Abstract
Multiple surgical strategies are available for managing the infected diabetic foot at risk for amputation. The authors present their experience with the closed instillation system in the management of 30 such cases in 29 patients over a 5-year period. Data were collected from the hospital records of neuropathic patients presenting with deep-plantar-space infections or presumed acute osteomyelitis. All 29 patients were male; 57% had marginal or poor vascular supply, and 83% were nutritionally compromised or had proteinuria. At the conclusion of the study, 34% of the patients were dead, reflecting the severity of comorbid conditions found in this population. Despite the marginal healing capacity of these patients, the procedure had a 90% success rate, as defined by expeditious return to prior level of functioning and residential living situation without need for re-operation or higher-level amputation.
The human and economic burden of the diabetic foot at risk for infection, ulceration, or amputation has been well documented.[1,2] For example, the Veterans Affairs system spends $341 million annually on the care of ulcers and amputations related to diabetes.[3] Of particular concern are deep-space infections and acute pedal osteomyelitis in this population. For the majority of patients who present with these limbthreatening conditions, surgical decompression with aggressive debridement of infected and necrotic tissues is the preferred treatment.[4]
Controversy abounds over how best to manage the open wound that results from incision and drainage of the infected foot.[5,6,7,8,9] The spectrum of options runs from proximal high-level amputation far from the site of infection to complete primary closure at the site of incision and drainage.[7,10,11] This lack of consensus may manifest itself in the observed geographic variations in rates of amputation. A study from the Netherlands reported a fourfold variation in rates of nontraumatic amputation in diabetic patients by geographic region, as compared with a twofold variation in rates of nontraumatic amputation in nondiabetic patients.[12] Variations in procedure rates are driven by patient characteristics, availability of resources, and degree of physician uncertainty regarding the outcome.[13] The authors present their experience with the closed instillation system in the hope of reducing the physician uncertainty that may lead to amputation of the at-risk infected foot.
A successful management strategy for these difficult wounds will 1) effectively manage the infection without re-infection, re-operation, or amputation at a higher level; 2) allow an outcome whereby the patient returns to preoperative functional and residential living status as quickly as possible (especially important given the limited life expectancy of these patients) (Table 1); and 3) result in as little dependence as possible on the medical system as indicated by number of hospital days, number of clinic visits, wound-care intensity, and number of nursing-home days. When the spectrum of options is considered, it is clear that procedures that involve primary wound closure while retaining the weightbearing platform of the leg best meet these objectives.

Table 1.
Mortality Rates of Diabetic Patients with Severe Foot Disease.
Procedures that use primary closure also seem to be favored from the perspective of the wound environment. Wounds heal best in a moist, thermally insulated environment with low bacterial loads.[14] Although historically favored because of its perceived safety, secondary-intention healing does not provide these ideal wound conditions.[5,15] Also, there is increasing recognition of the risk that a chronic open wound, surgical or not, poses to a diabetic or systemically compromised patient.[16] There is still controversy regarding primary closure of acutely infected wounds, as it is considered by some to predispose the patient to incomplete resolution and recurrence of infection.[11,15] Several alternatives have been proposed that incorporate the benefits of primary closure yet feature improved safety profiles. One such alternative is the closed instillation system, which is a modification of Kritter’s technique.
In 1973, Kritter[6] first described his system for surgical management of the infected diabetic foot in a report of a series of 12 diabetic patients with foot infection. The approach presented here incorporates many of Kritter’s original thoughts on wound management, but also reflects logistic changes and current trends in the delivery of surgical care. This article describes the authors’ experience with a modified version of Kritter’s closed instillation system and suggests that this may be a valuable tool in achieving wound healing while minimizing the extent and rate of amputation in the infected diabetic foot.
The majority of published material relating to ingress and egress of antibiotic solution through an infected surgical wound was written in the early 1970s and has received little attention since that time. Perhaps the perceived safety of secondary-intention wound healing, lack of recognition of the sequelae of plantar scarring, and lack of monetary pressures dictating shorter hospital stays accounted for the absence of a stimulus for change in surgical practices.
