
Relationship Between Frequency of Physical Activity, Functional Mobility, and Self-Perceived Health in People with Different Levels of Pain: A Cross-Sectional Study

 , ,
, ,  , ,
, ,  and
and 
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Data Resources
2.2.1. European Health Surveys in Spain 2014 and 2020 (EHSS)
2.2.2. The Spanish National Health Survey 2017 (SNHS)
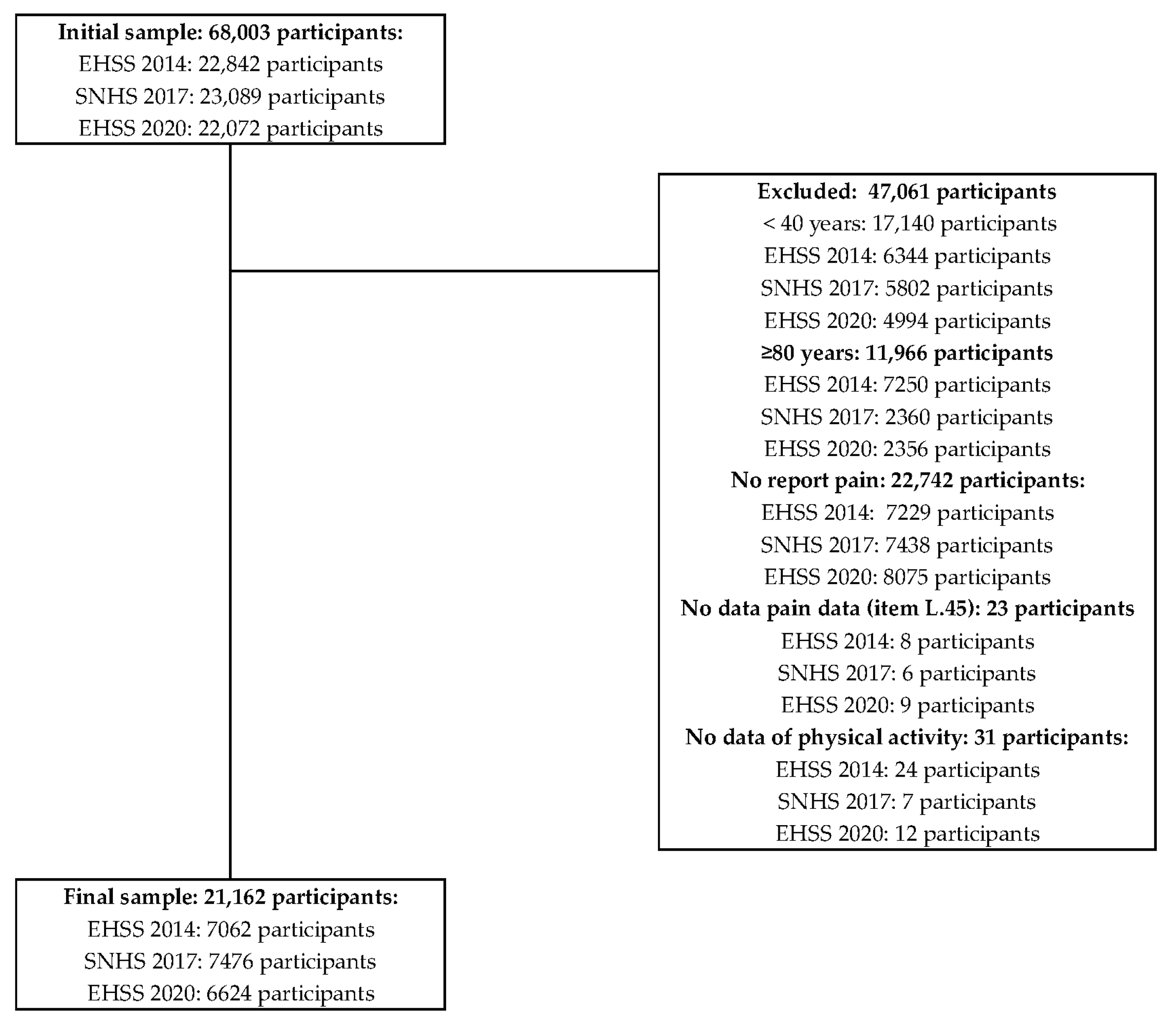
2.3. Participants
2.4. Variables
2.4.1. Outcome Variables
2.4.2. Socio-Demographic Variables
2.5. Statistical Analysis
3. Results
3.1. Descriptive Analysis of the Sample
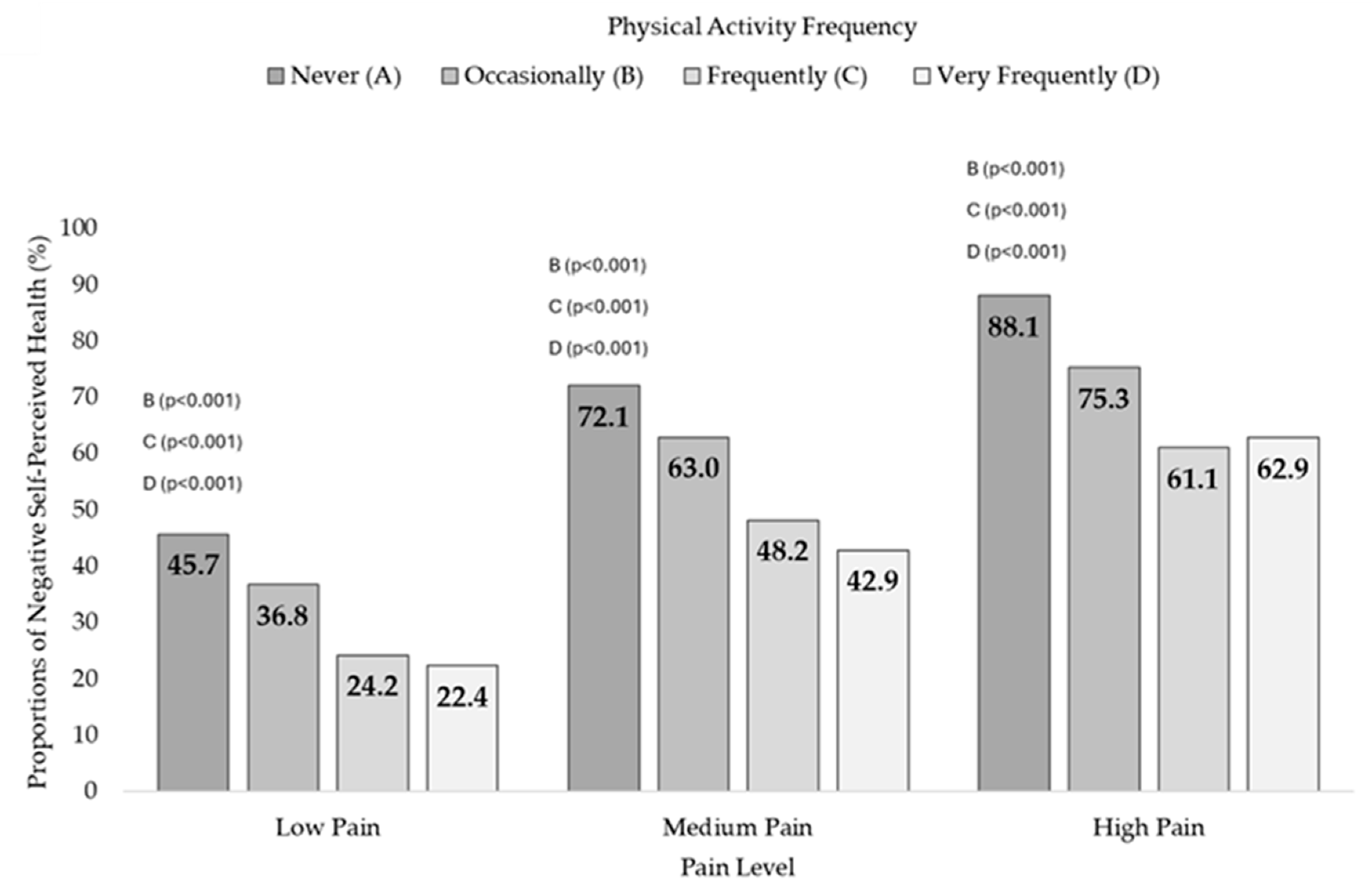
