Abstract
Background: The influence of digital media on public perception of sexual health is significant and relates to its effects on knowledge, attitudes, and behaviors. Motion graphics and animation represent a novel innovation in health-related communication. The visual attractiveness and adaptability to cultural issues offer an alternative means of conveying often sensitive issues. This systematic review aimed to provide an overview of their efficacy in delivering sexual health messages and to identify the components contributing to success. Methods: A literature search was conducted using Scopus, MEDLINE (via PubMed), and DOAJ, covering studies from inception to 31 August 2025. All eligible studies included randomized controlled trials, quasi-experimental studies, and other evaluations, which were synthesized by outcomes related to knowledge, attitudes, behaviors, intentions, and/or psychosocial well-being. The study was pre-registered on the INPLASY platform (INPLASY202580073). Results: Eleven studies published between the years 1989 and 2025 met the inclusion criteria. The majority reported improvements in sexual health knowledge and attitudes, and several studies also demonstrated improved behaviors and psychosocial well-being. Factors that contributed to interventions that have been successful were cultural adaptation, being based on theory, and presentation over time. Conclusions: Motion graphics and animation, therefore, represent an exciting means of sexual health promotion and stigma reduction. Future studies should therefore focus on the determination of standardized formats for media presentations, the evaluation of long-term effects, and the evaluation of cost–benefit to enhance the effectiveness of media communication in health promotion.
1. Introduction
Sexual health education is a comprehensive approach that is biopsychosocial and promotes the understanding of biological, psychological, social, and reproductive health. The goal of sexual health education is to provide patients with the necessary knowledge, skills, and positive attitudes to make decisions to prevent adverse health outcomes such as sexually transmitted infections (STIs) and unintended pregnancies and promote autonomy in sexual health [,,]. Sexual health education improves health outcomes. Increases in knowledge and understanding promote protective behaviors in which individuals engage in consistent contraceptive and barrier use, thus decreasing the rates of risky sexual behaviors among adolescents [,,]. These benefits are then reflected in the lower rates of STIs (including HIV) and fewer unintended pregnancies []. Sexual health education also contributes to psychosocial health by fostering respect, communication, and consent in relationships—protective factors against sexual violence and sexual abuse [,]. Furthermore, inclusive curricula promote the acceptance of diversity and stigma reduction and are especially beneficial for lesbian, gay, bisexual, transgender, queer/questioning, and other sexual and gender minority (LGBTQ+) youth []. The benefits of sexual health education go beyond individuals and affect educational and social outcomes. Schools with sexual health education can better engage their students academically, who may be faced with fewer distractions related to sexual health or a more inclusive climate []. As beneficial as sexual health education is, barriers such as limited funding, limited teacher training, and socio-cultural resistance hinder the delivery of sexual health education worldwide [].
Considering these challenges, innovative educational media in the form of motion graphics and animated videos may be valuable tools for effectively enhancing the delivery and engagement of sexual health education. Animated video materials have been shown to considerably increase student engagement and interest in various contexts. For example, animated videos lead to improved understanding and self-directed learning among undergraduate accounting students [], as well as increased motivation and acquisition of motor skills in a physical education setting []. Animated videos are not only beneficial for student engagement but also for improved learning outcomes. Students who learned vocabulary or psychology content through animations scored higher on tests and preferred animated videos over traditional materials [,]. Additionally, animated videos can improve the comprehension of complex concepts found in areas such as machine learning and natural sciences, as there is a comprehension benefit from the visualization and memorization of abstract learning content [].
Motion graphics are a screen-based medium that creates the illusion of movement by sequencing images, often combined with text, audio, and numerous multimedia factors. As a hybrid visual communication, they provide additional clarity, engagement, and emotional depth []. Instead of a narrative focus, as seen in animations, motion graphics use animated graphic elements with low-stylized representations to convey information and concepts []. Their uses range from advertising to education and from design interfaces to digital content, and this distinct visual storytelling technique has become increasingly popular as a vehicle for communicating information and concepts []. Like motion graphics, animated videos are audiovisual productions that communicate information, ideas, and narratives through movement using animation approaches, such as hand-drawn illustrations, computer-generated imagery, or frame-by-frame production. Animated videos combine vibrant visual forms (such as drawings, models, or images) with audio elements (such as sound effects, narration, and music), not only to motivate learners but also to provide an interactive effect to aid understanding [,]. Unlike motion graphics, animated videos creatively portray concrete realities and abstract concepts, the latter of which can depict events or concepts that cannot be easily captured using video and storytelling. Animated documentaries have depicted psychological experiences, events from the past, or art that has never been recorded in audiovisual form, reestablishing the referential value of digital media.
While sexual health education has seen widespread advancement in practice, it is typically designed using conventional text-based modes of delivery or traditionally didactic approaches that do not engage learners effectively or consider sensitive topics in accessible ways. Recent evidence shows that motion graphics and animated videos can improve engagement, understanding, and retention when implemented in various educational modalities; however, the utilization of these innovations in sexual health education has yet to be systematically summarized. Individual studies have reported positive improvements in sexual health knowledge, attitudes, and protective behaviors, and even decreased risky behaviors in sexual health when using motion graphics/animated videos. However, these interventions also varied in design domains, populations, theories informing the designs, and levels of quality, making it important to conduct a review in this area. A review summarizing the current state of knowledge with respect to interventions provides information on consensus and gaps, and assists in informing future intervention designs. This systematic review examines the use of motion graphics and animated videos in sexual health education. More specifically, the review will (i) describe the features and design characteristics of these interventions; (ii) describe the educational and behavioral outcomes addressed with motion graphics and animated videos in sexual health education; and (iii) summarize the evidence of the effectiveness of motion graphics and animated videos in improving knowledge, attitudes, behaviors, and related outcomes in sexual health.
2. Materials and Methods
This systematic review adheres to PRISMA 2020 guidelines for systematic reviews [] (Supplementary File: PRISMA checklist). The review protocol was prospectively registered using the INPLASY International Platform of Registered Systematic Review and Meta-analysis Protocols (INPLASY registration number: INPLASY202580073). This study was approved by the Walailak University Ethics Committee (WUEC-25-326-01).
2.1. Eligibility Criteria
The eligibility and inclusion criteria were determined a priori. Studies were eligible if they examined a sample of any population regardless of age, sex, or setting and assessed an intervention addressing sexual or sexual health content that used motion graphics, animated videos, educational animations, digital animation, explainer videos, 2D/3D animations, or animated infographics. There were no restrictions on comparators (e.g., standard education, some other intervention, or no intervention). To be included in the review, studies were required to assess and report on at least one relevant outcome related to sexual health, specifically knowledge, awareness, attitudes, behaviors, behavioral changes, intention, uptake, or practice. Both experimental (e.g., randomized controlled trials, quasi-experimental, or pre–post studies) and other quantitative evaluation designs (e.g., observational or pilot interventions reporting measurable outcomes) were eligible for inclusion. Only the studies published in English were eligible for inclusion. If researchers could not retrieve the full text of a study through reasonable means, it was dropped from the inclusion criteria. The eligible studies were later grouped for synthesis based on intervention characteristics and reported outcome measures.
2.2. Information Sources
A literature search was performed using three major electronic databases: Scopus, MEDLINE (via PubMed), and Directory of Open Access Journals (DOAJ). The databases were searched from their inception to 31 August 2025. The reference lists of included articles were screened for additional relevant studies. The grey literature and unpublished studies were not searched in this review, as the aim was to synthesize evidence from the peer-reviewed published literature to ensure a high-quality method, reliability, and replicable study findings.
