Abstract
This case report describes the esthetic and functional rehabilitation of a 45-year-old male patient presenting with a missing maxillary right lateral incisor (#12). Due to persistent insufficiency of alveolar ridge width following multiple augmentation procedures, implant placement was contraindicated. A minimally invasive prosthetic approach was therefore selected, consisting of a single-retainer lithium disilicate resin-bonded fixed dental prosthesis (RBFDP) combined with laminate veneers to optimize anterior esthetics. The cantilever design and adhesive protocol were selected based on biomechanical principles aimed at minimizing interfacial stresses and preserving enamel structure. The prosthesis was fabricated using a fully digital workflow, and adhesive bonding was performed following established ceramic and enamel surface conditioning protocols. The restoration fulfilled the patient’s esthetic and functional expectations, and clinical follow-up at 18 months demonstrated stable bonding, healthy peri-abutment tissues, and absence of technical or biological complications. This case highlights the role of lithium disilicate cantilever RBFDPs as a minimally invasive and clinically viable treatment option for the replacement of maxillary lateral incisors when implant therapy is contraindicated, with outcomes limited to short- to medium-term observation.
1. Introduction
Replacement of missing maxillary lateral incisors represents a common esthetic and functional challenge in dentistry. Loss or congenital absence of a maxillary lateral incisor in the esthetic zone presents a complex clinical scenario requiring careful consideration of biological, functional, and patient-related factors. Beyond functional impairment, anterior tooth loss may negatively affect oral health-related quality of life, phonetics, and patient self-perception, underscoring the importance of treatment strategies that achieve optimal esthetic outcomes while preserving biological integrity. Several treatment options have been described, including removable partial dentures, conventional fixed dental prostheses (FDPs), implant-supported restorations, and resin-bonded fixed dental prostheses (RBFDPs) [1,2].
Each treatment modality presents distinct benefits and limitations. Removable partial dentures offer a non-invasive and cost-effective solution; however, their use in the anterior region is frequently associated with compromised esthetics, reduced comfort, and limited long-term acceptance [3]. Conventional fixed dental prostheses provide reliable function and esthetics but require extensive preparation of adjacent teeth, which may compromise sound tooth structure and increase the risk of pulpal complications [4]. Implant-supported restorations are widely regarded as a predictable option for single-tooth replacement; nevertheless, their indication may be limited by insufficient alveolar bone volume, the need for surgical intervention, prolonged treatment time, and increased biological and financial costs [5].
In contrast, resin-bonded fixed dental prostheses (RBFDPs) represent a minimally invasive alternative that preserves enamel, reduces biological risk, and maintains future treatment options. Early RBFDP designs, particularly fixed-fixed configurations, were associated with higher debonding rates, highlighting the importance of appropriate prosthesis design and adhesive protocols for long-term success [6].
Among these options, RBFDPs have gained acceptance as conservative and esthetically reliable alternatives, particularly in the anterior region where preservation of sound tooth structure is desirable [7]. Resin-bonded fixed dental prostheses were originally introduced as minimally invasive restorations relying on adhesive bonding to enamel rather than extensive tooth preparation, offering a biologically favorable alternative to conventional FDPs [8,9].
Although early resin-bonded designs were initially regarded as provisional or medium-term restorations, their primary limitation was debonding rather than catastrophic structural failure. Subsequent improvements in adhesive protocols, surface conditioning, and prosthetic design demonstrated that RBFDPs could function as definitive restorations with favorable long-term outcomes when appropriately indicated [10]. The transition toward all-ceramic RBFDPs addressed the esthetic limitations of metal frameworks and shifted clinical focus toward design- and adhesion-related factors rather than material failure alone [11].
Prosthesis design has been shown to play a critical role in the longevity of RBFDPs. Fixed-fixed designs are more susceptible to debonding due to differential abutment mobility, whereas single-retainer cantilever designs reduce interfacial stress by eliminating constraints between abutments [11,12,13].
Systematic reviews and long-term clinical studies have demonstrated that, when appropriately indicated, RBFDPs can achieve favorable clinical outcomes, with debonding consistently reported as the most common technical complication and biological or structural failures occurring less frequently [12,14]. More recent studies emphasize the clinical reliability of lithium disilicate RBFDPs, highlighting their ability to combine favorable esthetics with durable adhesive bonding when appropriate material selection and bonding protocols are applied [15,16]. In addition, clinical case reports support the use of RBFDPs for the management of missing maxillary lateral incisors when implant therapy is not feasible, reporting high levels of patient satisfaction and stable short- to medium-term outcomes [17].
Lithium disilicate glass ceramics, such as IPS e.max Press (Ivoclar Vivadent, Schaan, Liechtenstein), are well suited for anterior resin-bonded fixed dental prostheses because they combine favorable optical properties with adequate flexural strength and reliable adhesive bonding to enamel [13]. These characteristics allow the fabrication of minimally invasive prosthetic designs that integrate harmoniously within the anterior dentition while preserving enamel, which is essential for predictable long-term adhesion. When used in combination with enamel-confined laminate veneers, lithium disilicate restorations facilitate comprehensive esthetic integration while maintaining maximal preservation of sound tooth structure [11,18].
From a material science perspective, lithium disilicate glass ceramics are silica-based materials consisting of a glassy matrix reinforced by a high volume fraction of lithium disilicate (Li2Si2O5) crystals, typically accounting for approximately 65–70% of the material [19]. The elongated, interlocking crystal morphology within the glass phase enhances flexural strength, improves resistance to crack propagation, and supports favorable translucency and optical performance [20]. This combination of mechanical durability and esthetic properties underpins the widespread clinical use of lithium disilicate in minimally invasive anterior restorations that depend on durable adhesive bonding protocols [21].
Although lithium disilicate cantilever RBFDPs are well documented in the literature, detailed clinical reports integrating digital planning, enamel-preserving preparation strategies, and explicit prosthesis design rationale remain limited. The present case focuses on the systematic application of established adhesive prosthodontic principles within a digital workflow to enhance treatment predictability and biological preservation.
