Salvage Radical Prostatectomy for Radio-Recurrent Prostate Cancer: An Updated Systematic Review of Oncologic, Histopathologic and Functional Outcomes and Predictors of Good Response


 ,
,
Abstract
:1. Introduction
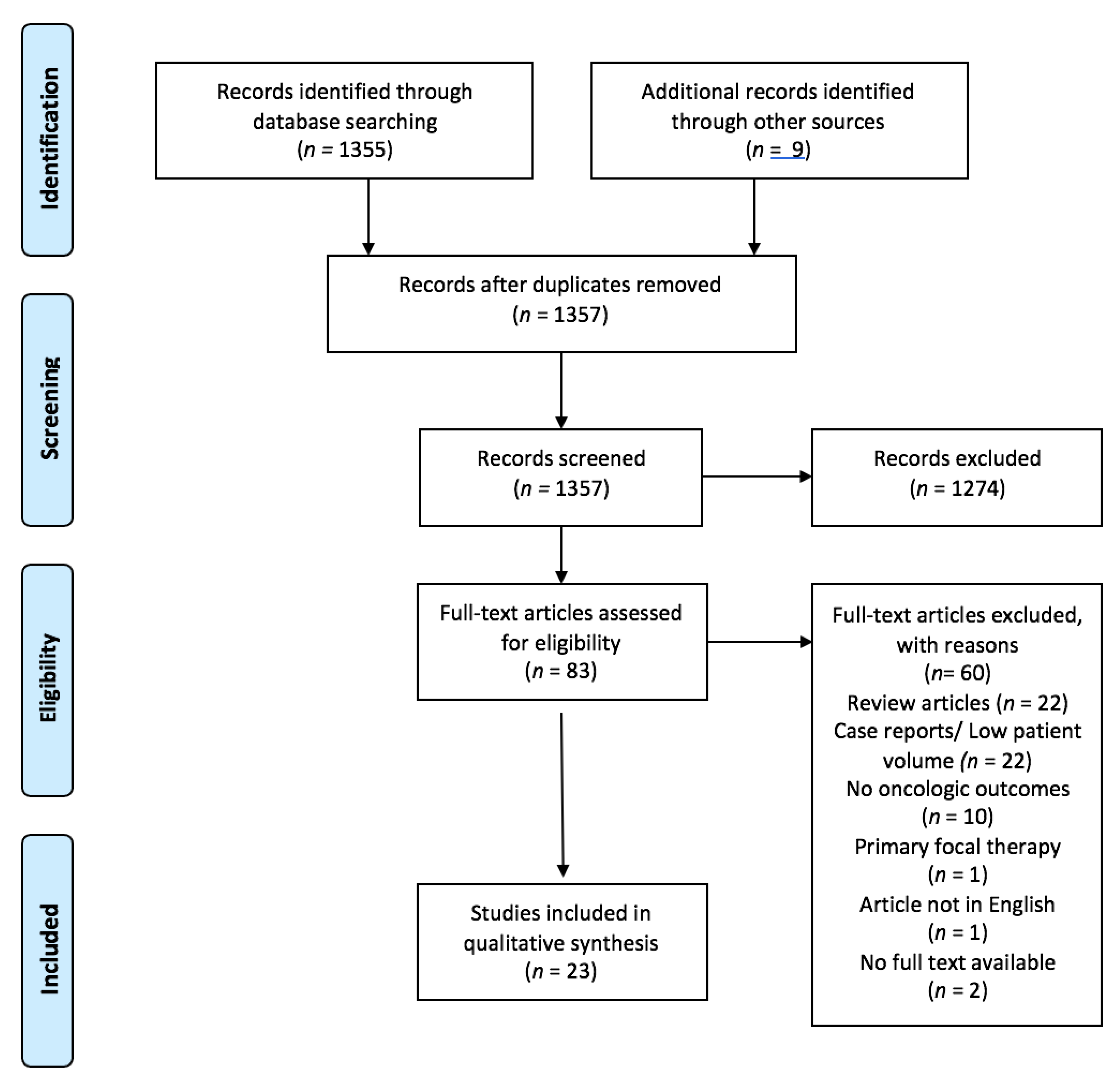
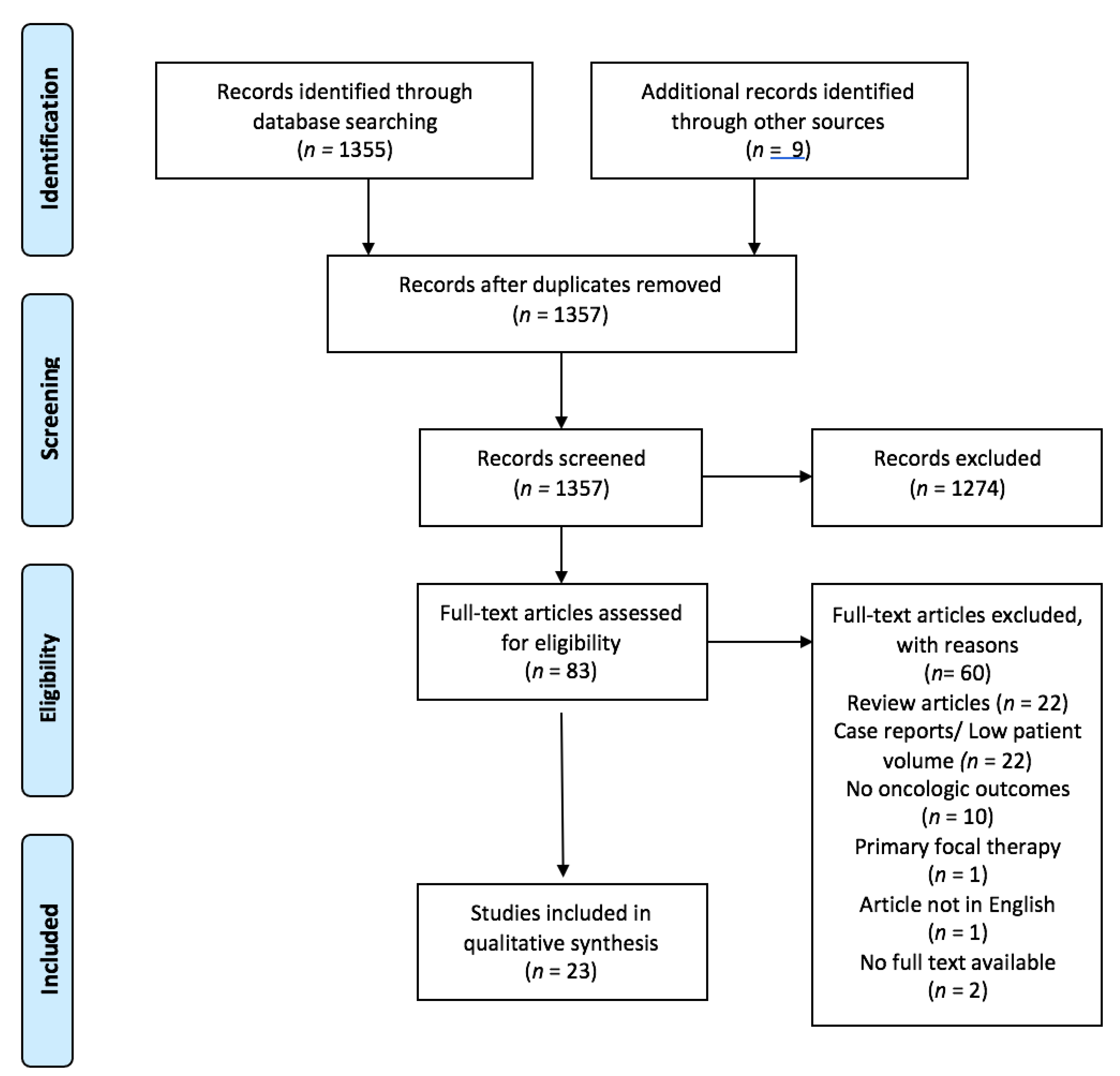
2. Methods
2.1. Search Strategy
2.2. Study Selection
2.3. Inclusion Criteria
2.4. Exclusion Criteria
2.5. Data Extraction
2.6. Missing Data
2.7. Statistics
3. Results
3.1. Epidemiology
3.2. Oncological Outcomes
3.3. Histopathological Outcomes
3.4. Functional Outcomes
3.5. Prognostic Risk Factors
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Cornford, P.; Bellmunt, J.; Bolla, M.; Briers, E.; Santis, M.D.; Gross, T.; Henry, A.M.; Joniau, S.; Lam, T.B.; Mason, M.D.; et al. EAU-ESTRO-SIOG Guidelines on Prostate Cancer. Part II: Treatment of Relapsing, Metastatic, and Castration-Resistant Prostate Cancer. Eur. Urol. 2017, 71, 630–642. [Google Scholar] [CrossRef]
- Agarwal, P.K.; Sadetsky, N.; Konety, B.R.; Resnick, M.I.; Carroll, P.R. (CaPSURE) C of the PSURE. Treatment failure after primary and salvage therapy for prostate cancer: Likelihood, patterns of care, and outcomes. Cancer 2008, 112, 307–314. [Google Scholar] [CrossRef]
- Shariat, S.F.; Kattan, M.W.; Vickers, A.J.; Karakiewicz, P.I.; Scardino, P.T. Critical review of prostate cancer predictive tools. Future Oncol. 2009, 5, 1555–1584. [Google Scholar] [CrossRef] [Green Version]
- Walz, J.; Gallina, A.; Perrotte, P.; Jeldres, C.; Trinh, Q.-D.; Hutterer, G.C.; Traumann, M.; Ramírez, A.; Shariat, S.F.; McCormack, M.; et al. Clinicians are poor raters of life-expectancy before radical prostatectomy or definitive radiotherapy for localized prostate cancer. BJU Int. 2007, 100, 1254–1258. [Google Scholar] [CrossRef]
- Chade, D.C.; Shariat, S.F.; Cronin, A.M.; Savage, C.J.; Karnes, R.J.; Blute, M.L.; Briganti, A.; Montorsi, F.; van der Poel, H.G.; Van Poppel, H.; et al. Salvage Radical Prostatectomy for Radiation-recurrent Prostate Cancer: A Multi-institutional Collaboration. Eur. Urol. 2011, 60, 205–210. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heidenreich, A.; Richter, S.; Thüer, D.; Pfister, D. Prognostic Parameters, Complications, and Oncologic and Functional Outcome of Salvage Radical Prostatectomy for Locally Recurrent Prostate Cancer after 21st-Century Radiotherapy. Eur. Urol. 2010, 57, 437–445. [Google Scholar] [CrossRef] [PubMed]
