Abstract
Background: Basic emergency care is an important component of health system strengthening in resource-limited settings in sub-Saharan Africa. Objectives: This scoping review mapped and synthesised evidence on the implementation, capacity-building approaches, and policy implications of the WHO/ICRC Basic Emergency Care (BEC) course in the region. Methods: Twenty studies from 13 countries were included. Reported facilitators of BEC implementation included perceived relevance to frontline practice, practical and structured course content, contextual adaptation, mentorship, and training-of-trainers or cascade approaches. Reported barriers included time constraints, staffing shortages, limited infrastructure and emergency care resources, and technological challenges affecting digital reinforcement strategies. Across studies, BEC was generally associated with short-term improvements in provider knowledge, confidence, and perceived competence. However, implementation outcomes were reported inconsistently and were largely limited to acceptability, feasibility, and appropriateness, with less evidence on adoption, cost, penetration, and sustainability. Evidence on longer-term retention, practice change, patient outcomes, and broader system-level impact remained limited. Conclusions: Overall, BEC appears to be a potentially useful and context-appropriate approach to strengthening frontline emergency care training, but stronger longitudinal and implementation-focused evaluations are needed.
1. Introduction
Sub-Saharan Africa faces a disproportionate burden of acute illnesses and injuries, yet emergency care systems across the region remain underdeveloped [1,2]. Several deaths and disabilities in low-resource settings are attributable to conditions that are potentially treatable with timely and appropriate emergency care [3]. However, limited training opportunities for frontline healthcare providers, inadequate infrastructure, inconsistent application of clinical protocols, and weak referral systems continue to undermine the delivery of effective emergency services [4,5]. These challenges contribute substantially to preventable morbidity and mortality and highlight the need for practical and scalable approaches to strengthen emergency care capacity across the region.
Emergency care has increasingly been recognised as an essential component of universal health coverage and resilient health systems [6]. In settings where specialist services are limited, frontline healthcare workers are often required to assess, stabilise, and initiate management for critically ill and injured patients with minimal support [7]. Building the competencies of these providers is therefore a key strategy for improving patient outcomes. Standardised training packages that are feasible in resource-constrained settings may help address current gaps by improving the early recognition and management of life-threatening conditions and by supporting timelier referral to higher levels of care.
The World Health Organization (WHO) Basic Emergency Care (BEC) course was developed in response to this need as a structured and context-appropriate training programme for frontline healthcare providers. First introduced in 2018, the course was developed through a collaboration between the International Committee of the Red Cross (ICRC), the International Federation for Emergency Medicine (IFEM), medical education specialists, and frontline health workers, including nurses, doctors, and clinical officers. The programme aims to strengthen the early recognition, initial stabilisation, and timely referral of critically ill and injured patients, particularly in low-resource settings [8]. This distinguishes BEC from other emergency care courses such as Advanced trauma life support (ATLS), which focuses on trauma, and Emergency Triage Assessment and Treatment (ETAT), which focuses on the triage and emergency treatment of children, by positioning BEC as a broad, practical course for frontline providers managing diverse adult and paediatric emergencies in resource-constrained settings [9,10]. Since its introduction, the BEC course has been implemented in several countries in sub-Saharan Africa such as Uganda, Rwanda, Nigeria, South Africa and Tanzania, and emerging evidence suggests that it may improve provider knowledge, confidence, and aspects of emergency care practice [11,12,13,14,15].
Despite this growing body of work, the evidence remains fragmented and is largely reported through individual country experiences or context-specific implementation studies. There is still limited synthesis of how the BEC course has been delivered across sub-Saharan Africa, the modalities used for capacity building, the barriers and facilitators influencing implementation, and the broader implications for policy and health system strengthening. This scoping review aims to map and synthesise the published evidence on the implementation of the WHO Basic Emergency Care course in sub-Saharan Africa and to identify key training modalities, implementation strategies, barriers, facilitators, and policy implications relevant to strengthening sustainable emergency care systems in the region.
2. Materials and Methods
2.1. Study Design
This study employed a scoping review design to systematically map the existing evidence on the implementation and outcomes of the WHO BEC training interventions in sub-Saharan Africa. The review was conducted in accordance with the Joanna Briggs Institute (JBI) methodological framework for scoping reviews [16]. The JBI framework builds on the seminal work of Arksey and O’Malley [17] and subsequent refinements proposed by Levac et al., which collectively outline a systematic process for identifying, selecting, and synthesizing relevant evidence [18].
The review process followed six sequential stages:
- Identification of the research questions.
- Identification of relevant studies.
- Study selection based on predefined eligibility criteria independently.
- Data charting and extraction.
- Collation and synthesis of evidence.
- Stakeholder consultation to contextualize findings.
To ensure transparency and reproducibility, this study adhered to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses Extension for Scoping Reviews (PRISMA-ScR) reporting guidelines [19].
2.2. Conceptual Framework
The analytical framework for this review integrates concepts from implementation science and health systems strengthening. Basic Emergency Care training programs aim to strengthen frontline clinical capacity to manage acute illness and injury, particularly in resource-limited settings where access to specialized emergency medicine training is limited.
To support a theoretically informed analysis, extracted data were mapped to two complementary lenses: Proctor’s implementation outcomes framework for reported implementation outcomes, and a health systems strengthening perspective for barriers, facilitators, capacity-building approaches, and policy implications. These analytical lenses informed both the synthesis and presentation of findings.
2.3. Eligibility Criteria (Population–Concept–Context Framework)
Eligibility criteria were defined using the Population–Concept–Context (PCC) framework recommended by the JBI for scoping reviews.
2.3.1. Population
The population included frontline healthcare providers involved in the delivery of emergency care services. Eligible participants included nurses, clinical officers, physicians, emergency medical personnel, and other healthcare workers involved in acute care management. Studies involving multidisciplinary teams or health professional trainees were also included if the intervention directly addressed emergency care competencies.