2.3. Search Strategy
A comprehensive search strategy was developed for each database, in conjunction with controlled vocabulary terms and free-text keywords. The search examined Scopus, MEDLINE (via PubMed), and DOAJ, from inception until 31 August 2025, using filters for English-language publications. The search strategy was a combination of terms related to the intervention (e.g., motion graphics, animation) and the topic (e.g., sexual health, HIV prevention, sex education), along with relevant outcomes (e.g., knowledge, attitudes, behaviors, and intention). The complete search strategy for Scopus is outlined below as an example, with similar strategies adapted for other databases.
TITLE-ABS-KEY(
(“motion graphic*” OR animation* OR “animated video*” OR “educational animation*”
OR “explainer video*” OR “digital animation*” OR “2D animation”
OR “3D animation” OR “animated infographic*”)
AND
(“sexual health” OR “sex education” OR “HIV prevention” OR “HIV education”
OR “HIV testing” OR condom* OR PrEP OR “pre-exposure prophylaxis” OR PEP
OR “post-exposure prophylaxis”)
AND
(knowledge OR awareness OR attitud* OR behav* OR “behavioral change”
OR intention* OR uptake OR practice*)
)
AND (LIMIT-TO (LANGUAGE, “English”))
2.4. Selection Process
All records identified from the database searches were imported into EndNote version 20 (Clarivate Analytics) and duplicates were removed. Title and abstract screening was conducted independently by two reviewers (NS and WT) according to the eligibility criteria stated above. The full texts of the potentially relevant articles were subsequently retrieved and independently assessed by the same reviewers. We consistently applied our eligibility criteria across both screening stages. Any conflicts regarding study selection were resolved through discussion, and if they could not be resolved, a third reviewer (DM) was consulted. No automation tools were used in the selection process.
2.5. Data Extraction and Synthesis
Two reviewers (NS and WT) independently extracted study data using a standardized extraction form. For each included publication, the data extracted included the authors and year of publication, country of the study, specific focus of the sex education topic, user characteristics, study design, details of the intervention, measures, and study findings. Educational and multimedia details of the motion graphics and animated video interventions were also extracted, including the type of animation (e.g., 2D, 3D, or mixed), duration and frequency, content focus (e.g., abstinence and contraception), delivery platform (e.g., mobile app and online video), pedagogical/educational design features (e.g., quizzes and gamification strategies), level of user interactivity, and any cultural or contextual adaptation described. Production and expertise information (i.e., who created or recommended the material) was also recorded. Data discrepancies were resolved through a discussion process involving all reviewers, and adjudication was sought from a third reviewer (DM) when reviewers could not come to a consensus. No automation tools were used, nor did we seek additional data from study authors.
Due to a marked level of methodological, clinical, and conceptual heterogeneity (across populations, settings, intervention formats, comparators, outcomes, and lengths of follow-up), a quantitative meta-analysis was not possible. Instead, we produced a narrative synthesis. Studies were first defined and grouped by the sexual health domain (knowledge, attitudes, behavioral intention, and psychosocial outcomes) and then by study design and population group (e.g., adolescents in school, university-based students, and persons living with HIV). Within each group, we compared the direction and statistical significance of effects, reported estimates of effect (when possible), and consistent effects across studies. Any contradictory or outlying effects were reported rather than statistically pooled. This strategy allowed us to report patterns of effects while concurrently accounting for heterogeneity in designs and outcomes.
2.6. Bias Assessment
The methodological quality of the included studies was evaluated according to the study design. For RCTs, the potential risk of bias was assessed using the Cochrane Risk of Bias 2 (RoB 2) tool [], which assesses the potential risk of bias in the RCT design according to five domains: randomization process, deviations from the intended intervention, missing outcome data, measurement of the outcome, and selection of the reported result. For non-randomized studies, the potential risk of bias was assessed using the Risk Of Bias In Non-randomized Studies of Interventions (ROBINS-I) tool, which has seven domains: confounding, selection of participants into the study, classification of interventions, deviation from the intended intervention, missing data, measurement of outcomes, and selection of reported results []. The risk of bias assessments were independently performed by two reviewers (NS and WT). Disagreements were resolved by discussion, and a third reviewer (DM) was consulted whenever necessary. Risk-of-bias judgments were subsequently taken into account when interpreting the direction and magnitude of effects within each outcome domain and when describing the overall strength of evidence in the Results and Discussion.
2.7. Assessment of the Strength of Evidence
Due to the limited number of studies in particular outcome domains and the high degree of design, intervention, and outcome measure heterogeneity, we did not conduct a formal Grading of Recommendations Assessment, Development and Evaluation (GRADE) rating for each outcome. Instead, we used a qualitative approach to assess evidence strength for each outcome domain (knowledge, attitudes, behavioral intention, and psychosocial well-being) by considering (i) study design (i.e., RCT versus non-randomized), (ii) overall risk-of-bias profile using RoB 2 and ROBINS-I, (iii) direction of effect (if any) was consistent, (iv) indirect nature of populations, intervention, and outcomes, and (v) precision of the reported estimates (e.g., confidence intervals, p-value, effect size if available). Given this approach, we have summarized the evidence as stronger or weaker in the Results and Discussion and not used formal categorical certainty ratings.
3. Results
Eleven studies published between 1989 and 2025 were included in this review (Table 1 and Table 2). Figure 1 illustrates the overall process flow for study selection in a PRISMA flow diagram. The studies were conducted in China (n = 5) [,,,,], the United States (n = 3) [,,], Malaysia (n = 1) [], Tanzania (n = 1) [], and Thailand (n = 1) []. The risk of bias assessment for the included studies is summarized in Table 3 and Table 4.

Table 1.
Characteristics of included studies.
Table 2.
Educational and multimedia characteristics of motion graphics and animated video interventions.
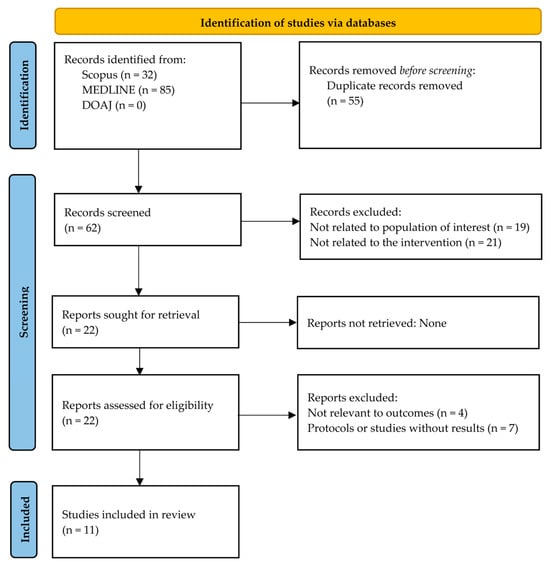
Figure 1.
PRISMA flow diagram of the study selection process. DOAJ, Directory of Open Access Journals; MEDLINE, Medical Literature Analysis and Retrieval System Online; PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Table 3.
Risk of bias assessment for randomized controlled trials using Cochrane Risk of Bias 2 tool (RoB2).
Table 4.
Risk of bias assessment for non-randomized studies of interventions using Risk Of Bias In Non-randomized Studies of Interventions (ROBINS-I).