- Gotto, G.T.; Yunis, L.H.; Vora, K.; Eastham, J.A.; Scardino, P.T.; Rabbani, F. Impact of Prior Prostate Radiation on Complications After Radical Prostatectomy. J. Urol. 2010, 184, 136–142. [Google Scholar] [CrossRef] [PubMed]
- Moschini, M.; Zaffuto, E.; Karakiewicz, P.; Mattei, A.; Gandaglia, G.; Fossati, N.; Montorsi, F.; Briganti, A.; Shariat, S.F. The effect of androgen deprivation treatment on subsequent risk of bladder cancer diagnosis in male patients treated for prostate cancer. World J. Urol. 2018, 37, 1127–1135. [Google Scholar] [CrossRef] [PubMed]
- Gandaglia, G.; Sun, M.; Popa, I.; Schiffmann, J.; Trudeau, V.; Shariat, S.F.; Trinh, Q.-D.; Graefen, M.; Widmer, H.; Saad, F.; et al. Cardiovascular Mortality in Patients With Metastatic Prostate Cancer Exposed to Androgen Deprivation Therapy: A Population-Based Study. Clin. Genitourin. Cancer 2015, 13, e123–e130. [Google Scholar] [CrossRef]
- Kluth, L.A.; Shariat, S.F.; Kratzik, C.; Tagawa, S.; Sonpavde, G.; Rieken, M.; Scherr, D.; Pummer, K. The hypothalamic–pituitary–gonadal axis and prostate cancer: Implications for androgen deprivation therapy. World J. Urol. 2013, 32, 669–676. [Google Scholar] [CrossRef]
- Chade, D.C.; Eastham, J.; Graefen, M.; Hu, J.C.; Karnes, R.J.; Klotz, L.; Montorsi, F.; van Poppel, H.; Scardino, P.T.; Shariat, S.F. Cancer Control and Functional Outcomes of Salvage Radical Prostatectomy for Radiation-recurrent Prostate Cancer: A Systematic Review of the Literature. Eur. Urol. 2012, 61, 961–971. [Google Scholar] [CrossRef] [PubMed]
- Onol, F.F.; Bhat, S.; Moschovas, M.; Rogers, T.; Ganapathi, H.; Roof, S.; Rocco, B.; Patel, V. Comparison of outcomes of salvage robot-assisted laparoscopic prostatectomy for post-primary radiation vs focal therapy. BJU Int. 2020, 125, 103. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jansen, B.H.; van Leeuwen, P.J.; Wondergem, M.; van der Sluis, T.M.; Nieuwenhuijzen, J.A.; Knol, R.J.; van Moorselaar, R.J.; van der Poel, H.G.; Oprea-Lager, D.-E.; Vis, A.N. Detection of Recurrent Prostate Cancer Using Prostate-specific Membrane Antigen Positron Emission Tomography in Patients not Meeting the Phoenix Criteria for Biochemical Recurrence After Curative Radiotherapy. Eur. Urol. Oncol. 