Therefore, contemporary literature supports single-retainer, all-ceramic RBFDPs as a predictable, conservative, and esthetically pleasing solution for the replacement of missing maxillary lateral incisors. This clinical report presents a minimally invasive rehabilitation using a lithium disilicate cantilever resin-bonded fixed dental prosthesis combined with laminate veneers and discusses the clinical outcome in light of current evidence.
2. Case Report
2.1. Patient Information
A 45-year-old male presented to the Prosthodontics Clinic at King Abdulaziz Medical City, Ministry of National Guard, Jeddah, Saudi Arabia, with a missing maxillary right lateral incisor (#12) and requested esthetic rehabilitation (Figure 1A,B). His chief complaint was: “I want my smile improved and the missing tooth replaced with a natural-looking option.” The patient reported no relevant medical conditions, and both medical and family histories were noncontributory.
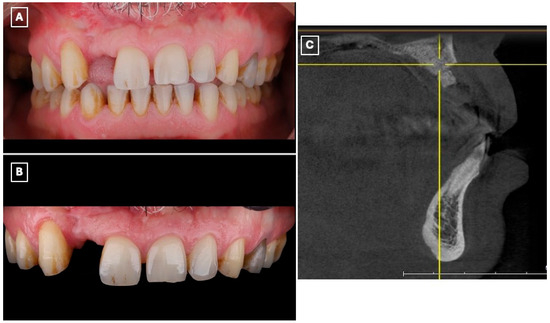
Figure 1.
Preoperative clinical and radiographic assessment of the maxillary anterior region supporting treatment selection. (A) Frontal intraoral view demonstrating the missing maxillary right lateral incisor (#12), associated asymmetry of the anterior smile line, and localized esthetic disharmony within the maxillary anterior segment. (B) Closer intraoral view highlighting the edentulous space, favorable gingival architecture, and intact adjacent enamel surfaces, which are prerequisites for predictable enamel-bonded adhesive restorations. (C) Sagittal cone-beam computed tomography (CBCT) cross-sectional image of the lateral incisor region demonstrating limited residual alveolar ridge width and altered ridge contour following previous augmentation procedures. These findings, in conjunction with prior surgical outcomes and patient preference to avoid further intervention, supported the exclusion of implant therapy and the selection of a minimally invasive, non-surgical adhesive prosthodontic approach.
2.2. Clinical Findings
All adjacent teeth were sound, with no evidence of caries, periodontal inflammation, or occlusal discrepancies. The gingival architecture in the anterior maxilla was favorable, and sufficient enamel was present on the abutment tooth to allow predictable adhesive bonding. Radiographic examination revealed no periapical or periodontal pathology.
2.3. Diagnostic Assessment and Treatment Planning
The patient had previously undergone multiple bone augmentation procedures in the periodontics department; however, despite these interventions, the residual alveolar ridge volume in the maxillary right lateral incisor region remained insufficient for predictable implant placement. This assessment was based on prior surgical outcomes, clinical ridge morphology, and interdisciplinary evaluation. Preoperative cone-beam computed tomography (CBCT) imaging (Figure 1C) demonstrated limited bucco-lingual ridge width and an unfavorable ridge contour at the lateral incisor site, further supporting the decision to exclude implant therapy.
Based on the clinical and radiographic findings and patient preferences, a single-retainer lithium disilicate resin-bonded fixed dental prosthesis (RBFDP) was chosen to preserve sound tooth structure, minimize biological risk, and maintain future treatment options. To enhance anterior esthetics and ensure harmonious integration of the prosthesis within the smile, laminate veneers were incorporated into the comprehensive treatment plan.
In addition to the replacement of the missing lateral incisor, the patient presented with pre-existing esthetic concerns affecting the maxillary anterior teeth, including discrepancies in tooth form, proportions, and color relative to the planned prosthetic restoration. The laminate veneers were therefore indicated to achieve esthetic continuity between the resin-bonded prosthesis and the adjacent dentition. Importantly, all veneers were planned as enamel-confined restorations and were not required for functional rehabilitation, but rather to optimize smile symmetry and visual integration while maintaining a minimally invasive treatment philosophy.
2.4. Clinical Procedure
Diagnostic records were obtained, including preliminary impressions, and diagnostic casts were fabricated. The casts were digitized using an intraoral scanner (Medit i700, Medit Corp., Seoul, Republic of Korea) to enable a fully digital workflow (Figure 2A). A digital wax-up was subsequently designed based on esthetic, functional, and occlusal parameters (Figure 2B), allowing three-dimensional evaluation of tooth proportions, pontic position, and incisal edge relationships relevant to a minimally invasive adhesive prosthetic approach. The approved digital wax-up was then fabricated using a three-dimensional printer (NextDent 5100, NextDent B.V., Soesterberg, The Netherlands) to produce a physical diagnostic model for clinical reference and transfer of the digital plan to the operative phase (Figure 2C).
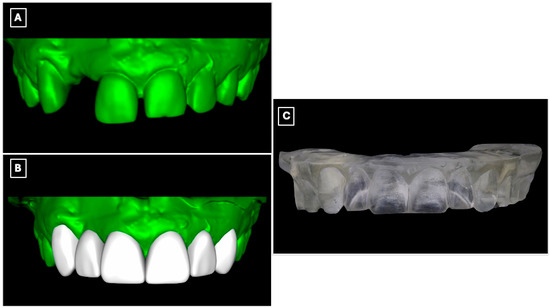
Figure 2.