Interventions addressed a range of sexual health topics; that is, HIV or STI prevention (n = 5) [,,,,], sexting prevention (n = 1) []; HPV vaccination intention (n = 1) [], sexuality education more broadly (n = 2) [,], pregnancy prevention (n = 1) [] or adherence/medication-related knowledge (n = 1) [].
The methodological designs were diverse: RCTs (n = 4) [,,,], quasi-experimental studies (n = 2) [,], longitudinal community-based studies (n = 1) [], and pre–post or pilot evaluations (n = 4) [,,,]. The sample size varied from 51 participants in a U.S. university study [] to 1835 preadolescents in a large-scale school-based intervention in China [].
The study population was heterogeneous. These included preadolescents aged 9–12 years in rural or primary schools (n = 2) [,], adolescents in vocational or secondary schools (n = 2) [,], diploma-level university students (n = 1) [], high school students who presented to clinics (n = 1) [], foreign-born Latino men (n = 1) [], HIV-positive men who have sex with men (n = 1) [], HIV-infected adolescents and their caregivers (n = 1) [], and adult university/community populations (n = 2) [,].
3.1. Intervention Characteristics
Among the eleven studies included in this review, the most common delivery method for animated and motion-graphic interventions was face-to-face in classrooms (n = 5) [,,,,]. These interventions were typically delivered through animated videos and structured lessons led by teachers and included interactive components such as discussions and quizzes. The second most common delivery method was digital or online (n = 4) [,,,], in which animated videos were provided via online surveys, private YouTube links, interactive games, or handheld devices. Two studies were conducted in clinical or community settings, using cartoon-style animated videos within family sessions in HIV clinics or individually tailored animated modules delivered on tablets [,].
The duration and frequency of interventions varied across studies. Three studies used brief single-session interventions [,,], whereas four studies implemented multi-session curricula lasting several weeks [,,,]. Four studies reported longer-term interventions delivered over several months, with follow-up extending to one year [,,,].
Most interventions (n = 8) incorporated interactive components such as group discussions, quizzes, individualized feedback, or follow-up conversations [,,,,,,,]. Regarding animation modality, two studies explicitly reported using 2D animation [,]. None explicitly reported 3D or mixed formats; the remaining studies did not specify the animation type. Cultural or contextual adaptation was noted in nine studies, most often as surface adaptations (e.g., translation or local iconography) and, in several cases, as deep-structure adaptations involving community or stakeholder input [,,,,,,,,]. These characteristics are summarized in Table 2.
3.2. Theoretical Frameworks and Pedagogical Approaches
Eight of the 11 studies included in the review clearly used theoretical or pedagogical frameworks to inform the design of their interventions. The Prototype Willingness Model (PWM) was used in one study [] to address sexting behaviors, whereas Li et al. [] applied the Behavioural and Social Drivers (BeSD) framework to assess willingness for HPV vaccination. The CHAMP+ Thailand family intervention was based on Social Action Theory [], and Paperny and Starn [] used Social Learning Theory in their interactive pregnancy-prevention games.
Several school-based programs were guided by comprehensive sexuality education standards from UNESCO or UNFPA, aligned with local engagement and social norms theory [,,]. Brock and Smith [] used self-efficacy theory to improve adherence to antiretroviral therapy in the United States, and Grieb et al. [] combined the Information–Motivation–Behavioral Skills (IMB) model with the Transtheoretical Model to promote HIV testing. Three studies did not cite a guiding theoretical model but employed pedagogical strategies such as peer education, co-design with local actors, or integration of digital health literacy principles [,,].
In terms of pedagogy, most interventions emphasized interactivity (n = 8), including quizzes, discussions, storytelling, or follow-up activities. Storytelling was most often employed to enhance comprehension among low-literacy participants or to strengthen cultural connectedness, as seen in CHAMP+ Thailand [] and the co-created HIV testing module for Latino men []. Cultural tailoring and linguistic adaptation were incorporated in nearly all studies to maximize acceptability.
3.3. Educational Outcomes
All 11 studies reported sexual health education-related outcomes, with the majority reporting knowledge (n = 9) and attitudes (n = 7), and some assessing intentions or behavioral outcomes (n = 6). Overall, the studies indicated that, in general, motion graphic and animated video health interventions increased individual sexual health knowledge, improved attitudes toward safer sex practices and inclusivity, and, in some cases, impacted intentions and behaviors related to sexual health prevention and decision-making.
Knowledge-related outcomes were reported in nine studies [,,,,,,,,]. Improvements in knowledge were widely documented across the studies, ranging from directed short-term gains resulting from a brief HPV vaccination video [] to short-term statistically significant acute increases in understanding of HIV medication after viewing a 17 min digital video among U.S. university students, with effects sustained over a 4–6 week period []. The sustained effects of sexual health programs and positive changes in sexual knowledge have also been seen in large school-based programs, with scores on sexual knowledge tests improving by 3.94 points immediately and 4.38 points at 1 year [] and a sustained increase in Tanzanian health education programs with 10–31% higher knowledge about HIV/AIDS and parasitic infections at 1 year []
Attitudinal outcomes were explored in seven studies [,,,,,,]. These studies reported positive attitudes such as greater inclusion of LGBTQ identities [], decreased stigma and internalized shame among HIV-infected youth [], increased contraceptive attitudes in U.S. adolescents [], and greater openness around HIV testing by Latino immigrant men []. In larger school-based interventions, attitudinal changes were observed that decreased slightly over time [].
Intentions and behavioral outcomes were assessed in six studies [,,,,,]. Mansor et al. (2023) [] reported significant reductions in intention and willingness to sext. Li et al. (2025) [] reported an increased willingness to receive HPV vaccinations. Grieb et al. (2017) [] reported an increase in HIV testing among Latino men, and Mi et al. (2015) [] reported improved HIV diagnosis disclosure and uptake of partner testing among MSM. Paperny and Starn (1989) [] noted an overall decrease in adolescent pregnancies in clinics that utilized their computer-assisted games.
3.4. Behavioral and Psychosocial Outcomes
Six studies reported outcomes that extend from knowledge and attitudes to the behavioral and psychosocial domains [,,,,,]. There were several behavioral outcomes. Mansor et al. (2023) [] indicated that among Malaysian diploma students who engaged in a short-animated video module, there were significant reductions in intention to sext (β = −0.12, p = 0.002) and willingness to sext (β = −0.16, p < 0.001). Li et al. (2025) [] reported that 88% of Chinese college students indicated a willingness to receive HPV vaccination after viewing a two-minute HPV prevention video. Mi et al. (2015) [] found that HIV-positive MSM who engaged in a web-based program with an animated game were more likely to disclose their HIV status to their partners (76% vs. 61%) and encourage their partners to undergo testing (42% vs. 26%). There was evidence of behavioral outcomes at a community level as well. Paperny and Starn (1989) [] reported that clinics implementing computer-assisted games recorded a 15% reduction in one year of adolescent positive pregnancy tests.
Three psychosocial outcomes were examined [,,]. Nestadt and colleagues found that the CHAMP+ Thailand family-based cartoon curricular approach led to significant improvement in youth mental health, HIV knowledge, adherence, caregiver–child communication, and reduced internalized stigma at 6 months post-intervention that were mostly sustained at 9 months. Zhou et al. (2024) [] did not find a significant change in sexual attitudes immediately or at one year post-intervention, but there did appear to be improvements, and any change in attitudes degraded over time, indicating that significant attitude change in large-scale school interventions is unlikely to be sustained over time. Holst and colleagues (2022) [] described psychosocial gains in Tanzania where youth who accessed community “InfoSpots” between animated health education reported increased engagement with health information and reinforced learning over the following 12 months.