2.3.2. Concept
The central concept examined in this review was the implementation of the WHO Basic Emergency Care (BEC) course and closely related interventions explicitly based on or adapted from the WHO/ICRC BEC toolkit. Broader emergency care training programmes were not included unless they directly incorporated BEC content or were clearly described as BEC-related implementation interventions. Eligible interventions were required to include structured educational components such as didactic instruction, simulation-based training, case-based learning, or clinical mentorship.
Studies were included only if they provided sufficient methodological detail to describe the intervention components, including curriculum content, delivery methods, and training duration, consistent with best practices for intervention reporting.
2.3.3. Context
The review focused on studies conducted in sub-Saharan Africa, a region where emergency care systems are undergoing rapid development but where access to specialized emergency medicine training remains limited. Both urban and rural healthcare settings were included, including district hospitals, regional referral hospitals, and primary health facilities providing emergency services.
2.4. Information Sources and Search Strategy
A comprehensive search strategy was developed in collaboration with a health sciences librarian to maximize sensitivity and reproducibility. Electronic databases searched included: PubMed/MEDLINE, CINAHL (Cumulative Index to Nursing and Allied Health Literature), Web of Science and Scopus. The search was performed between September -December 2024. The most recent search was conducted on 30 March 2026. The protocol is registered at the Open Science Framework (OSF) Registries 10.17605/OSF.IO/PVE7J.
Search terms combined controlled vocabulary (MeSH terms) and free-text keywords related to emergency care training, health workforce capacity building, and sub-Saharan Africa. No historical or language restrictions were applied. Boolean operators (AND, OR) were used to combine search concepts, and truncation was applied to capture variations of key terms.
An example search strategy used in PubMed included:
(“Basic Emergency Care” OR BEC) AND (“course” OR training OR program) AND (implementation OR evaluation OR impact OR outcomes OR effectiveness) AND (sub–Saharan Africa OR Africa OR LMIC OR “low income” OR “middle income” OR “resource limited” OR “clinical training”).
In addition to database searches, grey literature sources were examined to identify relevant reports, technical documents, and non-indexed studies related to BEC implementation in sub-Saharan Africa. These included WHO reports, conference proceedings, institutional repositories, and online dissertations. Stakeholder consultation with emergency care experts was also used to identify additional publications not indexed in major academic databases.
2.5. Study Selection
All retrieved records were imported into a reference management software program for deduplication and screening. Titles and abstracts were independently screened by two reviewers using predefined eligibility criteria. Studies that met the inclusion criteria or required further assessment were subjected to full-text review.
Disagreements between reviewers (PM, RN and SIT) were resolved through discussion and consensus. In cases where consensus could not be reached, a fourth reviewer was consulted to adjudicate the final decision.
2.6. Data Charting
Data from eligible studies were extracted using a standardized data charting form designed according to the Template for Intervention Description and Replication (TIDieR) checklist [20]. Data extraction was undertaken by five reviewers, and the extracted data were cross-checked by two independent reviewers to ensure consistency and accuracy. The extracted variables included study characteristics (authors, year, country, and study design), healthcare setting and facility type, participant characteristics and healthcare worker cadre, intervention description and curriculum content, mode of delivery (e.g., in-person training, simulation, blended learning), duration and frequency of training sessions, and evaluation methods and outcome measures. Any discrepancies in extracted data were resolved through discussion among the review team.
2.7. Assessment of Implementation Outcomes
Implementation outcomes were assessed using the framework proposed by Proctor et al. [21], which is widely applied in implementation science research. This framework evaluates the performance of interventions across multiple operational dimensions. The following implementation outcomes were examined where reported Acceptability, Feasibility Appropriateness, Adoption, Fidelity, Cost, Penetration, and Sustainability.
2.8. Data Analysis and Synthesis
Quantitative data were summarized using descriptive statistical methods, including frequencies and proportions describing training outcomes, knowledge improvements, and implementation indicators. Where pre- and post-training assessments were reported, changes in participant knowledge or clinical competencies were documented.
Qualitative data describing implementation barriers, facilitators, and contextual factors were analyzed using thematic synthesis, allowing the identification of cross-cutting patterns across studies. Themes were categorized according to health system domains, including workforce capacity, infrastructure limitations, and institutional support.
To ensure methodological reliability, the search strategy was independently replicated by an information specialist, and extracted data were cross-checked by two independent reviewers (MGT and DB). In addition, reported implementation outcomes were mapped to Proctor’s framework, while qualitative findings were synthesised according to broader health systems strengthening domains. No formal methodological quality assessment or risk-of-bias appraisal was conducted, as this review aimed to map the breadth and characteristics of the evidence in line with scoping review methodology.
The PRISMA flow diagram is presented in Figure 1, and the PRISMA-ScR checklist is provided in Supplementary Table S1.
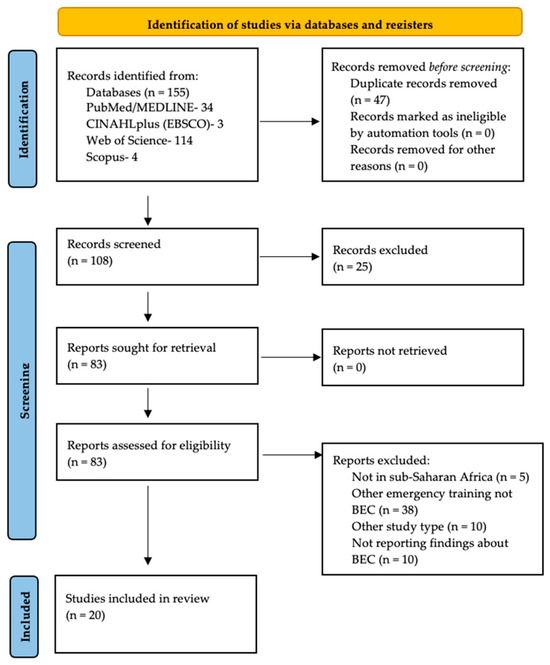
Figure 1.
