- Article

Impact of Metabolic-Dysfunction-Associated Steatotic Liver Disease (MASLD) and Steatohepatitis (MASH) on Clostridioides difficile Inpatient Outcomes: A Propensity-Matched Study
- Saksham Kohli,
- Anil Philip and
- Hemant Mutneja
- + 5 authors
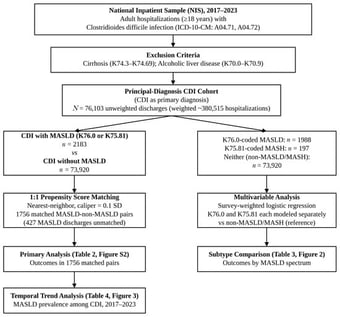
Background: Clostridioides difficile infection (CDI) remains a leading cause of hospital-acquired infection. Metabolic-dysfunction-associated steatotic liver disease (MASLD) is the most common chronic liver disease worldwide and has been associated with increased infectious susceptibility. However, whether non-cirrhotic MASLD independently worsens inpatient CDI outcomes and whether this differs across the MASLD spectrum remain unclear. Methods: We conducted a retrospective cohort study using the National Inpatient Sample (NIS) 2017–2023, identifying adult hospitalizations with a principal diagnosis of CDI. Patients with cirrhosis and alcoholic liver disease were excluded. Propensity score matching (1:1) was performed for the primary MASLD vs. non-MASLD comparison in the principal-diagnosis CDI cohort. To evaluate whether outcomes differ across the MASLD spectrum, survey-weighted multivariable logistic regression was used to compare K76.0-coded (MASLD without steatohepatitis) and K75.81-coded (MASH) hospitalizations against non-MASLD/MASH hospitalizations within the principal-diagnosis CDI cohort. The primary outcome was in-hospital mortality; secondary outcomes included complications, healthcare utilization, and discharge disposition. Results: The principal-diagnosis CDI cohort comprised 76,103 discharges (weighted ~380,515). MASLD prevalence among non-cirrhotic CDI hospitalizations nearly doubled from 1.98% in 2017 to 3.74% in 2023 (OR per year 1.089; p < 0.001). After propensity score matching (1756 pairs), MASLD was not associated with significantly higher in-hospital mortality (OR 1.252; p = 0.574) or most adverse outcomes, but was associated with lower odds of non-routine discharge (OR 0.794; p = 0.003). In the matched utilization analysis, length of stay and total charges were not significantly different, although the adjusted pre-match analysis showed higher charges among MASLD hospitalizations (+$4431; p = 0.001). Within the same principal-diagnosis cohort, K76.0-coded MASLD (n = 1988) was associated with lower odds of acute kidney injury (aOR 0.821; p = 0.004) and non-routine discharge (aOR 0.805; p = 0.001). K75.81-coded MASH (n = 197) was independently associated with higher in-hospital mortality (aOR 2.840, 95% CI 1.154–6.985; p = 0.023) and peritonitis (aOR 4.136, 95% CI 1.543–11.082; p = 0.005), although confidence intervals were wide and the number of MASH-coded hospitalizations was modest. Conclusions: The prevalence of MASLD among CDI hospitalizations is rising. Non-cirrhotic MASLD without steatohepatitis does not independently worsen inpatient CDI outcomes after adjustment, whereas K75.81-coded MASH may identify a higher-risk subgroup with increased mortality and peritonitis, pending confirmation in larger cohorts. These findings suggest that hepatic inflammatory activity, rather than steatosis alone, may drive adverse CDI outcomes and support further investigation of MASLD phenotyping in CDI risk stratification.
12 June 2026