3.2. Self-Perceived Health and Physical Activity Frequency
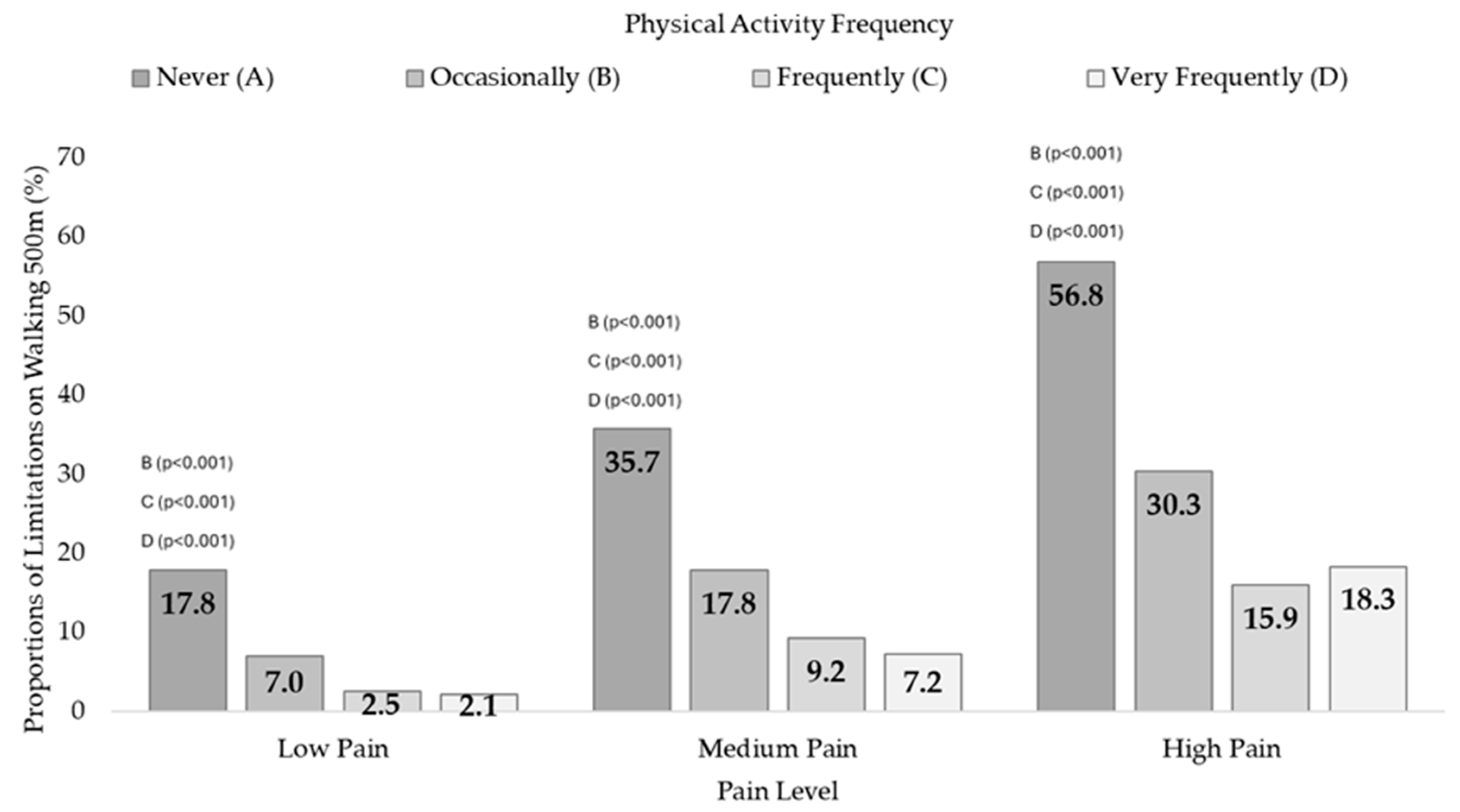
3.3. 500-Metre Walking Difficulties and Physical Activity Frequency
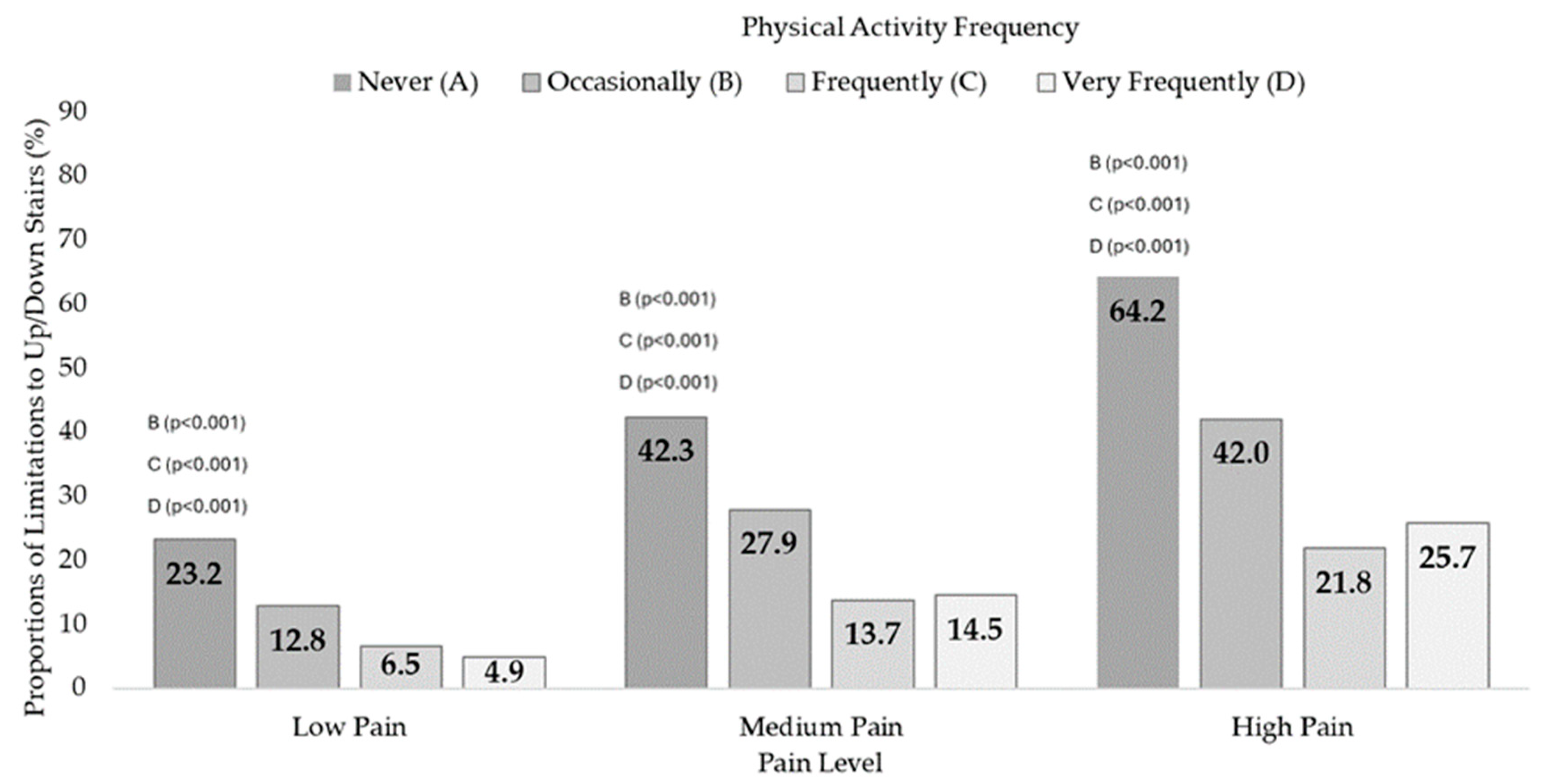
3.4. 12 Steps Difficulties and Physical Activity Frequency
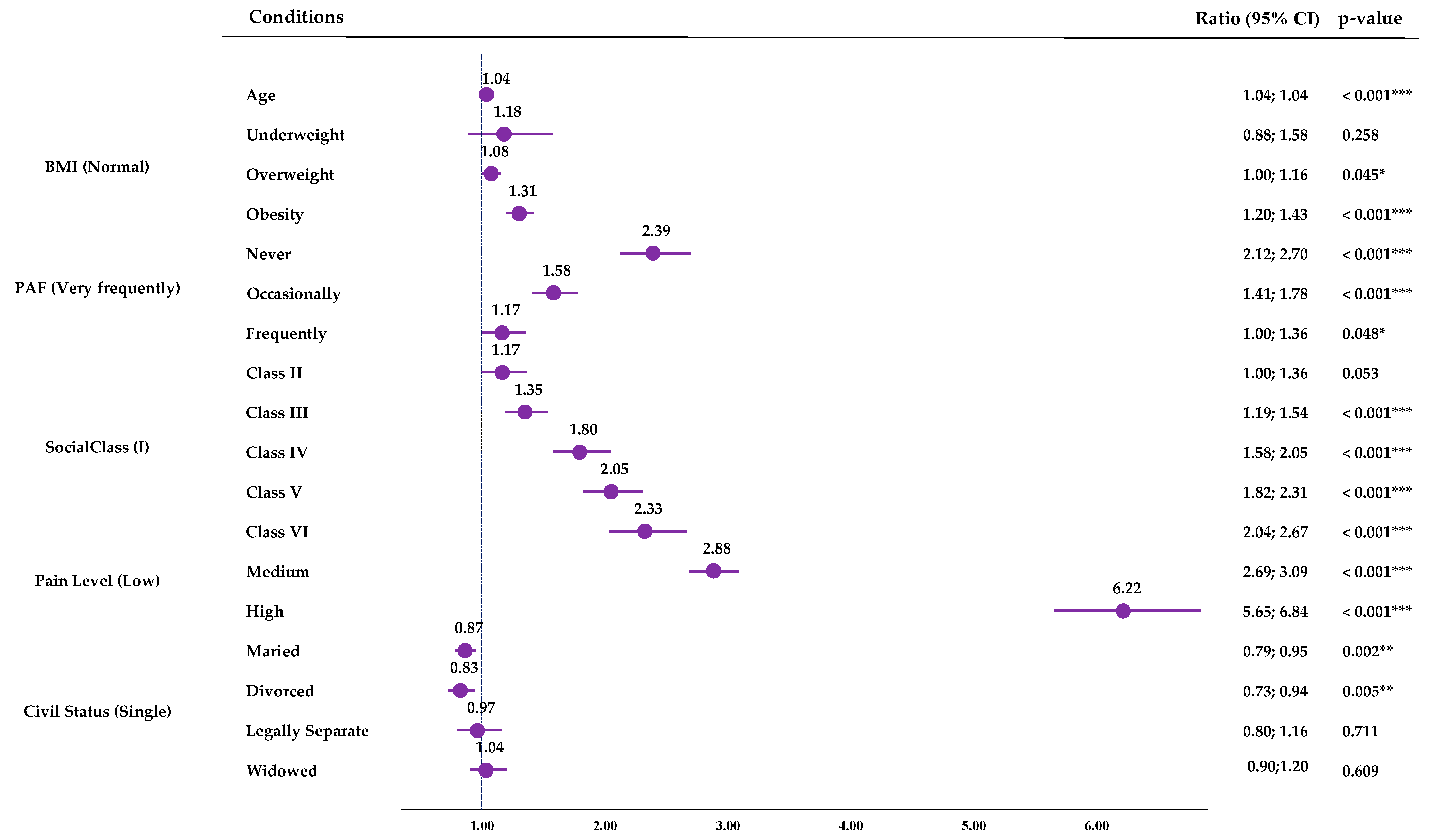