2020, in press. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grubmüller, B.; Baltzer, P.; D’Andrea, D.; Korn, S.; Haug, A.; Hacker, M.; Grubmüller, K.H.; Goldner, G.M.; Wadsak, W.; Pfaff, S.; et al. 68Ga-PSMA 11 ligand PET imaging in patients with biochemical recurrence after radical prostatectomy–diagnostic performance and impact on therapeutic decision-making. Eur. J. Nucl. Med. Mol. Imaging 2017, 49, 1374–1378. [Google Scholar] [CrossRef]
- Mohler, J.L.; Antonarakis, E.S.; Armstrong, A.J.; D’Amico, A.V.; Davis, B.J.; Dorff, T.; Eastham, J.A.; Enke, C.A.; Farrington, T.A.; Higano, C.S.; et al. Prostate Cancer, Version 2.2019, NCCN Clinical Practice Guidelines in Oncology. JNCCN 2019, 17, 479–505. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. J. Clin. Epidemiol. 2009, 62, e1-34. [Google Scholar] [CrossRef] [Green Version]
- Metcalfe, M.J.; Troncoso, P.; Guo, C.C.; Chen, H.-C.; Bozkurt, Y.; Ward, J.F.; Pisters, L.L. Salvage prostatectomy for post-radiation adenocarcinoma with treatment effect: Pathological and oncological outcomes. Can. Urol. Assoc. J. 2017, 11, E277–E284. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kenney, P.A.; Nawaf, C.B.; Mustafa, M.; Wen, S.; Wszolek, M.F.; Pettaway, C.A.; Ward, J.; Davis, J.W.; Pisters, L.L. Robotic-assisted laparoscopic versus open salvage radical prostatectomy following radiotherapy. Can. J. Urol. 2016, 23, 8271–8277. [Google Scholar] [PubMed]
- Mandel, P.; Steuber, T.; Ahyai, S.; Kriegmair, M.; Schiffmann, J.; Boehm, K.; Heinzer, H.; Michl, U.; Schlomm, T.; Haese, A.; et al. Salvage radical prostatectomy for recurrent prostate cancer: Verification of European Association of Urology guideline criteria. BJU Int. 2015, 117, 55–61. [Google Scholar] [CrossRef] [Green Version]
- Bates, A.S.; Samavedi, S.; Kumar, A.; Mouraviev, V.; Rocco, B.; Coelho, R.; Palmer, K.; Patel, V.R. Salvage robot assisted radical prostatectomy: A propensity matched study of perioperative, oncological and functional outcomes. European journal of surgical oncology. EJSO 2015, 41, 1540–1546. [Google Scholar] [CrossRef] [PubMed]
- Yuh, B.; Ruel, N.; Muldrew, S.; Mejia, R.; Novara, G.; Kawachi, M.; Wilson, T. Complications and outcomes of salvage robot-assisted radical prostatectomy: A single-institution experience. BJU Int. 2014, 113, 769–776. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Meeks, J.J.; Walker, M.; Bernstein, M.; Eastham, J.A. Seminal vesicle involvement at salvage radical prostatectomy. BJU Int. 2013, 111, E342–E347. [Google Scholar] [CrossRef] [PubMed]