PRISMA flow diagram.
3. Results
3.1. Study Characteristics
The review included 20 studies conducted in Uganda, Tanzania, Malawi, Rwanda, South Africa, Zambia, Sierra Leone, Cameroon, Djibouti, Liberia, Nigeria, Kenya and Somalia [5,11,12,13,14,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36]. Most studies employed mixed methods, combining pre- and post-course assessments with qualitative evaluations of participants’ experiences. Sample sizes ranged from 20 to over 3500 healthcare workers, including nurses, clinical officers, and physicians. The study characteristics are presented in Table 1.

Table 1.
Characteristics of studies included in the review.
Applying the analytical framework, findings were synthesised across two linked dimensions: reported implementation outcomes, including acceptability, feasibility, appropriateness, adoption, fidelity, cost, penetration, and sustainability; and broader health systems themes related to uptake, barriers and facilitators, capacity building, implementation strategies, and policy implications. Ten (10) studies reported implementation outcomes including acceptability [22,23,24,28,32,33], feasibility [24,25,28,30], appropriateness [23,28,33,34], adoption [25,32] and only one reported on cost [35].
3.2. Facilitators for the Uptake of Emergency Care Training by Health Workers
3.2.1. Mentorship and Post-Course Support
One recurring strong facilitator was ongoing support after the initial course. In Malawi, participants and mentors identified supportive mentorship as a key enabler of continued use of emergency skills; mentors helped clarify missed concepts, sharpen skills, provide reminders during emergencies, and create more time for practice [28]. The same study also found that the BEC course plus follow-up longitudinal mentorship was feasible and acceptable, and likely important for longer-term retention of knowledge and skills. Related evidence from Liberia suggests that implementation support may be strengthened when BEC-based training is accompanied by clinical mentorship embedded within routine care delivery, allowing providers to apply knowledge with guided support in practice [24]. These studies suggest that mentorship and structured post-course support are more than optional add-ons, as they appear to be among the clearest facilitators of sustained BEC uptake in practice.
3.2.2. Good Instructors and Hands-On Teaching
Several papers point to the importance of how BEC is delivered, not just what is taught. In the Malawi study, participants said the instructors’ teaching style, openness, and encouragement made them feel comfortable asking questions and engaging with the course, while hands-on skills sessions made emergency skills more usable in real care [28]. In the Cameroon multi-country BEC implementation, participants gave universal praise to the quality of the training materials, the course itself, and the facilitation methodology [14]. These findings suggest that skilled facilitators, a welcoming learning environment, and practical teaching methods are major enablers of BEC uptake.
3.2.3. Perceived Relevance and Immediate Usefulness
BEC seems easier to take up when participants see it as directly relevant to their daily work. In South Africa, nurses described the course as highly useful and relevant, with themes including contextual relevance and skills update [13]. In Nigeria, the course was also reported as well received, alongside significant gains in knowledge and confidence [12]. These studies suggest that uptake is facilitated when staff quickly recognize that the content matches the realities of frontline care and helps them manage emergencies more confidently.
3.2.4. Training-of-Trainers and Cascade Models
Scalability itself emerged as a facilitator. By training local health workers to deliver the course within their facilities, training-of-trainers and locally led delivery models enabled rapid scale-up, built local ownership, and supported sustainable emergency care capacity. In the WHO pilot across Uganda, Tanzania, and Zambia, the BEC course was taught by local instructors after a structured training-of-trainers process, suggesting that the course can be successfully transferred to local teaching teams [33]. In Uganda, a cascade training model enabled knowledge to spread far beyond the original trainee group. The 511 trainers went on to train 3,550 healthcare workers, which the authors describe as an efficient and replicable approach in low-resource settings [34]. Similarly, the Cameroon BEC study reported that after a 1-day training-of-trainers component, provisional trainers were able to expand the training within their own regions [14]. These findings suggest that BEC uptake is supported when programmes deliberately build local trainer capacity rather than relying only on external faculty.
3.2.5. User-Centred and Supported Digital Implementation
For digital BEC tools, uptake was facilitated by stakeholder involvement and hands-on support during implementation. The Lean software paper describes the BEC app work as using Lean development with maximal stakeholder involvement to improve acceptance [11]. In Tanzania, the companion app study found that most users could not adopt the app independently, but 63% were able to download and use it successfully with moderator support, and the authors recommended future roll-out models based on super users and peer support [5]. Similar lessons were reported in the mixed-methods study of the BEC mobile application adjunct, which showed that successful use depended not only on the tool itself, but also on implementation support and user engagement strategies [32]. Taken together, these findings suggest that for digital BEC uptake, the key facilitators were not technology alone, but co-design, user support, and socially supported implementation.
3.3. Barriers to the Uptake of Emergency Care Training by Health Workers
3.3.1. Health System and Organisational Constraints
A major barrier to the uptake of emergency care training among health workers is the broader fragility of emergency care systems. Across the literature, participation in training is constrained in settings where facilities lack standardised emergency unit protocols, essential equipment and medicines, an adequate cadre of dedicated emergency care staff, and sufficient institutional recognition of emergency care as a distinct service area [34]. In such contexts, health workers are often required to balance training attendance with ongoing clinical responsibilities in already understaffed units, limiting both participation and the practical application of newly acquired skills. Weak system support may also reduce opportunities for post-training reinforcement, supervision, and integration of learning into routine practice. Related evidence from Liberia suggests that these barriers may be less restrictive when BEC-informed training is implemented as part of a broader emergency care strengthening intervention rather than as a stand-alone educational activity [24].