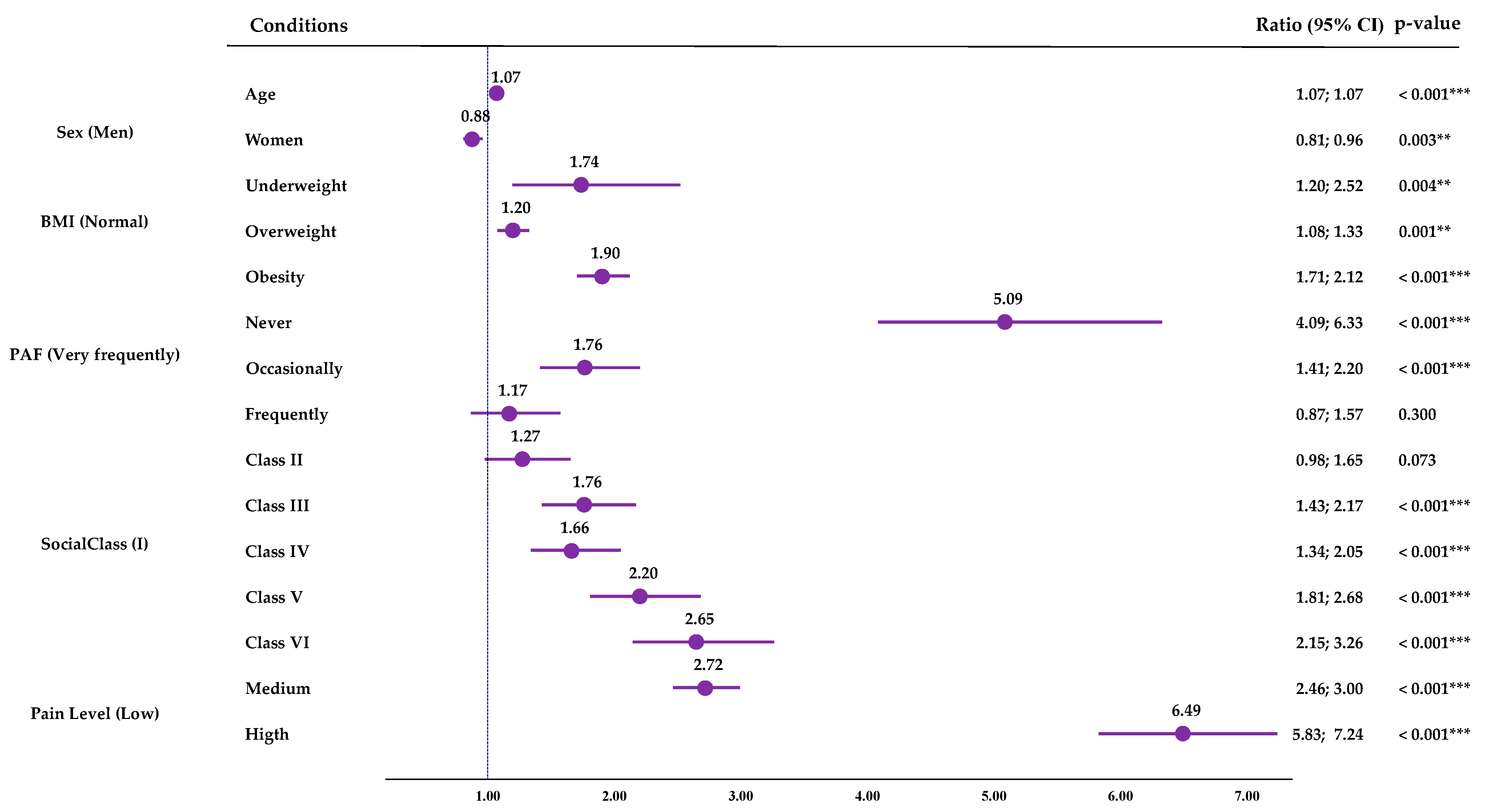
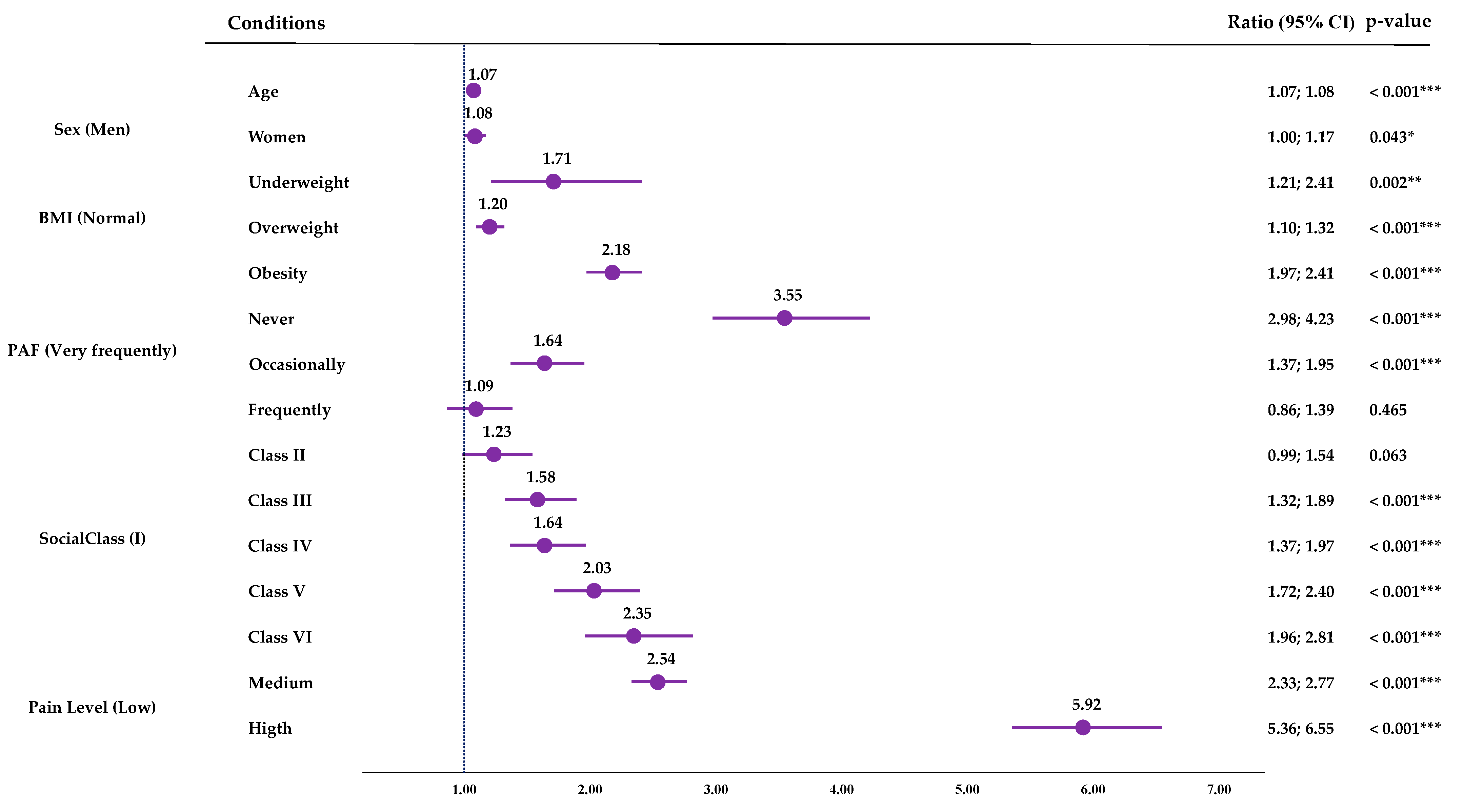
3.5. Multiple Binary Logistic Regression
4. Discussion
4.1. Main Findings
4.2. Practical Applications, and Future Lines
4.3. Strength and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Piggin, J. What Is Physical Activity? A Holistic Definition for Teachers, Researchers and Policy Makers. Front. Sports Act. Living 2020, 2, 72. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Physical Activity. Available online: https://www.who.int/news-room/fact-sheets/detail/physical-activity (accessed on 17 June 2024).
