Abstract
Nature-based solutions (NbS) are increasingly promoted in European policy for their potential to support climate adaptation and contribute to human health. Yet evidence on their health impacts remains fragmented across disciplines and limited to specific health outcomes or ecosystems. We carried out a systematic review of studies assessing the links between NbS and human health in Europe, covering multiple ecosystem types (agricultural, coastal, forest, mountain, urban, rural and freshwater ecosystems) and both mental and physical health outcomes. A total of 115 studies met the inclusion criteria and were concentrated in the United Kingdom (38%) and Spain (17%), with urban (45%) and forest (17%) ecosystems most frequently examined. Most studies evaluated Type 1 NbS (minimal intervention) and focused on adult populations (58%). Mental health outcomes were studied nearly twice as often as physical health, including positive mental health, circulatory diseases and mental and behavioural disorders. Nearly 88% of quantitative studies reported at least one positive association, whereas qualitative studies highlighted that perceived health benefits of NbS were often shaped by participants’ subjective experiences. Our findings emphasise the need for more longitudinal and experimental research designs, attention to NbS types and equity considerations, and better integration of human health into NbS planning and policy.
1. Introduction
Urban populations are expanding rapidly across the world [1], with 75% of Europe’s population residing in urban areas as of 2023 [2]. This growth, in combination with the severe impacts of current climate breakdown, including rising urban temperatures, storms, extreme droughts and precipitation, and other environmental hazards, places substantial pressure on cities to provide good living conditions for their residents [3,4]. Urbanisation is associated with lifestyle changes that contribute to the rising prevalence of non-communicable diseases (NCDs) across Europe [5,6]. NCDs, such as diabetes, obesity, chronic respiratory diseases, cancer, mental and cardiovascular disorders, are dominating the current global disease burden in Europe [7,8]. NbS such as urban green and blue spaces can support citizens’ well-being and coping capacity, for example, by encouraging time spent outdoors in cleaner air, which may help reduce the risk of these diseases [9].
The World Health Organization’s International Classification of Disease (WHO ICD-11) categorises common mental disorders as mood disorders and neurotic, stress-related and somatoform disorders [10]. Depression and anxiety, in particular, are among the most disabling conditions, affecting over 320 million and 260 million people worldwide, respectively [11,12]. Common mental disorders pose a substantial public health challenge, influencing a broad spectrum of health, economic, and social outcomes [13]. They account for 13% of the total global burden of diseases [14] and for 7.4% of disability-adjusted life years (DALYs) [15]. Similarly, physical health outcomes related to urban environments remain a major concern. Factors such as air and noise pollution, poor urban design, and higher population densities can lead to both acute and chronic respiratory diseases, heart diseases, hypertension, lung cancer and asthma [16,17,18]. Poorly chosen vegetation can further aggravate respiratory and allergic issues through increased pollen.
Urban environments are also characterised by elevated levels of harmful exposures, including air pollution and noise generated by motorised traffic and industrial activities [19,20]. In addition, air pollution causes around four million premature deaths annually, largely from heart disease, stroke, respiratory illnesses, and cancers linked to fine particulate matter (PM2.5). Excessive urban noise can disrupt sleep, elevate stress, and affect cardiovascular health, and urban design plays a key role in shaping daily habits such as physical activity and diet, which directly influence health and well-being [17]. Air pollution alone accounts for around 600,000 deaths annually in the pan-European region [21], while noise is a recognised health risk, causally linked to, for example, mental and cardiovascular disorders [20].
There is growing consensus that biodiversity and ecosystem services play a crucial role in human health and well-being [22]. For instance, neighbourhood greenness is broadly associated with improved quality of life [23], life satisfaction [24] and subjective well-being [25], and reduced prevalence of negative dimensions of mental health such as depression [26] and anxiety [27]. Exposure to greenspaces has also been shown to be protective against risk factors for mental ill-health such as psychological stress [28,29] and can contribute to attention restoration [30]. Living in greener areas has been associated with reduced all-cause mortality, with particularly pronounced effects among men, infants, and lower socioeconomic groups [31]. Greenspace exposure during pregnancy is associated with improved foetal growth, birth outcomes, and childhood cognitive development [32]. Emerging research highlights the importance of contact with nature in developing a healthy internal biome, potentially reducing inflammatory diseases such as asthma [33]. While evidence is mixed, some studies suggest a positive or weak association between greenspace and obesity-related health indicators [34]. Additionally, exposure to natural environments has been associated with favourable physiological outcomes, including improved heart rate, blood pressure [35], vitamin D levels [36], and cortisol levels [37], as well as lower prevalence of type 2 diabetes [38]. Health outcomes are shaped by multiple and interdependent factors that span not only individual characteristics (such as age, gender, etc.) but also wider social and environmental determinants [39]. When sections of the population experience greater disadvantages in the conditions in which they live, work and socialise, they are likely to have poorer health outcomes in comparison to populations who experience fewer disadvantages. These avoidable differences in health outcomes, caused by structural systems, are known as health inequalities and intersect across socioeconomic status (SES), gender, sexuality, disability, age and ethnicity [40]. Addressing these inequalities requires interventions that can improve both environmental conditions and health outcomes across diverse populations.
While there is compelling evidence of the link between nature and health, the explicit relationship between NbS and health remains underexplored. Nature-based solutions (NbS) are being increasingly recognised as an integrated approach to addressing urban environmental challenges while simultaneously delivering health and well-being benefits [41,42]. NbS include a wide range of interventions, including ecosystem restoration, the greening of grey surfaces, and integrated climate change mitigation measures such as afforestation, natural flood control, or constructing wetlands [4,43]. Furthermore, NbS can be classified into three types based on the level of human intervention [44]. Type 1 NbS entail minimal intervention, focusing primarily on conservation and protection measures for existing ecosystems. Type 2 involve more active management practices aimed at ensuring sustainable and multifunctional use of ecosystems, typically requiring moderate intervention, while Type 3 represent the highest level of intervention, such as the creation of entirely new ecosystems.
Existing NbS frameworks often prioritise environmental and ecological outcomes over direct health impacts [4]. Therefore, more research is needed to better understand the health and well-being benefits of NbS and how they can better be integrated into planning frameworks. Moreover, much of the evidence assessing the health and well-being benefits of NbS relies on relatively simple metrics to measure exposure, such as the amount of accessible greenspace [45]. While such studies provide important insights, we still lack a clear understanding of the causal pathways and mechanisms that link NbS, health and well-being [46]. This lack of mechanistic understanding of pathways linking NbS to health and well-being limits the application of NbS in public health and influence on policy [47]. Therefore, more research is needed that explores how different pathways shape the relationship between NbS, human health and well-being.
The evidence base for the health benefits of NbS is growing rapidly. Yet, we still need to understand the shape of the relationships between specific elements of biodiversity and health and well-being outcomes [46,48]. To date, it remains unclear what constitutes a high-quality NbS from an ecological perspective and what the role of biodiversity is in this complex relationship [49]. There is some evidence suggesting that biodiverse NbS provide additional benefits for people’s health and well-being compared to greenspaces low in biodiversity [45,50,51]. However, while people prefer experiencing high species diversity [45], they tend to gain benefits from perceived rather than actual biodiversity [45,52,53]. Nevertheless, we still know little about the specific contributions that these different biodiversity attributes of NbS make to health and well-being [53].
Inequalities exist in access to and experience of biodiversity, with those from different social groups (SES, gender, sexuality, etc.) being less likely to visit parks, gardens and other natural spaces [54]. However, when those who are less likely to do so use NbS, the experienced health benefits from environmental interventions can be greater than for less-disadvantaged groups [55,56]. This suggests that, if improvements in the access to and characteristics of NbS promote greater use of these spaces, they could have the potential to reduce health inequalities. However, there is limited evidence on whether and how NbS can mitigate such health inequalities for vulnerable social groups, particularly in light of climate breakdown [57]. Therefore, more research is needed to examine the long-term effectiveness of NbS in reducing health disparities and to identify the specific mechanisms through which these benefits are realised.
Despite evidence of health benefits, research on the economic value of NbS remains limited, particularly regarding cost-effectiveness, healthcare savings, and return on investment [29]. Most valuations focus on property price differentials or recreational benefits, rather than direct health outcomes [58]. Methodological challenges hinder standardised economic assessments [59]. However, emerging studies suggest substantial cost savings. For instance, studies report that equitable greenspace access in England could save £2.1 billion annually in healthcare costs [59]. However, further research is needed to refine valuation methods and strengthen the economic case for NbS in public health.
We conducted a systematic review of the links between NbS and human health, expanding beyond previous reviews that focused on specific health outcomes. There are several reviews focusing on the relationships between human health and nature, e.g., [4,34,60,61,62,63,64,65,66,67,68], focusing on climate change adaptation [69], vulnerable or disadvantaged groups [70,71], and more specifically on greenspaces and mental health [72,73,74,75,76,77,78,79]. The number of studies investigating the health and well-being effects of nature has increased since these reviews. To the best of our knowledge, a targeted search (2023-April 2026) revealed no existing peer-reviewed systematic review matching our scope, i.e., synthesising links between NbS and human health across Europe, covering a broad range of ecosystem types and physical and mental health outcomes. Here, we provide a stocktake of the current research on NbS and human health in Europe, identifying key knowledge gaps in the existing literature to guide future research. Specifically, we assessed the geographic distribution of evidence in Europe to understand whether there are any under-represented areas and assess which ecosystem types are assessed across studies. Our focus on Europe is grounded not only due to this study being part of the Invest4Nature project [80], a Horizon Europe research project, but also in the continent’s diverse socioecological contexts, governance frameworks, and growing policy interest in implementing NbS. Furthermore, we explored how NbS exposure was measured across studies and which study designs were predominantly used. We examined what types of NbS are typically being assessed and unpack links between NbS type and health outcomes. By assessing a broad range of physical and mental health outcomes we reveal which health outcomes we currently lack knowledge about. Finally, we explored potential negative health impacts of NbS, and the extent to which NbS can provide health benefits for vulnerable social groups and mitigate climate change and disaster risks.
2. Materials and Methods
2.1. Search Criteria
We conducted a systematic literature review following the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) [81] guidelines, spanning two electronic databases, Web of Science Core Collection [82] and Scopus [83], using queries designed to identify studies conducted in Europe that addressed NbS in relation to mental and physical health outcomes. We adopted the World Health Organization’s definition of health, considering it as “a state of complete physical, mental and social well-being and not merely the absence of disease or infirmity” [84]. These definitions guided our inclusion and exclusion criteria for assessing eligible studies for this review. The search strategy involved developing a list of relevant keywords and queries tailored to our research objectives. These predefined queries were then applied to the selected databases in April 2023 (Table 1).

Table 1.
Search strings for the electronic databases Web of Science Core Collection and Scopus.
2.2. Eligibility Criteria
The term “Nature-based Solutions” (NbS) was first introduced in 2009, but many of the activities and interventions encompassed by the concept have been implemented well before they have been defined as a concept [85]. Hence, we did not apply any restrictions on publication dates. The PRISMA flow diagram (Figure 1) was used to document each stage of the review process, including the number of records identified, screened, included, and excluded, as well as the reasons for exclusion. All identified records were organised and screened in HubMeta [86] following the procedures outlined below. Eligibility criteria required studies to present original research, be published in peer-reviewed journals, and be available in English. Publications such as case reports, reviews, opinion pieces, editorials, comments, newsletters, and grey literature were excluded from the analysis. Studies needed to meet three main criteria: (1) reference to NbS or nature, (2) assessment of NbS impact or similar interventions on human health and well-being, and (3) location within geographical Europe [87]. Studies not meeting these criteria were excluded.
NbS have been defined by the United Nations Environmental Assembly (UNEA) as “actions to protect, conserve, restore, sustainably use and manage natural or modified terrestrial, freshwater, coastal and marine ecosystems, which address social, economic and environmental challenges effectively and adaptively, while simultaneously providing human well-being, ecosystem services and resilience and biodiversity benefits” [88]. We operationalised NbS as per this definition by UNEA using search terms (Table 1) to capture diverse ecosystem types (e.g., urban, forests, mountains), even when not explicitly labelled ‘NbS’. This ensured that our search string picked up interventions that fit the UNEA definition (see Section 1) of NbS even when they were not labelled as such.
2.3. Screening Stage
We employed a two-stage screening process to identify studies that met our eligibility criteria. In the first stage, two reviewers independently screened the titles and abstracts of all retrieved records. Studies meeting the inclusion criteria at this stage were advanced to the second stage, where one reviewer conducted a full-text assessment of each study. An additional reviewer then cross-checked these full-text decisions to ensure that all included and excluded studies met the established criteria. Conflicts or uncertainties at any stage were discussed collectively by the research team until a consensus was reached, following the predefined criteria to ensure consistency and transparency.
The search string resulted in 3000 records from Web of Science (n = 1466) and Scopus (n = 1534). After duplicates were removed, 2426 studies remained for screening. Title and abstract screening led to 332 studies moving to full-text review. Following the final review process, 115 studies met all eligibility criteria and were approved for data extraction and analysis. Separate data extraction sheets (Supplementary S1) were prepared for quantitative (n = 101) and qualitative (n = 14) studies (Figure 1). Studies that employed both methods were categorised as quantitative, and for these, the same data categories were extracted along with additional quantitative indicators.

Figure 1.
Identification of studies via the electronic databases Web of Science Core Collection and Scopus, through a PRISMA flowchart [89]. A total of 115 studies were included in this review.

