Simple Summary
Cutaneous pseudolymphomas are non-cancerous skin conditions that can closely resemble skin lymphomas, especially a type called mycosis fungoides, both in appearance and under the microscope. They can be triggered by many causes such as autoimmune diseases, infections, medications, insect bites, or even tattoos. Because they can look very similar to true lymphoma, they can sometimes be misdiagnosed, leading to unnecessary anxiety or treatment. This review explains the main conditions that mimic lymphoma and highlights key clinical and microscopic clues that help doctors tell them apart. These include features like the type of immune cells present, patterns in the skin, and how the condition behaves over time. Understanding these differences is essential to ensure patients receive the correct diagnosis and avoid overtreatment.
Abstract
Cutaneous pseudolymphomas are benign reactive lymphoid proliferations that often mimic cutaneous lymphomas both clinically and histologically. A diverse array of inflammatory, infectious, and drug-induced dermatoses can closely resemble cutaneous T-cell lymphomas (CTCLs), particularly mycosis fungoides (MFs), posing significant diagnostic challenges. These mimickers may show histopathological features such as epidermotropism, dense lymphocytic infiltrates, or even clonality, making accurate differentiation crucial to avoid overtreatment. This review endeavors to comprehensively discuss the clinicopathologic features of the various inflammatory and infectious dermatoses that may simulate CTCL, drawing on illustrative examples across disease categories. By highlighting important comparative features and emphasizing the importance of clinicopathologic correlation, this review outlines practical strategies for distinguishing true lymphoma from its inflammatory mimics.
1. Introduction
Cutaneous pseudolymphomas (CPLs) are benign lymphoid proliferations of the skin that histologically and, at times, clinically resemble cutaneous lymphomas, particularly cutaneous T-cell lymphoma (CTCL). These lesions arise as reactive processes to a wide array of stimuli, including infections, drugs, trauma, autoimmune diseases, and foreign materials such as tattoos, or they may even remain idiopathic [1]. While benign by definition and lacking malignant potential and systemic dissemination, CPLs cannot be differentiated from true lymphoma based on clinical presentation and often exhibit histopathological features that raise suspicion for malignancy.
The diagnostic overlap between pseudolymphomatous inflammatory conditions and CTCL, especially mycosis fungoides (MFs), is well-recognized [2,3]. MF itself is a highly polymorphic disease, with several clinicopathologic variants including lichenoid, spongiotic, psoriasiform, folliculotropic, and zosteriform MF, leading to the frequent misclassification of mimickers that can share features such as band-like lymphocytic infiltrates, epidermotropism, adnexotropism, and even molecular evidence of T-cell clonality [4,5]. In addition, pan–T-cell antigen (CD7) loss or partial loss and predominant CD4+ lymphocytes are not exclusive to lymphoma but may also be observed in inflammatory dermatoses and infection [4,6].
Several autoimmune/inflammatory diseases may closely simulate MF such as lupus erythematosus (LE) [7,8]. Recent studies have highlighted the diagnostic utility of CD123 immunostaining in LE [6,9]. Lichen sclerosus, morphea, and lichen planus are other autoimmune interface dermatoses known to histopathologically mimic CTCL [5,10,11,12]. Syringotropic variants of these conditions further blur the lines with adnexotropic MF [13,14]. Psoriasiform diseases, such as palmoplantar pustular psoriasis (PPPP), can also imitate CTCL/MF [15,16]. Similarly, chronic eczematous dermatoses, such as contact and atopic dermatitis, can display prominent lymphoid infiltrates [17,18,19,20].
Drug-induced pseudolymphomas, particularly fixed drug eruptions (FDEs), may mimic CD8+ epidermotropic CTCL in both immunophenotype and clinical course, making diagnosis particularly challenging [21,22]. Tattoo-related pseudolymphomas, characterized by dense dermal lymphoid infiltrates, often CD4+-predominant, pose another diagnostic trap and have been reported for both black and colored inks [23,24].
Infectious etiologies also comprise a significant proportion of pseudolymphomatous conditions. Cutaneous manifestations of syphilis, molluscum contagiosum, herpes simplex virus, and Borrelia burgdorferi infection have all been described as mimicking cutaneous lymphomas [25,26,27,28,29]. These conditions may show dense lymphoid infiltrates with atypical cells and, in some cases, even clonal rearrangement [30]. Fungal infections, though less frequently discussed, also warrant consideration in the differential diagnosis of CTCL mimickers [2].
Because histologic mimickers of MF are not only challenging but also hold serious implications for patient management, a misdiagnosis of lymphoma may lead to overtreatment with systemic therapies, unnecessary psychosocial burden, and increased surveillance. On the other hand, failure to diagnose CTCL/MF will delay diagnosis and proper therapy until later [4,6]. Therefore, a high index of suspicion, clinicopathologic correlation, and, when necessary, molecular and immunohistochemical adjuncts are indispensable to ensure diagnostic accuracy. This review aims to provide a comprehensive overview of cutaneous inflammatory and infectious conditions that histologically mimic CTCL/MF. Each entity is described with attention to clinical–pathologic hallmarks and distinguishing features.
