) | |
| III | 413 (61%) | 195 (60%) | |
| IV | 32 (5%) | 16 (5%) | |
| V | 0 (0%) | 1 (0.5%) | |
| Anesthetic agents | |||
| N2O | 52 (8%) | 23 (7%) | 0.86 |
| Sevoflurane | 614 (90%) | 296 (92%) | 0.66 |
| Desflurane | 68 (11%) | 42 (13%) | 0.19 |
| Isoflurane | 2 (1%) | 21 (7%) | <0.001 |
| Opioids | 664 (97%) | 322 (99%) | 0.06 |
| Propofol infusion | 53 (8%) | 183 (57%) | <0.001 |
| Duration of procedure (min) | 122 ± 6 | 209 ± 5 | <0.001 |
| (a) | |||||||
| Baseline mRS (Total N = 619) | Long-term mRS (Total N = 596) | ||||||
| Neurologically intact | Good neurologic outcome | Poor neurologic outcome | Neurologically intact | Good neurologic outcome | Poor neurologic outcome | ||
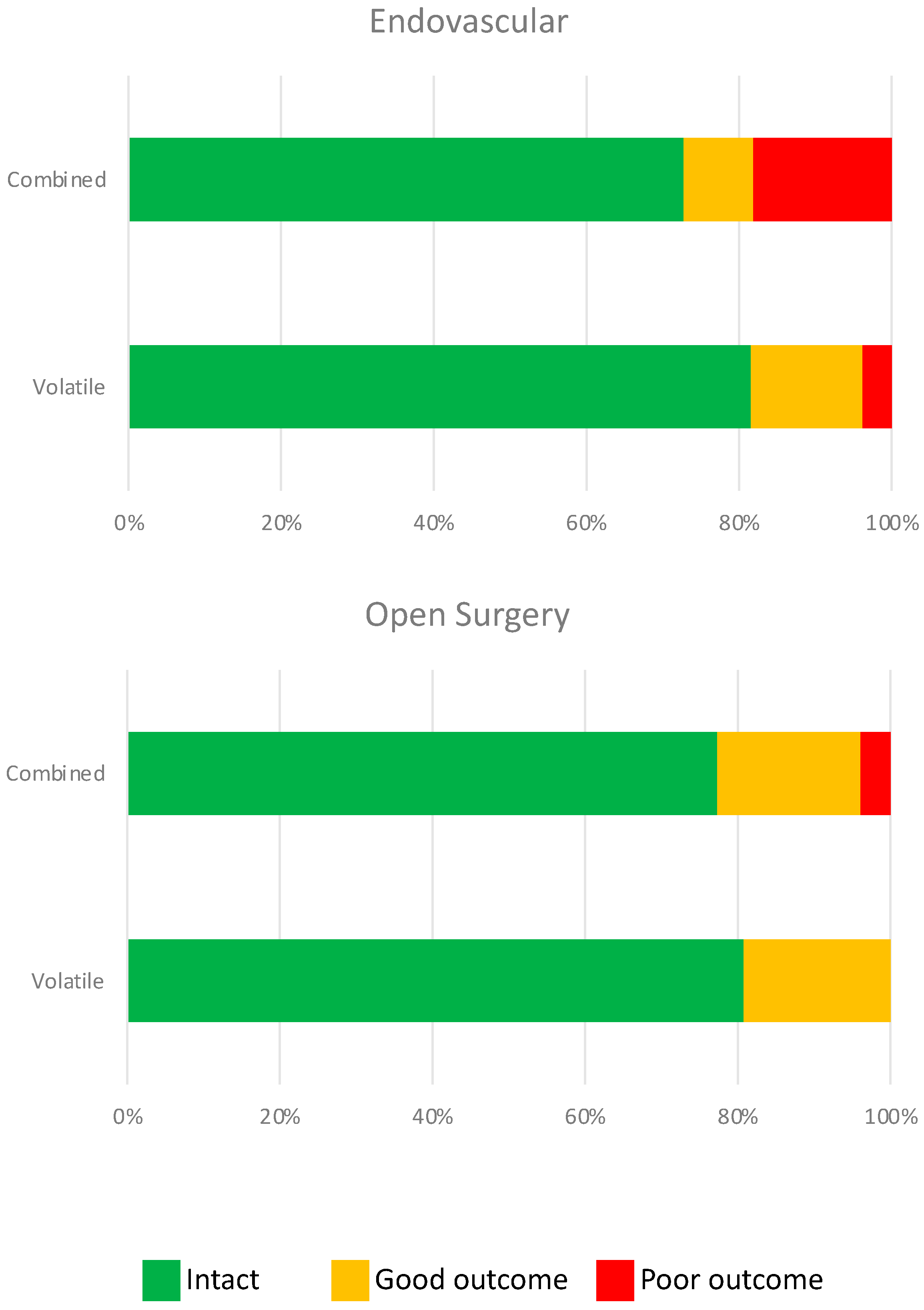
| Volatile (N = 466) | 289 (62%) | 150 (32%) | 27 (6%) | Volatile (N = 446) | 363 (81%) | 70 (16%) | 13 (2%) |
| Combined (N = 153) | 100 (65%) | 46 (30%) | 7 (5%) | Combined (N = 150) | 115 (77%) | 26 (17%) | 4 (3%) |
| p value | 0.4 | p value | 0.1 | ||||
| (b) | |||||||
| Baseline mRS (Total N = 619) | Long-term mRS (Total N = 596) | ||||||
| Neurologically intact | Good neurologic outcome | Poor neurologic outcome | Neurologically intact | Good neurologic outcome | Poor neurologic outcome | ||
| Endovascular (N = 382) | 235 (62%) | 119 (31%) | 28 (7%) | Endovascular (N = 364) | 295 (81%) | 52 (14%) | 17 (5%) |
| Open (N = 237) | 154 (65%) | 77 (32%) | 6 (3%) | Open (N = 232) | 183 (79%) | 44 (19%) | 5 (2%) |
| p value | 0.2 | p value | 0.6 | ||||
| Variables | Coefficients | Odds Ratio | 95% CI | p Value |
|---|---|---|---|---|
| N2O | 0.11 (0.39) | 1.13 | 0.72–1.13 | 0.7 |
| Sevoflurane | −0.33 (0.56) | 0.72 | 0.22–2.18 | 0.5 |
| Desflurane | −0.25 (0.48) | 0.77 | 0.28–1.90 | 0.5 |
| Isoflurane | 0.61 (1.20) | 1.84 | 0.08–16.6 | 0.6 |
| Propofol infusion | 0.29 (0.23) | 1.33 | 0.83–2.10 | 0.1 |
| Opioids | −0.31 (1.13) | 0.72 | 0.10–14.6 | 0.7 |
| Age | −0.02 (0.008) | 0.97 | 0.95–0.99 | 0.002 |
| Sex | −0.18 (0.25) | 0.83 | 0.49–1.36 | 0.4 |
| ASA status | 0.22 (0.20) | 1.23 | 0.83–1.85 | 0.2 |
| BMI | 0.04 (0.01) | 1.04 | 1.01–1.08 | 0.005 |
| ICU Admission | ICU-LOS | H-LOS | |||
|---|---|---|---|---|---|
| Anesthetic (N) ± SD | |||||
| Volatile (765) | 67% | 2 (0–2) | 2.1 ± 3.5 | 2 (2–3) | 3.8 ± 5.6 |
| Combined (236) | 80% | 2 (2–3) | 3.5 ± 5.4 | 4 (3–6) | 5.7 ± 6 |
