
Do Only Calcium and Vitamin D Matter? Micronutrients in the Diet of Inflammatory Bowel Diseases Patients and the Risk of Osteoporosis

 , , , and
, , , and
Abstract
1. Introduction
2. Nutrition in IBD
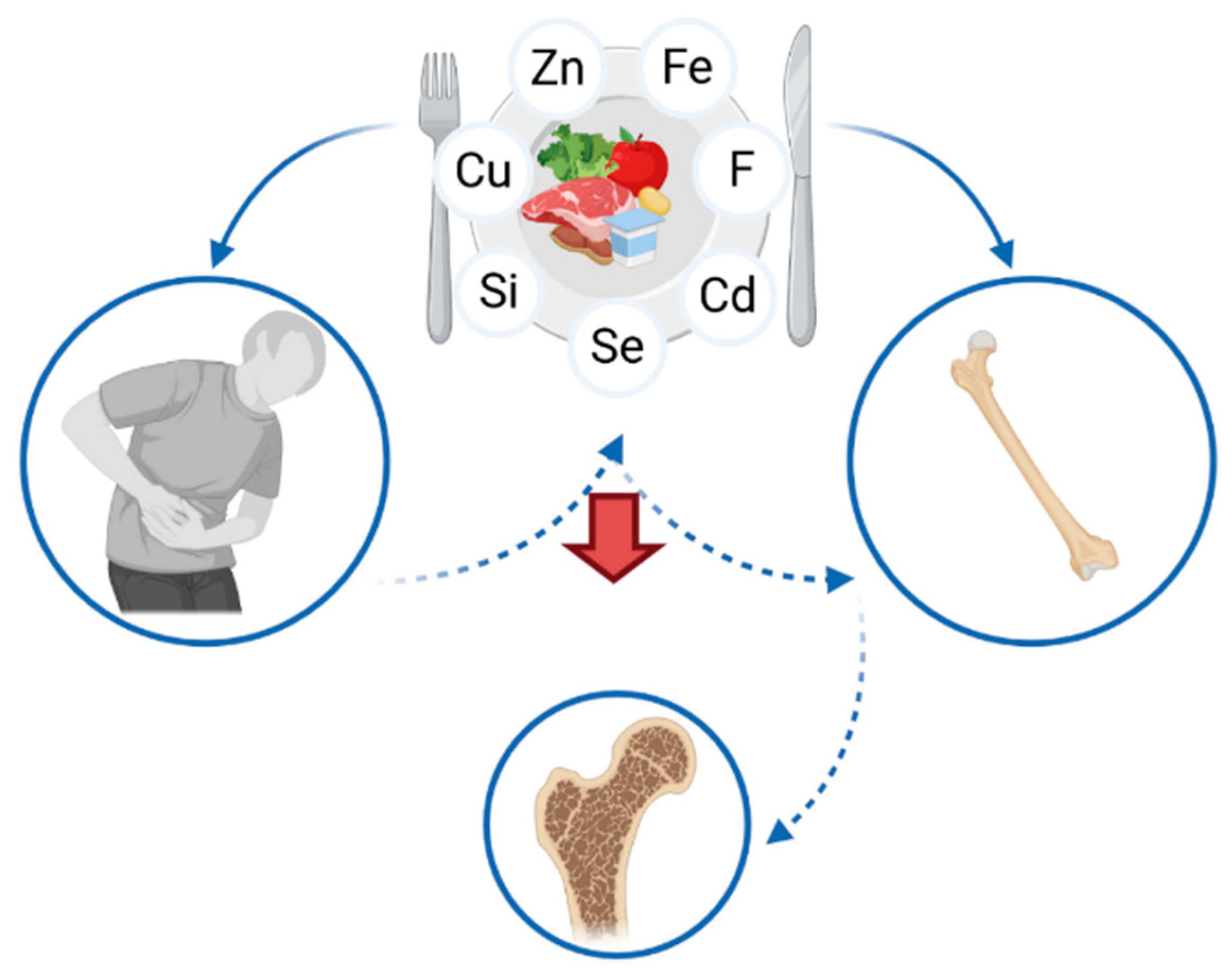
3. Osteoporosis in IBD
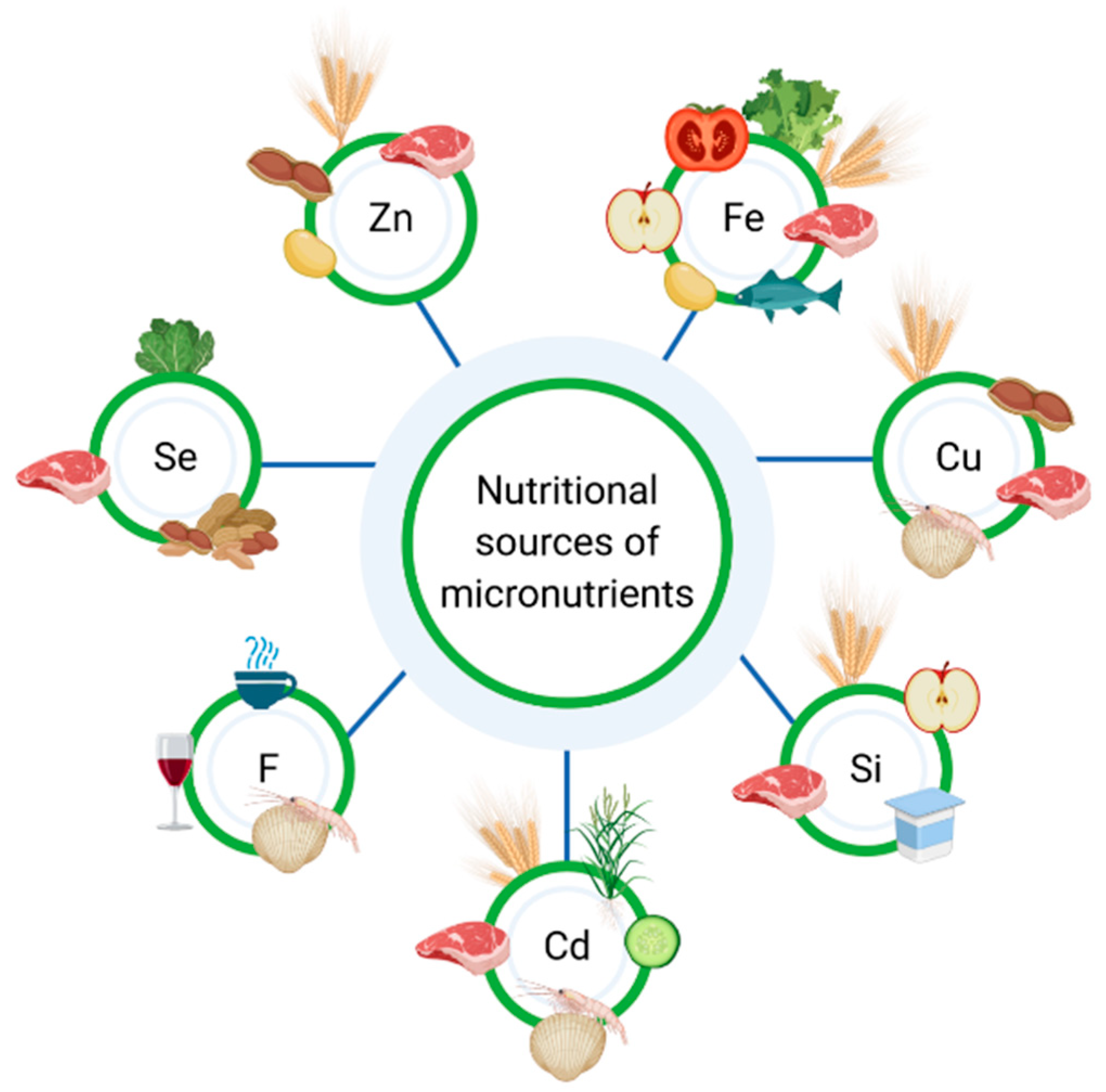
4. Micronutrients in the Diet of IBD Patients
4.1. Zinc
4.2. Copper
4.3. Selenium
4.4. Iron
4.5. Cadmium
4.6. Silicon
4.7. Fluorine
5. Gut Microbiota and Micronutrients
6. Summary
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Alatab, S.; Sepanlou, S.G.; Ikuta, K.; Vahedi, H.; Bisignano, C.; Safiri, S.; Sadeghi, A.; Nixon, M.R.; Abdoli, A.; Abolhassani, H.; et al. The Global, Regional, and National Burden of Inflammatory Bowel Disease in 195 Countries and Territories, 1990–2017: A Systematic Analysis for the Global Burden of Disease Study 2017. Lancet Gastroenterol. Hepatol. 2020, 5, 17–30. [Google Scholar] [CrossRef]
- Burisch, J.; Munkholm, P. The Epidemiology of Inflammatory Bowel Disease. Scand. J. Gastroenterol. 2015, 50, 942–951. [Google Scholar] [CrossRef]
- Hsu, Y.-C.; Wu, T.-C.; Lo, Y.-C.; Wang, L.-S. Gastrointestinal Complications and Extraintestinal Manifestations of Inflammatory Bowel Disease in Taiwan: A Population-Based Study. J. Chin. Med. Assoc. 2017, 80, 56–62. [Google Scholar] [CrossRef]
- Fact Sheets—Malnutrition. Available online: https://www.who.int/news-room/fact-sheets/detail/malnutrition (accessed on 15 January 2021).
- Krela-Kaźmierczak, I.; Michalak, M.; Szymczak-Tomczak, A.; Łykowska-Szuber, L.; Stawczyk-Eder, K.; Waszak, K.; Kucharski, M.A.; Dobrowolska, A.; Eder, P. Prevalence of Osteoporosis and Osteopenia in a Population of Patients with Inflammatory Bowel Diseases from the Wielkopolska Region. Pol. Arch. Intern. Med. 2018, 128, 447–454. [Google Scholar] [CrossRef]
- Scaldaferri, F.; Pizzoferrato, M.; Lopetuso, L.R.; Musca, T.; Ingravalle, F.; Sicignano, L.L.; Mentella, M.; Miggiano, G.; Mele, M.C.; Gaetani, E.; et al. Nutrition and IBD: Malnutrition and/or Sarcopenia? A Practical Guide. Gastroenterol. Res. Pract. 2017, 2017. [Google Scholar] [CrossRef]
- Pulley, J.; Todd, A.; Flatley, C.; Begun, J. Malnutrition and Quality of Life among Adult Inflammatory Bowel Disease Patients. JGH Open 2020, 4, 454–460. [Google Scholar] [CrossRef]
- Yamada, S.; Inaba, M. [Osteoporosis and mineral intake]. Clin. Calcium 2004, 14, 96–99. [Google Scholar]
- Karaaslan, F.; Mutlu, M.; Mermerkaya, M.U.; Karaoğlu, S.; Saçmaci, Ş.; Kartal, Ş. Comparison of Bone Tissue Trace-Element Concentrations and Mineral Density in Osteoporotic Femoral Neck Fractures and Osteoarthritis. Clin. Interv. Aging 2014, 9, 1375–1382. [Google Scholar] [CrossRef]
- Liu, S.-Z.; Yan, H.; Xu, P.; Li, J.-P.; Zhuang, G.-H.; Zhu, B.-F.; Lu, S.-M. Correlation Analysis between Bone Mineral Density and Serum Element Contents of Postmenopausal Women in Xi’an Urban Area. Biol. Trace Elem. Res. 2009, 131, 205–214. [Google Scholar] [CrossRef]
- Rayman, M.P. Selenium Intake, Status, and Health: A Complex Relationship. Horm. Athens Greece 2020, 19, 9–14. [Google Scholar] [CrossRef]
- Bischoff, S.C.; Escher, J.; Hébuterne, X.; Kłęk, S.; Krznaric, Z.; Schneider, S.; Shamir, R.; Stardelova, K.; Wierdsma, N.; Wiskin, A.E.; et al. ESPEN Practical Guideline: Clinical Nutrition in Inflammatory Bowel Disease. Clin. Nutr. Edinb. Scotl. 2020, 39, 632–653. [Google Scholar] [CrossRef]
- Weaver, C.M.; Alexander, D.D.; Boushey, C.J.; Dawson-Hughes, B.; Lappe, J.M.; LeBoff, M.S.; Liu, S.; Looker, A.C.; Wallace, T.C.; Wang, D.D. Calcium plus Vitamin D Supplementation and Risk of Fractures: An Updated Meta-Analysis from the National Osteoporosis Foundation. Osteoporos. Int. J. Establ. Result Coop. Eur. Found. Osteoporos. Natl. Osteoporos. Found. USA 2016, 27, 367–376. [Google Scholar] [CrossRef]
