

Clin. Transl. Neurosci. 2026, 10(3), 22; https://doi.org/10.3390/ctn10030022 - 3 Aug 2026
Abstract
►
Show Figures
Recent developments in cognitive neuroscience, neuroimaging, and embodied cognition have stimulated growing interest in neuroscience-informed architecture. However, despite the rapid expansion of the field, neuroarchitectural scholarship remains conceptually fragmented and methodologically diverse, and its institutional evolution, thematic structure, and translational implications have not
[...] Read more.
Recent developments in cognitive neuroscience, neuroimaging, and embodied cognition have stimulated growing interest in neuroscience-informed architecture. However, despite the rapid expansion of the field, neuroarchitectural scholarship remains conceptually fragmented and methodologically diverse, and its institutional evolution, thematic structure, and translational implications have not been comprehensively synthesised. Using a narrative critical synthesis supported by translational qualitative structuring and conceptual synthesis, this study examines foundational publications, institutional documents, conference outputs, and applied studies that have shaped neuroscience-informed architecture since the early 2000s. The review identifies recurring thematic domains, including sensory perception, spatial cognition, emotion, empathy, embodied cognition, environmental behaviour, healthcare design, and evidence-based architectural practice. It indicates that ANFA-related scholarship has played a significant role in legitimising neuroscience as a relevant framework for understanding architectural experience and informing design practices in therapeutic, educational, and behavioural contexts. The review also highlights persistent methodological challenges in translating neuroscientific findings into architectural research, particularly given that architectural experience is multisensory, embodied, socially situated, and temporally dynamic. The study concludes that neuroscience-informed architecture should be understood not as a deterministic explanatory model but as a translational framework that connects neuroscientific knowledge with architectural theory and practice. This expanding evidence base calls for more ecologically valid, interdisciplinary, and methodologically rigorous research, while encouraging architects and practitioners to adopt evidence-based, human-centred design strategies that enhance health, well-being, and user experience across diverse built environments.
Full article
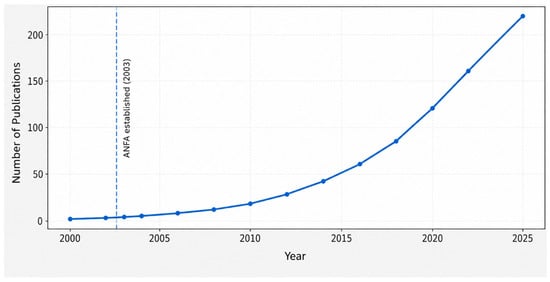
Figure 1















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}