Methods
A retrospective chart review was conducted of 30 procedures performed in 29 male patients over a 5year period (between 1993 and 1998). All patients presented to the high-risk foot clinic at the Veterans Affairs Medical Center in White River Junction, Vermont. This facility is currently a secondary-care center. Patients presented with deep-plantar-space infection of the foot, suspected acute pedal osteomyelitis, or both; 90% of patients had diabetes. The average age of the patients was 66 years (range, 39 to 89 years). All chart abstracts were performed or reviewed by one author (J.E.C.) to ensure consistency. Patient candidacy for the closed instillation procedure was determined by the two lead authors according to standardized criteria. All procedures were performed by either of the two lead authors.
Several patient characteristics were assessed in the chart review. Protective threshold was determined using a 5.07 Semmes-Weinstein monofilament. The plantar aspects of the hallux and the first and fifth metatarsal heads were examined. Loss of sensation in one or more of the six sites indicated a lack of protective threshold.[17] Vascular status was determined by a combination of two or more of the following: Doppler wave form, ankle-brachial index, toe pressure, transcutaneous oxygen tension, and whether a recent revascularization procedure was performed. All patients were stratified by wound-healing potential related to severity of vascular disease (Table 2). Patients with an “acceptable” rating had vascular-assessment results that conformed with accepted minimum values for amputation healing, according to published reports.[18,19,20,21,22] Patients with a “marginal” rating were unlikely to have amputation healing but warranted intervention on the basis of significant impact of a lower-extremity amputation.[23] Patients with a “poor” rating were those who would most likely only be considered for higher-level amputation in other institutions. These patients were given the option of having closed instillation intervention when the impact of high-level amputation would dramatically conflict with their life goals and when the likelihood of re-operation, with its attendant risks, was clearly understood. The patient breakdown by vascular status was 43% acceptable, 43% marginal, and 13% poor; 33% of the patients had undergone recent revascularization.
Table 2.
Rating Scale for Lower-Extremity Vascular Status.
The issue of recent or periamputation lower-extremity vascular surgery was part of the inclusion criteria for several reasons. There were two specific considerations related to recent revascularization, which the authors defined as procedures performed specifically for the presenting infection and subsequent need for foot debridement following a period of critical or relative ischemia. First, if a revascularization procedure was performed around the time of the foot amputation, there would not be sufficient time for the improved blood flow to remedy the damage caused by chronic suboptimal tissue oxygenation and malnutrition. Second, the reactive hyperemia commonly seen following revascularization may cause tension along a surgical wound in the foot due to edema that may predispose these wounds to re-infection. The authors are not suggesting that either of these considerations will affect the surgeon’s decision to intervene, but they may aid in preoperative risk assessment. No data were found to support or contradict the authors’ opinions on this matter.
Hemoglobin values were collected as a possible indicator of potential tissue oxygenation.[24] Forty-six percent of the patients in this study had hemoglobin levels below 12 g/dL. Renal function was assessed via tests of serum creatinine level and proteinuria (found in 40% of the patients in this study).[25] Nutritional status was determined by serum albumin level and absolute lymphocyte count.[26,27,28] The albumin level was less than 3 g/dL in 48% of the patients in this study and the total lymphocyte count was less than 1,500/µL in 67% of the patients.
Infection was monitored by means of white blood cell count, bone biopsy, wound culture, Gram’s stain, and measurement of body temperature. Data were collected on diabetic status, dispensation at discharge, and classification as a first or second procedure.
The main outcome measures were 1) level of independence as assessed by a comparison of level of functioning and residential living status with preoperative levels, and 2) the occurrence of re-operation or amputation at a higher level.
Technique
A closed instillation system with loose primary closure was implemented in this study. The particular technique derives directly from the work of Kritter[6] but features several notable differences (Table 3). At the beginning of the procedure the patient is prepared and draped at a level sufficiently proximal to allow access to all infected compartments of the foot and leg. The use of a tourniquet is contraindicated. The authors have found that exsanguinating an abscessed limb may cause transient septicemia, and assessing the viability of tissue is difficult without normal capillary bleeding. Incision planning is begun with thorough examination of the foot, in conjunction with radiographs, in an effort to discern visual and palpable signs of abscess. A simple stab incision was performed and appropriate cultures were taken when pus was expressed. Efforts were then directed toward a more formal incision and drainage of the foot in order to identify, open, and evacuate all pockets of abscess to prevent proximal spread of infection and diminish bacterial load. All tissues were debrided to bleeding in the well-vascularized patient, or at least to noninfected tissue otherwise, to promote healing and minimize the nidus for recurrent infection, and to control sepsis and its sequelae in these often very ill patients.5 At the conclusion of the debridement, “milking” of the leg in a proximal-to-distal direction was performed to ensure that no drainage remained hidden upstream of the surgical field.