- Paschalis, E.P.; Gamsjaeger, S.; Hassler, N.; Fahrleitner-Pammer, A.; Dobnig, H.; Stepan, J.J.; Pavo, I.; Eriksen, E.F.; Klaushofer, K. Vitamin D and Calcium Supplementation for Three Years in Postmenopausal Osteoporosis Significantly Alters Bone Mineral and Organic Matrix Quality. Bone 2017, 95, 41–46. [Google Scholar] [CrossRef]
- Reyes-Garcia, R.; Mendoza, N.; Palacios, S.; Salas, N.; Quesada-Charneco, M.; Garcia-Martin, A.; Fonolla, J.; Lara-Villoslada, F.; Muñoz-Torres, M. Effects of Daily Intake of Calcium and Vitamin D-Enriched Milk in Healthy Postmenopausal Women: A Randomized, Controlled, Double-Blind Nutritional Study. J. Womens Health 2002 2018, 27, 561–568. [Google Scholar] [CrossRef]
- Henriksen, K.; Byrjalsen, I.; Andersen, J.R.; Bihlet, A.R.; Russo, L.A.; Alexandersen, P.; Valter, I.; Qvist, P.; Lau, E.; Riis, B.J.; et al. A Randomized, Double-Blind, Multicenter, Placebo-Controlled Study to Evaluate the Efficacy and Safety of Oral Salmon Calcitonin in the Treatment of Osteoporosis in Postmenopausal Women Taking Calcium and Vitamin D. Bone 2016, 91, 122–129. [Google Scholar] [CrossRef] [PubMed]
- Ratajczak, A.E.; Rychter, A.M.; Zawada, A.; Dobrowolska, A.; Krela-Kaźmierczak, I. Nutrients in the Prevention of Osteoporosis in Patients with Inflammatory Bowel Diseases. Nutrients 2020, 12, 1702. [Google Scholar] [CrossRef] [PubMed]
- Owczarek, D.; Rodacki, T.; Domagała-Rodacka, R.; Cibor, D.; Mach, T. Diet and Nutritional Factors in Inflammatory Bowel Diseases. World J. Gastroenterol. 2016, 22, 895–905. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.S.; Lee, J. Musculoskeletal Manifestation in Inflammatory Bowel Disease. Korean J. Gastroenterol. 2019, 73, 276–284. [Google Scholar] [CrossRef]
- Föger-Samwald, U.; Dovjak, P.; Azizi-Semrad, U.; Kerschan-Schindl, K.; Pietschmann, P. Osteoporosis: Pathophysiology and Therapeutic Options. EXCLI J. 2020, 19, 1017–1037. [Google Scholar] [CrossRef]
- Sandhu, S.K.; Hampson, G. The Pathogenesis, Diagnosis, Investigation and Management of Osteoporosis. J. Clin. Pathol. 2011, 64, 1042–1050. [Google Scholar] [CrossRef]
- Wang, N.; Xie, D.; Wu, J.; Wu, Z.; He, H.; Yang, Z.; Yang, T.; Wang, Y. Selenium and Bone Health: A Protocol for a Systematic Review and Meta-Analysis. BMJ Open 2020, 10, e036612. [Google Scholar] [CrossRef] [PubMed]
- Lane, N.E. Epidemiology, Etiology, and Diagnosis of Osteoporosis. Am. J. Obstet. Gynecol. 2006, 194, S3–S11. [Google Scholar] [CrossRef] [PubMed]
- Adriani, A.; Pantaleoni, S.; Luchino, M.; Ribaldone, D.G.; Reggiani, S.; Sapone, N.; Sguazzini, C.; Isaia, G.; Pellicano, R.; Astegiano, M. Osteopenia and Osteoporosis in Patients with New Diagnosis of Inflammatory Bowel Disease. Panminerva Med. 2014, 56, 145–149. [Google Scholar]
- Pellicano, R.; Ribaldone, D.G. Osteoporosis, Osteopenia, and Inflammatory Bowel Disease: Lessons from a Real-world Study. Pol. Arch. Intern. Med. 2018, 128, 411–413. [Google Scholar] [CrossRef]
- Hoffmann, P.; Krisam, J.; Kasperk, C.; Gauss, A. Prevalence, Risk Factors and Course of Osteoporosis in Patients with Crohn’s Disease at a Tertiary Referral Center. J. Clin. Med. 2019, 8, 2178. [Google Scholar] [CrossRef]
- Krela-Kaźmierczak, I.; Kaczmarek-Ryś, M.; Szymczak, A.; Michalak, M.; Skrzypczak-Zielińska, M.; Drwęska-Matelska, N.; Marcinkowska, M.; Eder, P.; Łykowska-Szuber, L.; Wysocka, E.; et al. Bone Metabolism and the c.-223C > T Polymorphism in the 5′UTR Region of the Osteoprotegerin Gene in Patients with Inflammatory Bowel Disease. Calcif. Tissue Int. 2016, 99, 616–624. [Google Scholar] [CrossRef]