3.5. Summary of Intervention Outcomes
A summary of findings across the 11 studies—covering knowledge, attitudes, behavioral intention, and psychosocial well-being—is presented in Table 5.
Table 5.
Summary of findings across included studies for knowledge gain, attitude change, behavioral intention, and psychosocial well-being.
4. Discussion
The results of this review show that motion graphics and animated videos have the potential to serve as new tools for sexual health education. Across the studies included in this review, the media consistently supported knowledge gain, attitude improvement, and intentions, behavior, and psychosocial outcomes in numerous studies. Interestingly, the effects were observed across a variety of populations, from preadolescents in school to HIV-positive adults in clinical care, and in some studies lasted up to one year after the intervention ended. Overall, these findings demonstrate the versatility of animated interventions across contexts and illustrate the ability of animated interventions to get participants to be more engaged than standard didactic teaching.
4.1. Motion Graphics and Animated Video Interventions and Educational Outcomes
The consistent knowledge gains observed across diverse populations support the idea that motion graphics and animated videos allow and advance knowledge processing of sexual health information because the content is delivered in an engaging multimedia format that simultaneously signals two channels for learning and application. Sustained knowledge improvements in school-based programs through social norms [,] suggest that delaying repeat exposures’ effects, with the potential of teacher-facilitated delivery, may allow knowledge to be reinforced and retained more than if just once, as noted with brief interventions, such as short HPV or HIV prevention videos, while the studies reported show short-term [,] knowledge gain and that well-designed, brief, low-dose learning interventions could be impactful. Attitudinal outcomes also suggested a positive change in terms of greater inclusivity toward LGBTQ+ identities [,] and more information and less stigma toward topics of sexual health and wellbeing. These studies demonstrate that animation is a safe place to examine sensitive or value-laden content. A decrease in attitudinal improvements over time suggests that in the absence of reinforcement, attitudinal change may be less stable or durable than knowledge outcomes []. An important variation in the studies reviewed is the durability of the effects. Although brief, one-time interventions such as short HPV or HIV videos showed immediate improvements in knowledge [,], indicating that animation is an effective way to engage learners quickly and get the key messages across. There was no question whether multi-session curricula designed to consider their placement within school programs had both immediate and sustained improvements in knowledge and, to a lesser extent, in attitudes up to one year post-delivery [,]. This indicates that short interventions can be efficient and scalable, but longer or more consistent exposure may be required to improve learning and change attitudes. The decline in attitudes over time in some larger-scale programs underlines the importance of thinking about reinforcement strategies to maintain psychosocial impact [].
With respect to promoting positive learning outcomes, it can be construed that several theoretical constructs might elucidate why motion graphics and animated video interventions have an effect. Among the more broadly articulated constructs is dual coding theory, as discussed by Arora and Giri (2022) [], which asserts that information is processed through both verbal and non-verbal systems. Each information system can be encoded to provide an equal yet distinct representation of conceptual information. If the content is delivered via both dual channels simultaneously or close in time, learners can build information with richer mental representations that will ultimately lead to a significantly deeper understanding and improved recall []. This principle appears to be echoed in research related to sexual health education, where narrated animations appear to increase the engagement and retention of knowledge []. Also, similarly aligned with multimedia learning research, the perspective of lessening cognitive load in relation to animations implies that both visual and verbal inputs may increase comprehensibility of material [,]. Collectively, these theories would support the premise that positive learning outcomes cited in the studies across the previous studies were tied to the nature of dual-channel processing.
Instructional animations are generally more interesting and more likely to attract learners’ attention than traditional text-based approaches. While text conveys information through printed words, animation uses a combination of visual cues, character design, voice acting, and dialogue to create a more enjoyable, motivational learning experience that also contributes to comprehension and retention []. In particular, when combining narratives with animated characters, learners enjoy the experience more and create an anxiety-free atmosphere in the learning environment, allowing for better separation between themselves and the difficult content []. It has also been demonstrated empirically that motion graphics can increase engagement and positively correlate with understanding, while alleviating stressors sometimes associated with traditional printed materials. These characteristics further demonstrate the role of engagement as a salient mechanism—both as a mediating variable influencing learning outcomes and as a protective factor that mitigates cognitive load.
While evidence of consistent positive change across studies has been observed, there is a need to interpret the level of evidence cautiously. Several studies included, and many non-randomized studies, were rated with a serious or moderate risk of bias primarily due to confounding, selection of participants, or measurement of outcomes. These biases could be overestimating the intervention or creating uncertainty about the generalizability of findings. There was too much methodological heterogeneity and variability in the quality of studies to do any quantitative weighting or sensitivity analysis. Thus, the studies and findings included in this review reported a qualitative synthesis, and future studies should utilize more rigorous designs, standardized outcomes, and transparently report quality to support the reliability of that evidence.
4.2. Motion Graphics and Animated Video Interventions and Behavioral and Psychosocial Outcomes
In addition to knowledge and attitudinal gains, some interventions showed substantial differences in behavioral and psychosocial outcomes. These animated modules, which specifically targeted sexting behaviors among Malaysian diploma students, reported reduced sexting intention and willingness. These results suggest that theory-based intervention designs can conceptualize ways to modify risky digital behavior []. Similarly, a brief HPV video intervention increased the likelihood of vaccination intention among Chinese college students, indicating that even brief exposure to animated and digitized health education can help positively frame health prevention intentions []. Behavioral change was also indicated in HIV-related contexts, where personalized animated videos increased HIV testing intention with Latino immigrant men [], and a web-based program that included an animated game promoted the disclosure of HIV status and partner testing with Chinese MSM []. Psychosocial gains were noted in family-based interventions in which cartoons were used as part of a curriculum to improve communication, decrease internalized stigma, and promote adherence among Thai adolescents living with HIV []. Community-based delivery models may also have implications for learning and engagement; Tanzanian participants reported increased knowledge gains and continued use of digital InfoSpots to seek health information []. Overall, these findings suggest that animated interventions can positively impact not only knowledge and awareness, but also actual behaviors and psychosocial well-being across a diverse range of cultural and clinical situations.
While multiple interventions showed short-term behavioral outcomes, many did not show sustained behavioral changes. Reductions in sexting intention and willingness among Malaysian diploma students were sustained three months after exposure to animated prevention modules, highlighting how effective repeated interventions based on theory can achieve enduring changes in risky digital behavior beyond the short term []. In one study on HIV prevention, researchers reported evidence of sustained explicit disclosure of HIV status and partner testing encouragement among Chinese MSM six months after participation in a web-based program that included an animated game. The authors suggested that animation was linked to the durability of behavioral change, especially when contained within multi-component web-based interventions []. Similarly, the CHAMP+ Thailand program improved adherence and family communication and reduced internalized stigma at nine months among HIV-infected adolescents []. These studies support the observation that animation may produce behavioral intention changes and sustainable behavioral changes when delivered in combination with curricula, peer support mechanisms, or family support mechanisms.
The identified changes in intentions, behaviors, and psychosocial well-being can be further contextualized using established behavioral change frameworks. The four models most relevant to the interventions reviewed are the PWM, Social Cognitive Theory (SCT), the Health Belief Model (HBM), and the IMB Model. Each model offers important features that explain the ability of animated interventions to impact decision-making, encourage protective behaviors, and address stigma.