2.4. Data Extraction and Analysis
Data for each study were extracted by a single reviewer, while two additional reviewers blindly rechecked the extracted data for accuracy and completeness. Any inconsistencies or uncertainties identified during this process were resolved through discussion among the reviewers until agreement was reached.
Using the stated eligibility criteria, we designed a data extraction table to abstract key information, including title, year of publication, countries studied, ecosystem types, NbS types, NbS objects (e.g., gardens, parks, woodland), NbS exposure, scale of NbS (in hectares), study design and population, sample size, health indicators and outcomes. In addition, we extracted information, where available, on economic valuation, vulnerable social groups, and any climate-change-related outcomes or co-benefits associated with the NbS interventions.
To improve comparability, all monetary values of health benefits reported in economic valuation studies were converted to Euros and standardised to 2023 prices using World Bank GDP purchasing power parity (PPP) [90] conversion factors and inflation adjustment for the relevant base year. Values were first converted to Euros using the relevant currency/PPP adjustment for the study year and then inflated to 2023 prices using the appropriate price index.
We primarily grouped all health outcomes based on the World Health Organization’s International Classification of Diseases, 11th revision (ICD-11) Mortality and Morbidity Statistics [91]. Some health outcomes in the studies did not fit directly in the ICD-11 categories, such as general health and health status factors. Hence, we created additional descriptive categories, defined in Supplementary Table S1, to improve consistency.
Due to marked heterogeneity across the 115 studies, such as in study designs, NbS types, exposure metrics, and health outcomes, meta-analysis and statistical synthesis were inappropriate. We therefore conducted a narrative synthesis instead. Data were thematically synthesised to record links between NbS and health outcomes and which NbS types and ecosystem types were studied.
Frequencies (n, %) report all counts by category, allowing multi-attribution; e.g., multi-country studies were counted per country, and studies with multiple types of study population or health outcomes were counted per relevant subcategory. Percentages use category-specific denominators (e.g., the percentage of cross-sectional studies was calculated as cross-sectional counts divided by total study design counts). Totals thus exceed 115 studies. Detailed information on the categorisation of health outcomes and the variables used in the data extraction tables, including their definitions, and summary statistics are provided in Supplementary S1 and S2.
3. Results
A total of 115 studies met the inclusion criteria and were included in the final synthesis, comprising 101 quantitative and 14 qualitative studies. The quantitative studies primarily employed cross-sectional survey designs and longitudinal and before–after studies, whereas the qualitative studies included interviews (n = 11) and focus groups (n = 3) to explore individual and community-level perceptions of health impacts.
3.1. Studies by Year and Geographical Region
Quantitative studies on NbS and health increased markedly after 2016, peaking in 2020 (n = 23). Geographically, research was heavily concentrated in Western Europe. The United Kingdom contributed the largest share (n = 79), followed by Spain (n = 40). Together, these account for over half of all reviewed studies. Other frequently studied countries include Italy (n = 11), Belgium (n = 9), and the Netherlands (n = 9). In contrast, evidence from Eastern and Southern Europe is sparse, with only isolated studies from countries such as Romania (n = 1), Slovenia (n = 1), and Slovakia (n = 1). Most of the qualitative studies were published between 2017 and 2021, mirroring the temporal pattern observed in the quantitative studies. The studies were concentrated in the United Kingdom (n = 9), followed by Finland (n = 2) and single contributions from Germany, Italy, and Sweden (Figure 2). Hence, the United Kingdom represented a total share of 38% (n = 88) across all reviewed studies, followed by Spain (n = 40; 17%).
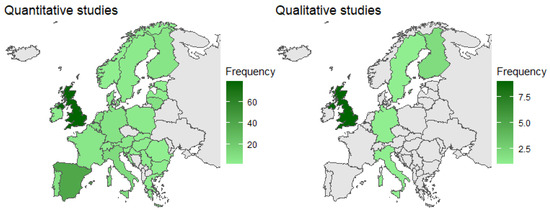
Figure 2.
Quantitative (left map) and qualitative (right map) studies—Distribution of the reviewed publications by country.
3.2. Ecosystems and NbS
The reviewed quantitative studies spanned multiple ecosystem types, with urban ecosystems most frequently studied (n = 81). Forest ecosystems were the second most studied (n = 31), followed by freshwater (n = 16) and coastal ecosystems (n = 15). Mountain (n = 10) and agriculture ecosystems (n = 9) appeared less often, while peri-urban (n = 7) and rural ecosystems (n = 7) were least represented (Figure 3). The qualitative studies showed similar trends, with urban environments being the most frequently represented (n = 9). Coastal and rural ecosystems appeared in four and five studies, respectively, followed by forests (n = 3), freshwater (n = 2), and mountain ecosystems (n = 1; Figure 4). Hence, urban ecosystems were studied in nearly half of all studies (n = 90; 45%), followed by forest and forestry (n = 40; 17%).
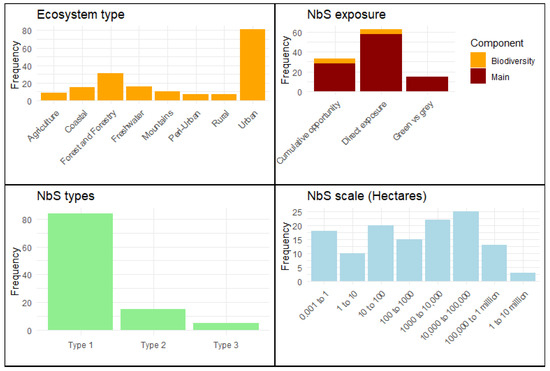
Figure 3.
Quantitative studies—frequency of ecosystem type, NbS exposure, NbS types and NbS scale found in the reviewed literature. Clockwise from top left: (1) Ecosystem types: frequencies indicate the number of quantitative studies focusing on each ecosystem type. (2) NbS exposure: (i) cumulative opportunity: studies assessing the aggregated potential for exposure to NbS over time or across different locations; (ii) direct exposure: studies where participants have immediate and firsthand interaction with NbS; (iii) green vs grey: comparative studies between nature-based (green) solutions and conventional (grey) infrastructure; and (iv) biodiversity component: within both direct exposure and cumulative opportunity, a subset of studies specifically emphasises biodiversity-related interventions. (3) NbS types: NbS initiatives are classified based on the level of intervention [44]. (4) This category represents the spatial extent of NbS implementations measured in hectares. Total frequency in the figure does not equate to the total number of studies due to multi-attribution.
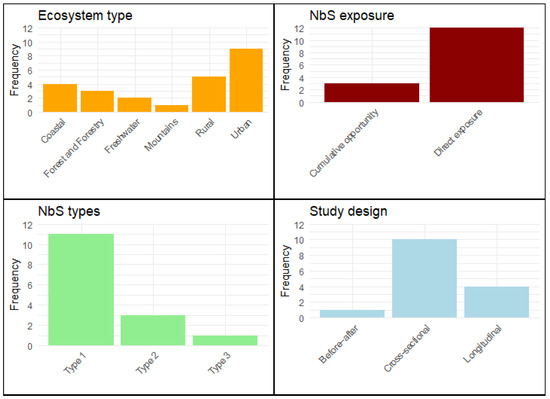
Figure 4.
Overview of the qualitative studies included in this review, showing the frequency of ecosystem types, NbS exposure, NbS types and study designs. Clockwise from top left: (1) Ecosystem types: frequencies indicate the number of qualitative studies focusing on each ecosystem type. (2) NbS exposure: (i) cumulative opportunity: studies assessing the aggregated potential for exposure to NbS over time or across different locations; (ii) direct exposure: studies where participants have immediate and firsthand interaction with NbS. (3) NbS types: NbS initiatives are classified based on the level of intervention [44]. (4) The study design depicts the frequency of research designs employed in the studies: (i) before–after studies compare health outcomes before and after the NbS intervention; (ii) cross-sectional studies, i.e., focus on a population at a single point in time; and (iii) longitudinal studies track the same participants over a time period. Total frequency in the figure does not equate to total number of studies due to multi-attribution.
Direct exposure, where research participants immediately interact with NbS, was the most common data collection method across both quantitative and qualitative studies (n = 70; 56%). Cumulative opportunity studies, which assess aggregated exposure potential over time or space, accounted for nearly 25% (n = 31). Comparisons of green vs. grey, which contrasts exposure to nature with built-up environments, appeared in 12% of all studies. Biodiversity-specific analyses were rare, with only 5% (n = 5) in each of the cumulative and direct exposure categories.
Across both types of studies, the most common NbS interventions were Type 1 (80%; n = 95). Type 2 interventions represented 15% (n = 18), while Type 3 interventions were least common (5%, n = 6).
For qualitative studies, NbS implementation scales varied widely, ranging from community gardens (<1 ha) to national parks and coastlines exceeding 10 million ha. The most frequent size category was between 10,000 and 100,000 ha (n = 25), followed by 1000 to 10,000 ha (n = 22) and 10 to 100 hectares (n = 20). Smaller interventions (0.001–1 ha, n = 18) typically involved urban squares or garden plots, while very large-scale projects (1–10 million ha, n = 3) were rare. Similarly, for qualitative studies, NbS ranged from small garden spaces and vegetation structures under 0.1 hectares to extensive countryside districts spanning nearly 190,000 hectares. Smaller scales included individual gardens, allotment gardens, and vegetation structures, which range from 0.0377 to 0.405 hectares. Medium-sized interventions, such as blue spaces and green trails, span 5.75 to 21 hectares, providing accessible natural areas within urban or suburban landscapes. Larger-scale NbS included parks, beaches, and coastal areas, with sizes from 360 hectares for woodland parks and up to 6035 hectares for beaches.
3.3. Methodology Used in the Studies
Across both quantitative and qualitative studies, cross-sectional study designs dominated (60%; n = 75), with before–after studies comprising 18% (n = 22). Longitudinal studies also accounted for 18% (n = 22) of studies, and quasi-experimental designs were least common (5%; n = 6). Adults (18+) were the primary focus (58%; n = 76), while children and elderly populations each appeared in 10% (n = 13) and 11% (n = 15), respectively, of studies. Studies of general populations represented 11% (n = 15), and 10% (n = 13) targeted NbS visitors specifically.
For quantitative studies, sample sizes varied widely, with the largest group of studies (n = 48) having between 1000 and 10,000 participants, followed by 100 to 1000 (n = 40). Large-scale studies (with more than 100,000 participants) were rare (n = 7).
3.4. Health Outcomes Measures
The impact of NbS interventions on mental health was examined more frequently than physical health across the reviewed literature. Panel A (Quantitative studies; Figure 5) illustrates the distribution of physical health outcomes reported. The most commonly examined outcome was general health (n = 20), encompassing health measures such as physical functioning (e.g., arm curls, chair stands), physical activity levels, and musculoskeletal pain. The circulatory system was the second most studied category (n = 11), focusing on cardiovascular metrics, including blood pressure, heart rate, and risks for hyper- or hypotension. Other categories included mortality and morbidity (n = 8), endocrine, nutritional, or metabolic (ENM) diseases (n = 6), and the respiratory system (n = 6), including factors such as diabetes, cholesterol, vitamin D levels, asthma, and overall respiratory health. Less frequently studied outcomes included the immune system (n = 2; allergies) and the digestive system (n = 1; gastroenteritis risks).
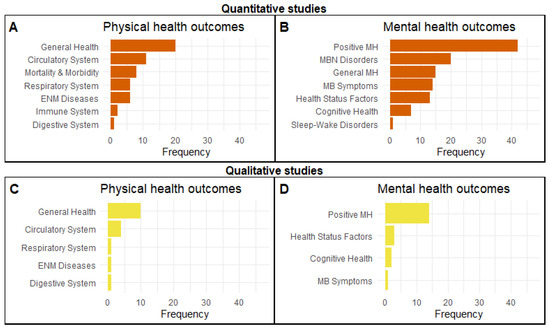
Figure 5.
Comparative analysis of health outcome categories from quantitative and qualitative studies, arranged in a panel of four bar charts. Each chart displays the frequency of specific physical or mental health outcomes identified in the reviewed literature. Abbreviations are: (A,C) ENM Diseases: endocrine, nutritional, and metabolic (ENM) diseases; (B,D) Positive MH: positive mental health (MH), MB symptoms: mental and behavioural (MB) symptoms and MBN disorders: mental, behavioural or neurodevelopmental (MBN) disorders. Total frequency in the figure does not equate to the total number of studies due to multi-attribution.
Indicators used to assess the impact of NbS on physical health outcomes spanned hospital records (e.g., respiratory admissions, mortality rate), physiological measures (e.g., blood pressure, heart rate variability), and validated psychometric scales such as the 12-Item Short Form Health Survey (SF-12) and International Study of Asthma and Allergies in Childhood (ISAAC). Other common approaches included medication sales or self-reported data on conditions such as hypertension, gastroenteritis, or general health. Several studies also included lifestyle and developmental health outcomes such as Body Mass Index (BMI), birth weight, and screen time, while others assessed disease metrics such as colon and breast cancer incidence and type 2 diabetes.