Table 3.
Comparison of the Technique of Kritter[6] with the Modified Closed Instillation System.
Once the primary objectives of the incision and drainage were met, the wound was prepared for closure. Minimizing the bacterial load within the wound was considered to be critical, particularly when primary closure was planned. The use of saline wound irrigation has been shown to be effective in achieving that objective.[29] The mechanical debridement of a pulsatile lavage system was used for removal of bacteria from irregular wound beds while preserving viable tissues. The size of the wound dictates the amount of irrigant. Between 2 and 4 liters of normal saline was used, as there has been no benefit shown with the use of antibiotic solutions in the operative flush.[30] The proximal surgical bone margin was cultured for histopathologic examinination.
The freshly debrided and lavaged surgical site was then managed as a cleaner wound. All contaminated instrumentation was set aside and the outermost surgical gloves were removed. Hemostasis was attained and the wound margins were revised as deemed necessary. The wound was manipulated to determine the most advantageous alignment of tissues in planning primary closure. Judicious debridement of deeper viable tissues was performed if there was tension along the wound margin. Any such revisions were done with the long-term function of the foot in mind.
After a plan for closing the amputation site was finalized, the wound was loosely approximated with simple interrupted sutures of 4-0 nylon. No deep or absorbable sutures were placed. With all but two or three sutures remaining to be thrown, a 16-gauge angiocatheter with a suturable hub was introduced through the skin into the amputation site near its apex. The catheter was directed to allow dependent drainage of the gentamicin solution, which bathed the entire surgical wound by following the law of gravity. The tip of the catheter was identified within the foot and cut on a 45° bevel, which decreased the likelihood of occlusion. The remaining sutures were placed with care so as not to cause tamponade of the angiocatheter. The wound margins were coapted, but loosely enough to allow free egress of the gentamicin solution through the surgical wound. Figure 1 illustrates the placement of the angiocatheter. A 1-liter bag of normal saline with 80 mg of gentamicin was suspended from the intravenous solution–supporting pole and connected to the angiocatheter with extension tubing. This tubing allowed the ingress of fluid into the wound to be regulated by a patient-controlled anesthesia unit. The system was tested by opening the tubing and observing the flush of fluid through the wound. If this failed, the pole supporting the intravenous solution was raised higher to employ gravity and the catheter was slightly withdrawn, while being rotated, until it began to run.

Figure 1.
Closed instillation system in place following a transmetatarsal amputation. (From Connolly JE, McDaniel ND, Wrobel JS, et al: Creative foot salvage. Adv Vasc Surg 6: 231, 1998. Reprinted by permission.).
Once the system was operating correctly, the hub was sutured through the epidermis as an anchor. A 4 × 4-inch piece of gauze was cut 2 inches across and placed under the catheter in order to protect the skin from the hub. The dressing consisted of two layers. The first layer was a fluff dressing covered by Kling wrap (Johnson & Johnson Medical, Inc, Arlington, Texas) and marked with a skin marker. That portion of the dressing remained intact for 48 hours. The second absorbent layer was more fluff dressing, which was replaced by Kerlix (Kendall Health Care Products Co, Mansfield, Massachusetts), an absorbent gauze roll dressing, as it became saturated. Figure 2 depicts the materials typically used with this technique. The system was tested one more time in the operating room.

Figure 2.
Materials used in the closed instillation procedure: Kling wrap, tape, patient-controlled anesthesia unit tubing, gentamicin, cut 4 × 4-inch gauze, Kerlix, and surgical marking pen.