PWM often views health behavior as a reasoned process of intentional behavior. In contrast, PWM delineates two separate pathways to health behavior: a reasoned pathway driven by deliberate intentions and a pathway driven by social reaction that involves the willingness to engage in behavior and heuristic processing []. The potentially unique constructs of PWM are behavioral willingness—an individual’s openness to engaging in a behavior whenever they are presented with an opportunity to do so—and prototypes, images of the typical person who engages in the behavior. These social images can have a particularly strong influence on adolescents, and importantly, adolescent willingness often predicts risky behavior better than intention at a younger age. Importantly, prototype favorability and similarity are not fixed and may be actively shifted by interventions. Evidence of these principles of PWM was confirmed in animations intended to effectively create new prototype perceptions and social norms: decreased willingness to sext in sexting prevention modules for Malaysian diploma students [] and increased willingness to vaccinate against HPV following a brief HPV-related video for Chinese university students []. The use of animation to create attitudinal change demonstrates how animated intervention can actualize PWM by changing young people’s social images and limiting their reactive engagement in risky behaviors.
SCT elucidates human behavior as a function of the interconnectedness of three dynamic and reciprocal factors: personal, behavioral, and environmental influencers. The schematic provides a framework for individuals’ self-efficacy and outcome expectancies related to personal behavior and notes the socio-structural influences on behavior, which are the central constructs of SCT []. In educational contexts and health promotion, animations serve to model appropriate behaviors, mitigate stigma, and enhance self-efficacy; to accomplish these educational goals, animations have relatable characters and scenarios, as illustrated in the CHAMP+ Thailand program that used cartoons in sessions to enhance communication, improve adherence to treatment, and reduce stigma among HIV-infected adolescents and their caregivers []. In the program, the intervention highlighted the coping strategies and provided role models leveraging observational learning, a key SCT principle intended to normalize conversations while reinforcing psychosocial behaviors to respond adaptively. Overall, this work illustrates how animations are an opportunity to put SCT principles into practice and foster individual capacity for agency, as well as build supportive social contexts for individuals to follow through with sustained altered behavior.
HBM conceptualizes preventive health behavior as being shaped by individuals’ perceptions of susceptibility, severity, benefits, barriers, and cues to action []. Animated interventions can increase perceived susceptibility and perceived benefits while reducing perceived barriers through clear and relatable messaging. For example, a two-minute HPV vaccination video increased the willingness for vaccination among Chinese university students [], whereas animated educational modules targeting barriers to HIV testing increased testing intentions among Latino immigrant men []. In both these examples, the animation functioned as a cue to action by making abstract risks more salient and bringing the benefits of preventive behaviors to the surface. Additionally, the HBM is applicable across diverse groups, which supports its utility in explaining why short, visually oriented media can encourage individuals to transition from awareness to action for prevention [].
Finally, the IMB model argues that three elements—accurate information, sufficient personal and social motivation, and skills needed to enact a behavior—must occur together to accomplish health behavioral changes []. Tailored animated interventions can potentially meet all three. The tailored video modules, individually focused on HIV prevention and care designed for Latino immigrant men and increased HIV testing intentions by providing information about testing, addressing motivational barriers such as stigma, and including skill-building content to access local services []. This demonstrates the strength of the model: animations can combine knowledge with motivational cues and problem-solving strategies that strengthen self-efficacy and reduce obstacles to action. Although it was initially designed for HIV-related behaviors, the organized yet adaptable nature of the IMB framework makes it particularly appropriate for multimedia interventions that blend storytelling, visual prompts, and culturally appropriate messaging [].
4.3. Conceptual Synthesis and Unified Framework
We synthesized the behavioral and learning theories referenced in the included studies and the literature, which encompass HBM [], PMT, TRA/TPB [], SCT [], IMB [], cognitive-affective learning theories (dual coding and coherence/signaling models), and narrative persuasion theory [,]. Figure 2 provides an overview of a model for some potential ways that animated and motion-graphic interventions might influence behavior change. In this model, design components (e.g., story, relatable characters, signaling, pacing, dual audio-visual cues, interactivity) and delivery features (e.g., setting, dosage/repetition, fidelity, access) influence proximal cognitive-affective mediators, including attention and engagement, comprehension and memory, emotion and identification, and perceived norms. These mediators in turn shape beliefs and efficacy (e.g., susceptibility, severity, benefits, barriers, self/response efficacy) factors (i.e., HBM, PMT, SCT, IMB), which influence attitude and intention (i.e., TRA/TPB) factors or constructs. These cognitive processes result in behavior (e.g., HIV testing, vaccination, condom use) as well as the sustaining of prevention behaviors.
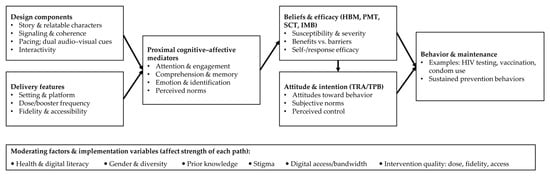
Figure 2.
Conceptual synthesis and unified framework for animated/motion-graphic sexual health interventions. HBM, Health Belief Model; PMT, Protection Motivation Theory; TRA, Theory of Reasoned Action; TPB, Theory of Planned Behavior; IMB, Information–Motivation–Behavioral Skills model; SCT, Social Cognitive Theory.
The model also accounts for moderating factors—health & digital literacy, gender & diversity, prior knowledge, stigma, digital access/bandwidth—as well as variables about the quality of the intervention (i.e., dose, fidelity, access) that may increase or decrease the overall efficacy of the intervention. This conceptual model provides clarity on where animated media will likely exert the most influence on behavior measures, through attention, comprehension, and identification with narrative, and demonstrates where future research will need to begin developing measurement instruments to assess these mediators and moderators in addition to measuring for equity-sensitive outcomes [,,].
4.4. Health and Digital Literacy as Moderators of Impact
The impact of animated or motion graphics interventions is likely to be modified by learners’ health and digital literacy. For those possessing lower health literacy, it is more difficult to understand, remember, and act on health information, which may reduce the impact of otherwise appealing media. Recent prospective data demonstrate that ineffective health literacy is associated with poor outcomes and greater health service usage, which suggests the importance of designing for low-literacy audiences and measuring literacy in subsequent trials []. Programs should, therefore, employ HL-informed design (simple language and concise messages, captions/voice-over in local language, and high contrast/icon-oriented visuals) and evaluate using brief teach-back prompts or facilitation.
4.5. Equity Considerations: Gender, Diversity, and Health/Digital Literacy
The efficacy and the equitability of animated sexual-health messages will likely differ by gender, sociocultural background, and health/digital literacy. Certainly, there is evidence of gender differences in health literacy, with women being higher in literacy than men and men with low mental health literacy being less likely to recognize and seek care [,]. Transgender and gender-diverse individuals experience structural barriers (such as limited accessible competent providers and travel barriers) that will influence how health information is accessed and utilized, even as high literacy results from self-education in some situations [,]. Health literacy is not the same across ethnic/racial groups or between migrants, where understanding and application of health information is impaired by language and cultural factors [,,]. In regard to animated media, these disparities indicate that content and delivery should either be health literacy-informed or culturally competent: scripting should be in plain language; if narratives or visuals are used, they should be inclusive and non-stigmatizing; subtitles or voice-overs should be in local languages; descriptive audio and high-contrast/icon-forward formats should be employed where possible; and brief teach-backs or facilitated discussions should also be considered to promote better understanding and action to the extent that they are feasible for animated interventions. Training implementers in cultural competence and health-literacy-sensitive communication may also enhance uptake and equity of outcomes []. Future investigations should pre-specify subgroup analyses (e.g., by gender identity/assumed gender, migrant/ethnic status, and literacy levels) and report equity-sensitive outcomes in addition to overall outcomes.
