
Colonic Dysbiosis Is Associated with Gastrointestinal Disorders More than Mother–Child Epidemiological Traits in Mexican Children with Autism Spectrum Disorders

 ,
,  , , , and
, , , and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Patient Characteristics
2.2. Gastrointestinal Assessment and Diagnosis
2.3. Methods and Assessments
2.3.1. Fecal DNA Extraction
2.3.2. 16S rRNA Gene Amplification (2S-PCR)
- Stage 1: The reaction mixture (24 µL) consisted of 2 µL (200 ng) DNA template, 12 µL of GoTaq® (DNA polymerase, dNTPs, MgCl2, and reaction buffer), sense (Fw)/antisense (Rv) primers (1 µL, 200 µM each), 8 µL PCR-grade water.
- Stage 2: 16S rRNA-amplified product (2 µL) was mixed with the same reaction mixture (total volume 24 µL) and amplified with a higher astringency (annealing temperature).
2.4. Statistical Analysis
3. Results and Discussion
3.1. Sociodemographic Information
3.2. Perinatal Clinical History of the Participants
3.3. Gastrointestinal Features of the Patients
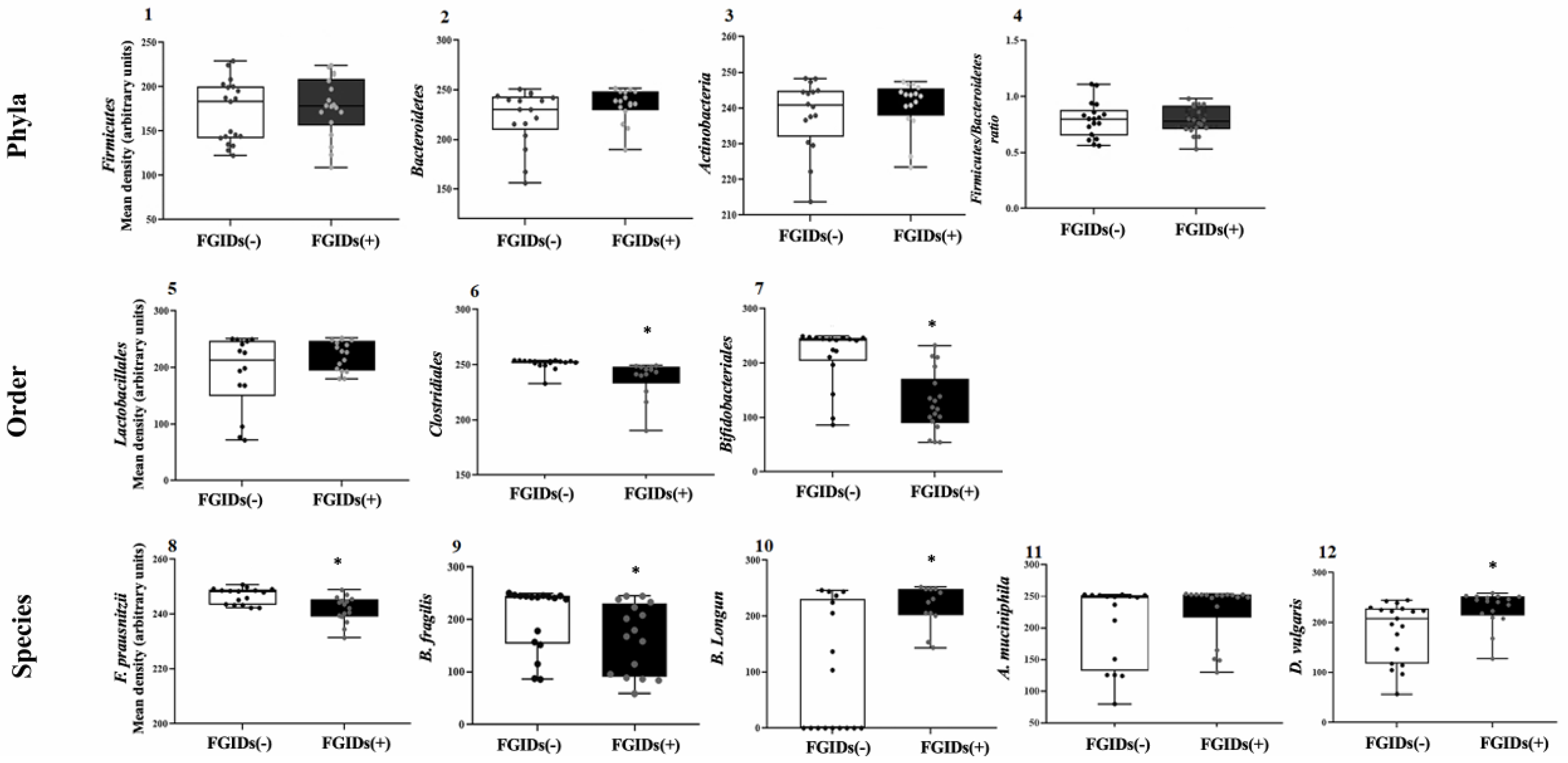
3.4. Colonic Fecal Microbiota Markers Associated with FGIDs in Autism
3.5. Differences in Colonic Fecal Microbiota Markers Between Case and Control: ROME IV Stratification
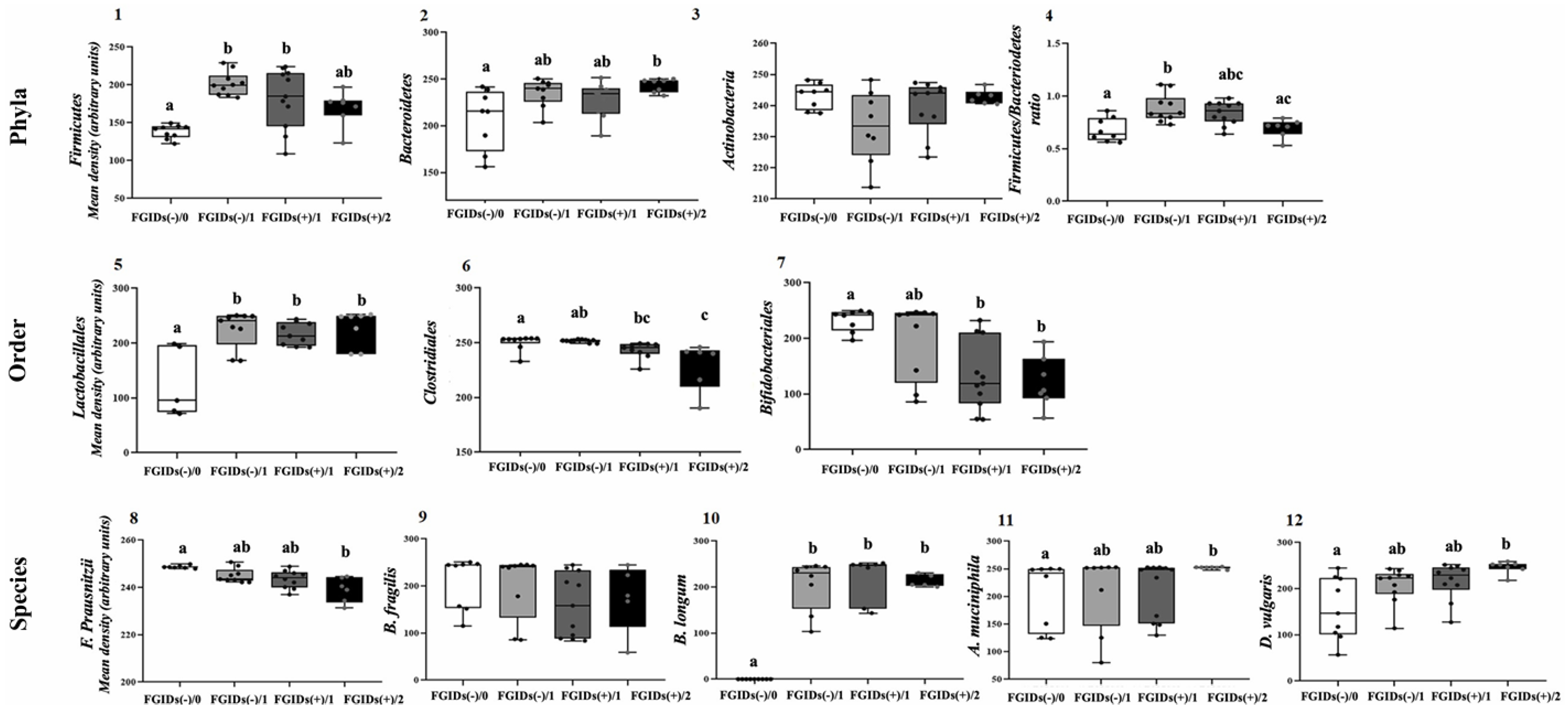
3.6. Differences in Colonic Fecal Microbiota Markers Grouped by Gastrointestinal Severity Index: ROME IV + 6-GSI Stratification
3.7. Limitations of the Study
4. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- American Psychological Association [APA]. Manual de Diagnóstico y Estadístico de los Trastornos Mentales (DSM-5); Editorial Médica Panamericana: Madrid, Spain, 2013. [Google Scholar]
- Wang, J.; Ma, B.; Wang, J.; Zhang, Z.; Chen, O. Global prevalence of autism spectrum disorder and its gastrointestinal symptoms: A systematic review and meta-analysis. Front. Psychiatry 2022, 13, 963102. [Google Scholar] [CrossRef]
- Madra, M.; Ringel, R.; Margolis, K.G. Gastrointestinal issues and autism spectrum disorder. Child Adolesc. Psychiatr. Clin. N. Am. 2020, 29, 501–513. [Google Scholar] [CrossRef]
- Drossman, D.A. Functional gastrointestinal disorders: History, pathophysiology, clinical features, and Rome IV. Gastroenterology 2016, 150, 1262–1279.e2. [Google Scholar] [CrossRef] [PubMed]
- Thulasi, V.; Steer, R.A.; Monteiro, I.M.; Ming, X. Overall severities of gastrointestinal symptoms in pediatric outpatients with and without autism spectrum disorder. Autism 2019, 23, 524–530. [Google Scholar] [CrossRef] [PubMed]
- Margolis, K.G.; Buie, T.M.; Turner, J.B.; Silberman, A.E.; Feldman, J.F.; Murray, K.F.; McSwiggan-Hardin, M.; Levy, J.; Bauman, M.L.; Veenstra-VanderWeele, J.; et al. Development of a brief parent-report screen for common gastrointestinal disorders in autism spectrum disorder. J. Autism Dev. Disord. 2018, 49, 349–362. [Google Scholar] [CrossRef]