- Gorin, M.A.; Manoharan, M.; Shah, G.; Eldefrawy, A.; Soloway, M.S. Urological Oncology Salvage open radical prostatectomy after failed radiation therapy: A single center experience. Cent. Eur. J. Urol. 2011, 64, 144–147. [Google Scholar] [CrossRef] [Green Version]
- Eandi, J.A.; Link, B.A.; Nelson, R.A.; Josephson, D.Y.; Lau, C.; Kawachi, M.H.; Wilson, T.G. Robotic Assisted Laparoscopic Salvage Prostatectomy for Radiation Resistant Prostate Cancer. J. Urol. 2010, 183, 133–137. [Google Scholar] [CrossRef] [PubMed]
- Pisters, L.L.; Leibovici, D.; Blute, M.; Zincke, H.; Sebo, T.J.; Slezak, J.M.; Izawa, J.; Ward, J.; Scott, S.M.; Madsen, L.; et al. Locally Recurrent Prostate Cancer After Initial Radiation Therapy: A Comparison of Salvage Radical Prostatectomy Versus Cryotherapy. J. Urol. 2009, 182, 517–527. [Google Scholar] [CrossRef]
- Leonardo, C.; Simone, G.; Papalia, R.; Franco, G.; Guaglianone, S.; Gallucci, M. Salvage radical prostatectomy for recurrent prostate cancer after radiation therapy. Int. J. Urol. Off. J. Jpn. Urol. Assoc. 2009, 16, 584–586. [Google Scholar] [CrossRef]
- Paparel, P.; Cronin, A.M.; Savage, C.; Scardino, P.T.; Eastham, J.A. Oncologic Outcome and Patterns of Recurrence after Salvage Radical Prostatectomy. Eur. Urol. 2009, 55, 404–410. [Google Scholar] [CrossRef] [PubMed]
- Sanderson, K.M.; Penson, D.; Cai, J.; Groshen, S.; Stein, J.P.; Lieskovsky, G.; Skinner, D.G. Salvage Radical Prostatectomy: Quality of Life Outcomes and Long-Term Oncological Control of Radiorecurrent Prostate Cancer. J. Urol. 2006, 176, 2025–2032. [Google Scholar] [CrossRef]
- Amling, C.L.; E Lerner, S.; Martin, S.K.; Slezak, J.M.; Blute, M.L.; Zincke, H. Deoxyribonucleic acid ploidy and serum prostate specific antigen predict outcome following salvage prostatectomy for radiation refractory prostate cancer. J. Urol. 1999, 161, 857–862. [Google Scholar] [CrossRef]
- Tefilli, M.V.; Gheiler, E.L.; Tiguert, R.; Banerjee, M.; Forman, J.; Pontes, J.; Wood, D.P. Salvage surgery or salvage radiotherapy for locally recurrent prostate cancer. Urology 1998, 52, 224–229. [Google Scholar] [CrossRef]