Digital workflow used for diagnostic evaluation and prosthetic planning of the maxillary anterior region. (A) Digitized diagnostic cast obtained from preliminary impressions, allowing three-dimensional assessment of tooth position, edentulous space morphology, and enamel contours relevant to adhesive prosthesis design. (B) Virtual model following digital processing and wax-up, illustrating the planned tooth proportions, pontic position, and incisal edge relationships used to guide minimally invasive tooth preparation and prosthesis design. (C) Three-dimensionally printed diagnostic cast derived from the digital wax-up, used as a physical reference for mock-up fabrication and to facilitate accurate transfer of the digital plan to the clinical setting.
A silicone putty index (Express™ STD Putty, 3M ESPE, St. Paul, MN, USA) was fabricated from the printed diagnostic wax-up, and an intraoral mock-up was performed using a bis-acryl provisional material (Protemp™ 4, 3M ESPE, St. Paul, MN, USA) (Figure 3A). The mock-up enabled clinical evaluation of tooth proportions, incisal edge position, and smile integration, and served as a communication tool to confirm esthetic acceptance with the patient before performing any irreversible procedures.

Figure 3.
Digital wax-up used for esthetic analysis and prosthetic planning of the anterior rehabilitation. (A) Virtual representation of the maxillary anterior region before wax-up, serving as a baseline for evaluating tooth position, incisal edge discrepancies, and space availability for the planned resin-bonded fixed dental prosthesis. (B) Digital wax-up design illustrating the proposed single-retainer cantilever resin-bonded fixed dental prosthesis and laminate veneers, with idealized tooth proportions, incisal edge position, and symmetry used to guide enamel-confined tooth preparation, pontic emergence profile, and overall esthetic integration within the smile.
Tooth preparation was performed under mock-up guidance to ensure minimal enamel reduction and to create optimal enamel-bonding surfaces (Figure 3B). Final impressions were obtained using a polyvinyl siloxane impression material (Imprint™ 4 PVS, 3M ESPE, St. Paul, MN, USA) and submitted to the dental laboratory for definitive fabrication.
Beyond its role in visualization, the digital wax-up and intraoral mock-up contributed directly to clinical decision-making and execution. The digitally planned wax-up enabled precise control of tooth proportions, incisal edge position, and pontic emergence profile, facilitating enamel-confined preparation and preservation of sound tooth structure. The intraoral mock-up functioned as a reduction guide during tooth preparation, minimizing unnecessary enamel removal and reducing chairside adjustments at the time of prosthesis seating. This digital-to-clinical transfer enhanced treatment predictability by allowing preoperative verification of esthetics and function, thereby improving clinical efficiency and patient acceptance.
The definitive restoration was fabricated as a full-contour lithium disilicate prosthesis using a low-translucency ingot (IPS e.max Press, Ivoclar Vivadent, Schaan, Liechtenstein). The prosthesis incorporated a single-retainer cantilever design with a modified ridge-lap pontic to optimize esthetics, biomechanics, and hygiene (Figure 4A,B). The single-retainer configuration was deliberately selected to eliminate differential abutment mobility and reduce interfacial shear stresses commonly associated with fixed-fixed designs. The palatal retainer was confined entirely to enamel and designed with smooth, well-defined margins to maximize adhesive bonding while preserving sound tooth structure (Figure 4B). Connector dimensions were carefully controlled to provide adequate fracture resistance without over-contouring, balancing mechanical strength with esthetic requirements. A modified ridge-lap pontic design was employed to achieve a natural emergence profile while maintaining a cleansable contour, allowing passive tissue contact and facilitating effective oral hygiene (Figure 4A,B).
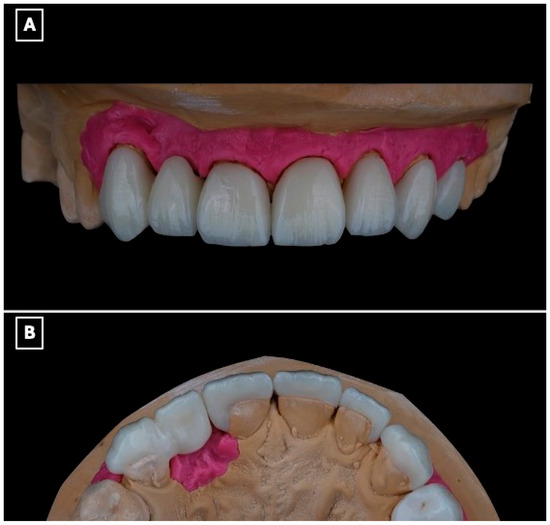
Figure 4.
Definitive lithium disilicate single-retainer cantilever resin-bonded fixed dental prosthesis illustrating key design features. (A) Labial view showing the esthetic integration of the restoration within the anterior smile zone and the single-retainer cantilever configuration, selected to eliminate differential abutment mobility and reduce interfacial shear stresses at the adhesive interface. (B) Palatal view illustrating the enamel-bonded palatal retainer with a defined connector region and a modified ridge-lap pontic design, providing controlled tissue contact for esthetics while facilitating oral hygiene access and minimizing plaque accumulation at the pontic-tissue interface.
Before adhesive cementation, the intaglio surface of the lithium disilicate restoration was treated to enhance micromechanical and chemical retention. The bonding surface was conditioned with 5% hydrofluoric acid (IPS Ceramic Etching Gel, Ivoclar Vivadent, Schaan, Liechtenstein) for 20 s, followed by thorough rinsing and air drying. Subsequently, a silane coupling agent (Monobond Plus, Ivoclar Vivadent, Schaan, Liechtenstein) was applied to facilitate chemical interaction between the ceramic substrate and the resin cement (Figure 5A,B).