- Lavelle, T.A.; Weinstein, M.C.; Newhouse, J.P.; Munir, K.; Kuhlthau, K.A.; Prosser, L.A. Economic burden of childhood autism spectrum disorders. Pediatrics 2014, 133, e520–e529. [Google Scholar] [CrossRef]
- Lyall, K.; Croen, L.; Daniels, J.; Fallin, M.D.; Ladd-Acosta, C.; Lee, B.K.; Park, B.Y.; Snyder, N.W.; Schendel, D.; Volk, H.; et al. The changing epidemiology of autism spectrum disorders. Annu. Rev. Public Health 2017, 38, 81–102. [Google Scholar] [CrossRef] [PubMed]
- Sanctuary, M.R.; Kain, J.N.; Angkustsiri, K.; German, J.B. Dietary considerations in autism spectrum disorders: The potential role of protein digestion and microbial putrefaction in the gut-brain axis. Front. Nutr. 2018, 5, 40. [Google Scholar] [CrossRef]
- Berding, K.; Donovan, S.M. Microbiome and nutrition in autism spectrum disorder: Current knowledge and research needs. Nutr. Rev. 2016, 74, 723–736. [Google Scholar] [CrossRef]
- Williams, B.L.; Hornig, M.; Buie, T.; Bauman, M.L.; Paik, M.C.; Wick, I.; Bennett, A.; Jabado, O.; Hirschberg, D.L.; Lipkin, W.I. Impaired carbohydrate digestion and transport and mucosal dysbiosis in the intestines of children with autism and gastrointestinal disturbances. PLoS ONE 2011, 6, e24585. [Google Scholar] [CrossRef]
- Li, Q.; Han, Y.; Dy, A.B.C.; Hagerman, R.J. The gut microbiota and autism spectrum disorders. Front. Cell. Neurosci. 2017, 11, 120. [Google Scholar] [CrossRef]
- Liu, F.; Li, J.; Wu, F.; Zheng, H.; Peng, Q.; Zhou, H. Altered composition and function of intestinal microbiota in autism spectrum disorders: A systematic review. Transl. Psychiatry 2019, 9, 43. [Google Scholar] [CrossRef] [PubMed]
- Fattorusso, A.; Di Genova, L.; Dell’Isola, G.B.; Mencaroni, E.; Esposito, S. Autism Spectrum Disorders and the Gut Microbiota. Nutrients 2019, 11, 521. [Google Scholar] [CrossRef] [PubMed]
- Tomova, A.; Husarova, V.; Lakatosova, S.; Bakos, J.; Vlkova, B.; Babinska, K.; Ostatnikova, D. Gastrointestinal microbiota in children with autism in Slovakia. Physiol. Behav. 2015, 138, 179–187. [Google Scholar] [CrossRef]
- Blesa Baviera, L.C. Trastornos digestivos funcionales pediátricos. Criterios Roma IV. Actual. Pediatría 2017, 3, 99–114. [Google Scholar]
- Heaton, K.W.; Radvan, J.; Cripps, H.; Mountford, R.A.; Braddon, F.E.; Hughes, A.O. Defecation frequency and timing, and stool form in the general population: A prospective study. Gut 1992, 33, 818–824. [Google Scholar] [CrossRef]
- Zhang, B.-W.; Li, M.; Ma, L.-C.; Wei, F.-W. A widely applicable protocol for DNA isolation from fecal samples. Biochem. Genet. 2006, 44, 494–503. [Google Scholar] [CrossRef]