- Lima, C.A.; Lyra, A.C.; Rocha, R.; Santana, G.O. Risk Factors for Osteoporosis in Inflammatory Bowel Disease Patients. World J. Gastrointest. Pathophysiol. 2015, 6, 210–218. [Google Scholar] [CrossRef]
- Kirchengast, S. Bone Loss and Physical Activity—A Bio Anthropological Perspective. J. Osteoporos. Phys. Act 2016. [Google Scholar] [CrossRef]
- Li, H.; Wallin, M.; Barregard, L.; Sallsten, G.; Lundh, T.; Ohlsson, C.; Mellström, D.; Andersson, E.M. Smoking-Induced Risk of Osteoporosis Is Partly Mediated by Cadmium From Tobacco Smoke: The MrOS Sweden Study. J. Bone Miner. Res. 2020, 35, 1424–1429. [Google Scholar] [CrossRef]
- Thomas, T.; Chandan, J.S.; Li, V.S.W.; Lai, C.Y.; Tang, W.; Bhala, N.; Kaplan, G.G.; Ng, S.C.; Ghosh, S. Global Smoking Trends in Inflammatory Bowel Disease: A Systematic Review of Inception Cohorts. PLoS ONE 2019, 14, e0221961. [Google Scholar] [CrossRef]
- Sole, K. Infliximab Increases Bone Mineral Density in Patients with Rheumatoid Arthritis. Nat. Clin. Pract. Rheumatol. 2006, 2, 120. [Google Scholar] [CrossRef]
- Bernstein, M.; Irwin, S.; Greenberg, G.R. Maintenance Infliximab Treatment Is Associated with Improved Bone Mineral Density in Crohn’s Disease. Am. J. Gastroenterol. 2005, 100, 2031–2035. [Google Scholar] [CrossRef]
- Bekheirnia, M.R.; Shamshirsaz, A.A.; Kamgar, M.; Bouzari, N.; Erfanzadeh, G.; Pourzahedgilani, N.; Tabatabaie, S.M.; Abdollah Shamshirsaz, A.; Kimiagar, M.; Ezzati, F.; et al. Serum Zinc and Its Relation to Bone Mineral Density in Beta-Thalassemic Adolescents. Biol. Trace Elem. Res. 2004, 97, 215–224. [Google Scholar] [CrossRef]
- Palacios, C. The Role of Nutrients in Bone Health, from A to Z. Crit. Rev. Food Sci. Nutr. 2006, 46, 621–628. [Google Scholar] [CrossRef]
- Yamaguchi, M. Role of Nutritional Zinc in the Prevention of Osteoporosis. Mol. Cell. Biochem. 2010, 338, 241–254. [Google Scholar] [CrossRef]
- Tucker, K.L. Vegetarian Diets and Bone Status. Am. J. Clin. Nutr. 2014, 100 (Suppl. 1), 329S–335S. [Google Scholar] [CrossRef]
- Santucci, N.R.; Alkhouri, R.H.; Baker, R.D.; Baker, S.S. Vitamin and Zinc Status Pretreatment and Posttreatment in Patients with Inflammatory Bowel Disease. J. Pediatr. Gastroenterol. Nutr. 2014, 59, 455–457. [Google Scholar] [CrossRef]
- Naber, T.H.; Van den Hamer, C.J.; Baadenhuysen, H.; Jansen, J.B. The Value of Methods to Determine Zinc Deficiency in Patients with Crohn’s Disease. Scand. J. Gastroenterol. 1998, 33, 514–523. [Google Scholar] [CrossRef]
- Sanna, A.; Firinu, D.; Zavattari, P.; Valera, P. Zinc Status and Autoimmunity: A Systematic Review and Meta-Analysis. Nutrients 2018, 10, 68. [Google Scholar] [CrossRef]
- Xiong, Y.; Wang, Y.; Wu, J.; He, H.; Wang, N.; Lei, G. [Cross-sectional association between dietary zinc intake and phalangeal osteoporosis]. Zhong Nan Da Xue Xue Bao Yi Xue Ban 2019, 44, 784–789. [Google Scholar] [CrossRef]
- Hyun, T.H.; Barrett-Connor, E.; Milne, D.B. Zinc Intakes and Plasma Concentrations in Men with Osteoporosis: The Rancho Bernardo Study. Am. J. Clin. Nutr. 2004, 80, 715–721. [Google Scholar] [CrossRef] [PubMed]
- Gür, A.; Colpan, L.; Nas, K.; Cevik, R.; Saraç, J.; Erdoğan, F.; Düz, M.Z. The Role of Trace Minerals in the Pathogenesis of Postmenopausal Osteoporosis and a New Effect of Calcitonin. J. Bone Miner. Metab. 2002, 20, 39–43. [Google Scholar] [CrossRef]
- Mutlu, M.; Argun, M.; Kilic, E.; Saraymen, R.; Yazar, S. Magnesium, Zinc and Copper Status in Osteoporotic, Osteopenic and Normal Post-Menopausal Women. J. Int. Med. Res. 2007, 35, 692–695. [Google Scholar] [CrossRef]
