


J. Funct. Morphol. Kinesiol., Volume 10, Issue 4 (December 2025) – 121 articles
Cover Story (view full-size image):
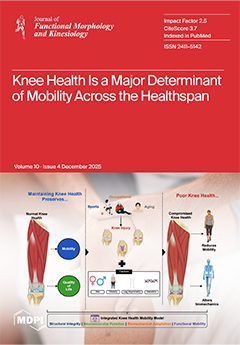
Knee health is a central determinant of mobility and functional independence across the healthspan. While knee pathologies pose global challenges, emerging evidence reveals how injury mechanisms and personal factors converge to disrupt biomechanics and reduce mobility. In this narrative review, we introduce the Integrated Knee Health–Mobility Model to conceptualize knee health as a dynamic system governed by four interconnected domains: structural integrity, neuromuscular function, biomechanical adaptations, and functional mobility. We briefly examine modifying factors, such as age, sex, obesity, limb asymmetry, and genetics, not as barriers but as variables that shape mobility outcomes. Together, these insights underscore the need for targeted interventions to preserve knee health and mitigate long-term decline. View this paper
- Issues are regarded as officially published after their release is announced to the table of contents alert mailing list.
- You may sign up for e-mail alerts to receive table of contents of newly released issues.
- PDF is the official format for papers published in both, html and pdf forms. To view the papers in pdf format, click on the "PDF Full-text" link, and use the free Adobe Reader to open them.
Previous Issue
Next Issue