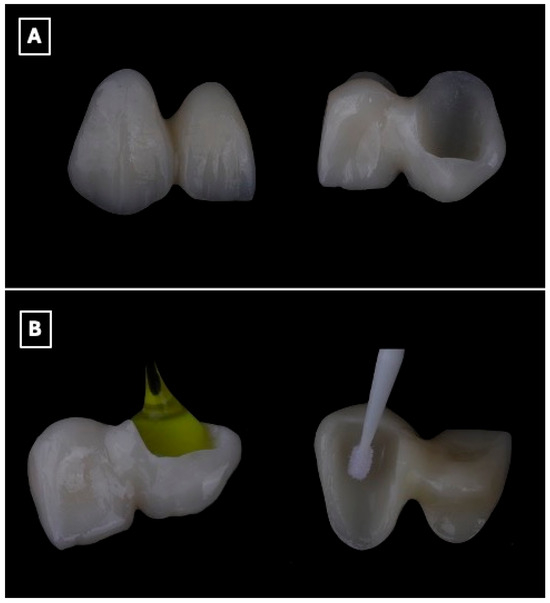
Figure 5.
Surface conditioning protocol of the lithium disilicate single-retainer cantilever resin-bonded fixed dental prosthesis prior to adhesive cementation. (A) Intaglio surface of the prosthesis before surface treatment, illustrating the defined bonding surface of the enamel-retained cantilever retainer and pontic, which is critical for maximizing adhesive surface area and stress distribution. (B) Sequential surface conditioning procedures, including hydrofluoric acid etching to selectively dissolve the glassy matrix and create micromechanical surface roughness, followed by application of a silane coupling agent to promote chemical bonding between the lithium disilicate ceramic and the resin cement, thereby enhancing bond durability and long-term retention in cantilever resin-bonded designs.
The enamel surface of the abutment tooth was selectively conditioned using 37% phosphoric acid gel (Total Etch, Ivoclar Vivadent, Schaan, Liechtenstein), followed by rinsing and controlled air-drying to maintain an enamel-restricted bonding substrate. A universal adhesive system (Adhese Universal, Ivoclar Vivadent, Schaan, Liechtenstein) was then applied according to the manufacturer’s recommendations. Cementation of the resin-bonded fixed dental prosthesis was performed using a light-cured resin cement (Variolink Esthetic LC, Ivoclar Vivadent, Schaan, Liechtenstein), with polymerization from multiple orientations to ensure adequate curing at the enamel-ceramic interface (Figure 6A–C). Excess cement was removed during the elastic phase, and occlusal refinement was subsequently carried out to eliminate static, functional, and excursive contacts on the pontic and retainer, thereby limiting mechanical loading on the cantilever restoration (Figure 6C).
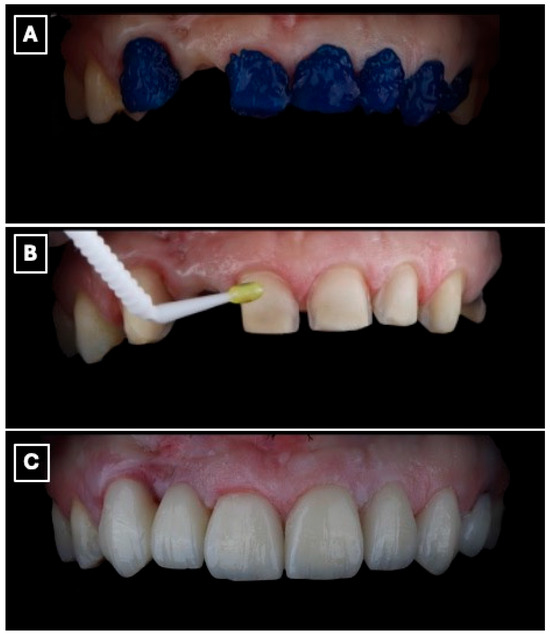
Figure 6.
Adhesive cementation of the lithium disilicate single-retainer cantilever resin-bonded fixed dental prosthesis using a light-cured resin cement. (A) Intraoral try-in and seating of the prosthesis prior to polymerization, confirming complete seating of the cantilever retainer, passive adaptation at the adhesive interface, and absence of premature contacts that could induce tensile or shear stresses. (B) Removal of excess resin cement during the gel phase following initial light activation, a critical step to prevent marginal overhangs, reduce plaque retention, and minimize the risk of gingival inflammation or marginal discoloration at the enamel-ceramic interface. (C) Final intraoral view after complete polymerization, demonstrating stable marginal adaptation, controlled occlusal scheme with elimination of functional contacts on the pontic, and harmonious esthetic integration of the restoration within the anterior smile zone, which are essential factors for long-term clinical success of cantilever resin-bonded prostheses.
The final restoration demonstrated harmonious integration with the adjacent dentition, with appropriate tooth proportions, shade matching, and alignment within the anterior smile zone (Figure 7).

Figure 7.
Postoperative intraoral view demonstrating the final lithium disilicate resin-bonded fixed dental prosthesis and laminate veneers. The image illustrates harmonious integration of the cantilever RBFDP within the anterior dentition, with appropriate tooth proportions, shade matching, and surface texture continuity relative to the adjacent natural teeth and veneers. The restoration exhibits favorable soft-tissue adaptation, stable gingival margins, and a natural emergence profile of the pontic, supporting both esthetic outcomes and periodontal health. Occlusal harmony in the anterior region is maintained, with no visible functional loading on the pontic, consistent with biomechanical principles for long-term success of single-retainer cantilever resin-bonded prostheses.
2.5. Follow-Up
The patient reported satisfaction with the esthetic and functional outcomes of the treatment. Follow-up evaluations at 1 week, 1 month, 6 months, 1 year, and 18 months showed maintained adhesive retention, healthy peri-abutment soft tissues, and no evidence of technical or biological complications during the observation period (Figure 8A–C).