In the recovery room, the patient-controlled anesthesia unit was set to a rate of 1 liter/day. The dressing was reinforced as needed and changed during every nursing shift. Activity was restricted to complete bed rest while the catheter was in the foot. Vital signs and blood work were closely monitored for 48 hours to ensure that the acute infection was resolving. Appropriate deep vein thrombosis prophylaxis was implemented. When the dressing was removed, the foot appeared markedly macerated. This was completely self-limiting and was not a problem for any of the patients. As an adjunct to the local instillation of antibiotic, empiric intravenous antibiotics were initiated preoperatively and continued until removal of the dressing 2 days postoperatively. A dry, sterile dressing was applied to the foot and changed once daily until the maceration resolved.
There were several reasons why the catheter was left in place for 48 hours: 1) the time required for the antibiotic to have a bactericidal effect was at least 2 hours; 2) reduction of hematoma, most of which would be deposited in this time, was critical to infection control; and 3) tension was reduced across the surgical wound margins by reducing fluid collection in the early inflammatory stage of healing. After the 48-hour catheterization period, if the bone margins were clear of infection and the clinical and laboratory findings were favorable, patients were treated with a soft-tissue course of antibiotic as directed by culture results. This was generally a 7- to 10-day course of treatment, beginning with the time of surgery, and might have consisted of intravenous, followed by oral, antibiotics. If the bone culture and biopsy results were positive, oral antibiotics were continued for 1 month.[31]
Results
Patients who underwent the closed instillation procedure had a 90% success rate according to the study definition of return to preoperative ambulatory status and preoperative residential living status without need for re-operation or a higher-level amputation. Figure 3 indicates the locations and types of the procedures that were performed for these patients. Histopathology results revealed that 77% of bone specimens showed evidence of osteomyelitis. The white blood cell count was more than 10,000/µL in 50% of patients; positive wound culture was found in 96% of patients. All bone was resected where osseous margins demonstrated appropriate color, bleeding, and hardness. One-third of these patients had the procedure done as a secondary procedure. An initial incision and drainage procedure was deemed necessary as an ablative procedure in order to stabilize these patients. The wounds of the majority of these patients were closed when the patient was medically stable, regardless of the status of wound infection. Median follow-up time for the entire series of patients was 23 months (range, 3 to 65 months).
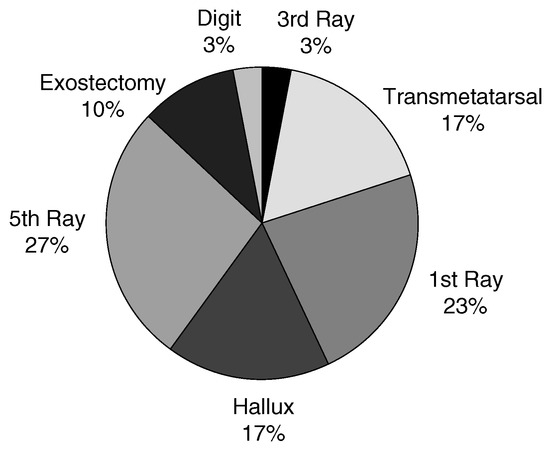
Figure 3.
Procedure types: anatomical distribution of amputations performed.
The procedure failed in three patients. Two patients required an above-the-knee amputation, and one patient required a below-the-knee amputation. All of these patients underwent amputation for chronic, nonhealing wounds long after the closed instillation procedure. The average time to amputation was 4 months (range, 2 to 6 months). Two of these patients were infected with methicillin-resistant Staphylococcus aureus. Table 4 summarizes the characteristics of the patients in whom the procedure failed.
Table 4.
Characteristics of the Patients in Whom the Procedure Failed.
The 90% success rate with the use of the safety standards established before performance of the procedure is notable. There were no perioperative deaths, no postoperative infections requiring re-operation, and no changes in renal function with the use of this technique.
Discussion
The 90% success rate of this procedure in this study seems high considering the underlying comorbid conditions and the disease severity of these patients. For example, 57% of patients had marginal or poor blood supply, 83% of patients had proteinuria (40%) or compromised nutritional status (48%), and 77% had positive results from bone biopsy for osteomyelitis. Since the inception of this work, 34% of patients have died as a result of their comorbid conditions, although this percentage includes one death that was due to homicide.