- Green, M.R.; Sambrook, J. Isolation of high-molecular-weight DNA using organic solvents. Cold Spring Harb. Protoc. 2017, 2017, 356–359. [Google Scholar] [CrossRef]
- Coretti, L.; Paparo, L.; Riccio, M.P.; Amato, F.; Cuomo, M.; Natale, A.; Borrelli, L.; Corrado, G.; De Caro, C.; Comegna, M.; et al. Gut microbiota features in young children with autism spectrum disorders. Front. Microbiol. 2018, 9, 3146. [Google Scholar] [CrossRef]
- Ye, F.; Gao, X.; Wang, Z.; Cao, S.; Liang, G.; He, D.; Lv, Z.; Wang, L.; Xu, P.; Zhang, Q. Comparison of gut microbiota in autism spectrum disorders and neurotypical boys in China: A case-control study. Synth. Syst. Biotechnol. 2021, 6, 120–126. [Google Scholar] [CrossRef]
- Fitzgerald, C.B.; Shkoporov, A.N.; Sutton, T.D.S.; Chaplin, A.V.; Velayudhan, V.; Ross, R.P.; Hill, C. Comparative analysis of Faecalibacterium prausnitzii genomes shows a high level of genome plasticity and warrants separation into new species-level taxa. BMC Genom. 2018, 19, 931. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Christophersen, C.T.; Sorich, M.J.; Gerber, J.P.; Angley, M.T.; Conlon, M.A. Low relative abundances of the mucolytic bacterium Akkermansia muciniphila and Bifidobacterium spp. in feces of children with autism. Appl. Environ. Microbiol. 2011, 77, 6718–6721. [Google Scholar] [CrossRef]
- Herrera-Mejía, J.; Campos-Vega, R.; Wall-Medrano, A.; Jiménez-Vega, F. A Two-Step single plex PCR method for evaluating key colonic microbiota markers in young Mexicans with autism spectrum disorders: Protocol and pilot epidemiological application. Diagnostics 2023, 13, 2387. [Google Scholar] [CrossRef]
- Adams, J.B.; Johansen, L.J.; Powell, L.D.; Quig, D.; Rubin, R.A. Gastrointestinal flora and gastrointestinal status in children with autism–comparisons to typical children and correlation with autism severity. BMC Gastroenterol. 2011, 11, 22. [Google Scholar] [CrossRef] [PubMed]
- Leader, G.; Abberton, C.; Cunningham, S.; Gilmartin, K.; Grudzien, M.; Higgins, E.; Joshi, L.; Whelan, S.; Mannion, A. Gastrointestinal symptoms in autism spectrum disorder: A systematic review. Nutrients 2022, 14, 1471. [Google Scholar] [CrossRef] [PubMed]
- Deng, W.; Wang, S.; Li, F.; Wang, F.; Xing, Y.P.; Li, Y.; Lv, Y.; Ke, H.; Li, Z.; Lv, P.J.; et al. Gastrointestinal symptoms have a minor impact on autism spectrum disorder and associations with gut microbiota and short-chain fatty acids. Front. Microbiol. 2022, 13, 1000419. [Google Scholar] [CrossRef]
- Wingate, M.S.; Epstein, A.E.; Bello, F.O. Perinatal Epidemiology. In International Encyclopedia of Public Health; Academic Press: Cambridge, MA, USA, 2017; pp. 442–448. [Google Scholar] [CrossRef]