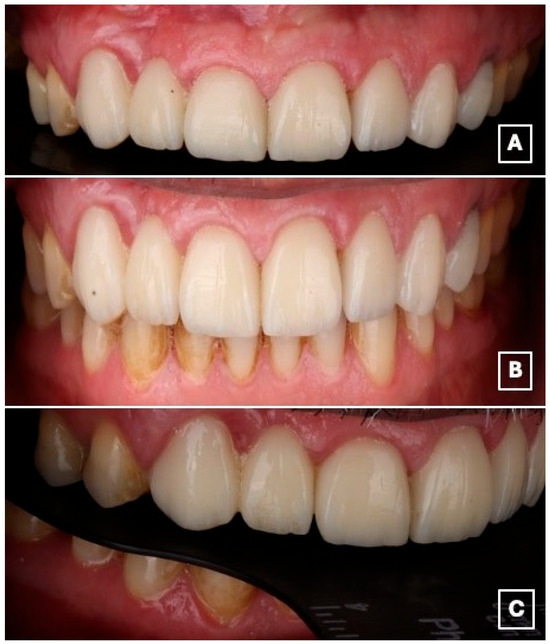
Figure 8.
Intraoral views at the 18-month follow-up demonstrate clinical stability of the restoration. (A) Frontal intraoral view showing stable esthetic integration of the cantilever RBFDP and laminate veneers within the smile. (B) Close-up frontal view highlighting maintained color stability, intact adhesive margins, and healthy peri-gingival tissues, suggesting favorable short- to medium-term adhesive performance. (C) Lateral intraoral view illustrating functional integration and preservation of occlusal relationships, with no evidence of chipping, debonding, or excessive wear at the cantilever region.
3. Discussion
This case illustrates the management of a missing maxillary lateral incisor using a lithium disilicate single-retainer cantilever resin-bonded fixed dental prosthesis (RBFDP) in combination with laminate veneers, resulting in acceptable short- to medium-term esthetic and functional outcomes.
The concept of enamel-bonded fixed prostheses emerged in the 1970s following the introduction of acid-etch techniques, culminating in the development of the so-called “Maryland Bridge,” which utilized a metal framework bonded to etched enamel [8]. Although early designs were limited by frequent debonding and compromised esthetics, advances in adhesive protocols and restorative materials have significantly improved their clinical performance [1]. The subsequent transition toward metal-free, all-ceramic RBFDPs addressed esthetic limitations associated with metallic retainers and enabled improved translucency, color integration, and enamel-compatible bonding, making them particularly suitable for the anterior esthetic zone [11].
Rather than proposing a novel material or technique, this report aims to provide a clinically instructive example of how established adhesive prosthodontic principles can be systematically applied using a digital workflow to enhance treatment planning accuracy, enamel preservation, and patient-centered decision-making.
Contemporary management of congenitally or developmentally missing maxillary lateral incisors emphasizes individualized treatment planning based on esthetic demands, occlusal considerations, periodontal status, and patient preferences. Recent evidence supports minimally invasive prosthetic strategies that prioritize biological preservation while delivering predictable esthetic outcomes, particularly when implant therapy is contraindicated or declined [13].
In the present case, a single-retainer cantilever design was selected in accordance with current evidence demonstrating superior outcomes compared with fixed-fixed designs. Fixed-fixed RBFDPs are more prone to debonding due to differential abutment mobility, which generates unfavorable stresses at the adhesive interface [14]. In contrast, cantilever RBFDPs allow the pontic to move synchronously with a single abutment, thereby reducing shear stresses and improving long-term stability. This biomechanical rationale has been extensively discussed by Drossart et al., who demonstrated that all-ceramic cantilever resin-bonded fixed dental prostheses represent a reliable and biologically conservative alternative for replacing missing anterior teeth, particularly in situations where implant therapy is limited by growth, bone volume, or esthetic constraints [22]. Their work further highlights that the cantilever configuration allows the periodontal ligament of the abutment tooth to act as a stress absorber, improving stress distribution at the adhesive interface and minimizing interfacial stress concentration commonly associated with two-retainer configurations [22].
From a biomechanical perspective, the cantilever configuration reduces interfacial stress concentration and minimizes partial debonding patterns commonly observed in two-retainer designs. When placed in the anterior maxilla, cantilever designs have demonstrated particularly favorable longevity, as occlusal forces are more predictable and functional loading is generally lower [18,23]. Recent in vitro evidence has demonstrated that connector geometry plays a critical role in the fracture resistance of cantilever resin-bonded fixed dental prostheses, with adequately dimensioned connectors significantly increasing load-to-fracture values regardless of the ceramic material used, further emphasizing the importance of prosthetic design in achieving predictable clinical outcomes [24,25].
Recent clinical guidelines and narrative reviews on congenitally missing lateral incisors further support the use of single-retainer resin-bonded prostheses, emphasizing their reversibility, enamel preservation, and compatibility with future treatment options, particularly in adult patients with completed craniofacial growth [26].
The preference for single-retainer designs is further supported by prospective clinical evidence demonstrating superior long-term survival compared with two-retainer resin-bonded prostheses. Landmark clinical investigations have attributed failures in two-retainer designs primarily to differential abutment mobility and asymmetric stress transfer, reinforcing the biomechanical advantage of cantilever designs in the anterior esthetic zone [14].
Available evidence from systematic reviews suggests that resin-bonded fixed dental prostheses can achieve clinically acceptable performance over time. In a comprehensive analysis published in 2017, event-free survival was reported to decline from 83.6% at 5 years to 64.9% at 10 years, with retention loss identified as the most common technical issue [14]. Comparable findings were reported by Alraheam et al., who estimated a 5-year success rate of approximately 88% and similarly observed that technical complications, primarily debonding, occurred more frequently than biological failures [27].
Long-term observational data focusing specifically on all-ceramic cantilever RBFDPs further suggest that this design may demonstrate favorable biomechanical behavior, with survival rates of 95.4% at 10 and 15 years and a decrease to 81.8% after 18 years, despite occasional ceramic fractures [28]. In the present case, the absence of complications at 18 months is consistent with these reports, although direct comparison is limited by the shorter observation period.