There are limitations to this study. First, it describes the preliminary experience of the authors with a highly selective, homogeneous patient population consisting of older white men admitted to a teaching hospital. Second, the authors were unable to determine number of foot-related hospital days from the chart reviews, although current health-care trends and the typical bimodal distribution of these data may preclude meaningful interpretation. Third, a precise return-to-function time could not be determined for all patients. Lastly, smoking status could not be determined for all patients.
To understand the rationale behind the closed instillation system, it must be recognized that the importance of local tissue concentrations of gentamicin probably surpasses that of systemic levels of antibiotics. One study involved rabbits with deep muscular wounds containing dead bone. The bone was inoculated with bacteria to induce osteomyelitis. The rabbits were treated with antibiotic beads, intravenous antibiotics, and a combination of the two. The bactericidal effect of the beads was the same with or without intravenous antibiotics.[32] Another method of increasing local tissue concentrations of antibiotics, retrograde venous perfusion, has shown benefit in human trials. Duration of therapy and critical complications of treatment were reduced when retrograde venous perfusion was added as adjunctive therapy.[33] As with antibiotic beads and retrograde venous perfusion, the closed instillation system with gentamicin elevates local tissue levels of antibiotic at the source of infection, and may therefore show many of the same benefits.
Delivery of gentamicin locally by means of solution is also unique to this technique. The environment created by instillation of a solution is very conducive to wound healing.[15] In the removal of exudate, local inflammation and tension about the wound are reduced. In the removal of hematoma, a potential nidus for infection is removed.[34] The moist environment prevents desiccation of tissues, and leaving the dressing in place for 48 hours allows the initial stages of wound healing to proceed undisturbed.
There is also evidence to support the selection of gentamicin specifically. The original work by Kritter[6] described the use of neomycin sulfate, which is no longer available because of its toxicity. Gentamicin is a water-soluble compound that displays concentration-dependent bactericidal activity.[35,36,37] Local instillation has a much broader spectrum of activity than does intravenous gentamicin, specifically with regard to many organisms commonly seen in diabetic foot wounds. Gritz et al,[30] in an in vitro study, demonstrated that, at the concentrations used in the present study and at a duration of more than 120 min, many Staphylococcus, Streptococcus, Enterococcus, and Pseudomonas species were sensitive to treatment. Also, persistent suppression of bacterial growth after exposure occurs with aminoglycosides and is referred to as the postantibiotic effect. It is believed that prolongation of exposure prolongs the postantibiotic effect.[30,37,38] Additionally, the postantibiotic effect for aminoglycosides is potentiated by the synergistic effect of host–leukocyte activity. It is believed that leukocytes have enhanced phagocytosis and killing activity after exposure to aminoglycosides.[35,36] Systemic levels of gentamicin are detectable with local irrigations, but elevated serum creatinine or other drug-induced side effects do not seem to occur.[39,40] The 80-mg dose used in this study is approximately 1 mg/kg. This is less than the current dosing recommendations for multiple daily dosing or single daily dosing of gentamicin of 2 to 3 mg/kg and 5 to 7 mg/kg, respectively.[35] The authors believe that this minimizes systemic toxicity as well.
The authors believe that primary closure with the closed instillation system offers many significant benefits. First, there is greater patient compliance with instructions to remain nonweightbearing, as the closed instillation system is in place for 48 hours, deterring ambulation. Second, minimal surgical scarring probably reduces the long-term risk of reulceration. Primary closure may also allow earlier return to weightbearing with less muscular atrophy and less need for rehabilitation, better glucose control, and less risk to the contralateral limb because of altered gait patterns. Third, less overall dependence on the medical system may result from shorter hospital stays and decreased need for intensive home-care nursing (ie, the number of visits and wound-care supplies for packing of open wounds). Primary closure increases the likelihood of healing in patients with vasculopathy,[41] and the immediate coverage of bone and deep tendon structures will minimize desiccation or re-infection from a nosocomial source. Lastly, the materials are inexpensive and widely available, and the technique is easily mastered.