- Lyall, K.; Schmidt, R.J.; Hertz-Picciotto, I. Maternal lifestyle and environmental risk factors for autism spectrum disorders. Int. J. Epidemiol. 2014, 43, 443–464. [Google Scholar] [CrossRef]
- Yong, Z.; Dou, Y.; Gao, Y.; Xu, X.; Xiao, Y.; Zhu, H.; Li, S.; Yuan, B. Prenatal, perinatal, and postnatal factors associated with autism spectrum disorder cases in Xuzhou, China. Transl. Pediatr. 2021, 10, 635–646. [Google Scholar] [CrossRef]
- Sandall, J.; Tribe, R.M.; Avery, L.; Mola, G.; Visser, G.H.; Homer, C.S.; Gibbons, D.; Kelly, N.M.; Kennedy, H.P.; Kidanto, H.; et al. Short-term and long-term effects of caesarean section on the health of women and children. Lancet 2018, 392, 1349–1357. [Google Scholar] [CrossRef]
- Hoang, D.M.; Levy, E.I.; Vandenplas, Y. The impact of Caesarean section on the infant gut microbiome. Acta Paediatr. 2021, 110, 60–67. [Google Scholar] [CrossRef]
- Zhang, C.; Li, L.; Jin, B.; Xu, X.; Zuo, X.; Li, Y.; Li, Z. The Effects of Delivery Mode on the Gut Microbiota and Health: State of Art. Front. Microbiol. 2021, 12, 724449. [Google Scholar] [CrossRef] [PubMed]
- Fabiano, V.; Indrio, F.; Verduci, E.; Calcaterra, V.; Pop, T.L.; Mari, A.; Zuccotti, G.V.; Cokugras, F.C.; Pettoello-Mantovani, M.; Goulet, O. Term infant formulas influencing gut microbiota: An overview. Nutrients 2021, 13, 4200. [Google Scholar] [CrossRef] [PubMed]
- Bellani, M.; Calderoni, S.; Muratori, F.; Brambilla, P. Brain anatomy of autism spectrum disorders II. Focus on amygdala. Epidemiol. Psychiatr. Sci. 2013, 22, 309–312. [Google Scholar] [CrossRef]
- Nishi, M.; Miyake, H.; Akashi, H.; Shimizu, H.; Tateyama, H.; Chaki, R.; Tsukuda, H.; Nomura, H.; Hatanaka, Y.; Nishi, M. An index for proportion of head size to body mass during infancy college. J. Child Neurol. 1992, 7, 400–403. [Google Scholar] [CrossRef] [PubMed]
- Goldstein, A.M.; Hofstra, R.M.W.; Burns, A.J. Building a brain in the gut: Development of the enteric nervous system. Clin. Genet. 2013, 83, 307–316. [Google Scholar] [CrossRef]
- Martin, C.R.; Ling, P.-R.; Blackburn, G.L. Review of infant feeding: Key features of breast milk and infant formula. Nutrients 2016, 8, 279. [Google Scholar] [CrossRef]
- Ma, J.; Li, Z.; Zhang, W.; Zhang, C.; Zhang, Y.; Mei, H.; Zhuo, N.; Wang, H.; Wang, L.; Wu, D. Comparison of gut microbiota in exclusively breast-fed and formula-fed babies: A study of 91 term infants. Sci. Rep. 2020, 10, 15792. [Google Scholar] [CrossRef]
- Laursen, M.F. Gut Microbiota Development: Influence of Diet from Infancy to Toddlerhood. Ann. Nutr. Metab. 2021, 77, 21–34. [Google Scholar] [CrossRef]
- ROME IV Diagnostic Criteria Disorders of Gut-Brain Interaction (DGBI); Rome Foundation: Rome, Italy, 2016.