- Zofková, I.; Nemcikova, P.; Matucha, P. Trace Elements and Bone Health. Clin. Chem. Lab. Med. CCLM 2013, 51, 1555–1561. [Google Scholar] [CrossRef]
- Pepa, G.D.; Brandi, M.L. Microelements for Bone Boost: The Last but Not the Least. Clin. Cases Miner. Bone Metab. 2016, 13, 181–185. [Google Scholar] [CrossRef] [PubMed]
- Qu, X.; He, Z.; Qiao, H.; Zhai, Z.; Mao, Z.; Yu, Z.; Dai, K. Serum Copper Levels Are Associated with Bone Mineral Density and Total Fracture. J. Orthop. Transl. 2018, 14, 34–44. [Google Scholar] [CrossRef]
- Mir, E.; Hossein-nezhad, A.; Bahrami, A.; Bekheirnia, M.R.; Javadi, E.; Naderi, A.A.; Larijani, B. Adequate Serum Copper Concentration Could Improve Bone Density, Postpone Bone Loss and Protect Osteoporosis in Women. Iran. J. Public Health 2007, 36, 24–29. [Google Scholar]
- Royer, A.; Sharman, T. Copper Toxicity. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2020. [Google Scholar]
- Głąbska, D.; Guzek, D.; Lech, G. Analysis of the Nutrients and Food Products Intake of Polish Males with Ulcerative Colitis in Remission. Nutrients 2019, 11, 2333. [Google Scholar] [CrossRef]
- Poursadegh, F.; Ahadi, M.; Vosoughinia, H.; Salehi, M.; Beheshti Namdar, A.; Farzanehfar, M.R.; Memar, B.; Ziaolhagh, R. A STROBE Compliant Observational Study on Trace Elements in Patients with Ulcerative Colitis and Their Relationship with Disease Activity. Medicine (Baltimore) 2018, 97, e13523. [Google Scholar] [CrossRef] [PubMed]
- Ojuawo, A.; Keith, L. The Serum Concentrations of Zinc, Copper and Selenium in Children with Inflammatory Bowel Disease. Cent. Afr. J. Med. 2002, 48, 116–119. [Google Scholar]
- Sierpinska, T.; Konstantynowicz, J.; Orywal, K.; Golebiewska, M.; Szmitkowski, M. Copper Deficit as a Potential Pathogenic Factor of Reduced Bone Mineral Density and Severe Tooth Wear. Osteoporos. Int. J. Establ. Result Coop. Eur. Found. Osteoporos. Natl. Osteoporos. Found. USA 2014, 25, 447–454. [Google Scholar] [CrossRef] [PubMed]
- Zeng, H.; Cao, J.J.; Combs, G.F. Selenium in Bone Health: Roles in Antioxidant Protection and Cell Proliferation. Nutrients 2013, 5, 97–110. [Google Scholar] [CrossRef]
- Navarro-Alarcon, M.; Cabrera-Vique, C. Selenium in Food and the Human Body: A Review. Sci. Total Environ. 2008, 400, 115–141. [Google Scholar] [CrossRef]
- Kieliszek, M.; Błażejak, S. Current Knowledge on the Importance of Selenium in Food for Living Organisms: A Review. Molecules 2016, 21, 609. [Google Scholar] [CrossRef]
- Han, Y.M.; Yoon, H.; Lim, S.; Sung, M.-K.; Shin, C.M.; Park, Y.S.; Kim, N.; Lee, D.H.; Kim, J.S. Risk Factors for Vitamin D, Zinc, and Selenium Deficiencies in Korean Patients with Inflammatory Bowel Disease. Gut Liver 2017, 11, 363–369. [Google Scholar] [CrossRef]
- Beukhof, C.M.; Medici, M.; Van den Beld, A.W.; Hollenbach, B.; Hoeg, A.; Visser, W.E.; De Herder, W.W.; Visser, T.J.; Schomburg, L.; Peeters, R.P. Selenium Status Is Positively Associated with Bone Mineral Density in Healthy Aging European Men. PLoS ONE 2016, 11, e0152748. [Google Scholar] [CrossRef]
- Wang, Y.; Xie, D.; Li, J.; Long, H.; Wu, J.; Wu, Z.; He, H.; Wang, H.; Yang, T.; Wang, Y. Association between Dietary Selenium Intake and the Prevalence of Osteoporosis: A Cross-Sectional Study. BMC Musculoskelet. Disord. 2019, 20, 585. [Google Scholar] [CrossRef] [PubMed]
- Arikan, D.C.; Coskun, A.; Ozer, A.; Kilinc, M.; Atalay, F.; Arikan, T. Plasma Selenium, Zinc, Copper and Lipid Levels in Postmenopausal Turkish Women and Their Relation with Osteoporosis. Biol. Trace Elem. Res. 2011, 144, 407–417. [Google Scholar] [CrossRef] [PubMed]
- Odabasi, E.; Turan, M.; Aydin, A.; Akay, C.; Kutlu, M. Magnesium, Zinc, Copper, Manganese, and Selenium Levels in Postmenopausal Women with Osteoporosis. Can Magnesium Play a Key Role in Osteoporosis? Ann. Acad. Med. Singapore 2008, 37, 564–567. [Google Scholar]