3.3.2. Staffing Shortages and Competing Workload Demands
Health workers often struggle to take up training because of heavy workloads, staff shortages, and the practical difficulty of being released from clinical duties. This is especially pronounced in low-resource settings where a small number of nurses or clinicians cover large patient volumes. During outbreaks and other high-pressure periods, training time becomes even harder to protect [34]. Time constraints, competing clinical responsibilities, and limited opportunities for refresher or follow-up support were also reported as barriers to consolidating skills after initial training [28,30]. These findings suggest that uptake is more likely to be sustained when training is designed to fit local service realities, when local trainers are used, and when delivery models reduce the need to repeatedly remove large numbers of staff from clinical care.
3.3.3. Limited Technological Access and Digital Readiness
For digital or app-supported emergency care training, uptake is often constrained by simple but important access problems. In Tanzania, barriers included not owning a smartphone, lack of battery charge, limited access to data or Wi-Fi, the cost of mobile data, outdated operating systems, insufficient phone storage, inconsistent internet access, variable smartphone literacy, language discordance, and frequent phone turnover [5,11]. These findings show that even well-designed digital learning tools may not reach the intended audience unless implementation accounts for device compatibility, connectivity, cost, and user support.
3.3.4. Insufficient Post-Training Support and Mentorship
Initial course delivery alone may not be enough for sustained uptake in practice. A recurring barrier is the absence of longitudinal support after the course, which can leave staff without reinforcement, coaching, or opportunities to consolidate skills. In Malawi, participants identified the need for more mentorship, and the study found that greater mentor–mentee contact appeared to support retention of knowledge and confidence over time [28]. Evidence from Sierra Leone likewise suggests that gains in knowledge and confidence can persist beyond the immediate post-course period, but that ongoing reinforcement is important if these benefits are to be sustained in practice [30]. These findings suggest that uptake is not only about attending the training once, but also about whether health workers receive enough post-course support to continue applying what they have learned.
3.3.5. Learner Preparedness, Language, and Confidence
Uptake can also be reduced by differences in language proficiency, digital literacy, and baseline preparedness. In the app implementation study, variable English proficiency and smartphone literacy affected use of the training adjunct [5]. More broadly, variation in prior training and professional background may influence how readily participants engage with BEC content, with some evidence that learning gains and retention differ across cadres [29]. This suggests that a single delivery format may not be equally accessible to all participants, and that successful uptake depends partly on how well training is adapted to differing learner needs.
3.4. Capacity-Building and Implementation Approaches
3.4.1. Short-Course and BEC-Based Training Models
Capacity building for emergency care health workers was commonly delivered through short, practice-oriented training tailored to frontline providers. Across several settings, the WHO Basic Emergency Care (BEC) course emerged as a central model for strengthening emergency care knowledge, confidence, and practical competence among frontline health workers, including nurses, clinical officers, and [12,13,14,22,23,33]. These findings suggest that short, structured, and practical emergency care courses remain an important mechanism for frontline workforce development in low-resource settings.
3.4.2. Contextual Adaptation and Stakeholder Engagement
A consistent implementation approach across studies was the adaptation of training to local health system needs, workforce roles, and resource constraints. In Nigeria and Cameroon, BEC was implemented through collaboration with local institutions and aligned with the realities of frontline practice, improving feasibility and acceptability [12,14]. In Liberia, application of the WHO Basic Emergency Care toolkit within a low-resource referral hospital further illustrates how BEC-informed training can be tailored to local service structures and clinical priorities [24]. Similar cadre-specific adaptation was seen in Tanzania, where the BEC course was introduced specifically for nurses in a tertiary hospital setting [22]. These studies suggest that emergency care training was more effective when implemented as a context-sensitive model rather than as a uniform package.
3.4.3. Mentorship and Longitudinal Reinforcement
In several settings, capacity building extended beyond one-off course delivery to include ongoing mentorship and post-course reinforcement. In Malawi, the combination of the BEC course with longitudinal mentorship was found to be feasible and acceptable and appeared to support retention of emergency care knowledge and confidence over time [28]. This suggests that mentorship was not simply an added feature, but an implementation approach intended to support continued knowledge use and translation into practice, particularly in rural or resource-constrained settings.
3.4.4. Cascade and Training-of-Trainers Approaches
Cascade training and training-of-trainers approaches were also used to widen emergency care capacity while reducing dependence on external faculty. In Uganda, a cascade training model implemented during the COVID-19 outbreak expanded emergency care capacity across many healthcare workers, demonstrating the potential of progressive knowledge transfer through locally engaged trainers [34]. Similar approaches were reported in the WHO BEC pilot across Uganda, Tanzania, and Zambia, where the course was delivered by local instructors following a structured training-of-trainers process [33]. In Cameroon, the BEC study also reported that a one-day training-of-trainers component enabled provisional trainers to expand delivery within their own regions [14]. Together, these findings suggest that locally anchored trainer models are important for both scalability and sustainability.
3.4.5. Digital and Blended Learning Approaches
Digital and blended learning tools were used as supportive approaches to reinforce BEC content and extend learning beyond face-to-face training. In Tanzania, the BEC Companion App was introduced to support continued engagement with emergency care content, while a related study showed that lean software methods improved acceptance and usability [5,11]. In Uganda, pre-course online cases were used to supplement the BEC course and enhance preparedness before in-person delivery [25]. These studies suggest that digital tools were most often used as adjuncts to reinforce and extend training rather than as stand-alone replacements.
3.4.6. Integration Within Broader Emergency Care Development
Some studies positioned BEC and related emergency care training within broader efforts to strengthen emergency care systems and workforce development. In Liberia, implementation of a comprehensive emergency care curriculum based on the WHO Basic Emergency Care toolkit was embedded within wider emergency unit strengthening and clinical mentorship [24]. In Uganda, emergency care training was also implemented as part of a wider workforce capacity-building response during the COVID-19 outbreak, illustrating how BEC-related approaches can be integrated into broader system needs [34]. This framing positions capacity building not simply as course delivery, but as part of wider service development and workforce strengthening.