The closed instillation technique appears to be as effective as other procedures designed for primary closure of infected foot wounds. For example, one study reported a 78% healing rate with the use of conservative surgery. The surgeons removed only the infected portion of bone and did not specify number of recurrences or method of closure. The median antibiosis duration was 111 days.[42] Another study investigated outcomes for 35 diabetic patients who had undergone transmetatarsal amputation, with 69% of patients ultimately healing. The primary indications for surgery were infection (in 83% of the patients) and peripheral vascular disease (34%), with primary closure in 29% of the cases.[43] Another study involved 39 diabetic patients who underwent 42 procedures for nonhealing ulcers.[7] Every patient had a lower-extremity vascular reconstruction procedure. A variety of procedures (eg, metatarsal head resection, metatarsal osteotomy, and panmetatarsal head resection) were performed; 83% of the patients healed initially and 95% eventually healed. All procedures used primary closure, and patients were kept nonweightbearing for 2 to 8 weeks. Kumagai et al[8] reported the results of a study involving a two-stage delayed primary closure procedure for 37 wounds, in which 20 cases had bone biopsy results consistent with osteomyelitis. The first stage of the procedure used longitudinal elliptical incisions that completely excised the ulcer and progressed to healthy bone. The wound was packed and left open, and delayed primary closure followed 4 to 8 days later. All patients were kept nonweightbearing for 1 month, and the patients with positive biopsy results received intravenous antibiotics for 6 weeks. The researchers reported an 87% success rate, with an average healing time of 57 days.
The closed instillation procedure also appears to be as effective as bead therapy and instillation drainage therapy. One study found an 80% success rate using instillation drainage, and an 84% success rate using gentamicin–polymethyl methacrylate chains.[9] The combination of the results of these studies and the observed healing rate of 90% in the current study indicates that closed instillation should be considered a viable alternative for the closure of infected foot wounds.
At the authors’ institution, the closed instillation system has had good results in the most challenging patients; the procedure has often been used as a salvage procedure in patients for whom there is a strong likelihood of high-level amputation. Future work needs to be performed to provide a better understanding of what procedures work best in this fragile population of high-risk diabetic patients. For example, a randomized trial by surgeons using differing surgical techniques could be performed. This information might decrease surgeon uncertainty as to how to best manage these wounds and thereby help reduce geographic variations observed in diabetesrelated amputation rates. The authors believe that the ability to close these wounds successfully with closed instillation, even in the presence of frank abscess, is due largely to meticulous technique in performing the incision and drainage, diminishing bacterial load with pulse lavage, and attaining high local concentrations of antibiotic for a protracted period of time. This procedure compares favorably with other procedures used to primarily close infected foot wounds. This type of primary closure is often accomplished with one procedure, at minimal cost and time to the patient and surgeon.
Acknowledgments
Martha D. McDaniel, MD, for leadership in the development of the high-risk foot clinic at the authors’ institution, her support of management efforts for the patients treated there, and review of this manuscript; Rick Dow, MD, for inspiration for the genesis of this project; W. Charles Myers, DPM, for contributions during the developmental stages of this project.