| p value | <0.001 | <0.001 | <0.001 | ||
| Treatment (N) | |||||
| Endovascular (678) | 68% | 2 (0–2) | 2.4 ± 4.3 | 2 (2–3) | 3.9 ± 6.4 |
| Open Craniotomy (323) | 76% | 2 (2–3) | 2.7 ± 3.6 | 4 (3–5) | 4.9 ± 4.2 |
| p value | <0.01 | <0.001 | <0.001 | ||
| EndovascularManagement (N) | |||||
| Volatile (625) | 67% | 2 (0–2) | 2.1 ± 3.6 | 2 (2–3) | 3.6 ± 5.9 |
| Combined (53) | 76% | 2 (2–4) | 5.9 ± 8.8 | 3 (2–11) | 7.6 ± 9.2 |
| p value | 0.2 | <0.001 | <0.001 | ||
| Open Craniotomy | |||||
| Volatile (140) | 69% | 2 (0–3) | 2.3 ± 3.4 | 3 (3–5) | 4.6 ± 3.7 |
| Combined (183) | 81% | 2 (2–3) | 2.8 ± 3.7 | 4 (3–5) | 5.2 ± 4.6 |
| p value | 0.01 | 0.08 | 0.2 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Esmaeeli, S.; Motayagheni, N.; Brenes Bastos, A.; Ogilvy, C.S.; Thomas, A.J.; Pollard, R.; Buhl, L.K.; Baker, M.B.; Phan, S.; Hassan, O.; et al. Propofol-Based Anesthesia Maintenance and/or Volatile Anesthetics during Intracranial Aneurysm Repair: A Comparative Analysis of Neurological Outcomes. J. Clin. Med. 2023, 12, 6954. https://doi.org/10.3390/jcm12216954
Esmaeeli S, Motayagheni N, Brenes Bastos A, Ogilvy CS, Thomas AJ, Pollard R, Buhl LK, Baker MB, Phan S, Hassan O, et al. Propofol-Based Anesthesia Maintenance and/or Volatile Anesthetics during Intracranial Aneurysm Repair: A Comparative Analysis of Neurological Outcomes. Journal of Clinical Medicine. 2023; 12(21):6954. https://doi.org/10.3390/jcm12216954
Chicago/Turabian StyleEsmaeeli, Shooka, Negar Motayagheni, Andres Brenes Bastos, Christopher S Ogilvy, Ajith J Thomas, Richard Pollard, Lauren K Buhl, Maxwell B Baker, Sheshanna Phan, Omron Hassan, and et al. 2023. "Propofol-Based Anesthesia Maintenance and/or Volatile Anesthetics during Intracranial Aneurysm Repair: A Comparative Analysis of Neurological Outcomes" Journal of Clinical Medicine 12, no. 21: 6954. https://doi.org/10.3390/jcm12216954
APA StyleEsmaeeli, S., Motayagheni, N., Brenes Bastos, A., Ogilvy, C. S., Thomas, A. J., Pollard, R., Buhl, L. K., Baker, M. B., Phan, S., Hassan, O., Fehnel, C. R., Eikermann, M., Shaefi, S., & Nozari, A. (2023). Propofol-Based Anesthesia Maintenance and/or Volatile Anesthetics during Intracranial Aneurysm Repair: A Comparative Analysis of Neurological Outcomes. Journal of Clinical Medicine, 12(21), 6954. https://doi.org/10.3390/jcm12216954