Figure 5B outlines the distribution of mental health outcomes studied in the quantitative studies. The most common health outcomes were positive mental health (n = 42), which encompassed general well-being, mindfulness, life satisfaction, and self-esteem, often using validated scales (around 50% of studies) such as the Warwick–Edinburgh Mental Well-being Scale (WEMWBS), World Health Organization-Five Well-Being Index (WHO-5), and the Rosenberg Self-Esteem Scale (RSE). Other commonly studied outcomes included mental and behavioural (MB) symptoms (n = 14), which assessed mood, fatigue, and affect, using validated scales such as the Profile of Mood States (POMS), Positive and Negative Affect Schedule (PANAS), General Mental Health (n = 15), General Health Questionnaire-12 (GHQ-12), and 36-Item Short Form Health Survey (SF-36). Additionally, mental, behavioural, and neurodevelopmental (MBN) disorders were examined in 20 studies, covering outcomes such as anxiety, depression, attention deficit hyperactivity, and autism spectrum disorders. Factors influencing health status (i.e., health status factors, n = 13) included indicators such as perceived stress levels, cortisol profiles and the UCLA Loneliness Scale. Finally, cognitive health was examined in seven studies, focusing on attention, memory, and cognitive performance, whereas sleep–wake disorders were the least represented (n = 1), indicating a limited focus on sleep-quality improvements associated with NbS in Europe.
For qualitative studies (Figure 5C,D), the most frequently reported physical health outcomes related to general health (e.g., physical fitness, pain relief, physical strain and headaches, n = 10) and the circulatory system (e.g., cardiovascular fitness, heartbeat, blood pressure, n = 4). Limited attention was given to the digestive system (e.g., gastrointestinal haemorrhage), respiratory system, and endocrine, nutritional, and metabolic diseases (e.g., cholesterol levels). Similar to quantitative studies, positive mental health was the most commonly studied health outcome (n = 14), while fewer studies addressed cognitive health (n = 2), factors affecting health status (reduced stress, anxiety and negative feelings, n = 3) and mental and behavioural symptoms (i.e., improved mood).
3.5. NbS and Health Benefits
Across the 115 European studies, NbS suggest evidence of positive associations with both physical and mental health. Consistent with other systematic reviews (e.g., [4,66]), our findings show that exposure to NbS is associated with improved general health, cardiovascular profiles and reduced risks of anxiety and depression. Growing up in neighbourhoods with lush vegetation was linked with a lower risk of psychiatric disorders later in life [92]. Across Belgium, more woodland canopy cover was associated with lower sales of mood-disorder medications [93]. Woodlands and pocket parks were perceived as “mentally restorative refuges” that help reduce stress [94]. Forest therapy, even a single session, was linked to reduced tension, depression and anxiety among psychiatric inpatients [95], while brief visits to urban woodlands lowered heart-rate variability indicators of stress in Finnish women [96]. In the UK, trail runners described the act of running in nature as a way to shed urban stress and “feel more alive” [97]. Finnish university students likened outdoor recreation amenities to a “reset button”, reporting calmer moods and sharper concentration after breaks in nature [98], while therapeutic horticulture gardens eased anxiety and improved self-esteem for some in the UK [99]. The benefits of horticultural programmes were attributed to the social support embedded in routine gardening tasks.
NbS interventions were frequently linked to increased physical activity. Six months after the Connswater Community Greenway was built in Belfast, residents living within a mile of the riverside park reported an average increase of 36 min per week in moderate-to-vigorous activity and small but significant BMI reductions [100]. Similarly, the Chopwell Wood referral project in North-East England found that woodland walks and conservation tasks helped participants with obesity, diabetes and low fitness to become regularly active [101]. For people with disabilities, the countryside offered empowering experiences. Visually impaired walkers highlighted fresh air and supportive group banter as key to both physical confidence and weight control [102]. Moreover, proximity to green space was repeatedly linked to cardiovascular health benefits. Residents living within 300 m of parks had significantly lower odds of hypertension [103], and regular park users experienced a 30–50% lower hazard of fatal and non-fatal cardiovascular disease over four years [104].
Rivers, canals or beaches provide good health benefits. For instance, German visitors reported stronger restorative feelings and decreases in blood pressure in freshwater ecosystems, compared to equally green parks [105]. A UK coastal study found that beaches and estuaries carry “time-deepened” emotional significance, especially for low-income and minority residents, making them powerful places for social inclusion as well as mental refreshment [106]. In Spain, beach users reported significantly greater psychological restoration and stress recovery compared to park visitors [107]. Furthermore, living within 1 km of the coast predicted better self-rated general health, partly explained by outdoor physical activity such as walking and water sports [108].
The reviewed evidence indicates that health benefits from NbS are mediated through fostering social interactions. For instance, garden projects created social settings that participants described as “as healing as the plants themselves”, resulting in higher life satisfaction [99,109]. In a four-city European study, time spent in parks predicted better mental health partly through reduced loneliness and stronger neighbourhood social cohesion [110]. Trail-running communities viewed protected landscapes as arenas for collective adventure and environmental care [97], while visually impaired walkers valued countryside hikes both for exercise and the sense of belonging fostered by group activities [102]. In Finland, respondents ranked “shared moments with family and friends outdoors” above solitude as their top well-being gain from ecosystems [111]. Workplace greening around London’s Victoria Station increased informal staff interaction and morale, offering firms an economic as well as well-being benefit [112].
3.6. Negative Health Impacts from Exposure to NbS
Despite these benefits, several quantitative studies reported negative impacts on both physical (n = 6) and mental health (n = 5) outcomes, especially for certain groups with allergies. For instance, two studies [113] identified increased asthma prevalence associated with living close to grassy areas and residential gardens. High grass cover, particularly in urban parks, was linked to a 60% higher prevalence of asthma [114], likely due to allergens. Another study found that higher stem density in green spaces was associated with a 20–24% increase in cardiovascular medication usage, potentially due to pollen release or increased particulate matter [115]. Risks such as skin cancer from prolonged sun exposure were noted when outdoor activities occurred in open green spaces without adequate shade or sun protection measures [116]. Dense vegetation was also linked to increased mood disorder medication sales (28 to 32%), possibly due to feelings of enclosure or reduced air quality [115]. Increased daytime noise levels in popular recreation areas were associated with higher annoyance if there are too many people visiting the place, reducing restorative quality [117]. Aesthetic choices, such as brightly coloured plants, were perceived by some as less relaxing than subtler green foliage, which might detract from the tranquillity typically sought in nature [52]. Finally, while gardening was found to be generally beneficial to health, some participants reported stress related to maintenance tasks such as weeding, which can be challenging for individuals with limited time or physical capacity [118].
For qualitative studies, no negative health impacts of NbS were reported in relation to physical health outcomes. However, some studies noted negative mental health impacts. These included time pressure to be outdoors in nature, stress related to garden maintenance (e.g., weeds, pests) and conflicts with neighbours and family members [119,120]. All health benefits were assessed using self-reported and perceived health outcome data.
3.7. Economic Valuation and Assessment Studies
Out of the 101 quantitative studies, only 10 included an economic valuation of health benefits associated with NbS implementation, primarily using avoided cost (e.g., reduced mortality/hospitalisations) and cost–benefit analysis methods focused on urban green or blue infrastructure and air quality.
All reviewed studies identified health-related cost savings from NbS implementation. For example, a large-scale green infrastructure plan was proposed for Rome aimed at reducing PM10 (particulate matter with diameter ≤ 10 µm) concentrations, estimating annual health-related cost savings of €71,200–€228,100 [121]. Similarly, a UK study valued pollutant removal by urban green and blue spaces, including PM2.5, NO2, SO2, and O3, at €194 million/year [122]. These cost savings reflected reductions in hospital admissions, mortality, and life years lost.
Another UK study estimated that woodland absorption of SO2 and PM10 prevented 5–7 deaths and 4–6 hospital admissions annually, which translated into cost savings of €29,000–€1.53 million/year [123]. Two studies [124,125] in Barcelona examined urban planning interventions. The superblock model, an urban and transport planning strategy, was estimated to prevent 667 premature deaths per year through lower NO2 levels and reduced noise and heat exposure, with an economic impact of €2.24 billion annually. The Eixos Verds Plan, designed to expand urban greenery, was estimated to save €50.1 million per year by reducing depression cases and associated healthcare costs. Physical-activity-related outcomes were also highlighted in the reviewed studies. For instance, a cost–benefit analysis of hiking trails in Berguedà (Spain) estimated annual health savings of €19,500 from reduced cardiovascular risk [126], while a regenerated riverside park in Spain was linked to mortality reductions valued at €18.4–€27.8 million annually, depending on attribution scenarios (i.e., one where 100% of physical activity is linked to the park and one where 50% is attributed to the park) [127]. A Portuguese study [128] assessed the economic burden of poor beach water quality, estimating gastroenteritis-related annual costs of approximately €14–€38 million [129].
Mental health valuations were explored in two UK studies. Cox et al. [130] projected that achieving minimal neighbourhood vegetation cover could reduce annual costs by up to €1.13 billion for depression and €5.88 billion for anxiety. Pretty et al. [131] examined ten green exercise case studies, noting that the National Health Service spends €10.1 billion per year on treating mental illness and social services, which suggests substantial potential savings through nature-based activities.
3.8. Vulnerable Social Segments and Climate Change
Some quantitative studies (n = 32) addressed the differential impact of NbS on vulnerable populations, including children, the elderly, and socioeconomically disadvantaged groups. For example, proximity to green spaces was linked to better cognitive function and fewer behavioural issues in children [132,133,134,135], while green and blue spaces reduced heat-related mortality among the elderly [136,137]. Some studies also explored the mental health benefits for low-income or socioeconomically disadvantaged groups (e.g., ethnic minorities, people with disabilities, the unemployed [115,131,138,139,140,141,142,143]. One study highlighted that typically, disadvantaged groups have a lower baseline “nature dose,” so increases in nearby nature produced larger absolute improvements in well-being [140]. Urban woodland improvement in deprived areas led to increased visits and better self-reported quality of life [142]. Similarly, local greening interventions such as horticultural interventions or street trees were associated with reduced perceived stress and improvements in self-reported health for residents, particularly for residents unable to travel to larger parks [139].
A small number of qualitative studies (n = 4) examined the physical (e.g., perceived cardiovascular health) and mental health (e.g., psychological well-being, relaxation, peace) outcomes associated with NbS such as beaches, gardens, vegetation and other urban green spaces on vulnerable groups. These included the elderly [120,144,145], children [146], residents of deprived areas [119], the unemployed, individuals with existing mental health issues, learning difficulties, or experiences of social isolation [119]. These studies have found that green and blue spaces can confer health benefits such as improved cognition to children, reduced heat mortality among the elderly, and improved mental health outcomes and social equity for disadvantaged populations. For instance, Milligan et al. [144] explored communal gardening among older people in northern England and found that allotment sites functioned as “therapeutic landscapes” where participants reported improved emotional well-being. However, evidence indicates that the physical limitations associated with ageing may require additional support to enable continued engagement in these activities. Ashbullby et al. [146], through interviews with families in a coastal region, found that beach environments encouraged physical activity among children and positive parent–child interactions that supported both physical and mental health. O’Brien et al. [145] used observational and self-reported data to show that environmental volunteering boosted self-esteem, expanded social networks and provided a sense of purpose among marginalised adults. One study from Rome [147] analysed the effects of park exposure on adults’ general physical and mental health, including stress reduction, fun, and relaxation. Notably, more than a third of participants (34%) believed that green areas play a significant role in climate adaptation and mitigation, such as managing heat waves and improving air quality.
Only three quantitative studies explored how NbS mitigate urban stressors such as heat, air pollution, and noise. One study [136] found that vegetation and water bodies, even at a distance, help to mitigate heat-related mortality among the elderly in Lisbon. Another study [141] described how Milan implemented NbS, including green walls, embankments and noise barriers at a railway stop, to lessen heat, noise and flooding. A third study [137] used spatial modelling to show that green roofs can lower indoor temperatures by 1.5–3 °C in four European cities, reducing heat-related mortality.
4. Discussion
While interest in NbS has grown significantly in recent years, research explicitly examining their links to human health remains relatively limited. The analysis revealed that NbS research has primarily concentrated on climate change impacts on cities and biodiversity loss, while human health remains a marginal concern within the broader landscape of societal challenges addressed by NbS studies [148]. Our systematic review shows a notable rise in publications occurred after 2016, coinciding with growing awareness of the term ‘nature-based solutions’ [149]. The peak in publications was in 2020, with many (n = 23) studies, possibly reflecting an increased focus on public health and the natural environment during the COVID-19 pandemic [150]. These trends may indicate a continued need for further research into the relationship between NbS and health.
4.1. Geographical Coverage
Both quantitative and qualitative types of studies covered a wide range of European countries. However, we revealed a strong bias of the evidence towards Western Europe, with countries such as the UK and Spain being strongly over-represented. In contrast, we identified a lack of studies from Eastern and Southern Europe, with some upper–middle-income countries such as Albania, Bosnia and Herzegovina, Montenegro and Ukraine remaining entirely unstudied. High-income countries such as Andorra, Cyprus, Iceland and Malta were also not featured in the reviewed studies [151]. Given the highly context-dependent relationship between NbS and health, shaped by the socioenvironmental characteristics of a given area [152], we recommend that future research addresses the geographical bias towards Western Europe. This is particularly important given that cities in Northern and Western Europe generally have more greenspace compared to Southern and Eastern Europe [153], which may contribute to existing health inequalities within Europe [154]. However, we must note that the search string only captured publications in English, and this may also be a reason due to their lack of representation.