- Pedrera-Zamorano, J.D.; Calderon-García, J.F.; Roncero-Martin, R.; Mañas-Nuñez, P.; Moran, J.M.; Lavado-Garcia, J.M. The Protective Effect of Calcium on Bone Mass in Postmenopausal Women with High Selenium Intake. J. Nutr. Health Aging 2012, 16, 743–748. [Google Scholar] [CrossRef]
- Abbaspour, N.; Hurrell, R.; Kelishadi, R. Review on Iron and Its Importance for Human Health. J. Res. Med. Sci. Off. J. Isfahan Univ. Med. Sci. 2014, 19, 164–174. [Google Scholar]
- Balogh, E.; Paragh, G.; Jeney, V. Influence of Iron on Bone Homeostasis. Pharmaceuticals 2018, 11, 107. [Google Scholar] [CrossRef]
- Imel, E.A.; Liu, Z.; McQueen, A.K.; Acton, D.; Acton, A.; Padgett, L.R.; Peacock, M.; Econs, M.J. Serum Fibroblast Growth Factor 23, Serum Iron and Bone Mineral Density in Premenopausal Women. Bone 2016, 86, 98–105. [Google Scholar] [CrossRef]
- Kim, B.-J.; Ahn, S.H.; Bae, S.J.; Kim, E.H.; Lee, S.-H.; Kim, H.-K.; Choe, J.W.; Koh, J.-M.; Kim, G.S. Iron Overload Accelerates Bone Loss in Healthy Postmenopausal Women and Middle-Aged Men: A 3-Year Retrospective Longitudinal Study. J. Bone Miner. Res. Off. J. Am. Soc. Bone Miner. Res. 2012, 27, 2279–2290. [Google Scholar] [CrossRef]
- Madanchi, M.; Fagagnini, S.; Fournier, N.; Biedermann, L.; Zeitz, J.; Battegay, E.; Zimmerli, L.; Vavricka, S.R.; Rogler, G.; Scharl, M.; et al. The Relevance of Vitamin and Iron Deficiency in Patients with Inflammatory Bowel Diseases in Patients of the Swiss IBD Cohort. Inflamm. Bowel Dis. 2018, 24, 1768–1779. [Google Scholar] [CrossRef] [PubMed]
- González Alayón, C.; Pedrajas Crespo, C.; Marín Pedrosa, S.; Benítez, J.M.; Iglesias Flores, E.; Salgueiro Rodríguez, I.; Medina Medina, R.; García-Sánchez, V. Prevalence of Iron Deficiency without Anaemia in Inflammatory Bowel Disease and Impact on Health-Related Quality of Life. Gastroenterol. Hepatol. 2018, 41, 22–29. [Google Scholar] [CrossRef] [PubMed]
- Khalili, H.; De Silva, P.S.; Ananthakrishnan, A.N.; Lochhead, P.; Joshi, A.; Garber, J.J.; Richter, J.R.; Sauk, J.; Chan, A.T. Dietary Iron and Heme Iron Consumption, Genetic Susceptibility, and Risk of Crohn’s Disease and Ulcerative Colitis. Inflamm. Bowel Dis. 2017, 23, 1088–1095. [Google Scholar] [CrossRef]
- Maurer, J.; Harris, M.M.; Stanford, V.A.; Lohman, T.G.; Cussler, E.; Going, S.B.; Houtkooper, L.B. Dietary Iron Positively Influences Bone Mineral Density in Postmenopausal Women on Hormone Replacement Therapy. J. Nutr. 2005, 135, 863–869. [Google Scholar] [CrossRef]
- Harris, M.M.; Houtkooper, L.B.; Stanford, V.A.; Parkhill, C.; Weber, J.L.; Flint-Wagner, H.; Weiss, L.; Going, S.B.; Lohman, T.G. Dietary Iron Is Associated with Bone Mineral Density in Healthy Postmenopausal Women. J. Nutr. 2003, 133, 3598–3602. [Google Scholar] [CrossRef]
- Kim, H.-S.; Park, H.-M.; Lee, H.S.; Lee, Y.-J. Hemoglobin Levels and Low Bone Mineral Density in Non-Anemic Older Adults: Secondary Analysis of the Korean National Health and Nutrition Examination Survey. Exp. Gerontol. 2019, 126, 110706. [Google Scholar] [CrossRef] [PubMed]
- Lee, K.S.; Jang, J.S.; Lee, D.R.; Kim, Y.H.; Nam, G.E.; Han, B.-D.; Do Han, K.; Cho, K.H.; Kim, S.M.; Choi, Y.S.; et al. Serum Ferritin Levels Are Positively Associated with Bone Mineral Density in Elderly Korean Men: The 2008-2010 Korea National Health and Nutrition Examination Surveys. J. Bone Miner. Metab. 2014, 32, 683–690. [Google Scholar] [CrossRef]
- Ohta, H.; Ichikawa, M.; Seki, Y. Effects of Cadmium Intake on Bone Metabolism of Mothers during Pregnancy and Lactation. Tohoku J. Exp. Med. 2002, 196, 33–42. [Google Scholar] [CrossRef]