4.6. Limitations
This study has several limitations. First, this review was limited to English-language and peer-reviewed articles; the grey literature and unpublished studies were not included. These decisions introduce potential language and publication biases and may result in the omission of relevant studies. However, the use of peer-reviewed articles guarantees that the included evidence was produced at a quality level with some standards. Future reviews might consider expanding the scope to include the non-English and grey literature to reduce selection bias. Second, substantial heterogeneity was observed among populations, sexual health topics, intervention types, comparator groups, assessment tools, and follow-ups. As such, a quantitative meta-analysis was not possible; narrative synthesis was used, and the results should be treated with caution. Furthermore, future research with more standardized and methodologically consistent studies would facilitate meta-analysis. Third, although the search strategy explored both 2D and 3D animation modalities, none of the included studies explicitly mentioned 3D or mixed formats. Thus, it was not possible to assess any possible differences in terms of learning effects across the different types of animation. In addition, although user interactivity and cultural adaptation were taken from the studies and summarized, the reporting was inconsistent, thereby inhibiting the assessment of the independent effects of these variables on the outcomes. Future studies should describe and assess these variables explicitly to enable more systematic comparisons and quantitative synthesis. Fourth, data were almost exclusively self-reported and used instruments of varying levels of validation, with harms or unintended consequences seldom addressed. Well-prepared research would use multiple sources of data and standardized measures in the assessment. Fifth, there was a lack of reporting of intervention fidelity, adherence, production quality, or implementation context (e.g., facilitator training, costs, and scalability); as such, it was difficult to evaluate feasibility and reproducibility in the real world. Future research should include reporting frameworks to document the delivery of interventions. Sixth, evidence was gathered from various geographic locations but primarily clumped in only a few countries, limiting the generalizability and implications for different cultural and educational contexts. Future research conducted in different geographic or sociocultural contexts would enhance the external validity and culturally relevant interventions. Finally, several included articles exhibited a serious or moderate risk of bias, specifically in the group of non-RCTs, which had issues with confounding, participant selection, and outcome measurement. Concerns regarding outcome assessment were noted, even in RCTs. The identified risk of bias could compromise the trustworthiness of the synthesized evidence, so results should be interpreted with caution. Taken together, the predominance of non-randomized designs, serious or moderate risk of bias ratings, and inconsistent outcome measures suggest that the overall strength of evidence in favor of motion graphics and animated videos in sexual health education is low to moderate and should be interpreted cautiously.
Despite the possibilities for animated and motion-graphic interventions as methods of communication, there is currently only a limited evidence base in terms of size, consistency, and rigor of methods. As a result, large-scale implementation or cost-effectiveness cannot be justified at this point. Nevertheless, the findings from this study suggest that these types of media may supplement existing health-education strategies, assuming that future research generates stronger evidence of effectiveness and sustainability. Future studies should evaluate implementation and economic outcomes (e.g., production costs, delivery feasibility, and scale across settings), which would inform public health planning at a more impactful level.
5. Conclusions
This systematic review emphasizes the promise of multimedia (motion graphics and animated videos) as a viable approach to health, health promotion, and sexual health messages. Multimedia consistently improved knowledge and attitudes in several audience contexts and, on some occasions, influenced intentions, behaviors, and psychosocial outcomes. Both short, scalable campaigns and more complex interventions that incorporated multiple sessions were effective; however, the authors found sustained change was most likely when the content was recurring and grounded in theory and the social context. Prior research has suggested using theories and frameworks for developing culturally tailored and theory-based interventions, including SCT, HBM, PWM, and IMB. Motion graphics and animated videos also provide a safe and engaging medium to address sensitive topics and serve as an avenue to alleviate stigma and embrace inclusivity in sexual health messages. Future studies should focus on standardization of the design and content, long-term effects, and facilitating implementation (i.e., fidelity, scalability, and cost). In conclusion, animated and motion graphics media have educational potential, but the evidence is insufficient to determine their widespread use or cost-effectiveness. Further research is needed to determine their long-term effects on learning outcomes and best practices for integrating these tools into educational settings. Technology will need to be tested in diverse learning environments as it advances. Motion graphics and animated media show promise for improving sexual-health knowledge and attitudes and, in select contexts, intentions and behaviors. However, the body of evidence is small and heterogeneous, with frequent high risk of bias; certainty is therefore low to moderate. Future research should prioritize standardized outcomes, longer follow-up, and implementation and cost-effectiveness evaluations before advocating large-scale adoption.
Supplementary Materials
The following supporting information can be downloaded at: https://www.mdpi.com/article/10.3390/healthcare13222895/s1. PRISMA checklist.
Author Contributions
Conceptualization, N.S., D.M., and W.T.; methodology, N.S., D.M., and W.T.; validation, N.S., D.M., and W.T.; formal analysis, N.S., D.M., and W.T.; investigation, N.S., D.M., and W.T.; data curation, W.T.; visualization, W.T.; writing—original draft preparation, N.S.; writing—review and editing, N.S., D.M., S.K., C.E., and W.T.; supervision, S.K. and C.E.; project administration, W.T. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Ethics Committee of Walailak University (protocol code WUEC-25-326-01), approved on 3 September 2025.
Informed Consent Statement
Not applicable.