- E Lerner, S.; Blute, M.L.; Zincke, H. Critical evaluation of salvage surgery for radio-recurrent/resistant prostate cancer. J. Urol. 1995, 154, 1103–1109. [Google Scholar] [CrossRef]
- Rogers, E.; Ohori, M.; Kassabian, V.S.; Wheeler, T.M.; Scardino, P.T. Salvage Radical Prostatectomy. J. Urol. 1995, 153, 104–110. [Google Scholar] [CrossRef] [PubMed]
- Zincke, H. Radical Prostatectomy and Exenterative Procedures for Local Failure after Radiotherapy with Curative Intent: Comparison of Outcomes. J. Urol. 1992, 147, 894–899. [Google Scholar] [CrossRef]
- Rainwater, L.M.; Zincke, H. Radical Prostatectomy After Radiation Therapy for Cancer of the Prostate: Feasibility and Prognosis. J. Urol. 1988, 140, 1455–1459. [Google Scholar] [CrossRef]
- Vartolomei, M.D.; D’Andrea, D.; Chade, D.C.; Soria, F.; Kimura, S.; Foerster, B.; Abufaraj, M.; Mathieu, R.; Moschini, M.; Rouprêt, M.; et al. Role of serum cholinesterase in patients treated with salvage radical prostatectomy. Urol. Oncol. Semin. Orig. Invest. 2019, 37, 123–129. [Google Scholar] [CrossRef]
- Pearce, S.M.; Richards, K.; Patel, S.G.; Pariser, J.; Eggener, S.E. Population-based analysis of salvage radical prostatectomy with examination of factors associated with adverse perioperative outcomes. Urol. Oncol. Semin. Orig. Invest. 2015, 33, 163.e1–163.e6. [Google Scholar] [CrossRef] [PubMed]
- Bianco, F.J.; Scardino, P.T.; Stephenson, A.J.; Diblasio, C.J.; Fearn, P.A.; Eastham, J.A. Long-term oncologic results of salvage radical prostatectomy for locally recurrent prostate cancer after radiotherapy. Int. J. Radiat. Oncol. 2005, 62, 448–453. [Google Scholar] [CrossRef]
- Rouvière, O.; Vitry, T.; Lyonnet, D. Imaging of prostate cancer local recurrences: Why and how? Eur. Radiol. 2010, 20, 1254–1266. [Google Scholar] [CrossRef]
- Luiting, H.B.; Van Leeuwen, P.J.; Busstra, M.B.; Brabander, T.; Van Der Poel, H.G.; Donswijk, M.; Vis, A.N.; Emmett, L.; Stricker, P.D.; Roobol, M.J. Use of gallium-68 prostate-specific membrane antigen positron-emission tomography for detecting lymph node metastases in primary and recurrent prostate cancer and location of recurrence after radical prostatectomy: An overview of the current literature. BJU Int. 2019, 125, 206–214. [Google Scholar] [CrossRef]