- Chunhabundit, R. Cadmium Exposure and Potential Health Risk from Foods in Contaminated Area, Thailand. Toxicol. Res. 2016, 32, 65–72. [Google Scholar] [CrossRef] [PubMed]
- Engström, A.; Michaëlsson, K.; Vahter, M.; Julin, B.; Wolk, A.; Åkesson, A. Associations between Dietary Cadmium Exposure and Bone Mineral Density and Risk of Osteoporosis and Fractures among Women. Bone 2012, 50, 1372–1378. [Google Scholar] [CrossRef] [PubMed]
- Lavado-García, J.M.; Puerto-Parejo, L.M.; Roncero-Martín, R.; Moran, J.M.; Pedrera-Zamorano, J.D.; Aliaga, I.J.; Leal-Hernández, O.; Canal-Macias, M.L. Dietary Intake of Cadmium, Lead and Mercury and Its Association with Bone Health in Healthy Premenopausal Women. Int. J. Environ. Res. Public. Health 2017, 14, 1437. [Google Scholar] [CrossRef]
- Zhu, G.; Wang, H.; Shi, Y.; Weng, S.; Jin, T.; Kong, Q.; Nordberg, G.F. Environmental Cadmium Exposure and Forearm Bone Density. Biometals Int. J. Role Met. Ions Biol. Biochem. Med. 2004, 17, 499–503. [Google Scholar] [CrossRef] [PubMed]
- Price, C.T.; Koval, K.J.; Langford, J.R. Silicon: A Review of Its Potential Role in the Prevention and Treatment of Postmenopausal Osteoporosis. Int. J. Endocrinol. 2013, 2013, 316783. [Google Scholar] [CrossRef] [PubMed]
- Jugdaohsingh, R. Silicon and Bone Health. J. Nutr. Health Aging 2007, 11, 99–110. [Google Scholar]
- Jugdaohsingh, R.; Tucker, K.L.; Qiao, N.; Cupples, L.A.; Kiel, D.P.; Powell, J.J. Dietary Silicon Intake Is Positively Associated with Bone Mineral Density in Men and Premenopausal Women of the Framingham Offspring Cohort. J. Bone Miner. Res. Off. J. Am. Soc. Bone Miner. Res. 2004, 19, 297–307. [Google Scholar] [CrossRef] [PubMed]
- Li, Z.; Karp, H.; Zerlin, A.; Lee, T.Y.A.; Carpenter, C.; Heber, D. Absorption of Silicon from Artesian Aquifer Water and Its Impact on Bone Health in Postmenopausal Women: A 12 Week Pilot Study. Nutr. J. 2010, 9, 44. [Google Scholar] [CrossRef]
- Bae, Y.-J.; Kim, J.-Y.; Choi, M.-K.; Chung, Y.-S.; Kim, M.-H. Short-Term Administration of Water-Soluble Silicon Improves Mineral Density of the Femur and Tibia in Ovariectomized Rats. Biol. Trace Elem. Res. 2008, 124, 157–163. [Google Scholar] [CrossRef] [PubMed]
- Everett, E.T. Fluoride’s Effects on the Formation of Teeth and Bones, and the Influence of Genetics. J. Dent. Res. 2011, 90, 552–560. [Google Scholar] [CrossRef]
- Vestergaard, P.; Jorgensen, N.R.; Schwarz, P.; Mosekilde, L. Effects of Treatment with Fluoride on Bone Mineral Density and Fracture Risk--a Meta-Analysis. Osteoporos. Int. J. Establ. Result Coop. Eur. Found. Osteoporos. Natl. Osteoporos. Found. USA 2008, 19, 257–268. [Google Scholar] [CrossRef]
- Kanduti, D.; Sterbenk, P.; Artnik, B. Fluoride: A review of use and effects on health. Mater. Socio-Medica 2016, 28, 133–137. [Google Scholar] [CrossRef]
- Von Tirpitz, C.; Klaus, J.; Steinkamp, M.; Hofbauer, L.C.; Kratzer, W.; Mason, R.; Boehm, B.O.; Adler, G.; Reinshagen, M. Therapy of Osteoporosis in Patients with Crohn’s Disease: A Randomized Study Comparing Sodium Fluoride and Ibandronate. Aliment. Pharmacol. Ther. 2003, 17, 807–816. [Google Scholar] [CrossRef] [PubMed]
- Abitbol, V.; Mary, J.Y.; Roux, C.; Soulé, J.C.; Belaiche, J.; Dupas, J.-L.; Gendre, J.P.; Lerebours, E.; Chaussade, S. Groupe D’etudes Thérapeutiques des Affections Inflammatoires Digestives (GETAID) Osteoporosis in Inflammatory Bowel Disease: Effect of Calcium and Vitamin D with or without Fluoride. Aliment. Pharmacol. Ther. 2002, 16, 919–927. [Google Scholar] [CrossRef]