Data Availability Statement
All data supporting the reported results are included in this article.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| ART | antiretroviral therapy |
| ATLG | Attitudes Toward Lesbians and Gay Men |
| BeSD | Behavioral and Social Drivers of Vaccination |
| DID | difference-in-differences |
| DOAJ | Directory of Open Access Journals |
| HBM | Health Belief Model |
| HIV | human immunodeficiency virus |
| IMB | Information–Motivation–Behavioral Skills model |
| LGBTQ+ | lesbian, gay, bisexual, transgender, queer/questioning, and other sexual and gender minorities |
| MEDLINE | Medical Literature Analysis and Retrieval System Online |
| MSM | men who have sex with men |
| PDA | personal digital assistant |
| PMT | Protection Motivation Theory |
| PrEP | pre-exposure prophylaxis |
| PEP | post-exposure prophylaxis |
| PSM | propensity score matching |
| PWM | Prototype Willingness Model |
| RCT | randomized controlled trial |
| ROBINS-I | Risk of Bias in Non-randomized Studies of Interventions |
| RoB 2 | Cochrane Risk of Bias 2 tool |
| SCT | Social Cognitive Theory |
| STI | sexually transmitted infection |
| TRA | Theory of Reasoned Action |
| TPB | Theory of Planned Behavior |
| UNFPA | United Nations Population Fund |
| UNESCO | United Nations Educational, Scientific and Cultural Organization |
References
- Bidaisee, S. Sexual and reproductive health education. In Caribbean Adolescents: Some Public Health Concerns; Nova Science Publishers, Inc.: New York, NY, USA, 2015; pp. 95–106. [Google Scholar]
- Prize, N.B.T.; Shimony-Kanat, S.; Wruble, A.C.K.W. Gaps in sexual health content of healthcare professional curriculum: A systematic review of educational interventions. BMC Med. Educ. 2023, 23, 926. [Google Scholar] [CrossRef] [PubMed]
- Szucs, L.E.; Barrios, L.C.; Young, E.; Robin, L.; Hunt, P.; Jayne, P.E. The CDC’s Division of Adolescent and School Health Approach to Sexual Health Education in Schools: 3 Decades in Review*. J. Sch. Health 2022, 92, 223–234. [Google Scholar] [CrossRef] [PubMed]
- Dickson, E.; Rishel Brakey, H.; Wilson, P.; Hackett, J.M.; McWethy, M. Classroom voices: Youth perspectives to direct school-based sexual health education. Sex Educ. 2024, 24, 479–496. [Google Scholar] [CrossRef]
- Djuric, P.; Stevanovic, A.; Rajovic, N.; Todorovic, J.; Laaser, U. Reproductive health of medical students: Exploring knowledge, experiences, and behaviors. South East. Eur. J. Public Health 2022, 2022. [Google Scholar] [CrossRef]
- Hall, W.J.; Jones, B.L.H.; Witkemper, K.D.; Collins, T.L.; Rodgers, G.K. State policy on school-based sex education: A content analysis focused on sexual behaviors, relationships, and identities. Am. J. Health Behav. 2019, 43, 506–519. [Google Scholar] [CrossRef]
- Sovianti, R.; Sarwoprasodjo, S.; Hubeis, A.V.S.; Herawati, T. Communication Infrastructure for the prevention of free sex behavior of adolescents in Bogor Regency, Indonesia. Multidiscip. Sci. J. 2024, 6, 2024214. [Google Scholar] [CrossRef]
- Manão, A.A.; Brazão, M.; Pascoal, P.M. How to Define Sexual Health? A Qualitative Analysis of People’s Perceptions. Int. J. Sex. Health 2025, 37, 131–152. [Google Scholar] [CrossRef]
- Mayo, C. Sexuality education policy and the educative potentials of risk and rights. Policy Futures Educ. 2011, 9, 406–415. [Google Scholar] [CrossRef]
- Ivanova, O.; Kemigisha, E.; Cruz Murueta, M.; Korri, R. Sexuality education from an international perspective. In Reproduction Policy in the Twenty-First Century: A Comparative Analysis; Edward Elgar Publishing: Cheltenham, UK, 2024; pp. 68–85. [Google Scholar]
- Holt, D. Young adults’ perspectives on sex education at school in Scotland. Pastor. Care Educ. 2025, 1–22. [Google Scholar] [CrossRef]
- Cushman, N.; Kantor, L.M.; Schroeder, E.; Eicher, L.; Gambone, G. Sexuality education: Findings and recommendations from an analysis of 10 United States programmes. Sex Educ. 2014, 14, 481–496. [Google Scholar] [CrossRef]
- Ulfah, W.A.; Santoso, N.; Putranto, D.; Ramadan, G. Application of video animation to increase students’ interest and physical skills in primary school physical education. Retos 2025, 66, 766–772. [Google Scholar] [CrossRef]
- Minalla, A.A. Enhancing Young EFL Learners’ Vocabulary Learning Through Contextualizing Animated Videos. Theory Pract. Lang. Stud. 2024, 14, 578–586. [Google Scholar] [CrossRef]
- Cookson, A.; Kim, D.; Hartsell, T. Enhancing Student Achievement, Engagement, and Satisfaction Using Animated Instructional Videos. Int. J. Inf. Commun. Technol. Educ. 2020, 16, 113–125. [Google Scholar] [CrossRef]
- Hapsari, A.S.; Hanif, M. Motion graphic animation videos to improve the learning outcomes of elementary school students. Eur. J. Educ. Res. 2019, 8, 1245–1255. [Google Scholar] [CrossRef]
- Crook, I.; Beare, P. Motion Graphics: Principles and Practices from the Ground Up; Bloomsbury Publishing: London, UK, 2017. [Google Scholar]
- Geng, L. Study of the motion graphic design at the Digital Age. In Proceedings of the 2nd International Conference on Arts, Design and Contemporary Education, Beijing, China, 5–7 May 2016; pp. 761–763. [Google Scholar]
- Chen, C.M.; Chang, Y.J. A Study On Development and Current Aplication of Motion Graphic In Taiwan’s Popular Music. PEOPLE Int. J. Social. Sci. 2019, 5, 124–134. [Google Scholar]
- Kleftodimos, A. Computer-Animated Videos in Education: A Comprehensive Review and Teacher Experiences from Animation Creation. Digital 2024, 4, 613–647. [Google Scholar] [CrossRef]
- Martinez, O.O.L. Criteria for defining animation: A revision of the definition of animation in the advent of digital moving images. Animation 2015, 10, 42–57. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Flemyng, E.; Moore, T.H.; Boutron, I.; Higgins, J.P.; Hróbjartsson, A.; Nejstgaard, C.H.; Dwan, K. Using Risk of Bias 2 to assess results from randomised controlled trials: Guidance from Cochrane. BMJ Evid. Based Med. 2023, 28, 260–266. [Google Scholar] [CrossRef]
- Jüni, P.; Loke, Y.; Pigott, T.; Ramsay, C.; Regidor, D.; Rothstein, H.; Sandhu, L.; Santaguida, P.; Schünemann, H.; Shea, B. Risk of bias in non-randomized studies of interventions (ROBINS-I): Detailed guidance. Br. Med. J. 2016, 355, i4919. [Google Scholar]
- Huang, E.; Zhang, A.; Yan, J. Effects of Delivering an Animation-Based Inclusive Sex Education Curriculum for Adolescents in China. J. Homosex. 2024, 71, 414–431. [Google Scholar] [CrossRef]
- Li, X.; Zheng, J.; Zhang, Z.; Fu, D.; Zhao, L.; Li, H.; Sun, Y.; Lan, Q.; Zhao, X.; Wang, M.; et al. An investigation of HPV vaccination willingness and influential factors among college students in Beijing based on the BeSD framework and evaluation of momentary intervention effect. Hum. Vaccin. Immunother. 2025, 21, 2505354. [Google Scholar] [CrossRef] [PubMed]