- Bull, F.C.; Al-Ansari, S.S.; Biddle, S.; Borodulin, K.; Buman, M.P.; Cardon, G.; Carty, C.; Chaput, J.-P.; Chastin, S.; Chou, R.; et al. World Health Organization 2020 guidelines on physical activity and sedentary behaviour. Br. J. Sports Med. 2020, 54, 1451–1462. [Google Scholar] [CrossRef] [PubMed]
- De la Corte-Rodriguez, H.; Roman-Belmonte, J.M.; Resino-Luis, C.; Madrid-Gonzalez, J.; Rodriguez-Merchan, E.C. The Role of Physical Exercise in Chronic Musculoskeletal Pain: Best Medicine—A Narrative Review. Healthcare 2024, 12, 242. [Google Scholar] [CrossRef] [PubMed]
- Rice, D.; Nijs, J.; Kosek, E.; Wideman, T.; I Hasenbring, M.; Koltyn, K.; Graven-Nielsen, T.; Polli, A. Exercise-Induced Hypoalgesia in Pain-Free and Chronic Pain Populations: State of the Art and Future Directions. J. Pain 2019, 20, 1249–1266. [Google Scholar] [CrossRef] [PubMed]
- Ambrose, K.R.; Golightly, Y.M. Physical exercise as non-pharmacological treatment of chronic pain: Why and when. Best Pract. Res. Clin. Rheumatol 2015, 29, 120–130. [Google Scholar] [CrossRef]
- Naugle, K.M.; Naugle, K.E.; Fillingim, R.B.; Samuels, B.; Riley, J.L. Intensity thresholds for aerobic exercise-induced hypoalgesia. Med. Sci. Sports Exerc. 2014, 46, 817–825. [Google Scholar] [CrossRef]
- Xu, Z.; An, N.; Rui, C.J.; Yang, Y. Modulation of pain perceptions following treadmill running with different intensities in females. Physiol. Rep. 2023, 11, e15831. [Google Scholar] [CrossRef]
- Tomschi, F.; Lieverkus, D.; Hilberg, T. Exercise-induced hypoalgesia (EIH) in response to different exercise intensities. Eur. J. Appl. Physiol. 2022, 122, 2213–2222. [Google Scholar] [CrossRef]
- Cunningham, C.; O’ Sullivan, R.; Caserotti, P.; Tully, M.A. Consequences of physical inactivity in older adults: A systematic review of reviews and meta-analyses. Scand. J. Med. Sci. Sports 2020, 30, 816–827. [Google Scholar] [CrossRef]
- Pišot, R. Physical inactivity—The human health’s greatest enemy. Slov. J. Public Health 2022, 61, 1–5. [Google Scholar] [CrossRef]
- World Health Organization. Global Status Report on Physical Activity 2022. Available online: https://www.who.int/publications/i/item/9789240059153 (accessed on 18 July 2024).
- Ding, D.; Lawson, K.D.; Kolbe-Alexander, T.L.; Finkelstein, E.A.; Katzmarzyk, P.T.; van Mechelen, W.; Pratt, M.; Lancet Physical Activity Series 2 Executive Committee. The economic burden of physical inactivity: A global analysis of major non-communicable diseases. Lancet 2016, 388, 1311–1324. [Google Scholar] [CrossRef]
- Santos, A.C.; Willumsen, J.; Meheus, F.; Ilbawi, A.; Bull, F.C. The cost of inaction on physical inactivity to public health-care systems: A population-attributable fraction analysis. Lancet Glob. Health 2023, 11, e32–e39. [Google Scholar] [CrossRef] [PubMed]
- Actividad Física Para el Dolor Crónico: Una Sinopsis de la Evidencia. CDA-AMC. Available online: https://www.cda-amc.ca/physical-activity-chronic-pain-synopsis-evidence (accessed on 5 September 2024).
- World Health Organization. International Classification of Functioning, Disability, and Health (ICF). Available online: https://search.library.wisc.edu/catalog/999977181002121 (accessed on 5 September 2024).
- American Occupational Therapy Association. Occupational Therapy Practice Framework: Domain and Process—Fourth Edition. Am. J. Occup. Ther. 2020, 74, 1–85. [Google Scholar] [CrossRef]
- Stathi, A.; Greaves, C.J.; Thompson, J.L.; Withall, J.; Ladlow, P.; Taylor, G.; Medina-Lara, A.; Snowsill, T.; Gray, S.; Green, C.; et al. Effect of a physical activity and behaviour maintenance programme on functional mobility decline in older adults: The REACT (Retirement in Action) randomised controlled trial. Lancet Public Health 2022, 7, e316–e326. [Google Scholar] [CrossRef]