- Sowers, M.; Whitford, G.M.; Clark, M.K.; Jannausch, M.L. Elevated Serum Fluoride Concentrations in Women Are Not Related to Fractures and Bone Mineral Density. J. Nutr. 2005, 135, 2247–2252. [Google Scholar] [CrossRef]
- Phipps, K.R.; Orwoll, E.S.; Mason, J.D.; Cauley, J.A. Community Water Fluoridation, Bone Mineral Density, and Fractures: Prospective Study of Effects in Older Women. BMJ 2000, 321, 860–864. [Google Scholar] [CrossRef]
- Kasaikina, M.V.; Kravtsova, M.A.; Lee, B.C.; Seravalli, J.; Peterson, D.A.; Walter, J.; Legge, R.; Benson, A.K.; Hatfield, D.L.; Gladyshev, V.N. Dietary Selenium Affects Host Selenoproteome Expression by Influencing the Gut Microbiota. FASEB J. 2011, 25, 2492–2499. [Google Scholar] [CrossRef] [PubMed]
- Zhai, Q.; Cen, S.; Li, P.; Tian, F.; Zhao, J.; Zhang, H.; Chen, W. Effects of Dietary Selenium Supplementation on Intestinal Barrier and Immune Responses Associated with Its Modulation of Gut Microbiota. Environ. Sci. Technol. Lett. 2018, 5, 724–730. [Google Scholar] [CrossRef]
- Starke, I.C.; Pieper, R.; Neumann, K.; Zentek, J.; Vahjen, W. The Impact of High Dietary Zinc Oxide on the Development of the Intestinal Microbiota in Weaned Piglets. FEMS Microbiol. Ecol. 2014, 87, 416–427. [Google Scholar] [CrossRef]
- Shao, Y.; Lei, Z.; Yuan, J.; Yang, Y.; Guo, Y.; Zhang, B. Effect of Zinc on Growth Performance, Gut Morphometry, and Cecal Microbial Community in Broilers Challenged with Salmonella Enterica Serovar Typhimurium. J. Microbiol. 2014, 52, 1002–1011. [Google Scholar] [CrossRef]
- Reed, S.; Neuman, H.; Moscovich, S.; Glahn, R.; Koren, O.; Tako, E. Chronic Zinc Deficiency Alters Chick Gut Microbiota Composition and Function. Nutrients 2015, 7, 9768–9784. [Google Scholar] [CrossRef] [PubMed]
- Tang, M.; Frank, D.; Hendricks, A.; Ir, D.; Esamai, F.; Liechty, E.; Hambidge, K.; Krebs, N. Iron in Micronutrient Powder Promotes an Unfavorable Gut Microbiota in Kenyan Infants. Nutrients 2017, 9, 776. [Google Scholar] [CrossRef] [PubMed]
- Zimmermann, M.B.; Chassard, C.; Rohner, F.; N’Goran, E.K.; Nindjin, C.; Dostal, A.; Utzinger, J.; Ghattas, H.; Lacroix, C.; Hurrell, R.F. The Effects of Iron Fortification on the Gut Microbiota in African Children: A Randomized Controlled Trial in Côte d’Ivoire. Am. J. Clin. Nutr. 2010, 92, 1406–1415. [Google Scholar] [CrossRef] [PubMed]
- Qasem, W.; Azad, M.B.; Hossain, Z.; Azad, E.; Jorgensen, S.; Castillo San Juan, S.; Cai, C.; Khafipour, E.; Beta, T.; Roberts, L.J.; et al. Assessment of Complementary Feeding of Canadian Infants: Effects on Microbiome & Oxidative Stress, a Randomized Controlled Trial. BMC Pediatr. 2017, 17, 54. [Google Scholar] [CrossRef]
- Fang, S.; Zhuo, Z.; Yu, X.; Wang, H.; Feng, J. Oral Administration of Liquid Iron Preparation Containing Excess Iron Induces Intestine and Liver Injury, Impairs Intestinal Barrier Function and Alters the Gut Microbiota in Rats. J. Trace Elem. Med. Biol. 2018, 47, 12–20. [Google Scholar] [CrossRef]
- Kortman, G.A.M.; Dutilh, B.E.; Maathuis, A.J.H.; Engelke, U.F.; Boekhorst, J.; Keegan, K.P.; Nielsen, F.G.G.; Betley, J.; Weir, J.C.; Kingsbury, Z.; et al. Microbial Metabolism Shifts Towards an Adverse Profile with Supplementary Iron in the TIM-2 In Vitro Model of the Human Colon. Front. Microbiol. 2016, 6. [Google Scholar] [CrossRef]
- Dekker Nitert, M.; Gomez-Arango, L.F.; Barrett, H.L.; McIntyre, H.D.; Anderson, G.J.; Frazer, D.M.; Callaway, L.K. Iron Supplementation Has Minor Effects on Gut Microbiota Composition in Overweight and Obese Women in Early Pregnancy. Br. J. Nutr. 2018, 120, 283–289. [Google Scholar] [CrossRef]
- Seura, T.; Yoshino, Y.; Fukuwatari, T. The Relationship between Habitual Dietary Intake and Gut Microbiota in Young Japanese Women. J. Nutr. Sci. Vitaminol. 2017, 63, 396–404. [Google Scholar] [CrossRef]