- Mi, G.; Wu, Z.; Wang, X.; Shi, C.X.; Yu, F.; Li, T.; Zhang, L.; McGoogan, J.M.; Pang, L.; Xu, J.; et al. Effects of a quasi-randomized web-based intervention on risk behaviors and treatment seeking among HIV-positive men who have sex with men in Chengdu, China. Curr. HIV Res. 2015, 13, 490–496. [Google Scholar] [CrossRef]
- Wang, K.; Xu, S.S.; Liu, Z.; Wang, W.; Hee, J.; Tang, K. A quasi-experimental study on the effectiveness of a standardized comprehensive sexuality education curriculum for primary school students. J. Adolesc. 2023, 95, 1666–1677. [Google Scholar] [CrossRef]
- Zhou, H.; Zhang, H.; Xiao, A.Y.; Yu, L.; Tang, K. Effects of an Animation-Based Comprehensive Sexuality Education Package: A 2-Year Repeated Intervention Study. Health Educ. Behav. 2024, 51, 733–747. [Google Scholar] [CrossRef]
- Brock, T.P.; Smith, S.R. Using digital videos displayed on personal digital assistants (PDAs) to enhance patient education in clinical settings. Int. J. Med. Inform. 2007, 76, 829–835. [Google Scholar] [CrossRef]
- Grieb, S.M.D.; Flores-Miller, A.; Page, K.R. Sólo Se Vive Una Vez! (you only live once): A pilot evaluation of individually tailored video modules aiming to increase HIV testing among foreign-born latino men. In Proceedings of the Journal of Acquired Immune Deficiency Syndromes, Paris, France, 23–26 July 2017; pp. S104–S112. [Google Scholar]
- Paperny, D.M.; Starn, J.R. Adolescent pregnancy prevention by health education computer games: Computer-assisted instruction of knowledge and attitudes. Pediatrics 1989, 83, 742–752. [Google Scholar] [CrossRef]
- Mansor, N.; Ahmad, N.; Md Said, S.; Tan, K.A.; Sutan, R. Effectiveness of a Theory-Based Digital Animated Video Intervention to Reduce Intention and Willingness to Sext Among Diploma Students: Cluster Randomized Controlled Trial. J. Med. Internet Res. 2023, 25, e48968. [Google Scholar] [CrossRef]
- Holst, C.; Stelzle, D.; Diep, L.M.; Sukums, F.; Ngowi, B.; Noll, J.; Winkler, A.S. Improving Health Knowledge Through Provision of Free Digital Health Education to Rural Communities in Iringa, Tanzania: Nonrandomized Intervention Study. J. Med. Internet Res. 2022, 24, e37666. [Google Scholar] [CrossRef] [PubMed]
- Nestadt, D.F.; Saisaengjan, C.; McKay, M.M.; Bunupuradah, T.; Pardo, G.; Lakhonpon, S.; Gopalan, P.; Leu, C.S.; Petdachai, W.; Kosalaraksa, P.; et al. CHAMP+ Thailand: Pilot Randomized Control Trial of a Family-Based Psychosocial Intervention for Perinatally HIV-Infected Early Adolescents. AIDS Patient Care STDS 2019, 33, 227–236. [Google Scholar] [CrossRef] [PubMed]
- Arora, B.; Giri, J.N. Dual coding theory and its application in healthcare facility. Int. J. Health Sci. 2022, 6, 5021–5025. [Google Scholar] [CrossRef]
- Bi, Y. Dual coding of knowledge in the human brain. Trends Cogn. Sci. 2021, 25, 883–895. [Google Scholar] [CrossRef]
- Lin, L.; Leh, A. Using visualizations to enhance learning: Theories and techniques. In Educational Technologies: Challenges, Applications and Learning Outcomes; Nova Science Publishers, Inc.: New York, NY, USA, 2016; pp. 1–16. [Google Scholar]
- Mayer, R.E. Applying the Science of Learning to Multimedia Instruction; Academic Press: London, UK, 2011; Volume 55, pp. 77–108. [Google Scholar]
- Liu, C.; Elms, P. Animating student engagement: The impacts of cartoon instructional videos on learning experience. Res. Learn. Technol. 2019, 27, 1–31. [Google Scholar] [CrossRef]
- Alhyari, N.; Marar, R.; Tedmori, S. The Impact of Motion Graphics versus Text-Based Formats on Anxiety and Learning: A Case Study in Jordan. Int. J. Eng. Pedagog. 2025, 15, 75–93. [Google Scholar] [CrossRef]
- Gibbons, F.X.; Stock, M.L.; Gerrard, M. The prototype-willingness model. Wiley Encycl. Health Psychol. 2020, 517–527. [Google Scholar] [CrossRef]
- Luszczynska, A.; Schwarzer, R. Social cognitive theory. Fac. Health Sci. Publ. 2015, 2015, 225–251. [Google Scholar]
- Anuar, H.; Shah, S.; Gafor, H.; Mahmood, M.; Ghazi, H.F. Usage of Health Belief Model (HBM) in health behavior: A systematic review. Malays. J. Med. Health Sci. 2020, 16, 2636–9346. [Google Scholar]
- Jones, C.J.; Smith, H.; Llewellyn, C. Evaluating the effectiveness of health belief model interventions in improving adherence: A systematic review. Health Psychol. Rev. 2014, 8, 253–269. [Google Scholar] [CrossRef]
- Chang, S.J.; Choi, S.; Kim, S.-A.; Song, M. Intervention strategies based on information-motivation-behavioral skills model for health behavior change: A systematic review. Asian Nurs. Res. 2014, 8, 172–181. [Google Scholar] [CrossRef]
- Dubov, A.; Altice, F.L.; Fraenkel, L. An information–motivation–behavioral skills model of PrEP uptake. AIDS Behav. 2018, 22, 3603–3616. [Google Scholar] [CrossRef] [PubMed]
- Cocchieri, A.; Cristofori, E.; Nurchis, M.C.; Nursing and Public Health Group; Damiani, G.; Cesare, M. Nursing Complexity and Health Literacy as Determinants of Patient Outcomes: A Prospective One-Year Multicenter Cohort Study. Nurs. Rep. 2025, 15, 135. [Google Scholar] [CrossRef] [PubMed]
- Blom, S.; Lindh, F.; Lundin, A.; Burström, B.; Hensing, G.; Löve, J. How gender and low mental health literacy are related to unmet need for mental healthcare: A cross-sectional population-based study in Sweden. Arch. Public Health 2024, 82, 12. [Google Scholar] [CrossRef]
- Chakraverty, D.; Baumeister, A.; Aldin, A.; Seven, Ü.S.; Monsef, I.; Skoetz, N.; Woopen, C.; Kalbe, E. Gender differences of health literacy in persons with a migration background: A systematic review and meta-analysis. BMJ Open 2022, 12, e056090. [Google Scholar] [CrossRef] [PubMed]
- Holloway, B.T.; Gerke, D.R.; Call, J.; Hostetter, C.R.; Greenfield, J.C.; Atteberry-Ash, B.; Walls, N.E. “The doctors have more questions for us”: Geographic differences in healthcare access and health literacy among transgender and nonbinary communities. Qual. Soc. Work. 2023, 22, 1073–1091. [Google Scholar] [CrossRef]
- Krueger, M.E.; Roque, R.A.; Reece-Nguyen, T.L.; MacCormick, H. Analysis of Transgender and Gender-Diverse Topics Within Diversity, Equity, and Inclusion Curricular Content in Pediatric Anesthesiology Fellowship Programs in the United States and Canada—A Prospective Survey. Paediatr. Anaesth. 2025, 35, 207–214. [Google Scholar] [CrossRef]
- Aldin, A.; Baumeister PhD, A.; Chakraverty, D.; Monsef, I.; Noyes, J.; Kalbe, E.; Woopen, C.; Skoetz, N. Gender differences in the context of interventions for improving health literacy in migrants: A qualitative evidence synthesis. Cochrane Database Syst. Rev. 2024, 2024, CD013302. [Google Scholar] [CrossRef]
- Yu, Y.; Altares, A.; Leib, A.; Bellows, L.L.; Berry, C.; Graham, D.J.; Mueller, M.P. Sociodemographic disparities in health literacy among American adults: A national survey study. Prev. Med. Rep. 2025, 57, 103179. [Google Scholar] [CrossRef]
- Lie, D.; Carter-Pokras, O.; Braun, B.; Coleman, C. What do health literacy and cultural competence have in common? Calling for a collaborative health professional pedagogy. J. Health Commun. 2012, 17, 13–22. [Google Scholar] [CrossRef] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).