3.5. Impact of Basic Emergency Care Training
3.5.1. Immediate Gains in Emergency Care Knowledge
Across the available BEC studies, the most consistently reported impact was improved emergency care knowledge immediately after training. In Nigeria, the average test score increased from 73.0% pre-training to 86.5% post-training (p < 0.001), indicating substantial short-term knowledge gain among frontline providers [12]. In South Africa, knowledge scores among 86 nurses in Gauteng primary health care facilities increased from 55.1% to 78.8% following the course [13]. In Cameroon, in a French-language BEC and training-of-trainers initiative involving participants from five Francophone countries, the median score rose from 72% pre-course to 88% post-course (p < 0.001) [14]. Similar immediate improvements in knowledge were also reported in the multicountry WHO BEC pilot conducted in Uganda, Tanzania, and Zambia [33]. Overall, the evidence indicates that BEC is consistently associated with short-term improvements in emergency care knowledge across diverse sub-Saharan African settings.
3.5.2. Improved Confidence and Perceived Competence
BEC training was also associated with improved confidence in managing emergency presentations. In Nigeria, participants reported significantly increased confidence across selected emergency care knowledge and skill areas following the course [12]. In South Africa, self-perceived competence and confidence improved from 2.72 to 3.54 after training, indicating gains not only in knowledge but also in participants’ perceived ability to respond to emergencies [13]. In Cameroon, participants’ self-confidence in handling acute care scenarios reportedly doubled after the course [14]. Similar improvements in confidence were also reported in the multicountry WHO BEC pilot conducted in Uganda, Tanzania, and Zambia [33]. Overall, these findings indicate that BEC is associated with short-term improvements in confidence and perceived competence, although most evidence comes from immediate post-course assessments and provides limited insight into whether these gains are sustained over time.
3.5.3. Sustained Benefit When Paired with Mentorship
Evidence from Malawi suggests that the impact of BEC may extend beyond the immediate post-course period when training is reinforced through longitudinal mentorship. In rural Neno District, the median improvement in examination score from pre-course to immediate post-course testing was 18.0 percentage points (95% CI 14.0–22.0; p < 0.001). Although scores declined at one year, they remained above baseline, with a median difference of 11.9 percentage points (95% CI 4.0–16.0; p = 0.009). The study also documented 174 mentorship activities, and greater mentor–mentee contact appeared to support continued knowledge retention [28]. This indicates that structured post-training support may help sustain gains over time, although the available evidence remains limited.
3.5.4. Positive Impact Across Multiple Country Contexts
Multicountry evidence also supports the role of BEC as a scalable training approach. In a WHO pilot conducted in Uganda, Tanzania, and Zambia, post-course test scores improved significantly compared with pre-course scores (p < 0.05), and participants also reported increased confidence in managing emergency conditions [33]. These findings indicate that a low-fidelity, openly available course taught by local instructors can support short-term knowledge transfer across different health system contexts. However, the available evidence remains largely limited to immediate educational outcomes, with little data on longer-term clinical application, patient-level outcomes, or mortality reduction. The broader impact of BEC is also shaped by contextual health system factors, including weak triage systems, shortages of essential equipment and medicines, limited staffing, and wider organisational constraints, all of which may reduce the translation of training gains into routine clinical practice [24]. BEC therefore appears to be a promising capacity-building intervention, but its potential to improve patient outcomes is likely to depend on parallel investments in emergency care systems, service organisation, and facility readiness.
4. Discussion
The review suggests that effective, sustainable BEC implementation depends on more than course delivery alone. Uptake appears strongest when training is locally owned and adapted to service realities, workforce roles, and resource constraints. Early engagement of local clinical leaders, use of locally relevant emergency-nursing frameworks, and needs-based tailoring may improve fit and acceptability [37,38,39]. Sustained benefit also appears more likely when training is reinforced through mentorship, coaching, or refresher activities, particularly where opportunities to practise emergency skills are limited [28,30]. Practical teaching, locally owned trainer models, and supported digital adjuncts may further strengthen uptake and scale-up [5,11,14,32,33,34]. Even so, these patterns should be interpreted cautiously, given the marked heterogeneity of the included studies in setting, cadre, sample size, delivery model, and degree of adaptation.
Viewed through Proctor’s implementation outcomes framework, the BEC literature is concentrated on feasibility, acceptability, and immediate educational effects, with much less evidence on fidelity, penetration, sustainability, or cost. Uganda’s cascade model and Rwanda’s hybrid delivery approach suggest possible routes to scale [34,36], while Malawi and Sierra Leone provide limited evidence that reinforcement may support maintenance over time [28,30]. Cost was rarely assessed; the only economic analysis came from Uganda and evaluated a broader WHO emergency care toolkit rather than BEC alone [35]. Overall, future evaluations would benefit from applying implementation frameworks prospectively and from reporting fidelity, reach, sustainability, and cost alongside provider- and patient-level outcomes.
Within the included studies, uptake was shaped by interrelated system, workforce, and learner-level constraints. Staffing shortages, workload pressures, limited supervision, weak triage and referral processes, and shortages of basic equipment and medicines all appeared to limit both participation in training and the translation of learning into practice [12,24,34]. These findings suggest that training alone is unlikely to shift practice where emergency care remains weakly organised or under-resourced. The broader Tanzanian literature and the WHO emergency-care policy framework reinforce this point: emergency-care gains are more likely to be sustained when workforce development is linked to service organisation, governance, referral pathways, and financing [4,40]. Emergency care therefore seems better viewed as a service area requiring policy and organisational support, rather than as a facility-level training issue alone.
Digital adjuncts may extend access, but the available studies show that uptake is constrained by device access, connectivity, data cost, language, and digital literacy [5,11]. This suggests that digital tools are most likely to be useful when introduced as supported adjuncts rather than stand-alone replacements. Offline-first design, simplified onboarding, and peer or moderator support may be more realistic than assuming independent app uptake, although the evidence for longer-term effectiveness remains limited. Related work from Tanzania and Uganda also suggests that short-course and blended approaches are more likely to be useful when adapted to local clinical realities and linked to broader emergency-care development [4,25,37].