2. Cutaneous Lupus Erythematous (CLE)
Cutaneous lupus erythematosus may rarely present with pseudolymphomatous lymphoid infiltrates that closely mimic CTCL across multiple clinical subtypes including discoid lupus, lupus tumidus, lupus panniculitis, and mucosal lupus (Figure 1) [8,9,31].
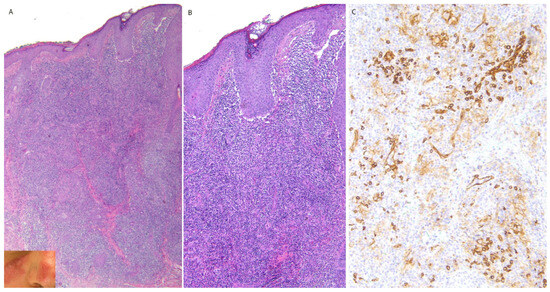
Figure 1.
(A–C) Pseudolymphomatous lupus erythrematosus with CD123-positive pDC clustering. Inset showing the clinical presentation with cheek, nose, and ear involvement. This figure is from the corresponding author’s laboratory and illustrates the pathological concept of typical pseudolymphomatous LE.
Recognition of CD123-positive pDC clustering, in conjunction with dermal mucin, interface change, and preserved T-cell immunophenotype, is critical for distinguishing pseudolymphomatous CLE from true CTCL and avoiding misdiagnosis (Table 1) [6,9,31,32,33].

Table 1.
Pseudolymphomatous cutaneous lupus erythematosus: MF-mimicking features and key distinguishing clues.
3. Lichen Sclerosus (LS)
Lichen sclerosus is a chronic inflammatory dermatosis that may, particularly in early or atypical stages, exhibit pseudolymphomatous histopathologic features closely simulating CTCL, most notably MF, leading to frequent diagnostic confusion (Figure 2) [3,5,10,34].
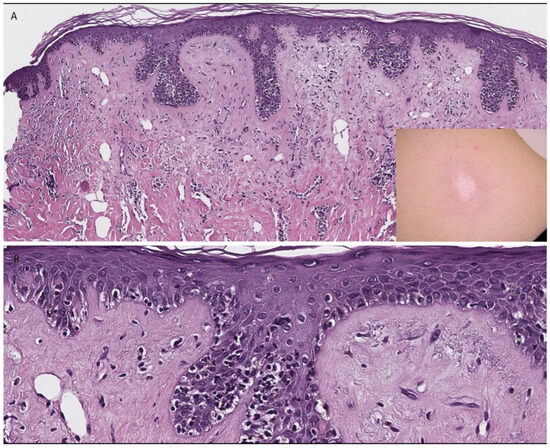
Figure 2.
(A,B) Pseudolymphomatous lichen sclerosus. Inset showing the clinical presentation. This figure is from the corresponding author’s laboratory and illustrates the pathological concept of typical pseudolymphomatous lichen sclerosus.
Early lichen sclerosus is characterized by a lichenoid lymphocytic infiltrate associated with papillary dermal hyalinization and basal vacuolar alteration in the absence of significant cytologic atypia, cerebriform lymphocytes, or disproportionate epidermotropism; involvement of the anogenital region further supports a reactive lichenoid dermatosis rather than mycosis fungoides (Table 2) [3,5,10,34,35].
Table 2.
Pseudolymphomatous lichen sclerosus: MF-mimicking features and key distinguishing clues.
Notably, several studies have demonstrated that lichen sclerosus may exhibit monoclonal T-cell receptor (TCR) gene rearrangements, including γ-chain clonality, despite its benign nature, underscoring that clonality alone does not establish a diagnosis of lymphoma and must be interpreted in the appropriate clinicopathologic context [36,37,38].
4. Vitiligo
Vitiligo is an immune-mediated depigmenting disorder that, in its inflammatory or early stages, may demonstrate pseudolymphomatous histopathologic features mimicking hypopigmented MF, creating a well-recognized diagnostic pitfall (Figure 3) [3,39,40].
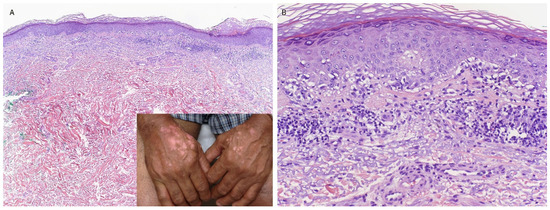
Figure 3.
(A,B) Pseudolymphomatous vitiligo (inset highlights the clinical presentation with depigmented patches on hands). This figure is from the corresponding author’s laboratory and illustrates the pathological concept of typical pseudolymphomatous vitiligo.