- Rinninella, E.; Raoul, P.; Cintoni, M.; Franceschi, F.; Miggiano, G.A.D.; Gasbarrini, A.; Mele, M.C. What is the healthy gut microbiota composition? A changing ecosystem across age, environment, diet, and diseases. Microorganisms 2019, 7, 14. [Google Scholar] [CrossRef]
- Rose, D.R.; Yang, H.; Serena, G.; Sturgeon, C.; Ma, B.; Careaga, M.; Hughes, H.K.; Angkustsiri, K.; Rose, M.; Hertz-Picciotto, I.; et al. Differential immune responses and microbiota profiles in children with autism spectrum disorders and co-morbid gastrointestinal symptoms. Brain Behav. Immun. 2018, 70, 354–368. [Google Scholar] [CrossRef]
- Xu, M.; Xu, X.; Li, J.; Li, F. Association between gut microbiota and autism spectrum disorder: A systematic review and meta-analysis. Front. Psychiatry 2019, 10, 473. [Google Scholar] [CrossRef] [PubMed]
- Agarwala, S.; Naik, B.; Ramachandra, N.B. Mucosa-associated specific bacterial species disrupt the intestinal epithelial barrier in the autism phenome. Brain Behav. Immun.-Health 2021, 15, 100269. [Google Scholar] [CrossRef] [PubMed]
- Wong, O.W.H.; Lam, A.M.W.; Or, B.P.N.; Mo, F.Y.M.; Shea, C.K.S.; Lai, K.Y.C.; Ma, S.L.; Hung, S.F.; Chan, S.; Kwong, T.N.Y.; et al. Disentangling the relationship of gut microbiota, functional gastrointestinal disorders and autism: A case–control study on prepubertal Chinese boys. Sci. Rep. 2022, 12, 10659. [Google Scholar] [CrossRef]
- Borriello, S. Clostridial disease of the gut. Clin. Infect. Dis. 1995, 20, S242–S250. [Google Scholar] [CrossRef]
- Uzal, F.A.; Navarro, M.A.; Li, J.; Freedman, J.C.; Shrestha, A.; McClane, B.A. Comparative pathogenesis of enteric clostridial infections in humans and animals. Anaerobe 2018, 53, 11–20. [Google Scholar] [CrossRef]
- Hughes, H.K.; Rose, D.; Ashwood, P. The gut microbiota and dysbiosis in autism spectrum disorders. Curr. Neurol. Neurosci. Rep. 2018, 18, 81. [Google Scholar] [CrossRef] [PubMed]
- Inoue, R.; Sakaue, Y.; Sawai, C.; Sawai, T.; Ozeki, M.; Romero-Pérez, G.A.; Tsukahara, T. A preliminary investigation on the relationship between gut microbiota and gene expressions in peripheral mononuclear cells of infants with autism spectrum disorders. Biosci. Biotechnol. Biochem. 2016, 80, 2450–2458. [Google Scholar] [CrossRef]
- He, X.; Liu, W.; Tang, F.; Chen, X.; Song, G. Effects of probiotics on autism spectrum disorder in children: A systematic review and meta-analysis of clinical trials. Nutrients 2023, 15, 1415. [Google Scholar] [CrossRef]
- Chen, Z.; Shi, K.; Liu, X.; Dai, Y.; Liu, Y.; Zhang, L.; Du, X.; Zhu, T.; Yu, J.; Fang, S.; et al. Gut microbial profile is associated with the severity of social impairment and IQ performance in children with autism spectrum disorder. Front. Psychiatry 2021, 12, 789864. [Google Scholar] [CrossRef]
- Lopez-Siles, M.; Duncan, S.H.; Garcia-Gil, L.J.; Martinez-Medina, M. Faecalibacterium prausnitzii: From microbiology to diagnostics and prognostics. ISME J. 2017, 11, 841–852. [Google Scholar] [CrossRef]
- Gilbert, J.A.; Krajmalnik-Brown, R.; Porazinska, D.L.; Weiss, S.J.; Knight, R. Towards effective probiotics for autism and other mental disorders? Cell 2013, 155, 1446–1448. [Google Scholar] [CrossRef] [PubMed]
- Ding, X.; Xu, Y.; Zhang, X.; Zhang, L.; Duan, G.; Song, C.; Li, Z.; Yang, Y.; Wang, Y.; Wang, X.; et al. Gut microbiota changes in patients with autism spectrum disorders. J. Psychiatr. Res. 2020, 129, 149–159. [Google Scholar] [CrossRef]
- De Angelis, M.; Piccolo, M.; Vannini, L.; Siragusa, S.; De Giacomo, A.; Serrazzanetti, D.I.; Cristofori, F.; Guerzoni, M.E.; Gobbetti, M.; Francavilla, R. Fecal microbiota and metabolome of children with autism and pervasive developmental disorder not otherwise specified. PLoS ONE 2013, 8, e76993. [Google Scholar] [CrossRef] [PubMed]
- Zou, R.; Xu, F.; Wang, Y.; Duan, M.; Guo, M.; Zhang, Q.; Zhao, H.; Zheng, H. Changes in the Gut Microbiota of Children with Autism Spectrum Disorder. Autism Res. 2020, 13, 1614–1625. [Google Scholar] [CrossRef]
- Elsaghir, H.; Reddy Reddivari, A.K. Bacteroides Fragilis. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2021. Available online: https://www.ncbi.nlm.nih.gov/books/NBK553032/ (accessed on 1 March 2024).