- Brandão, G.S.; Sampaio, A.A.C.; Andrade, L.D.; Fonseca, A.L.; Campos, F.K.R.; Silva, A.S.; Silva, M.M.; Oliveira-Silva, I.; Vieira, R.P.; Donner, C.F.; et al. Home physical exercise improves functional mobility and quality of life in the elderly: A CONSORT-prospective, randomised controlled clinical trial. Int. J. Clin. Pract. 2021, 75, e14347. [Google Scholar] [CrossRef]
- López-López, S.; Abuín-Porras, V.; Berlanga, L.A.; Martos-Duarte, M.; Perea-Unceta, L.; Romero-Morales, C.; Pareja-Galeano, H. Functional mobility and physical fitness are improved through a multicomponent training program in institutionalized older adults. GeroScience 2023, 46, 1201–1209. [Google Scholar] [CrossRef]
- Bonner, W.I.A.; Weiler, R.; Orisatoki, R.; Lu, X.; Andkhoie, M.; Ramsay, D.; Yaghoubi, M.; Steeves, M.; Szafron, M.; Farag, M. Determinants of self-perceived health for Canadians aged 40 and older and policy implications. Int. J. Equity Health 2017, 16, 94. [Google Scholar] [CrossRef]
- Machón, M.; Vergara, I.; Dorronsoro, M.; Vrotsou, K.; Larrañaga, I. Self-perceived health in functionally independent older people: Associated factors. BMC Geriatr. 2016, 16, 66. [Google Scholar] [CrossRef]
- Moor, I.; Spallek, J.; Richter, M. Explaining socioeconomic inequalities in self-rated health: A systematic review of the relative contribution of material, psychosocial and behavioural factors. J. Epidemiol. Community Health 2017, 71, 565–575. [Google Scholar] [CrossRef]
- Caramenti, M.; Castiglioni, I. Determinants of Self-Perceived Health: The Importance of Physical Well-Being but Also of Mental Health and Cognitive Functioning. Behav. Sci. 2022, 12, 498. [Google Scholar] [CrossRef]
- Raja, S.N.; Carr, D.B.; Cohen, M.; Finnerup, N.B.; Flor, H.; Gibson, S.; Keefe, F.J.; Mogil, J.S.; Ringkamp, M.; Sluka, K.A.; et al. The revised International Association for the Study of Pain definition of pain: Concepts, challenges, and compromises. Pain 2020, 161, 1976–1982. [Google Scholar] [CrossRef]
- Pereira, L.V.; de Vasconcelos, P.P.; Souza, L.A.F.; Pereira, G.d.A.; Nakatani, A.Y.K.; Bachion, M.M. Prevalence and intensity of chronic pain and self-perceived health among elderly people: A population-based study. Rev. Lat.-Am. Enferm. 2014, 22, 662–669. [Google Scholar] [CrossRef] [PubMed]
- Denche-Zamorano, Á.; Mendoza-Muñoz, M.; Carlos-Vivas, J.; Muñoz-Bermejo, L.; Rojo-Ramos, J.; Pastor-Cisneros, R.; Giakoni-Ramírez, F.; Godoy-Cumillaf, A.; Barrios-Fernandez, S. A Cross-Sectional Study on Self-Perceived Health and Physical Activity Level in the Spanish Population. Int. J. Environ. Res. Public Health 2022, 19, 5656. [Google Scholar] [CrossRef]
- Denche-Zamorano, A.; Perez-Gomez, J.; Barrios-Fernandez, S.; Oliveira, R.; Adsuar, J.C.; Brito, J.P. Relationships between Physical Activity Frequency and Self-Perceived Health, Self-Reported Depression, and Depressive Symptoms in Spanish Older Adults with Diabetes: A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2023, 20, 2857. [Google Scholar] [CrossRef]
- Dostálová, R.; Stillman, C.; Erickson, K.I.; Slepička, P.; Mudrák, J. The Relationship between Physical Activity, Self-Perceived Health, and Cognitive Function in Older Adults. Brain Sci. 2021, 11, 492. [Google Scholar] [CrossRef]
- Smith, J.; Ylitalo, K.R. Physical activity recommendation by health care providers to adults with and without functional limitations. Prev. Med. 2021, 153, 106730. [Google Scholar] [CrossRef]
- Instituto Nacional de Estadística. Clasificación Nacional de Ocupaciones. CNO-11. Available online: https://www.ine.es/dyngs/INEbase/es/operacion.htm?c=Estadistica_C&cid=1254736177033&menu=ultiDatos&idp=1254735976614 (accessed on 16 May 2023).
- Umeda, M.; Kim, Y. Gender Differences in the Prevalence of Chronic Pain and Leisure Time Physical Activity Among US Adults: A NHANES Study. Int. J. Environ. Res. Public Health 2019, 16, 988. [Google Scholar] [CrossRef]
- Australian Institute of Health and Welfare. Chronic Pain in Australia. Available online: https://www.aihw.gov.au/getmedia/10434b6f-2147-46ab-b654-a90f05592d35/aihw-phe-267.pdf.aspx (accessed on 15 July 2024).