Across the included studies, BEC was most consistently associated with short-term gains in knowledge, confidence, and perceived competence. These gains were reported in Nigeria, South Africa, Cameroon, and the multicountry WHO pilot, and in some settings appeared more durable when mentorship or follow-up support was provided [12,13,14,24,28,30,33]. However, most studies assessed outcomes immediately after training, and evidence for longer-term practice change, patient benefit, or mortality reduction remained sparse. Educational gains should therefore not be treated as equivalent to system-level impact. Translation into routine care is likely to depend on staffing, supervision, triage, referral pathways, and access to basic emergency-care resources. More robust longitudinal and patient-centred evaluations are still needed before stronger conclusions can be drawn about sustained clinical impact.
Based on the available evidence, BEC implementation may be better supported when it is aligned with broader emergency care strengthening rather than delivered as a stand-alone training course. Across settings, uptake and implementation appeared more favourable when delivery was adapted to local contexts, reinforced through mentorship or follow-up support, and, in some cases, expanded through local trainer or cascade models. Digital tools may also help reinforce learning, but the included studies suggest that they are most useful as supported adjuncts rather than replacements for face-to-face training. Given the predominance of short-term educational outcomes and the limited evidence on longer-term practice and patient-level effects, these recommendations should be interpreted cautiously. Future work would benefit from longer follow-up and closer evaluation of how BEC is sustained and applied in routine care.
5. Conclusions
Across the included studies, BEC was consistently associated with short-term improvements in emergency care knowledge, confidence, and perceived competence among frontline health workers. Some studies further suggested that these gains may be better sustained when training is reinforced through mentorship or follow-up support. Uptake and implementation appeared to be facilitated by local adaptation, local trainer models, practical teaching approaches, and supported digital tools, while staffing shortages, workload pressures, weak system support, limited technology access, and insufficient post-course reinforcement were reported as important barriers.
Overall, the included studies suggest that BEC is a feasible and potentially useful approach to frontline emergency care capacity building in sub-Saharan Africa. However, the evidence base remains relatively small and heterogeneous, and most reported outcomes were short-term and educational in nature. Evidence on sustained practice change, patient-level outcomes, and mortality reduction was limited, so the findings should be interpreted cautiously and as context-dependent rather than uniformly generalisable.
Supplementary Materials
The following supporting information can be downloaded at: https://www.mdpi.com/article/10.3390/ecm3020017/s1, Table S1: Preferred Reporting Items for Systematic reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR) Checklist.
Author Contributions
Conceptualization, P.M. and S.I.T.; methodology, M.G.T. and R.N.; validation, M.G.T. and D.B.; formal analysis, P.M., R.N., A.K., I.N. and L.K.K.; data curation, P.M., S.I.T. and R.N.; writing—original draft preparation, P.M., G.N., R.N.N., M.G.T., D.B. and R.N.; writing—review and editing, S.I.T., A.K., I.N., L.K.K. and T.D.N.; visualization, R.N.N. and G.N.; supervision, T.D.N.; project administration, P.M., R.N. and S.I.T. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Data Availability Statement
No new data were created or analyzed in this study. Data sharing is not applicable to this article.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| AFEM | African Federation for Emergency Medicine |
| BEC | Basic Emergency Care Course |
| ICRC | International Committee of the Red Cross |
| IFEM | International Federation for Emergency Medicine |
| PCC | Population–Concept–Context |
| PRISMA-ScR | Preferred Reporting Items for Systematic Reviews and Meta-Analyses Extension for Scoping Reviews |
| TIDieR | Template for Intervention Description and Replication |
| ToT | Training of Trainers |
| WHO | World Health Organization |
References
- Alayande, B.; Chu, K.M.; Jumbam, D.T.; Kimto, O.E.; Musa Danladi, G.; Niyukuri, A.; Anderson, G.A.; El-Gabri, D.; Miranda, E.; Taye, M.; et al. Disparities in Access to Trauma Care in Sub-Saharan Africa: A Narrative Review. Curr. Trauma Rep. 2022, 8, 66–94. [Google Scholar] [CrossRef]
- Kannan, V.C.; Tenner, A.; Sawe, H.R.; Osiro, M.; Kyobe, T.; Nahayo, E.; Rasamimanana, N.G.; Kivlehan, S.; Moresky, R. Emergency care systems in Africa: A focus on quality. Afr. J. Emerg. Med. 2020, 10, S65–S72. [Google Scholar] [CrossRef]
- Bergquist, H.B.; Burkholder, T.W.; Muhammad Ali, O.A.; Omer, Y.; Wallis, L.A. Considerations for service delivery for emergency care in low resource settings. Afr. J. Emerg. Med. 2020, 10, S7–S11. [Google Scholar] [CrossRef]
- Reynolds, T.A.; Mfinanga, J.A.; Sawe, H.R.; Runyon, M.S.; Mwafongo, V. Emergency care capacity in Africa: A clinical and educational initiative in Tanzania. J. Public Health Policy 2012, 33, S126–S137. [Google Scholar] [CrossRef]
- Greenberg, A.L.; Rose, C.C.; Nicholaus, P.; Mfinanga, J.A.; Sawe, H.R.; Tenner, A.G. Reaching further: Lessons from the implementation of the WHO Basic Emergency Care Course Companion App in Tanzania. Afr. J. Emerg. Med. 2021, 11, 325–330. [Google Scholar] [CrossRef] [PubMed]
- Shanahan, T.; Risko, N.; Razzak, J.; Bhutta, Z. Aligning emergency care with global health priorities. Int. J. Emerg. Med. 2018, 11, 52. [Google Scholar] [CrossRef] [PubMed]
- Buowari, D.Y.; Owoo, C.; Gupta, L.; Schell, C.O.; Baker, T. Essential Emergency and Critical Care: A Priority for Health Systems Globally. Crit. Care Clin. 2022, 38, 639–656. [Google Scholar] [CrossRef] [PubMed]
- WHO/ICRC. Basic Emergency Care: Approach to the Acutely Ill and Injured; WHO: Geneva, Switzerland, 2018; Available online: https://iris.who.int/server/api/core/bitstreams/63432b9f-8808-44c5-9692-cea717c0cbda/content (accessed on 10 October 2024).