- Oehus, A.-K.; Kroeze, S.G.C.; Schmidt-Hegemann, N.-S.; Vogel, M.M.E.; Kirste, S.; Becker, J.; Burger, I.A.; Derlin, T.; Bartenstein, P.; Eiber, M.; et al. Efficacy of PSMA ligand PET-based radiotherapy for recurrent prostate cancer after radical prostatectomy and salvage radiotherapy. BMC Cancer 2020, 20, 362–369. [Google Scholar] [CrossRef]
- Ingrosso, G.; Becherini, C.; Lancia, A.; Caini, S.; Ost, P.; Francolini, G.; Høyer, M.; Bottero, M.; Bossi, A.; Zilli, T.; et al. Nonsurgical Salvage Local Therapies for Radiorecurrent Prostate Cancer: A Systematic Review and Meta-analysis. Eur. Urol. Oncol. 2020, 3, 183–197. [Google Scholar] [CrossRef]
- Marra, G.; Karnes, R.J.; Calleris, G.; Oderda, M.; Alessio, P.; Palazzetti, A.; Battaglia, A.; Pisano, F.; Munegato, S.; Munoz, F.; et al. Oncological outcomes of salvage radical prostatectomy for recurrent prostate cancer in the contemporary era: A multicenter retrospective study. Urol. Oncol. Semin. Orig. Invest. 2021, 39, 296.e21–296.e29. [Google Scholar] [CrossRef]
- Alibhai, S.M.; Gogov, S.; Allibhai, Z. Long-term side effects of androgen deprivation therapy in men with non-metastatic prostate cancer: A systematic literature review. Crit. Rev. Oncol. 2006, 60, 201–215. [Google Scholar] [CrossRef] [PubMed]
- Philippou, Y.; Parker, R.A.; Volanis, D.; Gnanapragasam, V.J. Comparative Oncologic and Toxicity Outcomes of Salvage Radical Prostatectomy Versus Nonsurgical Therapies for Radiorecurrent Prostate Cancer: A Meta–Regression Analysis. Eur. Urol. Focus 2016, 2, 158–171. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Valle, L.F.; Lehrer, E.J.; Markovic, D.; Elashoff, D.; Levin-Epstein, R.; Karnes, R.J.; Reiter, R.E.; Rettig, M.; Calais, J.; Nickols, N.G.; et al. A Systematic Review and Meta-analysis of Local Salvage Therapies After Radiotherapy for Prostate Cancer (MASTER). Eur. Urol. 2020, in press. [Google Scholar] [CrossRef] [PubMed]
- Duchesne, G.M.; Woo, H.H.; Bassett, J.K.; Bowe, S.; D’Este, C.; Frydenberg, M.; King, M.; Ledwich, L.; Loblaw, A.; Malone, S.; et al. Timing of androgen-deprivation therapy in patients with prostate cancer with a rising PSA (TROG 03.06 and VCOG PR 01-03 [TOAD]): A randomised, multicentre, non-blinded, phase 3 trial. Lancet Oncol. 2016, 17, 727–737. [Google Scholar] [CrossRef]
- Payne, H.; Khan, A.; Chowdhury, S.; Davda, R. Hormone therapy for radiorecurrent prostate cancer. World J. Urol. 2012, 31, 1333–1338. [Google Scholar] [CrossRef]