4.2. NbS and Ecosystems
Nearly half of the included studies examined urban ecosystems, while other ecosystem types such as forests, coastal and freshwater ecosystems, agriculture, mountain ecosystems, protected areas, and peri-urban and rural ecosystems were examined much less frequently in relation to health outcomes. This concentration on urban ecosystems likely mirrors continuing global urbanisation trends and the growing interest in addressing associated health and environmental challenges [155]. As of 2020, approximately 73% of Europeans lived in urban areas, reflecting decades of urban growth that channels research and policy attention toward cities [156]. The limited attention to non-urban ecosystem types (e.g., mountains, freshwater and forests) is concerning, as these settings may provide equally important pathways to human health. Limited understanding of their contributions risks missing opportunities to enhance health benefits derived from these ecosystems. Future research should therefore focus more on these under-represented ecosystem types.
Direct exposure to NbS was the most frequently employed approach to measure health effects, followed by cumulative opportunity studies and green vs. grey evaluations. Surprisingly, only a few studies examined exposure to biodiversity. This is notable given the growing recognition that biodiverse NbS may offer additional health benefits compared to less diverse spaces [45,46,49,50,157]. Previous reviews have highlighted important research gaps in this area [53,158], which may reflect a lack of appropriate methodological tools to assess links between biodiversity and health.
Our analysis of both quantitative and qualitative studies reveals a clear imbalance in research attention across different types of NbS, with Type 1 interventions dominating the literature. Type 1 NbS involve minimal or no intervention in ecosystems, aiming to preserve or improve the delivery of ecosystem services. This focus on Type 1 studies may reflect the relative ease of implementing and studying these NbS, as well as their alignment with broader conservation priorities. In contrast, Type 2 and Type 3 interventions were substantially under-represented, despite their potential to offer targeted solutions in more intensively managed or urbanised landscapes [44]. This leaves critical gaps in understanding their health-related impacts. The scarcity of studies on Type 3 NbS, which involve highly intrusive management or the creation of entirely new ecosystems, is particularly striking. These interventions, such as constructed wetlands or green roofs, have substantial potential to address specific urban health challenges such as air pollution, urban heat islands, and stormwater management [159]. However, their complexity, higher implementation costs, and the difficulty of measuring long-term health impacts may explain their limited presence in the literature. This imbalance in NbS type representation has important implications for both policy and practice. While the focus on Type 1 interventions provides important insights into the health benefits of conserving natural ecosystems, it may limit our understanding of how more intensive management or newly created ecosystems can contribute to human health. This is particularly relevant in urban environments, where Type 2 and Type 3 interventions could play a crucial role in mitigating health risks and improving urban resilience [160]. Hence, research should prioritise less-represented NbS types, i.e., Type 3 or intensively managed landscapes across different ecosystem types, to develop a better understanding of their health benefits [161].
In terms of scale, both types of studies focused on intermediate scales (10,000–100,000 ha) of NbS implementation, which appear to be large enough to identify measurable health impacts while maintaining manageable study boundaries. This supports findings from Fuller & Gaston [162], who showed that green space coverage in European cities scales non-linearly with urban area, suggesting that intermediate-scale interventions may offer the best return for health outcomes. In contrast, larger-scale studies (more than 100,000 ha) were relatively few, representing a gap in understanding how broader landscape-level NbS affect health. This is concerning, given the growing emphasis on scaling NbS interventions (such as national parks and forest networks) beyond the local level, perhaps leading to health benefits through their impact on air quality and climate regulation [163].
4.3. Study Design
Most studies employed cross-sectional study designs (63%). This bias limits our understanding of long-term effects and causal relationships, as noted by Kabisch et al. [164], who highlighted the need for more longitudinal studies in NbS research to capture temporal dynamics and long-term changes in health. The under-representation of experimental and quasi-experimental designs is concerning, as these methods are crucial for establishing causal links between NbS interventions and health outcomes. This gap echoes findings by Raymond et al. [161], who emphasised the importance of robust experimental designs in evaluating NbS effectiveness. The focus on adult populations (55%) while children and elderly groups were less studied suggests a potential bias in understanding NbS health impacts across different life stages and on vulnerable groups. This imbalance may limit our understanding of how NbS health impacts vary across age groups, an aspect highlighted as critical by Frumkin et al. [165].
4.4. Associations Between NbS and Human Health
The systematic review shows that NbS can have positive associations with physical and mental health. However, there is a stronger focus on readily quantifiable indicators such as blood pressure, BMI and self-reported well-being, while more complex physiological and psychological pathways, including immune and endocrine responses, cognitive function, and long-term disease prevention, remain under-represented [165,166]. Additionally, understanding the mediators through which NbS impact health is essential for explaining causal mechanisms and designing relevant policies. Most studies primarily focused on physical activity, air quality improvement, and stress reduction, while few quantify the role of social cohesion, environmental aesthetics, biodiversity or sense of place, despite growing evidence that these social–cultural dimensions can influence mental health and resilience [46,167].
Further research is needed to clarify the underlying mechanisms linking biodiversity to health outcomes [168]. Research frequently relies on subjective perceptions of biodiversity rather than objective ecological measures. While there is evidence suggesting that perceived biodiversity, rather than actual biodiversity, plays a stronger role in influencing health outcomes, our understanding of how actual biodiversity contributes to these outcomes remains limited [168]. Most studies are also concentrated in urban or high-income settings, leaving substantial gaps in how biodiversity–health relationships manifest in rural areas, low-income regions, or culturally diverse populations [168]. Additionally, the complex interplay between biodiversity loss, climate change, and emerging infectious diseases remains poorly understood [169]. The role of biodiversity in addressing urban health inequalities is particularly underexplored. For instance, access to biodiverse NbS may differ across socioeconomic groups, influencing disparities in health outcomes [168]. Addressing these gaps will require the development of standardised methodologies for assessing biodiversity and its health effects. For instance, psychometric tools specifically designed to measure biodiversity–health relationships, such as the BIO-WELL scale developed in the UK [49,157], may provide a foundation for more consistent and robust research in this field.
While NbS can deliver substantial health benefits, some studies also reported negative health impacts from their implementation. The association between grassy areas and increased asthma prevalence is particularly concerning given that climate change is making pollen seasons longer and more intense [170]. Current evidence suggests that approximately 40% of the European population have pollen allergies, making this a substantial public health consideration [171]. However, most epidemiological studies investigating greenspace health effects have not considered plant species composition or allergenic potential [172]. Moreover, engaging with nature included feelings of enclosure, loneliness, or stress from garden upkeep. These findings highlight that experiences of nature are shaped by personal and contextual factors, highlighting the need for human-centred design in NbS implementation. Incorporating the needs and perceptions of local communities, including under-represented groups, can help ensure that such interventions enhance well-being rather than inadvertently contributing to stress or exclusion [173,174].
Furthermore, we currently lack robust estimates of the economic value of health benefits of NbS due to the limited number of studies. This is particularly concerning given the substantial costs associated with poor health and environmental degradation. For instance, Europe faces annual losses of €166 billion from air pollution and €600 billion from the costs of mental ill-health [175]. Moreover, existing valuations tend to focus on outcomes such as improved air quality and mortality reduction.
4.5. Study Population Groups
Much of the reviewed evidence of NbS health impacts on vulnerable social segments was observational, where causality is often inferred rather than directly established. This limits the strength of the conclusions that can be drawn. Moreover, the magnitude and direction of effects vary depending on the type, quality, and accessibility of green or blue space, as well as the specific health outcomes measured. Lower-income areas often have less access to green space, a “luxury effect” that limits benefits for those most at risk [176]. Similarly, the elderly may face barriers due to isolation or limited mobility [177]. These findings echo the literature which indicates that vulnerable groups can disproportionately benefit from NbS [55,56]. Cities like Victoria-Gasteiz and Oslo, which guarantee nature access within 300 m for all residents, offer models for fair implementation [178]. This highlights the need for more rigorous, longitudinal, and experimental research designs to better understand causal pathways and to identify which types of nature exposure are most beneficial for vulnerable populations. Future research is also called for to broaden economic valuation approaches to capture the economic value of a wider range of health outcomes, including mental health, social cohesion, and preventive healthcare savings [179,180].
4.6. Limitations
This systematic review provides a stocktake of evidence of the relationship between NbS and human health in Europe. However, we recognise that it has some limitations. First, the search covered only two databases, which means that we may have missed relevant studies from other relevant databases. Future studies, therefore, may extend their search to a larger diversity of literature databases. Second, due to marked heterogeneity across the 115 studies, no formal risk-of-bias assessment was conducted; all studies meeting inclusion criteria received equal descriptive weight in the narrative synthesis. This omission means low-quality studies may disproportionately influence results. Finally, the fact that many of the reviewed studies employed observational research designs highlights the risk of reverse causality, meaning that healthier people may seek out NbS. It also results in an elevated risk of residential self-selection, i.e., people choose NbS-rich areas, and residual confounding, i.e., unmeasured factors like socioeconomic background. These biases causal claims, highlighting the need for more experimental studies, precisely the gaps our review highlights. Nevertheless, our review highlights some key gaps to guide future research and policy efforts in environmental science and public health.
5. Conclusions
Our systematic review of 115 European studies shows that NbS are associated with better mental health, improved general health and cardiovascular health. Evidence spans urban parks, forests, gardens, street trees and blue spaces, amongst others. These benefits are mostly concentrated in Western Europe, frequently detected for proximal, everyday exposures and observed where access is easy. However, the evidence is methodologically imbalanced. Studies overwhelmingly assess Type 1 NbS and rely on cross-sectional designs and self-reported outcome measures, while Type 2 and 3 NbS in urban retrofits and longitudinal or quasi-experimental evidence remain scarce. Moreover, we identified negative health impacts, including allergenic pollen loads, perceived enclosure, noise, UV exposure and gardening maintenance-related stress.
Despite this growing evidence base, several important gaps persist. Current research rarely differentiates among NbS types or dosage (e.g., urban parks versus coastal environments), and causal pathways remain poorly understood. Questions of equity are critical, as certain population segments face barriers to meaningful nature engagement. Addressing these gaps will require longitudinal, interdisciplinary research and policy frameworks that prioritise ecological integrity and equitable access to green and blue spaces [70,181]. Further work should also address the lack of economic valuation studies, the limited assessment of physical health outcomes, and the insufficient focus on vulnerable population groups.
We hope this systematic review can encourage researchers, planners, and policymakers to integrate health considerations more explicitly into NbS design and evaluation. Ultimately, greater investment in NbS may contribute to improved health and well-being for European populations while advancing biodiversity and climate resilience goals.
Supplementary Materials
The following supporting information can be downloaded at: https://www.mdpi.com/article/10.3390/environments13060300/s1, Table S1: Data extraction variables for quantitative and qualitative studies. This table lists the variables extracted from all included studies. When a single study reported multiple study designs, ecosystem types, or other relevant categories, each was coded separately to ensure that all information was accurately represented; Supplementary S1; Supplementary S2.
Author Contributions
Conceptualisation, D.C., M.N. and W.C.; methodology, D.C., M.N. and W.C.; validation, D.C., M.N., W.C., A.S., C.B., D.N., M.Z. and H.R.; formal analysis, D.C., M.N. and W.C.; investigation, D.C., M.N., W.C., A.S., C.B., D.N., M.Z. and H.R.; data curation, D.C., M.N., A.S. and C.B.; writing—original draft preparation, D.C. and M.N.; writing—review and editing, D.C., M.N., W.C., A.S., C.B., D.N., M.Z., H.R. and A.T.; visualisation, D.C.; supervision, W.C.; project administration, W.C., M.Z. and A.T.; funding acquisition, W.C., M.Z. and A.T. All authors have read and agreed to the published version of the manuscript.
Funding
This work has been funded by the European Union under the Horizon Europe grant 101061083 (Invest4Nature). Views and opinions expressed are, however, those of the author(s) only and do not necessarily reflect those of the European Union or the European Commission and its European Research Executive Agency (REA)—hereinafter referred to as the granting authority. Neither the European Union nor the granting authority can be held responsible for them.
Data Availability Statement
The original contributions presented in this study are included in the Supplementary Material. Further enquiries can be directed to the corresponding author.
Acknowledgments
The authors would like to thank Viktoria Kofler, Francesca Tedeschini, Nicole Margrethe Witt, Sigurd Linnehol, Christine Kamange and Shukur Abuduryim for their valuable support during data extraction and analysis, as well as Julián Eduardo Lozano Galindez, Elisa Fuchs, David Blaettner and Alison Bauer for their contributions to the screening stages of the systematic review.
Conflicts of Interest
The authors declare no conflicts of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
References
- United Nations. Department of Economic and Social Affairs, Population Division. In World Urbanization Prospects: The 2018 Revision (ST/ESA/SER.A/420); United Nations: New York, NY, USA, 2019. [Google Scholar]
- Eurostat Urban-Rural Europe—Demographic Developments in Cities. Available online: https://ec.europa.eu/eurostat/statistics-explained/index.php?title=Urban-rural_Europe_-_demographic_developments_in_cities (accessed on 17 December 2025).