- King, C.; Dube, A.; Zadutsa, B.; Banda, L.; Langton, J.; Desmond, N.; Lufesi, N.; Makwenda, C.; Hildenwall, H. Paediatric Emergency Triage, Assessment and Treatment (ETAT)-preparedness for implementation at primary care facilities in Malawi. Glob. Health Action 2021, 14, 1989807. [Google Scholar] [CrossRef]
- Trauma AcoSCo. Advanced Trauma Life Support Program for Doctors: ATLS; American College of Surgeons: Chicago, IL, USA, 1997. [Google Scholar]
- Rose, C.; Nichols, T.; Hackner, D.; Chang, J.; Straube, S.; Jooste, W.; Sawe, H.; Tenner, A. Utilizing Lean Software Methods To Improve Acceptance of Global eHealth Initiatives: Results From the Implementation of the Basic Emergency Care App. JMIR Form. Res. 2021, 5, e14851. [Google Scholar] [CrossRef]
- Olufadeji, A.; Usoro, A.; Akubueze, C.E.; Aiwonodagbon, B.O.; Strong, J.; Kivlehan, S.M.; Akodu, B. Results from the implementation of the World Health Organization Basic Emergency Care Course in Lagos, Nigeria. Afr. J. Emerg. Med. 2021, 11, 231–236. [Google Scholar] [CrossRef]
- Botes, M.; King, L.L.; Holliman, R.; de Lange, S.; Tumusiime, S.I.; Kutoane, M.; Quiroga, D.; Brysiewicz, P. Impact of the WHO/ICRC Basic Emergency Care (BEC) course on nurses’ knowledge, confidence, and competence in Primary Health Care facilities in Gauteng, South Africa. Afr. J. Emerg. Med. 2025, 15, 100890. [Google Scholar] [CrossRef]
- Kouomogne, B.A.N.; Tania, B.L.; Ndongo, C.B.; Noulala, A.C.; Ntembwa, H.K.; Kariyo, P.C.; Pouth, B.B.; Epee, D.; Joss, B.L.; Nteungue, B.B.K.; et al. Improving emergency care capacity with the WHO-ICRC Basic Emergency Care (BEC) course. Afr. J. Emerg. Med. 2025, 15, 100892. [Google Scholar] [CrossRef]
- Kivlehan, S.M.; Dixon, J.; Kalanzi, J.; Sawe, H.R.; Chien, E.; Robert, J.; Wallis, L.; Reynolds, T.A. Strengthening emergency care knowledge and skills in Uganda and Tanzania with the WHO-ICRC Basic Emergency Care Course. Emerg. Med. J. 2021, 38, 636–642. [Google Scholar] [CrossRef]
- Peters, M.; Godfrey, C.; McInerney, P.; Soares, C.B.; Khalil, H.; Parker, D. Methodology for JBI scoping reviews. In The Joanna Briggs Institute Reviewers Manual 2015; Joanna Briggs Institute: Adelaide, Australia, 2015. [Google Scholar]
- Arksey, H.; O’Malley, L. Scoping studies: Towards a methodological framework. Int. J. Soc. Res. Methodol. 2005, 8, 19–32. [Google Scholar] [CrossRef]
- Levac, D.; Colquhoun, H.; O’Brien, K.K. Scoping studies: Advancing the methodology. Implement. Sci. 2010, 5, 69. [Google Scholar] [CrossRef]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef] [PubMed]
- Hoffmann, T.C.; Glasziou, P.P.; Boutron, I.; Milne, R.; Perera, R.; Moher, D.; Altman, D.G.; Barbour, V.; Macdonald, H.; Johnston, M. Better reporting of interventions: Template for intervention description and replication (TIDieR) checklist and guide. BMJ (Clin. Res. Ed) 2014, 348, g1687. [Google Scholar] [CrossRef] [PubMed]
- Proctor, E.; Silmere, H.; Raghavan, R.; Hovmand, P.; Aarons, G.; Bunger, A.; Griffey, R.; Hensley, M. Outcomes for Implementation Research: Conceptual Distinctions, Measurement Challenges, and Research Agenda. Adm. Policy Ment. Health Ment. Health Serv. Res. 2011, 38, 65–76. [Google Scholar] [CrossRef]
- Avrith, N.; Suh, Y.; Sunderwirth, R.; Suleman, S.; Akrabi, A.M. Introduction of WHO BEC course for nurses at Bugando Medical Center in Mwanza, Tanzania. Afr. J. Emerg. Med. 2023, 13, 274–280. [Google Scholar] [CrossRef] [PubMed]
- Broccoli, M.C.; Dixon, J.; Skarpiak, B.; Phiri, G.; Muck, A.E.; Hynes, E.J.C. Application of the World Health Organization’s Basic Emergency Care course in Zambia. Afr. J. Emerg. Med. 2021, 11, 140–143. [Google Scholar] [CrossRef]
- Epps, L.; Ramachandran, A.; Yi, S.; Mayah, A.; Burkholder, T.; Jaung, M.; Haider, A.; Wesseh, P.; Shakpeh, J.; Bills, C.; et al. Implementation and outcomes of a comprehensive emergency care curriculum at a low-resource referral hospital in Liberia: A novel approach to application of the WHO Basic Emergency Care toolkit. PLoS ONE 2023, 18, e0282690. [Google Scholar] [CrossRef] [PubMed]
- Friedman, A.; Wallis, L.A.; Bullick, J.C.; Cunningham, C.; Kalanzi, J.; Kavuma, P.; Osiro, M.; Straube, S.; Tenner, A.G. Pre-course online cases for the world health organization’s basic emergency care course in Uganda: A mixed methods analysis. Afr. J. Emerg. Med. 2022, 12, 148–153. [Google Scholar] [CrossRef]