- Siddiqui, S.A.; Boorjian, S.A.; Inman, B.; Bagniewski, S.; Bergstralh, E.J.; Blute, M.L. Timing of Androgen Deprivation Therapy and its Impact on Survival After Radical Prostatectomy: A Matched Cohort Study. J. Urol. 2008, 179, 1830–1837, discussion 1837. [Google Scholar] [CrossRef] [PubMed]
- Boorjian, S.A.; Thompson, R.H.; Tollefson, M.K.; Rangel, L.J.; Bergstralh, E.J.; Blute, M.L.; Karnes, R.J. Long-Term Risk of Clinical Progression After Biochemical Recurrence Following Radical Prostatectomy: The Impact of Time from Surgery to Recurrence. Eur. Urol. 2011, 59, 893–899. [Google Scholar] [CrossRef]
- Brassetti, A.; Bollens, R. Laparoscopic radical prostatectomy in 2018: 20 years of worldwide experiences, experimentations, researches and refinements. Minerva Chir. 2019, 74, 37–53. [Google Scholar] [CrossRef]
- Klotz, L. Active surveillance for prostate cancer: For whom? J. Clin. Oncol. 2005, 23, 8165–8169. [Google Scholar] [CrossRef] [PubMed]
- Fossati, N.; Willemse, P.-P.M.; den Broeck, T.V.; van den Bergh, R.C.N.; Yuan, C.Y.; Briers, E.; Bellmunt, J.; Bolla, M.; Cornford, P.; Santis, M.D.; et al. The Benefits and Harms of Different Extents of Lymph Node Dissection During Radical Prostatectomy for Prostate Cancer: A Systematic Review. Eur. Urol. 2017, 72, 84–109. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| First Author/Yr | Nb. of Patients | RT Type, % (RT/BT/COMB or Other Focal) | RT + ADT, % | Median Follow-Up | PSM% | Lymph Node Involvement, % | >pT2 after SRP, % |
|---|---|---|---|---|---|---|---|
| Onol/2020 [12] | 94 | 60.6/24.5/14.9 | 25.5 | 32 | 17 | 10.6 | 50 |
| Vartolomei/2019 [35] | 214 | - | 47.7 | 25.3 | 22 | 18.7 | 43 |
| Metcalfe/2017 [17] | 70 | 68.6/20/11.4 | 26 | - | 20 | 45.8 | 61.4 |
| Kenney/2016 [18] | 39 | 61.5/38.5/0 | - | - | 15.4 | 12.8 | 61.5 |
| Mandel/2016 [19] | 55 | 49.1/50.9/0 | 45 | 36 | 27 | 21.8 | 50 |
| Bates/2015 [20] | 53 | 62.2/26.4/11.2 | - | 36 | 18.9 | 26.4 | 51 |
| Pearce/2014 [36] | 408 | 89/11/0 | - | - | 33.7 | 6.2 | 49 |
| Yuh/2014 [21] | 51 | 47.1/43.1/9.8 | 19.6 | 36 | 31.4 | 78.4 | 51 |
| Meeks/2013 [22] | 206 | 66/29/5 | - | - | 14 | 21 | 57 |
| Gorin/2011 [23] | 24 | 54/46/0 | 58 | - | 45.8 | 13.3 | 54.2 |
| Chade/2011 [5] | 404 | 65/19/16 | - | - | 25 | 16 | 45 |
| Eandi/2010 [24] | 18 | - | 2.2 | 18 | 28 | 20 | 50 |