- Meana, M.; Cho, R.; DesMeules, M. Chronic Pain: The Extra Burden on Canadian Women. BMC Women’s Health 2004, 4, S17. [Google Scholar] [CrossRef]
- Osborne, N.R.; Davis, K.D. Sex and gender differences in pain. Int. Rev. Neurobiol. 2022, 164, 277–307. [Google Scholar] [CrossRef]
- eClinicalMedicine. Gendered pain: A call for recognition and health equity. eClinicalMedicine 2024, 69, 102558. [Google Scholar] [CrossRef]
- Okifuji, A.; Hare, B. The association between chronic pain and obesity. J. Pain Res. 2015, 14, 399–408. [Google Scholar] [CrossRef]
- Chin, S.-H.; Huang, W.-L.; Akter, S.; Binks, M. Obesity and pain: A systematic review. Int. J. Obes. 2020, 44, 969–979. [Google Scholar] [CrossRef] [PubMed]
- Olsson, M.; Currow, D.C.; Ekström, M.P. Exploring the most important factors related to self-perceived health among older men in Sweden: A cross-sectional study using machine learning. BMJ Open 2022, 12, e061242. [Google Scholar] [CrossRef] [PubMed]
- Rojas-Caballero, J.; Zacaria, V.E.; Ferreira-Gaona, M.; Díaz-Reissner, C. Chronic pain and general self-perceived health in a Paraguayan reference hospital. Rev. Salud Publica Parag. 2019, 9, 41–46. [Google Scholar] [CrossRef]
- Morais, E.; Pinheira, V. Chronic Pain and Functional Mobility—Relationships and Impact on the Quality of Life of the Elderly. In Longevity and Development: New Perspectives on Ageing Communities, Proceedings of the 2nd International Congress Age.Comm, 11–12 November 2021; Lecture Notes in Bioengineering; Moreira, M.J.G., Carvalho, L.S.A., Gonçalves, P.J.S., Pinheira, V.M.B., Eds.; Springer: Cham, Switzerland, 2021; pp. 119–134. [Google Scholar] [CrossRef]
- Pelletier, R.; Purcell-Lévesque, L.; Girard, M.-C.; Roy, P.-M.; Léonard, G. Pain Intensity and Functional Outcomes for Activities of Daily Living, Gait and Balance in Older Adults Accessing Outpatient Rehabilitation Services: A Retrospective Study. J. Pain Res. 2020, 13, 2013–2021. [Google Scholar] [CrossRef]
- Hodges, P.W.; Smeets, R.J. Interaction Between Pain, Movement, and Physical Activity: Short-term Benefits, Long-term Consequences, and Targets for Treatment. Clin. J. Pain 2015, 31, 97–107. [Google Scholar] [CrossRef]
- Singh, A.; Akkala, S.; Nayak, M.; Kotlo, A.; Poondla, N.; Raza, S.; Stankovich, J.; Antony, B. Impact of Pain on Activities of Daily Living in Older Adults: A Cross-Sectional Analysis of Korean Longitudinal Study of Aging (KLoSA). Geriatrics 2024, 9, 65. [Google Scholar] [CrossRef]
- Stamm, T.A.; Pieber, K.; Crevenna, R.; Dorner, T.E. Impairment in the activities of daily living in older adults with and without osteoporosis, osteoarthritis and chronic back pain: A secondary analysis of population-based health survey data. BMC Musculoskelet. Disord. 2016, 17, 139. [Google Scholar] [CrossRef]
- Geneen, L.J.; Moore, R.A.; Clarke, C.; Martin, D.; Colvin, L.A.; Smith, B.H. Physical activity and exercise for chronic pain in adults: An overview of Cochrane Reviews. Cochrane Database Syst. Rev. 2017, 4, CD011279. [Google Scholar] [CrossRef]
- Briggs, A.M.; Cross, M.J.; Hoy, D.G.; Sànchez-Riera, L.; Blyth, F.M.; Woolf, A.D.; March, L. Musculoskeletal Health Conditions Represent a Global Threat to Healthy Aging: A Report for the 2015 World Health Organization World Report on Ageing and Health. Gerontol. 2016, 56 (Suppl. S2), S243–S255. [Google Scholar] [CrossRef]
- O’Neill, A.; O’Sullivan, K.; McCreesh, K. Lower levels of physical activity are associated with pain progression in older adults, a longitudinal study. Eur. J. Pain (Lond. Engl.) 2021, 25, 1462–1471. [Google Scholar] [CrossRef] [PubMed]
- Niederstrasser, N.G.; Attridge, N. Associations between pain and physical activity among older adults. PLoS ONE 2022, 17, e0263356. [Google Scholar] [CrossRef] [PubMed]
- Naciones Unidas. The Sustainable Development Goals Summit. Available online: https://www.un.org/en/summits2019/pdf/SDG-Summit.pdf (accessed on 10 June 2023).
- Casale, R.; Atzeni, F.; Bazzichi, L.; Beretta, G.; Costantini, E.; Sacerdote, P.; Tassorelli, C. Pain in Women: A Perspective Review on a Relevant Clinical Issue that Deserves Prioritization. Pain Ther. 2021, 10, 287–314. [Google Scholar] [CrossRef] [PubMed]
- Skinner, A.M.; Rowlands, A.V.; Vlachopoulos, D.; Barker, A.R.; Janz, K.F.; Moore, S.A. The Influence of Accelerometer Epoch Length on Associations of Physical Activity Intensity and Volume with Bone Outcomes. J. Sport Sci. Med. 2023, 22, 117–132. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Denche-Zamorano, Á.; Salas-Gómez, D.; Barrios-Fernandez, S.; Tomás-Carus, P.; Adsuar, J.C.; Parraca, J.A. Relationship Between Frequency of Physical Activity, Functional Mobility, and Self-Perceived Health in People with Different Levels of Pain: A Cross-Sectional Study. J. Funct. Morphol. Kinesiol. 2024, 9, 198. https://doi.org/10.3390/jfmk9040198
Denche-Zamorano Á, Salas-Gómez D, Barrios-Fernandez S, Tomás-Carus P, Adsuar JC, Parraca JA. Relationship Between Frequency of Physical Activity, Functional Mobility, and Self-Perceived Health in People with Different Levels of Pain: A Cross-Sectional Study. Journal of Functional Morphology and Kinesiology. 2024; 9(4):198. https://doi.org/10.3390/jfmk9040198
Chicago/Turabian StyleDenche-Zamorano, Ángel, Diana Salas-Gómez, Sabina Barrios-Fernandez, Pablo Tomás-Carus, José Carmelo Adsuar, and Jose A. Parraca. 2024. "Relationship Between Frequency of Physical Activity, Functional Mobility, and Self-Perceived Health in People with Different Levels of Pain: A Cross-Sectional Study" Journal of Functional Morphology and Kinesiology 9, no. 4: 198. https://doi.org/10.3390/jfmk9040198
APA StyleDenche-Zamorano, Á., Salas-Gómez, D., Barrios-Fernandez, S., Tomás-Carus, P., Adsuar, J. C., & Parraca, J. A. (2024). Relationship Between Frequency of Physical Activity, Functional Mobility, and Self-Perceived Health in People with Different Levels of Pain: A Cross-Sectional Study. Journal of Functional Morphology and Kinesiology, 9(4), 198. https://doi.org/10.3390/jfmk9040198