References
- CLARK CM: The burden of diabetes: introductory remarks. Diabetes Care 1998, 21 (suppl), C1. [CrossRef]
- MAYFIELD, JA; REIBER, GE; SANDERS, LJ. ET AL: Preventive foot care in people with diabetes. Diabetes Care 1998, 21, 2161. [Google Scholar] [CrossRef]
- REIBER, GE. Diabetic foot care: financial implications and practice guidelines. Diabetes Care 1992, 15 (suppl), 29. [Google Scholar] [CrossRef]
- ENEROTH, M; APELQVIST, J. STENTSTROM A: Clinical characteristics and outcome in 223 diabetic patients with deep foot infections. Foot Ankle Int 1997, 18, 716. [Google Scholar] [CrossRef]
- SAGE R: “Surgery of the Infected Foot,” in Medical and Surgical Management of the Diabetic Foot; Kominsky, SJ, Ed.; CV Mosby: St Louis, 1994; p. 279. [Google Scholar]
- KRITTER AE: A technique for salvage of the infected diabetic gangrenous foot. Orthop Clin North Am 1973, 4, 21. [CrossRef]
- ROSENBLUM, BI; POMPOSELLI, FB; GIURINI, JM. ET AL: Maximizing foot salvage by a combined approach to foot ischemia and neuropathic ulceration in patients with diabetes: a five year experience. Diabetes Care 1994, 17, 983. [Google Scholar] [CrossRef]
- KUMAGAI, SG; MAHONEY, CR; FITZGIBBONS, TC. ET AL: Treatment of diabetic (neuropathic) foot ulcers with twostage debridement and closure. Foot Ankle Int 1998, 19, 160. [Google Scholar] [CrossRef] [PubMed]
- SCHMIDT, J; HACKENBROCH, MH; KUMM, D. ET AL: Is instillation drainage for the treatment of infected joints, bones, and soft tissues still up to date? Arch Orthop Trauma Surg 1996, 115, 149. [Google Scholar] [CrossRef] [PubMed]
- MARTIN, JD; DELBRIDGE, L; REEVE, TS. ET AL: Radical treatment of mal perforans in diabetic patients with arterial insufficiency. J Vasc Surg 1990, 12, 264. [Google Scholar] [CrossRef][Green Version]
- EFFENEY, DJ; LIM, RC. SCHECTER WP: Transmetatarsal amputation. Arch Surg 1977, 112, 1366. [Google Scholar] [CrossRef]
- VONHOUTUM, WH; LAVERY, LA. Regional variation in the incidence of diabetes-related amputations in the Netherlands. Diabetes Res Clin Pract 1996, 31, 125. [Google Scholar] [CrossRef]
- WENNBERG J: Understanding geographic variations in health care delivery. N Engl J Med 1999, 340, 52. [CrossRef] [PubMed]
- LADIN DA: Understanding dressings. Clin Plast Surg 1998, 25, 433. [CrossRef]
- SCHER, KS. STEELE FJ: The septic foot in patients with diabetes. Surgery 1988, 104, 661. [Google Scholar] [PubMed]
- PECORARO, RE; REIBER, GE; BURGESS, EM. Pathways to diabetic limb amputation: basis for prevention. Diabetes Care 1990, 13, 513. [Google Scholar] [CrossRef]
- OLMOS, PR; CATALAND, S; O’DORISIO, TM. ET AL: The SemmesWeinstein monofilament as a potential predictor of foot ulceration in patients with noninsulin-dependent diabetes. Diabetes Care 1992, 15, 1386. [Google Scholar]
- BALLARD, JL; EKE, CC; BUNT, TJ. ET AL: A prospective evaluation of transcutaneous oxygen measurements in the management of diabetic foot problems. J Vasc Surg 1995, 22, 485. [Google Scholar] [CrossRef] [PubMed]
- WAGNER FW: The dysvascular foot: a system for diagnosis and treatment. Foot Ankle 1981, 2, 64. [CrossRef]
- EUROPEAN SOCIETY OF VASCULAR SURGERY: Chronic critical leg ischaemia. Eur J Vasc Surg 1992, 6, 1.