| Pisters/2009 [25] | 42 | 92.9/7.1/0 | 0 | 96 | - | - | - |
| Leonardo/2009 [26] | 32 | 100/0/0 | 0 | 35 | 34.4 | 0 | 46.9 |
| Paparel/2008 [27] | 146 | - | - | 45 | 16 | 13 | 63 |
| Sanderson/2006 [28] | 51 | 59/23/18 | 18 | 84 | 35.5 | 15.7 | 44 |
| Bianco/2005 [37] | 100 | 29/42/29 | 16 | 60 | 21 | 9 | 65 |
| Amling/1999 [29] | 108 | 98/2/0 | 0 | - | 36 | 18 | 61 |
| Tefilli/1998 [30] | 27 | - | - | 34 | 18.5 | - | 33 |
| Lerner/1995 [31] | 79 | 90/10/0 | - | 50 | 40 | 8 | 61 |
| Rogers/1995 [32] | 40 | 35/65/0 | 2.5 | 39 | 37 | 5 | 80 |
| Zincke/1992 [33] | 32 | 100/0/0 | 0 | 48 | - | - | - |
| Rainwater/1988 [34] | 30 | - | - | 80 | - | - | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Grubmüller, B.; Jahrreiss, V.; Brönimann, S.; Quhal, F.; Mori, K.; Heidenreich, A.; Briganti, A.; Tilki, D.; Shariat, S.F. Salvage Radical Prostatectomy for Radio-Recurrent Prostate Cancer: An Updated Systematic Review of Oncologic, Histopathologic and Functional Outcomes and Predictors of Good Response. Curr. Oncol. 2021, 28, 2881-2892. https://doi.org/10.3390/curroncol28040252
Grubmüller B, Jahrreiss V, Brönimann S, Quhal F, Mori K, Heidenreich A, Briganti A, Tilki D, Shariat SF. Salvage Radical Prostatectomy for Radio-Recurrent Prostate Cancer: An Updated Systematic Review of Oncologic, Histopathologic and Functional Outcomes and Predictors of Good Response. Current Oncology. 2021; 28(4):2881-2892. https://doi.org/10.3390/curroncol28040252
Chicago/Turabian StyleGrubmüller, Bernhard, Victoria Jahrreiss, Stephan Brönimann, Fahad Quhal, Keiichiro Mori, Axel Heidenreich, Alberto Briganti, Derya Tilki, and Shahrokh F. Shariat. 2021. "Salvage Radical Prostatectomy for Radio-Recurrent Prostate Cancer: An Updated Systematic Review of Oncologic, Histopathologic and Functional Outcomes and Predictors of Good Response" Current Oncology 28, no. 4: 2881-2892. https://doi.org/10.3390/curroncol28040252
APA StyleGrubmüller, B., Jahrreiss, V., Brönimann, S., Quhal, F., Mori, K., Heidenreich, A., Briganti, A., Tilki, D., & Shariat, S. F. (2021). Salvage Radical Prostatectomy for Radio-Recurrent Prostate Cancer: An Updated Systematic Review of Oncologic, Histopathologic and Functional Outcomes and Predictors of Good Response. Current Oncology, 28(4), 2881-2892. https://doi.org/10.3390/curroncol28040252