- McPhearson, T.; Karki, M.; Herzog, C.; Fink, H.S.; Abbadie, L.; Kremer, P.; Clark, C.M.; Palmer, M.I.; Perini, K.; Dubbeling, M. Urban Ecosystems and Biodiversity. In Climate Change and Cities: Second Assessment Report of the Urban Climate Change Research Network; Rosenzweig, C., Solecki, W., Romero-Lankao, P., Mehrotra, S., Dhakal, S., Ibrahim, S.A., Eds.; Cambridge University Press: Cambridge, UK, 2018; pp. 257–318. [Google Scholar]
- Van Den Bosch, M.; Ode Sang, A. Urban Natural Environments as Nature-Based Solutions for Improved Public Health—A Systematic Review of Reviews—ScienceDirect. Environ. Res. 2017, 158, 373–384. [Google Scholar] [CrossRef]
- Budreviciute, A.; Damiati, S.; Sabir, D.K.; Onder, K.; Schuller-Goetzburg, P.; Plakys, G.; Katileviciute, A.; Khoja, S.; Kodzius, R. Management and Prevention Strategies for Non-Communicable Diseases (NCDs) and Their Risk Factors. Front. Public Health 2020, 8, 574111. [Google Scholar] [CrossRef]
- Beaglehole, R.; Bonita, R.; Horton, R.; Adams, C.; Alleyne, G.; Asaria, P.; Baugh, V.; Bekedam, H.; Billo, N.; Casswell, S.; et al. Priority Actions for the Non-Communicable Disease Crisis. Lancet 2011, 377, 1438–1447. [Google Scholar] [CrossRef] [PubMed]
- Global Burden of Disease Study 2013 Collaborators Global, Regional, and National Incidence, Prevalence, and Years Lived with Disability for 301 Acute and Chronic Diseases and Injuries in 188 Countries, 1990–2013: A Systematic Analysis for the Global Burden of Disease Study 2013. Lancet 2015, 386, 743–800. [CrossRef]
- WHO. Noncommunicable Diseases. Available online: https://www.who.int/news-room/fact-sheets/detail/noncommunicable-diseases (accessed on 17 December 2025).
- Franco, M.; Bilal, U.; Diez-Roux, A.V. Preventing Non-Communicable Diseases through Structural Changes in Urban Environments. J. Epidemiol. Community Health 2015, 69, 509–511. [Google Scholar] [CrossRef]
- Harrison, J.E.; Weber, S.; Jakob, R.; Chute, C.G. ICD-11: An International Classification of Diseases for the Twenty-First Century. BMC Med. Inform. Decis. Mak. 2021, 21, 206. [Google Scholar] [CrossRef]
- Ali, G.-C.; Ryan, G.; De Silva, M.J. Validated Screening Tools for Common Mental Disorders in Low and Middle Income Countries: A Systematic Review. PLoS ONE 2016, 11, e0156939. [Google Scholar] [CrossRef]
- WHO. Depression and Other Common Mental Disorders: Global Health Estimates; World Health Organization: Geneva, Switzerland, 2017. [Google Scholar]
- Moussavi, S.; Chatterji, S.; Verdes, E.; Tandon, A.; Patel, V.; Ustun, B. Depression, Chronic Diseases, and Decrements in Health: Results from the World Health Surveys. Lancet 2007, 370, 851–858. [Google Scholar] [CrossRef]
- GBD 2019 Diseases and Injuries Collaborators Global Burden of 369 Diseases and Injuries in 204 Countries and Territories, 1990–2019: A Systematic Analysis for the Global Burden of Disease Study 2019. Lancet 2020, 396, 1204–1222. [CrossRef]
- Whiteford, H.A.; Degenhardt, L.; Rehm, J.; Baxter, A.J.; Ferrari, A.J.; Erskine, H.E.; Charlson, F.J.; Norman, R.E.; Flaxman, A.D.; Johns, N.; et al. Global Burden of Disease Attributable to Mental and Substance Use Disorders: Findings from the Global Burden of Disease Study 2010. Lancet 2013, 382, 1575–1586. [Google Scholar] [CrossRef] [PubMed]
- Hankey, S.; Marshall, J.D.; Brauer, M. Health Impacts of the Built Environment: Within-Urban Variability in Physical Inactivity, Air Pollution, and Ischemic Heart Disease Mortality. Environ. Health Perspect. 2012, 120, 247–253. [Google Scholar] [CrossRef] [PubMed]
- Nieuwenhuijsen, M.; Nazelle, A.d.; Garcia-Aymerich, J.; Khreis, H.; Hoffmann, B. Shaping Urban Environments to Improve Respiratory Health: Recommendations for Research, Planning, and Policy. Lancet Respir. Med. 2024, 12, 247–254. [Google Scholar] [CrossRef]
- Grazuleviciene, R.; Andrusaityte, S.; Dėdelė, A.; Grazulevicius, T.; Valius, L.; Rapalavicius, A.; Kapustinskiene, V.; Bendokiene, I. Urban Environment and Health: A Cross-Sectional Study of the Influence of Environmental Quality and Physical Activity on Blood Pressure. Int. J. Environ. Res. Public Health 2021, 18, 6126. [Google Scholar] [CrossRef]
- Koolen, C.D.; Rothenberg, G. Air Pollution in Europe. ChemSusChem 2019, 12, 164–172. [Google Scholar] [CrossRef] [PubMed]
- Münzel, T.; Sørensen, M.; Daiber, A. Transportation Noise Pollution and Cardiovascular Disease. Nat. Rev. Cardiol. 2021, 18, 619–636. [Google Scholar] [CrossRef]
- WHO. Almost 600,000 Deaths Due to Air Pollution in Europe: New WHO Global Report. Available online: https://www.who.int/europe/news/item/25-03-2014-almost-600-000-deaths-due-to-air-pollution-in-europe-new-who-global-report (accessed on 17 December 2025).
- Marselle, M.R. Theoretical Foundations of Biodiversity and Mental Well-Being Relationships. In Biodiversity and Health in the Face of Climate Change; Marselle, M.R., Stadler, J., Korn, H., Irvine, K.N., Bonn, A., Eds.; Springer International Publishing: Cham, Switzerland, 2019; pp. 133–158. [Google Scholar]
- Stigsdotter, U.K.; Ekholm, O.; Schipperijn, J.; Toftager, M.; Kamper-Jørgensen, F.; Randrup, T.B. Health Promoting Outdoor Environments—Associations between Green Space, and Health, Health-Related Quality of Life and Stress Based on a Danish National Representative Survey. Scand. J. Public Health 2010, 38, 411–417. [Google Scholar] [CrossRef]
- White, M.P.; Alcock, I.; Wheeler, B.W.; Depledge, M.H. Would You Be Happier Living in a Greener Urban Area? A Fixed-Effects Analysis of Panel Data. Psychol. Sci. 2013, 24, 920–928. [Google Scholar] [CrossRef]
- Mavoa, S.; Davern, M.; Breed, M.; Hahs, A. Higher Levels of Greenness and Biodiversity Associate with Greater Subjective Wellbeing in Adults Living in Melbourne, Australia. Health Place 2019, 57, 321–329. [Google Scholar] [CrossRef]
- Roberts, H.; van Lissa, C.; Hagedoorn, P.; Kellar, I.; Helbich, M. The Effect of Short-Term Exposure to the Natural Environment on Depressive Mood: A Systematic Review and Meta-Analysis. Environ. Res. 2019, 177, 108606. [Google Scholar] [CrossRef] [PubMed]
- Gascon, M.; Sánchez-Benavides, G.; Dadvand, P.; Martínez, D.; Gramunt, N.; Gotsens, X.; Cirach, M.; Vert, C.; Molinuevo, J.L.; Crous-Bou, M.; et al. Long-Term Exposure to Residential Green and Blue Spaces and Anxiety and Depression in Adults: A Cross-Sectional Study. Environ. Res. 2018, 162, 231–239. [Google Scholar] [CrossRef]
- Yao, W.; Zhang, X.; Gong, Q. The Effect of Exposure to the Natural Environment on Stress Reduction: A Meta-Analysis. Urban For. Urban Green. 2021, 57, 126932. [Google Scholar] [CrossRef]
- Lovell, R.; Depledge, M.; Maxwell, S. Health and the Natural Environment: A Review of Evidence, Policy, Practice and Opportunities for the Future; Department for Environment, Food and Rural Affairs (Defra): London, UK, 2018.
- Ohly, H.; White, M.P.; Wheeler, B.W.; Bethel, A.; Ukoumunne, O.C.; Nikolaou, V.; Garside, R. Attention Restoration Theory: A Systematic Review of the Attention Restoration Potential of Exposure to Natural Environments. J. Toxicol. Environ. Health Part B 2016, 19, 305–343. [Google Scholar] [CrossRef]
- Barboza, E.P.; Cirach, M.; Khomenko, S.; Iungman, T.; Mueller, N.; Barrera-Gómez, J.; Rojas-Rueda, D.; Kondo, M.; Nieuwenhuijsen, M. Green Space and Mortality in European Cities: A Health Impact Assessment Study. Lancet Planet. Health 2021, 5, e718–e730. [Google Scholar] [CrossRef]
- Gailey, S. Changes in Residential Greenspace and Birth Outcomes among Siblings: Differences by Maternal Race. Int. J. Environ. Res. Public Health 2023, 20, 6790. [Google Scholar] [CrossRef]
- Rook, G.A. Regulation of the Immune System by Biodiversity from the Natural Environment: An Ecosystem Service Essential to Health. Proc. Natl. Acad. Sci. USA 2013, 110, 18360–18367. [Google Scholar] [CrossRef] [PubMed]
- Lachowycz, K.; Jones, A.P. Greenspace and Obesity: A Systematic Review of the Evidence. Obes. Rev. 2011, 12, e183–e189. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Y.; Bao, W.-W.; Yang, B.-Y.; Liang, J.-H.; Gui, Z.-H.; Huang, S.; Chen, Y.-C.; Dong, G.-H.; Chen, Y.-J. Association between Greenspace and Blood Pressure: A Systematic Review and Meta-Analysis. Sci. Total Environ. 2022, 817, 152513. [Google Scholar] [CrossRef] [PubMed]
- Odebeatu, C.C.; Darssan, D.; Revez, J.A.; Roscoe, C.; Do, P.; Reid, S.; Osborne, N.J. The Role of Greenspace in Vitamin D Status: Cross-Sectional, Observational Evidence from the UK Biobank. Int. J. Hyg. Environ. Health 2025, 264, 114502. [Google Scholar] [CrossRef]
- Jones, R.; Tarter, R.; Ross, A.M. Greenspace Interventions, Stress and Cortisol: A Scoping Review. Int. J. Environ. Res. Public Health 2021, 18, 2802. [Google Scholar] [CrossRef]
- Ccami-Bernal, F.; Soriano-Moreno, D.R.; Fernandez-Guzman, D.; Tuco, K.G.; Castro-Díaz, S.D.; Esparza-Varas, A.L.; Medina-Ramirez, S.A.; Caira-Chuquineyra, B.; Cortez-Soto, A.G.; Yovera-Aldana, M.; et al. Green Space Exposure and Type 2 Diabetes Mellitus Incidence: A Systematic Review. Health Place 2023, 82, 103045. [Google Scholar] [CrossRef]
- WHO. Closing the Gap in a Generation: Health Equity Through Action on the Social Determinants of Health—Final Report of the Commission on Social Determinants of Health. Available online: https://www.who.int/publications/i/item/WHO-IER-CSDH-08.1 (accessed on 17 December 2025).