- APELQVIST, J; CASTENFORS, J; LARSSON, J; et al. Prognostic value of systolic ankle and toe blood pressure levels in outcome of diabetic foot ulcer. Diabetes Care 1989, 12, 373. [Google Scholar] [CrossRef]
- VITTI, MJ; ROBINSON, DV; HAUER-JENSEN, M. ET AL: Wound healing in forefoot amputations: the predictive value of toe pressure. Ann Vasc Surg 1994, 8, 99. [Google Scholar] [CrossRef]
- WATERS, RL; PERRY, J; ANTONELLI, D; et al. Energy cost of walking of amputees: the influence of level of amputation. J Bone Joint Surg Am 1976, 58, 42. [Google Scholar] [CrossRef]
- LARSSON, J; AGRDH, CD; APELQVIST, J; ET, AL. Clinical characteristics in relation to final amputation level in diabetic patients with foot ulcers: a prospective study of healing below or above the ankle in 187 patients. Foot Ankle Int 1995, 16, 69. [Google Scholar] [CrossRef]
- APELQVIST, J; LARSSON, J; AGARDH, CD. Medical risk factors in diabetic patients with foot ulcers and severe peripheral vascular disease and their influence on outcome. J Diabetes Complications 1992, 6, 167. [Google Scholar] [CrossRef] [PubMed]
- DICKHAUT, SC; DELEE, JC; PAGE, CP. Nutritional status: importance in predicting wound-healing after amputation. J Bone Joint Surg Am 1984, 66, 71. [Google Scholar] [CrossRef]
- CATALDO, CB; DEBRUYNE, LK. WHITNEY EN: “Nutritional Intervention,”. In Nutrition and Diet Therapy: Principles and Practice, 4th Ed; Cataldo, CB, DeBruyne, LK, Whitney, EN, Eds.; West Publishing Co: Minneapolis, 1995; p. 352. [Google Scholar]
- PINZUR, M; KAMINSKY, M; SAGE, R. ET AL: Amputations at the middle level of the foot. J Bone Joint Surg Am 1986, 68, 1061. [Google Scholar] [CrossRef] [PubMed]
- BADIA, JM; TORRES, JM; TU, C. ET AL. Saline wound irrigation reduces the postoperative infection rate in guinea pigs. J Surg Res 1996, 63, 457. [Google Scholar] [CrossRef]
- GRITZ, DC; CEVALLOS, AV; SMOLIN, G; ET, AL. Antibiotic supplementation of intraocular irrigating solutions: an in vitro model of antibacterial action. Ophthalmology 1996, 103, 1204. [Google Scholar] [CrossRef]
- MADER, JT; ORITZ, M; CALHOUN, JH. Update on the diagnosis and management of osteomyelitis. Clin Podiatr Med Surg 1996, 13, 701. [Google Scholar] [CrossRef]
- CHEN, NT; HONG, HZ; HOOPER, DC; ET, AL. The effect of systemic antibiotic bacterial clearance wounds containing contaminated dead bone. Plast Reconstr Surg 1993, 92, 1305. [Google Scholar]
- EL-SARKY M EL S: Local intravenous therapy in chronic inflammatory and vascular disorders of the foot. Int Surg 1997, 82, 175.
- KRIZEK, TJ; DAVIS, JH. Effect of diabetes on experimental infection. Surg Forum 1964, 60. [Google Scholar]
- GONZALEZ, LS; SPENCER, JP. Aminoglycosides: a practical review. Am Fam Physician 1998, 58, 1811. [Google Scholar] [PubMed]
- MCEVOY GK: “Aminoglycosides,” in AHFS Drug Information, ed by GK McEvoy, p 56; American Society of Health-System Pharmacists: Bethesda, MD, 1997.
- LORTHOLARY O, TODD M, COHEN Y: Aminoglycosides. Med Clin North Am 1995, 79, 761. [CrossRef]
- VOGELMAN, B. CRAIG WA: Kinetics of antimicrobial activity. J Pediatr 1986, 108, 835. [Google Scholar] [CrossRef]
- KOPEL, ME; RIEMERSMA, L; FINLAYSON, DC. Gentamicin solution for mediastinal irrigation: systemic absorption, bactericidal activity, and toxicity. Ann Thorac Surg 1989, 48, 228. [Google Scholar] [CrossRef]
- BORTNEM, KD; WETMORE, RW; BLACKBURN, GW; et al. Analysis of therapeutic efficacy, cost, and safety of gentamicin lavage solution in orthopaedic surgery prophylaxis. Orthop Rev 1990, 19, 797. [Google Scholar]
- GIBBONS, GW. “Infection of the Diabetic Foot,” in Management of Diabetic Foot Problems, 2nd Ed; Kozak, GP, Campbell, DR, Frykberg, RG, Eds.; WB Saunders: Philadelphia, 1995; p. 121. [Google Scholar]
- HA VAN, G; SINEY, H; DANAN, JP; et al. Treatment of osteomyelitis in the diabetic foot. Diabetes Care 1996, 19, 1257. [Google Scholar] [CrossRef]
- HOSCH, J; QUIROGA, C; BOSMA, J; et al. Outcomes of transmetatarsal amputations in patients with diabetes mellitus. J Foot Ankle Surg 1997, 36, 430. [Google Scholar] [CrossRef] [PubMed]



© 2000 American Podiatric Medical Association