Although implant-supported restorations are often considered the gold standard for single-tooth replacement, they may be contraindicated in patients with inadequate alveolar ridge dimensions or in those unwilling to undergo additional surgical procedures. The reviewed literature stresses that in such scenarios, resin-bonded prosthetic solutions provide predictable esthetic outcomes with reduced morbidity, treatment time, and cost compared with surgical alternatives [15]. RBFDPs preserve adjacent teeth and maintain future treatment options, whereas conventional fixed dental prostheses require substantial tooth reduction and may compromise pulpal vitality, particularly in the anterior esthetic zone [1,11,18,29]. Implant suitability in clinical practice is influenced not only by ridge width measurements but also by prior surgical outcomes, patient tolerance for further interventions, and overall risk-benefit assessment, all of which contributed to treatment selection in the present case.
The bonding protocol employed hydrofluoric acid etching, silanization of the ceramic surface, phosphoric acid etching of enamel, application of a universal adhesive, and resin cementation, procedures that align with contemporary adhesive dentistry recommendations [30]. Durable adhesion at the ceramic-enamel interface remains a critical determinant of success, particularly in cantilever all-ceramic RBFDPs where retention relies exclusively on adhesive bonding [15].
Experimental and in vitro studies have demonstrated that lithium disilicate cantilever RBFDPs can withstand physiological masticatory forces in the anterior region, even when fabricated with reduced material thickness [15]. The interlocking lithium disilicate crystal microstructure contributes to high flexural strength and resistance to crack propagation, which is particularly relevant in cantilever configurations where stress concentration occurs at the connector region [31]. Finite element and fracture resistance studies further emphasize the influence of connector geometry and material thickness on stress distribution and load-bearing capacity [32,33]. Recent finite element analysis comparing lithium disilicate with zirconia and 3D-printed composite materials for anterior bridge restorations demonstrated that lithium disilicate exhibits a balanced stress distribution under simulated occlusal loading, supporting its suitability for anterior applications where both biomechanical reliability and esthetic performance are required [34].
Case reports and clinical studies consistently highlight the positive esthetic and psychological impact of adhesive prostheses in patients with missing maxillary lateral incisors, particularly when implant therapy is not feasible [17,29]. Patients frequently report high satisfaction related to smile esthetics, phonetics, and self-confidence following minimally invasive rehabilitation strategies [35].
Despite their documented clinical success, single-retainer cantilever RBFDPs are not universally indicated and require careful patient selection. Potential limitations include parafunctional habits, unfavorable occlusal schemes with excessive lateral or protrusive loading, and limited enamel availability on the abutment tooth, all of which may compromise adhesive retention and long-term stability [36]. Beyond debonding, reported complications include ceramic fracture, marginal discoloration, secondary caries, and localized periodontal inflammation related to pontic design [24,37,38]. Occlusal wear of the ceramic surface or opposing dentition has also been reported, though less frequently in anterior applications [39,40]. Careful case selection, appropriate prosthetic design, meticulous adhesive procedures, and regular follow-up are therefore essential.
The combined use of a single-retainer cantilever resin-bonded fixed dental prosthesis and laminate veneers should be interpreted within the framework of minimally invasive dentistry. In the present case, the veneers were not required for functional correction but were incorporated to address pre-existing discrepancies in tooth morphology and shade, thereby enhancing esthetic continuity within the anterior dentition. All veneer preparations were strictly limited to enamel, preserving the biological advantages of adhesive techniques and avoiding unnecessary removal of sound tooth structure. Nevertheless, laminate veneers represent an elective adjunct and should be prescribed selectively based on individual esthetic requirements, available enamel substrate, and informed patient consent.
A further limitation of this clinical report is the duration of follow-up. Although the restoration demonstrated stable esthetic integration and satisfactory function over an 18-month observation period, this timeframe reflects only short- to medium-term performance. As a single-case presentation, the findings should not be interpreted as indicative of long-term clinical reliability, and extended follow-up, as well as larger clinical studies, are required to substantiate long-term outcomes.
4. Conclusions
When implant therapy is contraindicated, resin-bonded prostheses represent a minimally invasive and esthetically reliable alternative for replacing maxillary lateral incisors. In the present case, a lithium disilicate single-retainer cantilever resin-bonded fixed dental prosthesis combined with laminate veneers resulted in satisfactory esthetic and functional outcomes over an 18-month follow-up period. Within the limitations of a single case report and short- to medium-term observation, this approach appears clinically viable; however, longer-term follow-up and larger clinical studies are required to confirm long-term predictability and durability.
Author Contributions
Conceptualization, L.A., H.A. and M.M.T.; methodology, L.A., M.M.T. and O.R.; software, M.M.T. and F.A.; validation, L.A., O.R. and H.A.; formal analysis, M.M.T. and L.A.; investigation, M.M.T., O.R. and F.A.; resources, H.A. and F.A.; data curation, M.M.T.; writing—original draft preparation, M.M.T. and L.A.; writing—review and editing, L.A., H.A., O.R. and F.A.; visualization, M.M.T.; supervision, L.A.; project administration, L.A.; funding acquisition, L.A. All authors have read and agreed to the published version of the manuscript.
Funding
The project was funded by KAU Endowment (WAQF) at king Abdulaziz University, Jeddah, Saudi Arabia. The authors, therefore, acknowledge with thanks WAQF and the Deanship of Scientific Research (DSR) for technical and financial support.
Institutional Review Board Statement
Ethical review and approval were waived for this study, as it represents a single clinical case report and does not involve experimental procedures.
Informed Consent Statement
Written informed consent was obtained from the patient for the publication of clinical data and accompanying images.