- Martin, O.C.B.; Olier, M.; Ellero-Simatos, S.; Naud, N.; Dupuy, J.; Huc, L.; Taché, S.; Graillot, V.; Levêque, M.; Bézirard, V.; et al. Haem Iron Reshapes Colonic Luminal Environment: Impact on Mucosal Homeostasis and Microbiome through Aldehyde Formation. Microbiome 2019, 7, 72. [Google Scholar] [CrossRef] [PubMed]
- Otten, J.J.; Hellwig, J.P.; Meyers, L.D. (Eds.) Dietary Reference Intakes: The Essential Guide to Nutrient Requirements; National Academy of Sciences: Washington, DC, USA, 2006. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Supplemented Micronutrients | Strain Growth | Reduction of Stains | Reference |
|---|---|---|---|
| Selenium | Akkermansia Turicibacter | Dorea Mucispirillum | Zhai, Q. [92] |
| Zinc | Lactobacillus | Salmonella sp. | Starke, I.C. [93] Shao, Y. [94] |
| Iron | Bacteroidetes * Bifidobacterium * Firmicutes | Bifidobacteriacea * Firmicutes | Qasem, W. [98] Seura, T. [102] Martin, O.C.B. [103] |
| Micronutrient | RDA for an Adult [104] | Food Sources | Deficiency in IBD | Association with Osteoporosis |
|---|---|---|---|---|
| Zinc | Women—8 mg/d Men—11 mg/d | meat, nuts, beans and whole grain products | Santucci et al., 2014 [38] Naber et al., 1998 [39] Sanna et al., 2018 [40] | Xiong, et al., 2019 [41] Hyun, et al., 2004 [42] Gür, et al., 2002 [43] Mutlu, et al., 2007 [44] |
| Copper | 900 mg/d | meat, seafood, nuts and grain | Ojuawo et al., 2002 [52] | Beukhof, et al., 2016 [58] Wang, et al., 2019 [59] |
| Selenium | 55 mg/d | plant and animal products (the content of Se in food is various) | Poursadegh et al., 2018 [51] Ojuawo et al., 2002 [52] Han et al., 2017 [57] | Beukhof, et al., 2016 [58] Wang, et al., 2019 [59] |
| Iron | Men—8 mg/d Women—18 mg/d (8 mg/d for women over 51 years old) | heme (meat, fish) and non-heme (grain, legumes, vegetables, fruits) | Madanchi et al., 2018 [67] González Alayón et al., 2018 [68] | Maurer, et al., 2005 [70] Harris, et al., 2003 [71] |
| Cadmium | No data | seafood, meat, vegetables, grain and rice | No data | Engström, et al., 2012 [76] Zhu, et al., 2004 [78] |
| Silicon | No data | plant products (cereals, grains, some fruit and vegetables), dairy products and meat | No data | Jugdaohsingh, et al., 2004 [81] Bae, et al., 2008 [83] |
| Fluorine * | Men—4 mg/d Women—3 mg/d | black and green tea, sea food and wine | No data | Vestergaard, et al., 2008 [85] Phipps, et al., 2000 [90] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ratajczak, A.E.; Rychter, A.M.; Zawada, A.; Dobrowolska, A.; Krela-Kaźmierczak, I. Do Only Calcium and Vitamin D Matter? Micronutrients in the Diet of Inflammatory Bowel Diseases Patients and the Risk of Osteoporosis. Nutrients 2021, 13, 525. https://doi.org/10.3390/nu13020525
Ratajczak AE, Rychter AM, Zawada A, Dobrowolska A, Krela-Kaźmierczak I. Do Only Calcium and Vitamin D Matter? Micronutrients in the Diet of Inflammatory Bowel Diseases Patients and the Risk of Osteoporosis. Nutrients. 2021; 13(2):525. https://doi.org/10.3390/nu13020525
Chicago/Turabian StyleRatajczak, Alicja Ewa, Anna Maria Rychter, Agnieszka Zawada, Agnieszka Dobrowolska, and Iwona Krela-Kaźmierczak. 2021. "Do Only Calcium and Vitamin D Matter? Micronutrients in the Diet of Inflammatory Bowel Diseases Patients and the Risk of Osteoporosis" Nutrients 13, no. 2: 525. https://doi.org/10.3390/nu13020525
APA StyleRatajczak, A. E., Rychter, A. M., Zawada, A., Dobrowolska, A., & Krela-Kaźmierczak, I. (2021). Do Only Calcium and Vitamin D Matter? Micronutrients in the Diet of Inflammatory Bowel Diseases Patients and the Risk of Osteoporosis. Nutrients, 13(2), 525. https://doi.org/10.3390/nu13020525