- Zamani, S.; Shariati, S.H.; Zali, M.R.; Aghdaei, H.A.; Asiabar, A.S.; Bokaie, S.; Nomanpour, B.; Sechi, L.A.; Feizabadi, M.M. Detection of enterotoxigenic Bacteroides fragilis in patients with ulcerative colitis. Gut Pathog. 2017, 9, 53. [Google Scholar] [CrossRef] [PubMed]
- Lin, T.-L.; Lu, C.-C.; Chen, T.-W.; Huang, C.-W.; Lu, J.-J.; Lai, W.-F.; Wu, T.-S.; Lai, C.-H.; Lai, H.-C.; Chen, Y.-L. Amelioration of maternal immune activation-induced autism relevant behaviors by gut commensal Parabacteroides goldsteinii. Int. J. Mol. Sci. 2022, 23, 13070. [Google Scholar] [CrossRef]
- Yao, S.; Zhao, Z.; Wang, W.; Liu, X. Bifidobacterium longum: Protection against inflammatory bowel disease. J. Immunol. Res. 2021, 2021, 8030297. [Google Scholar] [CrossRef]
- Srikantha, P.; Mohajeri, M.H. The possible role of the microbiota-gut-brain-axis in autism spectrum disorder. Int. J. Mol. Sci. 2019, 20, 2115. [Google Scholar] [CrossRef]
- Finegold, S.M. Desulfovibrio species are potentially important in regressive autism. Med. Hypotheses 2011, 77, 270–274. [Google Scholar] [CrossRef]
- Luo, Y.; Lan, C.; Li, H.; Ouyang, Q.; Kong, F.; Wu, A.; Ren, Z.; Tian, G.; Cai, J.; Yu, B.; et al. Rational consideration of Akkermansia muciniphila targeting intestinal health: Advantages and challenges. npj Biofilms Microbiomes 2022, 8, 81. [Google Scholar] [CrossRef]
- Clark, M.E.; He, Z.; Redding, A.M.; Joachimiak, M.P.; Keasling, J.D.; Zhou, J.Z.; Arkin, A.P.; Mukhopadhyay, A.; Fields, M.W. Transcriptomic and proteomic analyses of Desulfovibrio vulgaris biofilms: Carbon and energy flow contribute to the distinct biofilm growth state. BMC Genom. 2012, 13, 138. [Google Scholar] [CrossRef] [PubMed]
- Heidelberg, J.F.; Seshadri, R.; Haveman, S.A.; Hemme, C.L.; Paulsen, I.T.; Kolonay, J.F.; Eisen, J.A.; Ward, N.; Methe, B.; Brinkac, L.M.; et al. The genome sequence of the anaerobic, sulfate-reducing bacterium Desulfovibrio vulgaris Hildenborough. Nat. Biotechnol. 2004, 22, 554–559. [Google Scholar] [CrossRef] [PubMed]
- Monteiro, M.A.; dos Santos, A.A.A.; Gomes, L.M.M.; Rito, R.V.V.F. Autism spectrum disorder: A systematic review about nutritional interventions. Rev. Paul. Pediatr. 2020, 38, e2018262. [Google Scholar] [CrossRef]
- Hert, D.G.; Fredlake, C.P.; Barron, A.E. Advantages and limitations of next-generation sequencing technologies: A Comparison of electrophoresis and non-electrophoresis methods. Electrophoresis 2008, 29, 4618–4626. [Google Scholar] [CrossRef] [PubMed]
- Guo, X.; Xia, X.; Tang, R.; Zhou, J.; Zhao, H.; Wang, K. Development of a real-time PCR method for Firmicutes and Bacteroidetes in faeces and its application to quantify intestinal population of obese and lean pigs. Lett. Appl. Microbiol. 2008, 47, 367–373. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.W.; Chen, M.K.; Yang, B.Y.; Huang, X.J.; Zhang, X.R.; He, L.Q.; Zhang, J.; Hua, Z.C. Use of 16S rRNA Gene-Targeted Group-Specific Primers for Real-Time PCR Analysis of Predominant Bacteria in Mouse Feces. Appl. Environ. Microbiol. 2015, 81, 6749–6756. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Delroisse, J.M.; Boulvin, A.L.; Parmentier, I.; Dauphin, R.D.; Vandenbol, M.; Portetelle, D. Quantification of Bifidobacterium spp. and Lactobacillus spp. in rat fecal samples by real-time PCR. Microbiol. Res. 2008, 163, 663–670. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez-Lara, A.; Plaza-Díaz, J.; López-Uriarte, P.; Vázquez-Aguilar, A.; Reyes-Castillo, Z.; Álvarez-Mercado, A.I. Fiber Consumption Mediates Differences in Several Gut Microbes in a Subpopulation of Young Mexican Adults. Nutrients 2022, 14, 1214. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Matsuki, T.; Watanabe, K.; Tanaka, R.; Fukuda, M.; Oyaizu, H. Distribution of bifidobacterial species in human intestinal microflora examined with 16S rRNA-gene-targeted species-specific primers. Appl. Environ. Microbiol. 1999, 65, 4506–4512. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]

{kind=link}
{kind=link}
| FGID (-) | FGID (+) | p Value | |
|---|---|---|---|
| Subjects (n) | n = 21 | n = 18 | - |
| Age (years) | 9.7 ± 4.1 | 10.8 ± 4.5 | 0.761 |
| Gender (n) | 0.711 | ||
| Male | 16 (77%) | 15 (83%) | |
| Female | 5 (23%) | 3 (17%) | |
| Health services (n) | 0.423 | ||
| Yes | 14 (67%) | 16 (89%) | |
| No | 7 (33%) | 2 (11%) | |
| Type of delivery (n) | 0.031 | ||
| Vaginal | 10 (48%) | 5 (27%) | |
| Cesarean | 11 (52%) | 13 (73%) | |
| Size at birth (cm) | 49.1 ± 5.0 | 54.1 ± 5.9 | 0.034 |
| Duration of formula feeding (months) | 18.5 ± 17.6 | 23.9 ± 19.0 | 0.028 |
| ROME IV diagnostic (n) | 0.00 | ||
| None | 18 (100%) | - | |
| Diarrhea | - | 1 (5%) | |
| Constipation | - | 14 (78%) | |
| Irritable bowel syndrome + Constipation | - | 3 (17%) | |
| Gastrointestinal severity index (value) | 2.1 (±1.0) | 4.6 (±1.7) | 0.014 |
| Gastrointestinal symptoms | |||
| (last month) (n) | |||
| Gas/Flatulence | 10 (48%) | 13 (72%) | 0.043 |
| Bowel constipation | 4 (19%) | 13 (72%) | 0.001 |
| Abdominal pain | 3 | 10 (56%) | 0.010 |
| Rectal pain | 0 | 7 (39%) | 0.006 |
| Jaundice | 0 | 2 (11%) | 0.036 |
| Bloody stools | 0 | 2 (11%) | 0.036 |
| Autistic severity (value) | 32.5 (±1.2) | 34.5 (±1.1) | 0.565 |
| Variables | Total (n = 39) | FGID (-) (n = 21) | FGID (+) (n = 18) | p Value * |
|---|---|---|---|---|
| Caregiver age (years) | 37.6 ± 8.3 | 38.2 ± 8.0 | 37.5 ± 8.8 | 0.88 |
| Birth weight (g) | 3046 ± 0.69 | 3005 ± 0.58 | 3388 ± 0.67 | 0.78 |
| Duration of lactation (months) | 4.2 ± 5.7 | 5.5 ± 6.5 | 2.9 ± 3.8 | 0.13 |
| (n, %) | ||||
| Caregiver sex | ||||
| Male | 4 (10) | 2 (9.5) | 2 (11) | |
| Female | 35 (90) | 19 (90.5) | 16 (89) | 0.81 |
| Caregiver education level | 0.02 * | |||
| Primary | 4 (10) | 0 (0) | 4 (23) | |
| Secondary | 8 (20) | 2 (9.5) | 6 (33) | |
| High school | 15 (39) | 9 (43) | 6 (33) | |
| Technical//Bachelor’s degree | 10 (26) | 9 (43) | 1 (5.5) | |
| Postgraduate | 2 (5) | 1 (4.5) | 1 (5.5) | |
| Patient education status | 0.45 | |||
| Schooled | 30 (77) | 15 (71) | 15 (83) | |
| Unschooled | 9 (33) | 6 (29) | 3 (17) | |
| Birth weight classification (WHO) | 0.67 | |||
| Low (1500–2499 g) | 3 (8) | 1 (4.5) | 2 (11) | |
| Insufficient (2500–2999 g) | 9 (23) | 7 (33.5) | 2 (11) | |
| Adequate (3000–3999 g) | 24 (61) | 13 (62) | 11 (61) | |
| Macrosomia (≥4000 g) | 3 (8) | 0 (0) | 3 (17) | |
| Oxygen requirement at birth | 0.42 | |||
| Yes | 4 (10) | 1 (5) | 3 (17) | |