- Ismail, B.M.; Ali, M.M.; Sydlowski, M.M.; Hussein, M.; Michaeli, N. Implementing the WHO/ICRC Basic Emergency Care course training for health workers in conflict-affected regions in Somalia. Afr. J. Emerg. Med. 2026, 16, 100965. [Google Scholar] [CrossRef]
- Kadakia, N.; Shakya, I.; Lee, J.; Kharel, R.; Diaz, M.; Mugemangago, P.; Ndebwanimana, V.; Karim, N. Implementation and Evaluation of the WHO Basic Emergency Care Course in Rwanda. Prehospital Disaster Med. 2023, 38, s19–s20. [Google Scholar] [CrossRef]
- Khongo, B.D.; Schmiedeknecht, K.; Aron, M.B.; Nyangulu, P.N.; Mazengera, W.; Ndarama, E.; Tenner, A.G.; Baltzell, K.; Connolly, E. Basic emergency care course and longitudinal mentorship completed in a rural Neno District, Malawi: A feasibility, acceptability, and impact study. PLoS ONE 2023, 18, e0280454. [Google Scholar] [CrossRef]
- Michaeli, N.; Beck, A.; De Luca, G.; Gitau, M.; Lubetkin, D.; Ochieng, D.; Wanjiku, G.W.; Myers, J.G. A prospective, longitudinal, comparative analysis of the World Health Organization/International Committee of the Red Cross Basic Emergency Care Course on emergency medicine knowledge and confidence among recent medical school graduates. Int. J. Emerg. Med. 2025, 18, 8. [Google Scholar] [CrossRef]
- Sonenthal, P.D.; Kachimanga, C.; Komba, D.; Bangura, M.; Ludmer, N.; Lado, M.; Patino, M.; Gerrard, R.B.; Vandy, M.J.; Marsh, R.H.; et al. Applying the WHO-ICRC BEC course to train emergency and inpatient healthcare workers in Sierra Leone early in the COVID-19 outbreak. BMC Health Serv. Res. 2022, 22, 197. [Google Scholar] [CrossRef]
- Straube, S.; Chang-Bullick, J.; Nicholaus, P.; Mfinanga, J.; Rose, C.; Nichols, T.; Hackner, D.; Murphy, S.; Sawe, H.; Tenner, A. Novel educational adjuncts for the World Health Organization Basic Emergency Care Course: A prospective cohort study. Afr. J. Emerg. Med. 2020, 10, 30–34. [Google Scholar] [CrossRef]
- Tenner, A.G.; Greenberg, A.L.; Nicholaus, P.; Rose, C.C.; Addo, N.; Shari, C.R.; Friedman, A.; George, U.N.; Losak, M.J.; Mfinanga, J.A.; et al. Mobile application adjunct to the WHO basic emergency care course: A mixed methods study. BMJ Open 2022, 12, e056763. [Google Scholar] [CrossRef] [PubMed]
- Tenner, A.G.; Sawe, H.R.; Amato, S.; Kalanzi, J.; Kafwamfwa, M.; Geduld, H.; Roddie, N.; Reynolds, T.A. Results from a World Health Organization pilot of the Basic Emergency Care Course in Sub Saharan Africa. PLoS ONE 2019, 14, e0224257. [Google Scholar] [CrossRef] [PubMed]
- Wasukira, S.B.; Kambugu, C.T.; Nanyondo, S.J.; Candia, E.; Aporu, S.E.; Ikwaru, P.; Kwagala, R.; Kwiringira, A.; Mukiibi, P.; Murungi, C.; et al. Implementation of a cascade training model to enhance emergency care capacity of healthcare workers during the COVID-19 outbreak in Uganda. Afr. J. Emerg. Med. 2025, 15, 565–570. [Google Scholar] [CrossRef] [PubMed]
- Werner, K.; Risko, N.; Kalanzi, J.; Wallis, L.A.; Reynolds, T.A. Cost-effectiveness analysis of the multi-strategy WHO emergency care toolkit in regional referral hospitals in Uganda. PLoS ONE 2022, 17, e0279074. [Google Scholar] [CrossRef] [PubMed]
- WHO. Hybrid Learning to Scale Up Delivery of Basic Emergency Care Training in Rwanda. 2024. Available online: https://www.who.int/news/item/09-10-2024-hybrid-learning-to-scale-up-delivery-of-basic-emergency-care-training-in-rwanda (accessed on 30 December 2024).
- Cunningham, C.; Brysiewicz, P.; Sepeku, A.; White, L.; Murray, B.; Lobue, N.; Sawe, H. Developing an emergency nursing short course in Tanzania. Afr. J. Emerg. Med. 2017, 7, 147–150. [Google Scholar] [CrossRef]
- Karim, N.; Nyinawankusi, J.D.; Belsky, M.S.; Mugemangango, P.; Mutabazi, Z.; Gonzalez Marques, C.; Zhang, A.Y.; Baird, J.; Marie Uwitonze, J.; Levine, A.C. Needs Assessment and Tailored Training Pilot for Emergency Care Clinicians in the Prehospital Setting in Rwanda. West. J. Emerg. Med. 2025, 26, 103–110. [Google Scholar] [CrossRef]
- Scott, T.; Brysiewicz, P. African emergency nursing curriculum: Development of a curriculum model. Int. Emerg. Nurs. 2016, 27, 60–63. [Google Scholar] [CrossRef] [PubMed]
- WHO. Emergency care systems for universal health coverage: Ensuring timely care for the acutely ill and injured. In Seventy-Second World Health Assembly, Geneva 28; WHA72 R: 16; WHO: Geneva, Switzerland, 2019; Available online: https://apps.who.int/gb/ebwha/pdf_files/wha72/a72_r16-en.pdf (accessed on 15 September 2024).

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license.