Data Availability Statement
Data sharing does not apply to this article, as no datasets were generated or analyzed during the current study.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Sabri, R. Management of missing maxillary lateral incisors. J. Am. Dent. Assoc. 1999, 130, 80–84. [Google Scholar] [CrossRef] [PubMed]
- Allen, P.F.; Anweigi, L.; Ziada, H. A prospective study of the performance of resin bonded bridgework in patients with hypodontia. J. Dent. 2016, 50, 69–73. [Google Scholar] [CrossRef]
- Peršić Kiršić, S.; Čelebić, A.; Filipović-Zore, I.; Strajnić, L.; Petričević, N. Assessing Esthetic and Functional Benefits of Three Types of Maxillary Partial Denture Designs over Five Years. Dent. J. 2025, 13, 610. [Google Scholar] [CrossRef]
- Kern, M.; Türp, L.; Yazigi, C. Long-term outcome of anterior cantilever zirconia ceramic resin-bonded fixed dental prostheses: Influence of the pontic location. J. Prosthet. Dent. 2025, 133, 1017–1023. [Google Scholar] [CrossRef]
- Jurado, C.A.; Garcia-Torres, F.; Rojas-Rueda, S.; Karimi, K.; Antal, M.A. Evaluating the Success of Immediate Implants in the Esthetic Zone: A Narrative Review with Case Illustration. Dent. J. 2025, 13, 365. [Google Scholar] [CrossRef]
- Panyasuksri, N.; Angkasith, P.; Yavirach, A.; Chaijareenont, P.; Saokaew, S.; Kanchanasurakit, S. Clinical Efficacy of Anterior Ceramic Materials in Resin-Bonded Fixed Dental Prostheses with Different Bridge Designs-A Systematic Review and Meta-Analysis. Prosthesis 2025, 7, 41. [Google Scholar] [CrossRef]
- El-Mowafy, O.; Rubo, M. Resin-Bonded Fixed Partial Dentures-A Literature Review with Presentation of a Novel Approach. Int. J. Prosthodont. 2000, 13, 460–467. [Google Scholar]
- Rochette, A.L. Attachment of a splint to enamel of lower anterior teeth. J. Prosthet. Dent. 1973, 30, 418–423. [Google Scholar] [CrossRef]
- Howe, D.F.; Denehy, G.E. Anterior fixed partial dentures utilizing the acid-etch technique and a cast metal framework. J. Prosthet. Dent. 1977, 37, 28–31. [Google Scholar] [CrossRef] [PubMed]
- Kern, M.; Sasse, M. Ten-year survival of anterior all-ceramic resin-bonded fixed dental prostheses. J. Adhes. Dent. 2011, 13, 407–410. [Google Scholar] [CrossRef] [PubMed]
- Rathee, M.; Alam, M.; Divakar, S.; Malik, S. Resin-bonded bridge as a simplified approach to restore missing teeth in esthetic zone by conventional and digital techniques. Dent. Res. J. 2022, 19, 92. [Google Scholar] [CrossRef]
- Creugers, N.H.; Käyser, A.F. An analysis of multiple failures of resin-bonded bridges. J. Dent. 1992, 20, 348–351. [Google Scholar] [CrossRef] [PubMed]
- Kern, M. Clinical long-term survival of two-retainer and single-retainer all-ceramic resin-bonded fixed dental prostheses. Quintessence Int. 2005, 36, 141–147. [Google Scholar]
- Balasubramaniam, G.R. Predictability of resin bonded bridges-A systematic review. Br. Dent. J. 2017, 222, 849–858. [Google Scholar] [CrossRef]
- Gresnigt, M.M.M.; Tirlet, G.; Bošnjak, M.; van der Made, S.; Attal, J.-P. Fracture strength of lithium disilicate cantilever resin bonded fixed dental prosthesis. J. Mech. Behav. Biomed. Mater. 2020, 103, 103615. [Google Scholar] [CrossRef] [PubMed]
- Türkaslan, S.; Mutluay, M.M.; Vallittu, P.K.; Arola, D.; Tezvergil-Mutluay, A. Fatigue resistance of metal-free cantilever bridges supported by labial laminate veneers. J. Mech. Behav. Biomed. Mater. 2020, 103, 103596. [Google Scholar] [CrossRef]
- Yew Hin, B.; Ariffin, Z. Prosthodontic Rehabilitation of Bilateral Maxillary Lateral Incisors Agenesis: A Case Report with One-Year Follow-Up. Arch. Orofac. Sci. 2021, 16, 241–251. [Google Scholar] [CrossRef]
- Mohamed, S.G.A.; Hussein, H.G.A.; Mohamed, G.A.; Ibrahim, S.R.M. Esthetic Rehabilitation of Bilaterally Missing Maxillary Lateral Incisors in a Young Adult: A Step-by-Step Clinical Case Report. J. Pharm. Bioallied Sci. 2025, 17, 93–96. [Google Scholar] [CrossRef]
- Al-Johani, H.; Haider, J.; Satterthwaite, J.; Silikas, N. Lithium Silicate-Based Glass Ceramics in Dentistry: A Narrative Review. Prosthesis 2024, 6, 478–505. [Google Scholar] [CrossRef]
- Kang, S.H.; Chang, J.; Son, H.H. Flexural strength and microstructure of two lithium disilicate glass ceramics for CAD/CAM restoration in the dental clinic. Restor. Dent. Endod. 2013, 38, 134–140. [Google Scholar] [CrossRef]
- Manziuc, M.; Kui, A.; Chisnoiu, A.; Labunet, A.; Negucioiu, M.; Ispas, A.; Buduru, S. Zirconia-Reinforced Lithium Silicate Ceramic in Digital Dentistry: A Comprehensive Literature Review of Our Current Understanding. Medicina 2023, 59, 2135. [Google Scholar] [CrossRef]