| No | 35 (90) | 20 (95) | 15 (83) | |
| Incubation at birth | 0.07 | |||
| Yes | 6 (15) | 2 (9.5) | 4 (22) | |
| No | 33 (85) | 19 (90.5) | 14 (72) | |
| Comorbidity | Total (n = 39) | FGID (-) (n = 21) | FGID (+) (n = 18) | OR (CI 95%) | p Value * |
|---|---|---|---|---|---|
| (n, %) | |||||
| Respiratory infections | 17 (43.6) | 7 (33.3) | 10 (55.6) | 2.67 (0.919–8.859) | 0.302 |
| Sleep disorders | 14 (35.9) | 8 (38.3) | 6 (33.3) | 0.99 (0.255–1.473) | 0.347 |
| Intestinal infections | 13 (33.3) | 5 (26.9) | 6 (33.3) | 1.36 (0.367–5.021) | 0.876 |
| Abdominal distension | 12 (31.8) | 5 (23.8) | 7 (38.9) | 1.72 (0.478–6.238) | 0.402 |
| Diarrheal stools | 12 (31.8) | 5 (23.8) | 7 (38.9) | 1.72 (0.478–6.238) | 0.402 |
| Hospitalizations | 12 (30.8) | 6 (28.6) | 6 (33.3) | 1.12 (0.311–4.071) | 0.831 |
| Urinary infections | 12 (30.8) | 7 (33.3) | 5 (27.8) | 0.84 (0.320–2.280) | 0.811 |
| Epilepsy | 8 (20.5) | 4 (19.0) | 4 (22.2) | 1.11 (0.246–3.111) | 0.947 |
| Dehydration | 7 (17.9) | 4 (19.0) | 3 (16.7) | 0.98 (0.112–1.981) | 0.712 |
| Changes in stool frequency | 7 (17.9) | 2 (19.2) | 5 (27.8) | 1.61 (0.391–6.680) | 0.506 |
| Inappetence | 6 (15.4) | 3 (14.2) | 3 (16.7) | 1.00 (0.215–5.640) | 0.909 |
| Low heigh | 6 (15.4) | 2 (9.5) | 4 (22.2) | 1.72 (0.426–11.267) | 0.341 |
| Diarrheal stools | 5 (12.8) | 3 (14.2) | 2 (11.1) | 0.98 (0.397–1.800) | 0.201 |
| Otitis | 5 (12.8) | 1 (4.8) | 4 (22.2) | 5.12 (0.996–25.989) | 0.050 |
| Asthma | 5 (12.8) | 3 (14.2) | 2 (11.1) | 0.96 (0.308–2.484) | 0.565 |
| Anemia | 4 (10.2) | 2 (9.5) | 2 (11.1) | 1.01 (0.292–2.163) | 0.578 |
| Undernutrition | 2 (5.1) | 1 (4.8) | 1 (5.6) | 1.56 (0.186–2.137) | 0.149 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Herrera-Mejía, J.; Wall-Medrano, A.; Ramos-Jiménez, A.; González-Córdova, A.F.; Jiménez-Vega, F.; Campos-Vega, R. Colonic Dysbiosis Is Associated with Gastrointestinal Disorders More than Mother–Child Epidemiological Traits in Mexican Children with Autism Spectrum Disorders. Gastroenterol. Insights 2025, 16, 15. https://doi.org/10.3390/gastroent16020015
Herrera-Mejía J, Wall-Medrano A, Ramos-Jiménez A, González-Córdova AF, Jiménez-Vega F, Campos-Vega R. Colonic Dysbiosis Is Associated with Gastrointestinal Disorders More than Mother–Child Epidemiological Traits in Mexican Children with Autism Spectrum Disorders. Gastroenterology Insights. 2025; 16(2):15. https://doi.org/10.3390/gastroent16020015
Chicago/Turabian StyleHerrera-Mejía, Julián, Abraham Wall-Medrano, Arnulfo Ramos-Jiménez, Aarón F. González-Córdova, Florinda Jiménez-Vega, and Rocio Campos-Vega. 2025. "Colonic Dysbiosis Is Associated with Gastrointestinal Disorders More than Mother–Child Epidemiological Traits in Mexican Children with Autism Spectrum Disorders" Gastroenterology Insights 16, no. 2: 15. https://doi.org/10.3390/gastroent16020015
APA StyleHerrera-Mejía, J., Wall-Medrano, A., Ramos-Jiménez, A., González-Córdova, A. F., Jiménez-Vega, F., & Campos-Vega, R. (2025). Colonic Dysbiosis Is Associated with Gastrointestinal Disorders More than Mother–Child Epidemiological Traits in Mexican Children with Autism Spectrum Disorders. Gastroenterology Insights, 16(2), 15. https://doi.org/10.3390/gastroent16020015