- McNamara, C.L.; Balaj, M.; Thomson, K.H.; Eikemo, T.A.; Solheim, E.F.; Bambra, C. The Socioeconomic Distribution of Non-Communicable Diseases in Europe: Findings from the European Social Survey (2014) Special Module on the Social Determinants of Health. Eur. J. Public Health 2017, 27, 22–26. [Google Scholar] [CrossRef] [PubMed]
- Nesshöver, C.; Assmuth, T.; Irvine, K.; Rusch, G.; Waylen, K.; Delbaere, B.; Haase, D.; Jones-Walters, L.; Keune, H.; Kovacs, E.; et al. The Science, Policy and Practice of Nature-Based Solutions: An Interdisciplinary Perspective. Sci. Total Environ. 2017, 579, 1215–1227. [Google Scholar] [CrossRef]
- Cousins, J.J. Justice in Nature-Based Solutions: Research and Pathways. Ecol. Econ. 2021, 180, 106874. [Google Scholar] [CrossRef]
- European Commission, Directorate General for Research and Innovation. Towards an EU Research and Innovation Policy Agenda for Nature-Based Solutions & Re-Naturing Cities: Final Report of the Horizon 2020 Expert Group on “Nature Based Solutions and Re Naturing Cities”; European Comission: Luxembourg, 2015. [Google Scholar]
- Eggermont, H.; Balian, E.; Azevedo, J.M.N.; Beumer, V.; Brodin, T.; Claudet, J.; Fady, B.; Grube, M.; Keune, H.; Lamarque, P.; et al. Nature-Based Solutions: New Influence for Environmental Management and Research in Europe. GAIA—Ecol. Perspect. Sci. Soc. 2015, 24, 243–248. [Google Scholar] [CrossRef]
- Dallimer, M.; Irvine, K.N.; Skinner, A.M.J.; Davies, Z.G.; Rouquette, J.R.; Maltby, L.L.; Warren, P.H.; Armsworth, P.R.; Gaston, K.J. Biodiversity and the Feel-Good Factor: Understanding Associations between Self-Reported Human Well-Being and Species Richness. BioScience 2012, 62, 47–55. [Google Scholar] [CrossRef]
- Marselle, M.R.; Hartig, T.; Cox, D.T.C.; de Bell, S.; Knapp, S.; Lindley, S.; Triguero-Mas, M.; Böhning-Gaese, K.; Braubach, M.; Cook, P.A.; et al. Pathways Linking Biodiversity to Human Health: A Conceptual Framework. Environ. Int. 2021, 150, 106420. [Google Scholar] [CrossRef] [PubMed]
- Hough, R.L. Biodiversity and Human Health: Evidence for Causality? Biodivers. Conserv. 2014, 23, 267–288. [Google Scholar] [CrossRef]
- Fisher, J.C.; Nawrath, M.; Dallimer, M.; Irvine, K.N.; Davies, Z.G. Connecting Biodiversity and Human Wellbeing. In Routledge Handbook of Urban Biodiversity; Routledge: London, UK, 2023; p. 13. [Google Scholar]
- Irvine, K.N.; Fisher, J.C.; Bentley, P.R.; Nawrath, M.; Dallimer, M.; Austen, G.E.; Fish, R.; Davies, Z.G. BIO-WELL: The Development and Validation of a Human Wellbeing Scale That Measures Responses to Biodiversity. J. Environ. Psychol. 2023, 85, 101921. [Google Scholar] [CrossRef]
- Fuller, R.A.; Irvine, K.N.; Devine-Wright, P.; Warren, P.H.; Gaston, K.J. Psychological Benefits of Greenspace Increase with Biodiversity. Biol. Lett. 2007, 3, 390–394. [Google Scholar] [CrossRef] [PubMed]
- Wolf, L.J.; Ermgassen, S.Z.; Balmford, A.; White, M.; Weinstein, N. Is Variety the Spice of Life? An Experimental Investigation into the Effects of Species Richness on Self-Reported Mental Well-Being. PLoS ONE 2017, 12, e0170225. [Google Scholar] [CrossRef]
- Hoyle, H.; Hitchmough, J.; Jorgensen, A. All about the “Wow Factor”? The Relationships between Aesthetics, Restorative Effect and Perceived Biodiversity in Designed Urban Planting. Landsc. Urban Plan. 2017, 164, 109–123. [Google Scholar] [CrossRef]
- Marselle, M.R.; Martens, D.; Dallimer, M.; Irvine, K.N. Review of the Mental Health and Well-Being Benefits of Biodiversity. In Biodiversity and Health in the Face of Climate Change; Marselle, M.R., Stadler, J., Korn, H., Irvine, K.N., Bonn, A., Eds.; Springer International Publishing: Cham, Switzerland, 2019; pp. 175–211. [Google Scholar]
- Marmot, M.; Allen, J.; Goldblatt, P.; Boyce, T.; McNeish, D.; Grady, M.; Geddes, I. Fair Society, Healthy Lives: The Marmot Review: Strategic Review of Health Inequalities in England Post-2010; UCL Institute of Health Equity: London, UK, 2010. [Google Scholar]
- McEachan, R.R.C.; Yang, T.C.; Roberts, H.; Pickett, K.E.; Arseneau-Powell, D.; Gidlow, C.J.; Wright, J.; Nieuwenhuijsen, M. Availability, Use of, and Satisfaction with Green Space, and Children’s Mental Wellbeing at Age 4 Years in a Multicultural, Deprived, Urban Area: Results from the Born in Bradford Cohort Study. Lancet Planet. Health 2018, 2, e244–e254. [Google Scholar] [CrossRef]
- Mitchell, R.; Popham, F. Effect of Exposure to Natural Environment on Health Inequalities: An Observational Population Study. Lancet 2008, 372, 1655–1660. [Google Scholar] [CrossRef]
- Barron, S.; Rugel, E. Tolerant Greenspaces: Designing Urban Nature-Based Solutions That Foster Social Ties and Support Mental Health among Young Adults. Environ. Sci. Policy 2023, 139, 1–10. [Google Scholar] [CrossRef]
- Atkinson, G.; Mourato, S. Cost-Benefit Analysis and the Environment; OECD Environment Working Papers: Tokyo, Japan, 2015; Volume 97. [Google Scholar]
- Hands, A.; Stimpson, A.; Ridgley, H.; Petrokofsky, C. Improving Access to Greenspace A New Review for 2020; Public Health England: London, UK, 2020.
- van den Bosch, M. Urban Green Spaces and Health—A Review of Evidence; WHO: Geneva, Switzerland, 2016. [Google Scholar]
- Dzhambov, A.M.; Dimitrova, D.D. Urban Green Spaces’ Effectiveness as a Psychological Buffer for the Negative Health Impact of Noise Pollution: A Systematic Review. Noise Health 2014, 16, 157–165. [Google Scholar] [CrossRef]
- Gascon, M.; Triguero-Mas, M.; Martínez, D.; Dadvand, P.; Rojas-Rueda, D.; Plasència, A.; Nieuwenhuijsen, M.J. Residential Green Spaces and Mortality: A Systematic Review. Environ. Int. 2016, 86, 60–67. [Google Scholar] [CrossRef] [PubMed]
- Hartig, T.; Mitchell, R.; de Vries, S.; Frumkin, H. Nature and Health. Annu. Rev. Public Health 2014, 35, 207–228. [Google Scholar] [CrossRef]
- Lovell, R.; Husk, K.; Bethel, A.; Garside, R. What Are the Health and Well-Being Impacts of Community Gardening for Adults and Children: A Mixed Method Systematic Review Protocol. Environ. Evid. 2014, 3, 20. [Google Scholar] [CrossRef]
- Tzoulas, K.; Korpela, K.; Venn, S.; Yli-Pelkonen, V.; Kaźmierczak, A.; Niemela, J.; James, P. Promoting Ecosystem and Human Health in Urban Areas Using Green Infrastructure: A Literature Review. Landsc. Urban Plan. 2007, 81, 167–178. [Google Scholar] [CrossRef]
- Twohig-Bennett, C.; Jones, A. The Health Benefits of the Great Outdoors: A Systematic Review and Meta-Analysis of Greenspace Exposure and Health Outcomes. Environ. Res. 2018, 166, 628–637. [Google Scholar] [CrossRef]
- Reyes-Riveros, R.; Altamirano, A.; De La Barrera, F.; Rozas-Vásquez, D.; Vieli, L.; Meli, P. Linking Public Urban Green Spaces and Human Well-Being: A Systematic Review. Urban For. Urban Green. 2021, 61, 127105. [Google Scholar] [CrossRef]
- Nieuwenhuijsen, M.J. Green Infrastructure and Health. Annu. Rev. Public Health 2021, 42, 317–328. [Google Scholar] [CrossRef]
- Johnson, B.A.; Kumar, P.; Okano, N.; Dasgupta, R.; Shivakoti, B.R. Nature-Based Solutions for Climate Change Adaptation: A Systematic Review of Systematic Reviews. Nat.-Based Solut. 2022, 2, 100042. [Google Scholar] [CrossRef]
- Rigolon, A.; Browning, M.H.E.M.; McAnirlin, O.; Yoon, H. (Violet) Green Space and Health Equity: A Systematic Review on the Potential of Green Space to Reduce Health Disparities. Int. J. Environ. Res. Public Health 2021, 18, 2563. [Google Scholar] [CrossRef]
- Kabisch, N.; van den Bosch, M.; Lafortezza, R. The Health Benefits of Nature-Based Solutions to Urbanization Challenges for Children and the Elderly—A Systematic Review. Environ. Res. 2017, 159, 362–373. [Google Scholar] [CrossRef]
- Bowler, D.; Buyung-Ali, L.; Knight, T.; Pullin, A. A Systematic Review of Evidence for the Added Benefits to Health of Exposure to Natural Environments. BMC Public Health 2010, 10, 456. [Google Scholar] [CrossRef]
- Callaghan, A.; McCombe, G.; Harrold, A.; McMeel, C.; Mills, G.; Moore-Cherry, N.; Cullen, W. The Impact of Green Spaces on Mental Health in Urban Settings: A Scoping Review. J. Ment. Health 2021, 30, 179–193. [Google Scholar] [CrossRef]
- Thompson Coon, J.; Boddy, K.; Stein, K.; Whear, R.; Barton, J.; Depledge, M.H. Does Participating in Physical Activity in Outdoor Natural Environments Have a Greater Effect on Physical and Mental Wellbeing than Physical Activity Indoors? A Systematic Review. Environ. Sci. Technol. 2011, 45, 1761–1772. [Google Scholar] [CrossRef]
- Dadvand, P.; Nieuwenhuijsen, M.J.; Esnaola, M.; Forns, J.; Basagaña, X.; Alvarez-Pedrerol, M.; Rivas, I.; López-Vicente, M.; De Castro Pascual, M.; Su, J.; et al. Green Spaces and Cognitive Development in Primary Schoolchildren. Proc. Natl. Acad. Sci. USA 2015, 112, 7937–7942. [Google Scholar] [CrossRef]
- Wendelboe-Nelson, C.; Kelly, S.; Kennedy, M.; Cherrie, J.W. A Scoping Review Mapping Research on Green Space and Associated Mental Health Benefits. Int. J. Environ. Res. Public Health 2019, 16, 2081. [Google Scholar] [CrossRef]
- Lackey, N.Q.; Tysor, D.A.; McNay, G.D.; Joyner, L.; Baker, K.H.; Hodge, C. Mental Health Benefits of Nature-Based Recreation: A Systematic Review. Ann. Leis. Res. 2021, 24, 379–393. [Google Scholar] [CrossRef]
- Kim, E.; Park, S.; Kim, S.; Choi, Y.; Cho, J.H.; Kim, G. Is Altitude a Determinant of the Health Benefits of Nature Exposure? A Systematic Review and Meta-Analysis. Front. Public Health 2022, 10, 1021618. [Google Scholar] [CrossRef]
- Barakat, C.; Yousufzai, S. Green Space and Mental Health for Vulnerable Populations: A Conceptual Review of the Evidence. J. Mil. Veteran Fam. Health 2020, 6, 51–57. [Google Scholar] [CrossRef]
- Invest4Nature Nature-Based Solutions. Available online: https://invest4nature.eu/ (accessed on 17 December 2025).
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Clarivate Web of Science Core Collection. Available online: https://clarivate.com/academia-government/scientific-and-academic-research/research-discovery-and-referencing/web-of-science/web-of-science-core-collection/ (accessed on 17 December 2025).
- Elsevier Scopus. Available online: https://www.elsevier.com/products/scopus (accessed on 17 December 2025).
- WHO. Health and Well-Being. Available online: https://www.who.int/data/gho/data/major-themes/health-and-well-being (accessed on 17 December 2025).
- International Union for Conservation of Nature. No Time to Lose: Make Full Use of Nature-Based Solutions in the Post-2012 Climate Change Regime. Position Paper for the Fifteenth Session of the Conference of the Parties to the United Nations Framework Convention on Climate Change (COP15); International Union for Conservation of Nature (IUCN): Gland, Switzerland, 2009. [Google Scholar]
- Steel, P.; Fariborzi, H.; Hendijani, R. An Application of Modern Literature Review Methodology: Finding Needles in Ever-Growing Haystacks; SAGE Publications Ltd.: Thousand Oaks, CA, USA, 2023. [Google Scholar]
- Poulsen, T.M.; Gordon East, W.; Windley, B.F.; Berentsen, W.H. Europe|History, Countries, Map, & Facts|Britannica. Available online: https://www.britannica.com/place/Europe (accessed on 17 December 2025).
- UNEP. Intergovernmental Consultations on Nature-Based Solutions. Available online: https://www.unep.org/about-un-environment/intergovernmental-consultations-nbs (accessed on 17 December 2025).
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A.; PRISMA-P Group. Preferred Reporting Items for Systematic Review and Meta-Analysis Protocols (PRISMA-P) 2015 Statement. Syst. Rev. 2015, 4, 1. [Google Scholar] [CrossRef]
- World Bank. World Bank Open Data. Available online: https://data.worldbank.org (accessed on 13 April 2026).
- International Classification of Diseases for Mortality and Morbidity Statistics ICD-11 for Mortality and Morbidity Statistics. Available online: https://icd.who.int/browse/2024-01/mms/en (accessed on 17 December 2025).