- Drossart, M.; Cheron, R.A.; Tirlet, G. All-ceramic cantilever resin-bonded fixed dental prostheses: A therapeutic option to replace a missing front tooth. J. Dentofac. Anom. Orthod. 2017, 20, 306. [Google Scholar] [CrossRef][Green Version]
- Jaoued, M.; Riahi, Z.; Hadyaoui, D.; Harzallah, B. Resin Bonded Bridges: A Comparative Case Study. Int. Dent. J. 2024, 74, S386–S387. [Google Scholar] [CrossRef]
- Ab Ghani, S.M.; Mohd Osman, M.L.; Chang, H.-C.; Ab Ghani, A.R.; Lim, T.W. Investigation of Connector Parameters for Fracture Strength of Zirconia and Lithium Disilicate Resin-Bonded Fixed Dental Prosthesis. Prosthesis 2025, 7, 115. [Google Scholar] [CrossRef]
- Khorshed, A.M.; Ghanem, L.; Shokry, T.E. Effect of connector size and configuration on the fracture resistance of a long-span implant-supported monolithic zirconia fixed partial denture (An in vitro Study). BMC Oral Health 2025, 25, 1375. [Google Scholar] [CrossRef] [PubMed]
- Marmar, L.; Shihabi, S.B.; Jamous, I. Replacement of Congenitally Missing Maxillary Lateral Incisor with Two-Buccal-Retainer Resin-Bonded Fixed Dental Prosthesis Modified by Proximal Boxes. Case Rep. Dent. 2022, 2022, 5117542. [Google Scholar] [CrossRef] [PubMed]
- Alraheam, I.A.; Ngoc, C.N.; Wiesen, C.A.; Donovan, T.E. Five-year success rate of resin-bonded fixed partial dentures: A systematic review. J. Esthet. Restor. Dent. 2019, 31, 40–50. [Google Scholar] [CrossRef]
- Kern, M. Fifteen-year survival of anterior all-ceramic cantilever resin-bonded fixed dental prostheses. J. Dent. 2017, 56, 133–135. [Google Scholar] [CrossRef]
- Sharma, M.; Nandan, R.; Sharma, R.; Kumar, S.; Gopi, A.; Agarwal, R.; Ashraf, S.; Mahata, S.; Barman, P. Prosthodontic Management of Congenitally Missing and Peg-Shaped Maxillary Lateral Incisors: A Case Report. Cureus 2025, 17, e83651. [Google Scholar] [CrossRef]
- Hilgemberg, B.; Figuerêdo de Siqueira, F.; Millan Cardenas, A.; Ribeiro, J.; Davila-Sanchez, A.; Sauro, S.; Loguercio, A.; Arrais, C. Effect of Bonding Protocols on the Performance of Luting Agents Applied to CAD–CAM Composites. Materials 2022, 15, 6004. [Google Scholar] [CrossRef]
- Zarone, F.; Di Mauro, M.I.; Ausiello, P.; Ruggiero, G.; Sorrentino, R. Current status on lithium disilicate and zirconia: A narrative review. BMC Oral Health 2019, 19, 134. [Google Scholar] [CrossRef]
- Oishi, Y.; Nozaki, K.; Nemoto, R.; Yue, Y.; Matsumura, M.; Saleh, O.; Fueki, K. Finite element analysis of stress distribution in cantilever resin-bonded zirconia fixed dental prosthesis and periodontal tissue with alveolar bone loss. J. Prosthodont. Res. 2025, 69, 351–358. [Google Scholar] [CrossRef]
- Keulemans, F.; Shinya, A.; Lassila, L.V.; Vallittu, P.K.; Kleverlaan, C.J.; Feilzer, A.J.; De Moor, R.J. Three-dimensional finite element analysis of anterior two-unit cantilever resin-bonded fixed dental prostheses. Sci. World J. 2015, 2015, 864389. [Google Scholar] [CrossRef]
- Di Francesco, P.; Bechir, A.; Popescu, A.I.; Chivu, M.V.; Dobrescu, A.M.; Comăneanu, R.M.; Târcolea, M. Finite element analysis (FEA) of the stress behavior of some dental materials. J. Med. Life 2025, 18, 29–37. [Google Scholar] [CrossRef]
- Babaei, M.; Kazemian, M.; Barekatain, M. A comparative analysis of patient satisfaction with various methods of digital smile design and simulation. Dent. Res. J. 2025, 22, 10. [Google Scholar] [CrossRef]
- Alaida, W.S.; Gadi, S.A.; Al-Ghannam, R.E.; Alamri, M.F.; Mirdad, F.I.; Argaibeh, R.M.; Alqahtani, B.A.; Alqahtani, A.M.; Al Jaban, A.A.; Alkuraydimi, T.M.; et al. Biomechanical and Occlusal Factors Influencing the Longevity of Single-Unit Restorations: A Comprehensive Review. Cureus 2025, 17, e85998. [Google Scholar] [CrossRef]
- Alqutaibi, A.; Alghauli, M.; Almuzaini, S.; Alharbi, A.; Alsani, A.; Mubarak, A.; Alhajj, M. Failure and complication rates of different materials, designs, and bonding techniques of ceramic cantilever resin-bonded fixed dental prostheses for restoring missing anterior teeth: A systematic review and meta-analysis. J. Esthet. Restor. Dent. 2024, 36, 1396–1411. [Google Scholar] [CrossRef]
- Chen, J.; Cai, H.; Ren, X.; Suo, L.; Pei, X.; Wan, Q. A Systematic Review of the Survival and Complication Rates of All-Ceramic Resin-Bonded Fixed Dental Prostheses. J. Prosthodont. 2018, 27, 535–543. [Google Scholar] [CrossRef]
- Gwon, B.; Bae, E.-B.; Lee, J.-J.; Cho, W.-T.; Bae, H.-Y.; Choi, J.-W.; Huh, J.-B. Wear Characteristics of Dental Ceramic CAD/CAM Materials Opposing Various Dental Composite Resins. Materials 2019, 12, 1839. [Google Scholar] [CrossRef]
- Branco, A.; Colaço, R.; Pina, C.; Serro, A. A State-of-the-Art Review on the Wear of the Occlusal Surfaces of Natural Teeth and Prosthetic Crowns. Materials 2020, 13, 3525. [Google Scholar] [CrossRef]








Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license.