- Engemann, K.; Svenning, J.; Arge, L.; Brandt, J.; Erikstrup, C.; Geels, C.; Hertel, O.; Mortensen, P.; Plana-Ripoll, O.; Tsirogiannis, C.; et al. Associations between Growing up in Natural Environments and Subsequent Psychiatric Disorders in Denmark. Environ. Res. 2020, 188, 109788. [Google Scholar] [CrossRef]
- Aerts, R.; Vanlessen, N.; Dujardin, S.; Nemery, B.; Van Nieuwenhuyse, A.; Bauwelinck, M.; Casas, L.; Demoury, C.; Plusquin, M.; Nawrot, T. Residential Green Space and Mental Health-Related Prescription Medication Sales: An Ecological Study in Belgium. Environ. Res. 2022, 211, 113056. [Google Scholar] [CrossRef]
- Adjei, P.; Agyei, F. Biodiversity, Environmental Health and Human Well-Being: Analysis of Linkages and Pathways. Environ. Dev. Sustain. 2015, 17, 1085–1102. [Google Scholar] [CrossRef]
- Bielinis, E.; Jaroszewska, A.; Łukowski, A.; Takayama, N. The Effects of a Forest Therapy Programme on Mental Hospital Patients with Affective and Psychotic Disorders. Int. J. Environ. Res. Public Health 2019, 17, 118. [Google Scholar] [CrossRef]
- Lanki, T.; Siponen, T.; Ojala, A.; Korpela, K.; Pennanen, A.; Tiittanen, P.; Tsunetsugu, Y.; Kagawa, T.; Tyrvainen, L. Acute Effects of Visits to Urban Green Environments on Cardiovascular Physiology in Women: A Field Experiment. Environ. Res. 2017, 159, 176–185. [Google Scholar] [CrossRef]
- MacBride-Stewart, S. Discourses of Wellbeing and Environmental Impact of Trail Runners in Protected Areas in New Zealand and the United Kingdom. Geoforum 2019, 107, 134–142. [Google Scholar] [CrossRef]
- Puhakka, R. University Students’ Participation in Outdoor Recreation and the Perceived Well-Being Effects of Nature. J. Outdoor Recreat. Tour.-Res. Plan. Manag. 2021, 36, 100425. [Google Scholar] [CrossRef]
- Harris, H. The Social Dimensions of Therapeutic Horticulture. Health Soc. Care Community 2017, 25, 1328–1336. [Google Scholar] [CrossRef]
- Hunter, R.F.; Adlakha, D.; Cardwell, C.; Cupples, M.E.; Donnelly, M.; Ellis, G.; Gough, A.; Hutchinson, G.; Kearney, T.; Longo, A.; et al. Investigating the Physical Activity, Health, Wellbeing, Social and Environmental Effects of a New Urban Greenway: A Natural Experiment (the PARC Study). Int. J. Behav. Nutr. Phys. Act. 2021, 18, 142. [Google Scholar] [CrossRef]
- O’Brien, L.; Snowdon, H. Health and Well-Being in Woodlands: A Case Study of the Chopwell Wood Health Project. Arboric. J. 2007, 30, 45–60. [Google Scholar] [CrossRef]
- Macpherson, H. Walkers with Visual-Impairments in the British Countryside: Picturesque Legacies, Collective Enjoyments and Well-Being Benefits. J. Rural. Stud. 2017, 51, 251–258. [Google Scholar] [CrossRef]
- Bauwelinck, M.; Zijlema, W.L.; Bartoll, X.; Vandenheede, H.; Cirach, M.; Lefebvre, W.; Vanpoucke, C.; Basagaña, X.; Nieuwenhuijsen, M.J.; Borrell, C.; et al. Residential Urban Greenspace and Hypertension: A Comparative Study in Two European Cities. Environ. Res. 2020, 191, 110032. [Google Scholar] [CrossRef]
- Tamosiunas, A.; Grazuleviciene, R.; Luksiene, D.; Dedele, A.; Reklaitiene, R.; Baceviciene, M.; Vencloviene, J.; Bernotiene, G.; Radisauskas, R.; Malinauskiene, V.; et al. Accessibility and Use of Urban Green Spaces, and Cardiovascular Health: Findings from a Kaunas Cohort Study. Environ. Health 2014, 13, 20. [Google Scholar] [CrossRef]
- Voelker, S.; Kistemann, T. Developing the Urban Blue: Comparative Health Responses to Blue and Green Urban Open Spaces in Germany. Health Place 2015, 35, 196–205. [Google Scholar] [CrossRef]
- Acott, T.; Willis, C.; Ranger, S.; Cumming, G.; Richardson, P.; O’Neill, R.; Ford, A. Coastal Transformations and Connections: Revealing Values through the Community Voice Method. People Nat. 2023, 5, 403–414. [Google Scholar] [CrossRef]
- Subiza-Perez, M.; Vozmediano, L.; San Juan, C. Green and Blue Settings as Providers of Mental Health Ecosystem Services: Comparing Urban Beaches and Parks and Building a Predictive Model of Psychological Restoration. Landsc. Urban Plan. 2020, 204, 103926. [Google Scholar] [CrossRef]
- Pasanen, T.; White, M.; Wheeler, B.; Garrett, J.; Elliott, L. Neighbourhood Blue Space, Health and Wellbeing: The Mediating Role of Different Types of Physical Activity. Environ. Int. 2019, 131, 105016. [Google Scholar] [CrossRef]
- Mourao, I.; Moreira, M.; Almeida, T.; Brito, L. Perceived Changes in Well-Being and Happiness with Gardening in Urban Organic Allotments in Portugal. Int. J. Sustain. Dev. World Ecol. 2019, 26, 79–89. [Google Scholar] [CrossRef]
- van den Berg, M.M.; van Poppel, M.; van Kamp, I.; Ruijsbroek, A.; Triguero-Mas, M.; Gidlow, C.; Nieuwenhuijsen, M.J.; Gražulevičiene, R.; van Mechelen, W.; Kruize, H.; et al. Do Physical Activity, Social Cohesion, and Loneliness Mediate the Association Between Time Spent Visiting Green Space and Mental Health? Environ. Behav. 2019, 51, 144–166. [Google Scholar] [CrossRef]
- Lyytimaki, J.; Pitkanen, K. Perceived Wellbeing Effects of Ecosystems in Finland. Hum. Ecol. 2020, 48, 335–345. [Google Scholar] [CrossRef]
- Cinderby, S.; Bagwell, S. Exploring the Co-Benefits of Urban Green Infrastructure Improvements for Businesses and Workers’ Wellbeing. Area 2018, 50, 126–135. [Google Scholar] [CrossRef]
- Aerts, R.; Dujardin, S.; Nemery, B.; Van Nieuwenhuyse, A.; Van Orshoven, J.; Aerts, J.; Somers, B.; Hendrickx, M.; Bruffaerts, N.; Bauwelinck, M.; et al. Residential Green Space and Medication Sales for Childhood Asthma: A Longitudinal Ecological Study in Belgium. Environ. Res. 2020, 189, 109914. [Google Scholar] [CrossRef] [PubMed]
- Dadvand, P.; Villanueva, C.; Font-Ribera, L.; Martinez, D.; Basagana, X.; Belmonte, J.; Vrijheid, M.; Grazuleviciene, R.; Kogevinas, M.; Nieuwenhuijsen, M. Risks and Benefits of Green Spaces for Children: A Cross-Sectional Study of Associations with Sedentary Behavior, Obesity, Asthma, and Allergy. Environ. Health Perspect. 2014, 122, 1329–1335. [Google Scholar] [CrossRef] [PubMed]
- Chi, D.; Aerts, R.; Van Nieuwenhuyse, A.; Bauwelinck, M.; Demoury, C.; Plusquin, M.; Nawrot, T.; Casas, L.; Somers, B. Residential Exposure to Urban Trees and Medication Sales for Mood Disorders and Cardiovascular Disease in Brussels, Belgium: An Ecological Study. Environ. Health Perspect. 2022, 130, 57003. [Google Scholar] [CrossRef] [PubMed]
- Cherrie, M.; Wheeler, B.; White, M.; Sarran, C.; Osborne, N. Coastal Climate Is Associated with Elevated Solar Irradiance and Higher 25(OH)D Level. Environ. Int. 2015, 77, 76–84. [Google Scholar] [CrossRef]
- Dzhambov, A.; Markevych, I.; Hartig, T.; Tilov, B.; Arabadzhiev, Z.; Stoyanov, D.; Gatseva, P.; Dimitrova, D. Multiple Pathways Link Urban Green- and Bluespace to Mental Health in Young Adults. Environ. Res. 2018, 166, 223–233. [Google Scholar] [CrossRef]
- Young, C.; Hofmann, M.; Frey, D.; Moretti, M.; Bauer, N. Psychological Restoration in Urban Gardens Related to Garden Type, Biodiversity and Garden-Related Stress. Landsc. Urban Plan. 2020, 198, 103777. [Google Scholar] [CrossRef]
- Birch, J.; Rishbeth, C.; Payne, S. Nature Doesn’t Judge You—How Urban Nature Supports Young People’s Mental Health and Wellbeing in a Diverse UK City. Health Place 2020, 62, 102296. [Google Scholar] [CrossRef] [PubMed]
- Hanson, H.; Eckberg, E.; Widenberg, M.; Olsson, J. Gardens’ Contribution to People and Urban Green Space. Urban For. Urban Green. 2021, 63, 127198. [Google Scholar] [CrossRef]
- Capotorti, G.; Alós Ortí, M.M.; Copiz, R.; Fusaro, L.; Mollo, B.; Salvatori, E.; Zavattero, L. Biodiversity and Ecosystem Services in Urban Green Infrastructure Planning: A Case Study from the Metropolitan Area of Rome (Italy). Urban For. Urban Green. 2019, 37, 87–96. [Google Scholar] [CrossRef]
- Jones, L.; Vieno, M.; Fitch, A.; Carnell, E.; Steadman, C.; Cryle, P.; Holland, M.; Nemitz, E.; Morton, D.; Hall, J.; et al. Urban Natural Capital Accounts: Developing a Novel Approach to Quantify Air Pollution Removal by Vegetation. J. Environ. Econ. Policy 2019, 8, 413–428. [Google Scholar] [CrossRef]
- Powe, N.A.; Willis, K.G. Mortality and Morbidity Benefits of Air Pollution (SO2 and PM10) Absorption Attributable to Woodland in Britain. J. Environ. Manag. 2004, 70, 119–128. [Google Scholar] [CrossRef]
- Mueller, N.; Rojas-Rueda, D.; Khreis, H.; Cirach, M.; Andres, D.; Ballester, J.; Bartoll, X.; Daher, C.; Deluca, A.; Echave, C.; et al. Changing the Urban Design of Cities for Health: The Superblock Model. Environ. Int. 2020, 134. [Google Scholar] [CrossRef]
- Vidal Yañez, D.; Pereira Barboza, E.; Cirach, M.; Daher, C.; Nieuwenhuijsen, M.; Mueller, N. An Urban Green Space Intervention with Benefits for Mental Health: A Health Impact Assessment of the Barcelona “Eixos Verds” Plan. Environ. Int. 2023, 174, 107880. [Google Scholar] [CrossRef] [PubMed]
- Maria Raya, J.; Martínez-Garcia, E.; Celma, D. Economic and Social Yield of Investing in Hiking Tourism: The Case of Berguedà, Spain. J. Travel Tour. Mark. 2018, 35, 148–161. [Google Scholar] [CrossRef]
- Vert, C.; Nieuwenhuijsen, M.; Gascon, M.; Grellier, J.; Fleming, L.; White, M.; Rojas-Rueda, D. Health Benefits of Physical Activity Related to an Urban Riverside Regeneration. Int. J. Environ. Res. Public Health 2019, 16, 462. [Google Scholar] [CrossRef] [PubMed]
- Machado, F.; Mourato, S. Evaluating the Multiple Benefits of Marine Water Quality Improvements: How Important Are Health Risk Reductions? J. Environ. Manag. 2002, 65, 239–250. [Google Scholar] [CrossRef]
- Federal Reserve Bank of St. Louis Table Data—U.S. Dollars to Euro Spot Exchange Rate|FRED|St. Louis Fed. Available online: https://fred.stlouisfed.org/data/exuseu? (accessed on 17 December 2025).
- Cox, D.; Shanahan, D.; Hudson, H.; Plummer, K.; Siriwardena, G.; Fuller, R.; Anderson, K.; Hancock, S.; Gaston, K. Doses of Neighborhood Nature: The Benefits for Mental Health of Living with Nature. BioScience 2017, 67, 147–155. [Google Scholar] [CrossRef]
- Pretty, J.; Peacock, J.; Hine, R.; Sellens, M.; South, N.; Griffin, M. Green Exercise in the UK Countryside: Effects on Health and Psychological Well-Being, and Implications for Policy and Planning. J. Environ. Plan. Manag. 2007, 50, 211–231. [Google Scholar] [CrossRef]
- Dzhambov, A.; Lercher, P.; Ruedisser, J.; Browning, M.; Markevych, I. Home Gardens and Distances to Nature Associated with Behavior Problems in Alpine Schoolchildren: Role of Secondhand Smoke Exposure and Biomarkers. Int. J. Hyg. Environ. Health 2022, 243, 113975. [Google Scholar] [CrossRef]
- Saenen, N.; Nawrot, T.; Hautekiet, P.; Wang, C.; Roels, H.; Dadvand, P.; Plusquin, M.; Bijnens, E. Residential Green Space Improves Cognitive Performances in Primary Schoolchildren Independent of Traffic-Related Air Pollution Exposure. Environ. Health 2023, 22, 33. [Google Scholar] [CrossRef] [PubMed]
- Scartazza, A.; Mancini, M.; Proietti, S.; Moscatello, S.; Mattioni, C.; Costantini, F.; Di Baccio, D.; Villani, F.; Massacci, A. Caring Local Biodiversity in a Healing Garden: Therapeutic Benefits in Young Subjects with Autism. Urban For. Urban Green. 2020, 47, 126511. [Google Scholar] [CrossRef]
- Thygesen, M.; Engemann, K.; Holst, G.; Hansen, B.; Geels, C.; Brandt, J.; Pedersen, C.; Dalsgaard, S. The Association between Residential Green Space in Childhood and Development of Attention Deficit Hyperactivity Disorder: A Population-Based Cohort Study. Environ. Health Perspect. 2020, 128, 127011. [Google Scholar] [CrossRef]
- Burkart, K.; Meier, F.; Schneider, A.; Breitner, S.; Canario, P.; Alcoforado, M.; Scherer, D.; Endlicher, W. Modification of Heat-Related Mortality in an Elderly Urban Population by Vegetation (Urban Green) and Proximity to Water (Urban Blue): Evidence from Lisbon, Portugal. Environ. Health Perspect. 2016, 124, 927–934. [Google Scholar] [CrossRef] [PubMed]
- Marvuglia, A.; Koppelaar, R.; Rugani, B. The Effect of Green Roofs on the Reduction of Mortality Due to Heatwaves: Results from the Application of a Spatial Microsimulation Model to Four European Cities. Ecol. Model. 2020, 438, 109351. [Google Scholar] [CrossRef]
- Cameron, R.; Brindley, P.; Mears, M.; McEwan, K.; Ferguson, F.; Sheffield, D.; Jorgensen, A.; Riley, J.; Goodrick, J.; Ballard, L.; et al. Where the Wild Things Are! Do Urban Green Spaces with Greater Avian Biodiversity Promote More Positive Emotions in Humans? Urban Ecosyst. 2020, 23, 301–317. [Google Scholar] [CrossRef]
- Chalmin-Pui, L.; Roe, J.; Griffiths, A.; Smyth, N.; Heaton, T.; Clayden, A.; Cameron, R. “It Made Me Feel Brighter in Myself”- The Health and Well-Being Impacts of a Residential Front Garden Horticultural Intervention. Landsc. Urban Plan. 2021, 205, 103958. [Google Scholar] [CrossRef]
- Cox, D.; Shanahan, D.; Hudson, H.; Fuller, R.; Gaston, K. The Impact of Urbanisation on Nature Dose and the Implications for Human Health. Landsc. Urban Plan. 2018, 179, 72–80. [Google Scholar] [CrossRef]
- Mahmoud, I.H.; Morello, E.; Vona, C.; Benciolini, M.; Sejdullahu, I.; Trentin, M.; Pascual, K.H. Setting the Social Monitoring Framework for Nature-Based Solutions Impact: Methodological Approach and Pre-Greening Measurements in the Case Study from Clever Cities Milan. Sustainability 2021, 13, 9672. [Google Scholar] [CrossRef]
- Thompson, C.; Roe, J.; Aspinall, P. Woodland Improvements in Deprived Urban Communities: What Impact Do They Have on People’s Activities and Quality of Life? Landsc. Urban Plan. 2013, 118, 79–89. [Google Scholar] [CrossRef]
- Zijlema, W.L.; Avila-Palencia, I.; Triguero-Mas, M.; Gidlow, C.; Maas, J.; Kruize, H.; Andrusaityte, S.; Grazuleviciene, R.; Nieuwenhuijsen, M.J. Active Commuting through Natural Environments Is Associated with Better Mental Health: Results from the PHENOTYPE Project. Environ. Int. 2018, 121, 721–727. [Google Scholar] [CrossRef]
- Milligan, C.; Gatrell, A.; Bingley, A. “Cultivating Health”: Therapeutic Landscapes and Older People in Northern England. Soc. Sci. Med. 2004, 58, 1781–1793. [Google Scholar] [CrossRef]
- O’Brien, L.; Burls, A.; Townsend, M.; Ebden, M. Volunteering in Nature as a Way of Enabling People to Reintegrate into Society. Perspect. Public Health 2011, 131, 71–81. [Google Scholar] [CrossRef] [PubMed]
- Ashbullby, K.; Pahl, S.; Webley, P.; White, M. The Beach as a Setting for Families’ Health Promotion: A Qualitative Study with Parents and Children Living in Coastal Regions in Southwest England. Health Place 2013, 23, 138–147. [Google Scholar] [CrossRef]
- Marcheggiani, S.; Tinti, D.; Puccinelli, C.; Mancini, L. Urban Green Space and Healthy Living: An Exploratory Study Among Appia Antica Parks Users (Rome-Italy). Fresenius Environ. Bull. 2019, 28, 4984–4989. [Google Scholar]
- Dunlop, T.; Khojasteh, D.; Cohen-Shacham, E.; Glamore, W.; Haghani, M.; van den Bosch, M.; Rizzi, D.; Greve, P.; Felder, S. The Evolution and Future of Research on Nature-Based Solutions to Address Societal Challenges. Commun. Earth Environ. 2024, 5, 132. [Google Scholar] [CrossRef]
- Yang, H.; Chae, J.; Song, C.; Choi, E. Research Trends of Nature-Based Solutions: From Urban to Climate Change. Front. For. Glob. Change 2024, 7, 1351189. [Google Scholar] [CrossRef]
- Labib, S.M.; Browning, M.H.E.M.; Rigolon, A.; Helbich, M.; James, P. Nature’s Contributions in Coping with a Pandemic in the 21st Century: A Narrative Review of Evidence during COVID-19. Sci. Total Environ. 2022, 833, 155095. [Google Scholar] [CrossRef]
- The World Bank World. Bank Country and Lending Groups—World Bank Data Help Desk. Available online: https://datahelpdesk.worldbank.org/knowledgebase/articles/906519-world-bank-country-and-lending-groups (accessed on 26 January 2026).
- Nawrath, M.; Guenat, S.; Elsey, H.; Dallimer, M. Exploring Uncharted Territory: Do Urban Greenspaces Support Mental Health in Low- and Middle-Income Countries? Environ. Res. 2021, 194, 110625. [Google Scholar] [CrossRef]
- European Environment Agency. Who Benefits from Nature in Cities?: Social Inequalities in Access to Urban Green and Blue Spaces Across Europe; Publications Office: Luxembourg, 2022. [Google Scholar]
- Forster, T.; Kentikelenis, A.; Bambra, C. Health Inequalities in Europe: Setting the Stage for Progressive Policy Action; FEPS: Bruxelles, Belgium, 2018. [Google Scholar]
- United Nations. The World’s Cities in 2018: Data Booklet; Statistical Papers—United Nations (Ser. A), Population and Vital Statistics Report; UN: New York, NY, USA, 2018. [Google Scholar]
- European Commission, Joint Research Centre (JRC) Share of Population Living in Urban Areas 2025. Available online: https://ghsl.jrc.ec.europa.eu (accessed on 20 May 2026).
- Jones, F.; Fisher, J.C.; Austen, G.E.; Irvine, K.N.; Dallimer, M.; Croager, L.; Nawrath, M.; Fish, R.D.; Davies, Z.G. Testing the BIO-WELL Scale In Situ: Measuring Human Wellbeing Responses to Biodiversity within Forests. J. Environ. Psychol. 2026, 109, 102897. [Google Scholar] [CrossRef]
- Lovell, R.; Wheeler, B.W.; Higgins, S.L.; Irvine, K.N.; Depledge, M.H. A Systematic Review of the Health and Well-Being Benefits of Biodiverse Environments. J. Toxicol. Environ. Health B Crit. Rev. 2014, 17, 1–20. [Google Scholar] [CrossRef]
- Frantzeskaki, N. Seven Lessons for Planning Nature-Based Solutions in Cities. Environ. Sci. Policy 2019, 93, 101–111. [Google Scholar] [CrossRef]
- Pereira, P.; Yin, C.; Hua, T. Nature-Based Solutions, Ecosystem Services, Disservices, and Impacts on Well-Being in Urban Environments. Curr. Opin. Environ. Sci. Health 2023, 33, 100465. [Google Scholar] [CrossRef]
- Raymond, C.M.; Frantzeskaki, N.; Kabisch, N.; Berry, P.; Breil, M.; Nita, M.R.; Geneletti, D.; Calfapietra, C. A Framework for Assessing and Implementing the Co-Benefits of Nature-Based Solutions in Urban Areas. Environ. Sci. Policy 2017, 77, 15–24. [Google Scholar] [CrossRef]
- Fuller, R.A.; Gaston, K.J. The Scaling of Green Space Coverage in European Cities. Biol. Lett. 2009, 5, 352–355. [Google Scholar] [CrossRef]
- European Environment Agency Scaling Nature-Based Solutions for Climate Resilience and Nature Restoration. Available online: https://www.eea.europa.eu/publications/scaling-nature-based-solutions (accessed on 26 January 2026).
- Kabisch, N.; Korn, H.; Stadler, J.; Bonn, A. Nature-Based Solutions to Climate Change Adaptation in Urban Areas—Linkages Between Science, Policy and Practice. In Nature-Based Solutions to Climate Change Adaptation in Urban Areas: Linkages Between Science, Policy and Practice; Kabisch, N., Korn, H., Stadler, J., Bonn, A., Eds.; Springer International Publishing: Cham, Switzerland, 2017; pp. 1–11. [Google Scholar]
- Frumkin, H.; Bratman, G.N.; Breslow, S.J.; Cochran, B.; Kahn, P.H.; Lawler, J.J.; Levin, P.S.; Tandon, P.S.; Varanasi, U.; Wolf, K.L.; et al. Nature Contact and Human Health: A Research Agenda. Environ. Health Perspect. 2017, 125, 075001. [Google Scholar] [CrossRef]
- Markevych, I.; Schoierer, J.; Hartig, T.; Chudnovsky, A.; Hystad, P.; Dzhambov, A.M.; de Vries, S.; Triguero-Mas, M.; Brauer, M.; Nieuwenhuijsen, M.J.; et al. Exploring Pathways Linking Greenspace to Health: Theoretical and Methodological Guidance. Environ. Res. 2017, 158, 301–317. [Google Scholar] [CrossRef]
- Jennings, V.; Bamkole, O. The Relationship between Social Cohesion and Urban Green Space: An Avenue for Health Promotion. Int. J. Environ. Res. Public Health 2019, 16, 452. [Google Scholar] [CrossRef]
- Robinson, J.M.; Breed, A.C.; Camargo, A.; Redvers, N.; Breed, M.F. Biodiversity and Human Health: A Scoping Review and Examples of Underrepresented Linkages. Environ. Res. 2024, 246, 118115. [Google Scholar] [CrossRef]
- Hopkins, S.R.; Lafferty, K.D.; Wood, C.L.; Olson, S.H.; Buck, J.C.; De Leo, G.A.; Fiorella, K.J.; Fornberg, J.L.; Garchitorena, A.; Jones, I.J.; et al. Evidence Gaps and Diversity among Potential Win–Win Solutions for Conservation and Human Infectious Disease Control. Lancet Planet. Health 2022, 6, e694–e705. [Google Scholar] [CrossRef]
- Ruggeri, A. Climate Change Is Supercharging Pollen and Making Allergies Worse. Available online: https://www.bbc.com/future/article/20250410-how-climate-driven-thunderstorms-supercharge-pollen-allergies (accessed on 21 January 2026).
- D’Amato, G.; Cecchi, L.; Bonini, S.; Nunes, C.; Annesi-Maesano, I.; Behrendt, H.; Liccardi, G.; Popov, T.; van Cauwenberge, P. Allergenic Pollen and Pollen Allergy in Europe. Allergy 2007, 62, 976–990. [Google Scholar] [CrossRef]
- Zhao, T.; Heinrich, J.; Brauer, M.; Fulman, N.; Idrose, N.S.; Baumbach, C.; Buters, J.; Markevych, I.; Ritz, B.; Tham, R.; et al. Urban Greenspace under a Changing Climate: Benefit or Harm for Allergies and Respiratory Health? Environ. Epidemiol. 2025, 9, e372. [Google Scholar] [CrossRef]
- Gionfra, S.; Utkarsh, S.; Moncorps, L. Leaving No One behind: Towards Inclusive Nature-Based Solutions; NetworkNature: Brussels, Belgium, 2023. [Google Scholar]
- Johri, N. The Importance of a Human-Centered Approach in Implementing the Sustainable Development Goals; Center for American Progress: Washington, DC, USA, 2016. [Google Scholar]
- Kopsieker, L.; Gerritsen, E.; Stainforth, T.; Lucic, A.; Costa Domingo, G.; Naumann, S.; Röschel, L.; Davis, M. Nature-Based Solutions and Their Socio-Economic Benefits for Europe’s Recovery: Enhancing the Uptake of Nature-Based Solutions Across EU Policies; Institute for European Environmental Policy: Brussels, Belgium, 2021; Volume 19. [Google Scholar]
- Li, Y.; Svenning, J.-C.; Zhou, W.; Zhu, K.; Abrams, J.F.; Lenton, T.M.; Ripple, W.J.; Yu, Z.; Teng, S.N.; Dunn, R.R.; et al. Green Spaces Provide Substantial but Unequal Urban Cooling Globally. Nat. Commun. 2024, 15, 7108. [Google Scholar] [CrossRef]
- Pérez González-Anguiano, P. Protecting Health and Equity in a Warming Europe. Available online: https://cicero.oslo.no/en/articles/protecting-health-and-equity-in-a-warming-europe (accessed on 21 January 2026).
- Mutafoglu, K.; ten Brink, P.; Schweitzer, J.-P.; Jones, H. Nature for Health and Equity; Institute for European Environmental Policy (IEEP): Brussels, Belgium, 2017. [Google Scholar]
- ten Brink, P.; Mutafoglu, K.; Schweitzer, J.-P.; Kettunen, M.; Twigger-Ross, C.; Kuipers, Y.; Emonts, M.; Tyrväinen, L.; Hujala, T.; Ojala, A. The Health and Social Benefits of Nature and Biodiversity Protection—Executive Summary; Institute for European Environmental Policy: Brussels, Belgium, 2016. [Google Scholar]
- Viti, M.; Löwe, R.; Sørup, H.J.D.; Rasmussen, M.; Arnbjerg-Nielsen, K.; McKnight, U.S. Knowledge Gaps and Future Research Needs for Assessing the Non-Market Benefits of Nature-Based Solutions and Nature-Based Solution-like Strategies. Sci. Total Environ. 2022, 841, 156636. [Google Scholar] [CrossRef]
- Kabisch, N.; Haase, D. Green Justice or Just Green? Provision of Urban Green Spaces in Berlin, Germany. Landsc. Urban Plan. 2014, 122, 129–139. [Google Scholar] [CrossRef]




Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license.