The correlation between melanocyte loss, preserved T-cell immunophenotype, type I interferon-associated pDC activity (which promotes local immune activation and recruitment of cytotoxic T cells targeting melanocytes), and clinical evolution is essential for distinguishing pseudolymphomatous vitiligo from hypopigmented MF (Table 3) [3,39,40].
Table 3.
Pseudolymphomatous vitiligo: MF-mimicking features and key distinguishing clues.
5. Pigmented Purpuric Dermatoses/Lichen Aureus
Pigmented purpuric dermatoses (PPD), particularly lichen aureus, may exhibit pseudolymphomatous lymphoid infiltrates that closely mimic CTCL, especially unilesional or purpuric variants of MF, creating a recognized diagnostic pitfall (Figure 4) [41,42,43].
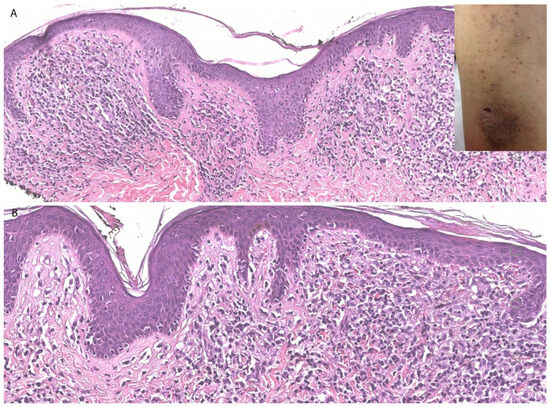
Figure 4.
(A,B) Pigmented purpuric dermatosis. Histology exhibits dense focally band-like dermal lymphoid infiltrate with extravasated erythrocytes. Inset showing the clinical presentation. This figure is from the corresponding author’s laboratory and illustrates the pathological concept of typical pseudolymphomatous PPD.
Recognition of erythrocyte extravasation, hemosiderin deposition, clinical stability, and absence of significant cytologic atypia is essential for distinguishing pseudolymphomatous PPD/lichen aureus from CTCL, even in cases demonstrating partial antigen loss or monoclonal T-cell receptor rearrangements (Table 4) [41,42,43,44].
Table 4.
Pseudolymphomatous pigmented purpuric dermatoses/lichen aureus: MF-mimicking features and key distinguishing clues.
Although most cases of pigmented purpuric dermatoses follow a benign course, patients may rarely subsequently develop lesions diagnostic of mycosis fungoides, and therefore, clinical follow-up is recommended, particularly in cases with widespread or persistent disease [45].
6. Psoriasis
Psoriasis is a chronic immune-mediated dermatosis that in atypical, long-standing, or treatment-resistant presentations may clinically and histopathologically mimic CTCL, particularly MF, and conversely, may be mimicked by MF, resulting in frequent diagnostic confusion [14,15,16].
Recognition of neutrophilic parakeratosis, absence of disproportionate epidermotropism, lack of lymphocyte atypia, and appropriate therapeutic response is essential for distinguishing psoriasis from MF (Table 5) [14,15,16].
Table 5.
Psoriasis as a mimicker of mycosis fungoides: overlapping and distinguishing features.
7. Morphea
Early morphea, particularly in its inflammatory stage, represents an important diagnostic pitfall, as it may closely mimic CTCL, especially MF, both clinically and histopathologically [46]. Several reports have demonstrated that morphea can exhibit band-like lymphocytic infiltrates, epidermotropism, and even interstitial patterns resembling CTCL, including patch-stage and interstitial variants [12]. In some cases, the histopathologic overlap may be striking, with features such as dense dermal lymphoid infiltrates and interface changes raising concern for lymphoma [47]. This overlap has been described in both localized and generalized forms of morphea, further complicating the diagnostic process [12,47]. These findings underscore the importance of careful clinicopathologic correlation and awareness of this entity to avoid misdiagnosis and inappropriate management [46,47].
8. Lichen Planus/Lichenoid Dermatitis
Lichen planus (LP) is a chronic T-cell-mediated inflammatory dermatosis that, particularly in its hypertrophic, adnexotropic, or atypical variants, may demonstrate pseudolymphomatous histopathologic features mimicking CTCL, most notably MF, creating a recognized diagnostic pitfall. Overlap with entities such as lichen striatus (LS) (Figure 5) and lichen planus-like keratosis (Figure 6) further broadens the morphologic spectrum, and several reports document LP or LS initially misinterpreted as lymphoma due to dense infiltrates, adnexotropism, or unusual cytotoxic phenotypes [11,13,48].
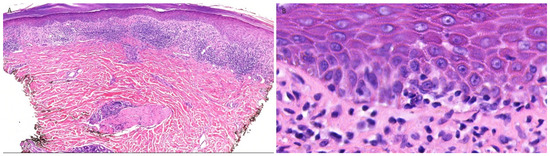
Figure 5.
(A,B) Pseudolymphomatous lichen striatus exhibiting lichenoid interface dermatitis with peri-eccrine involvement. This figure is from the corresponding author’s laboratory and illustrates the pathological concept of typical pseudolymphomatous lichen striatus.
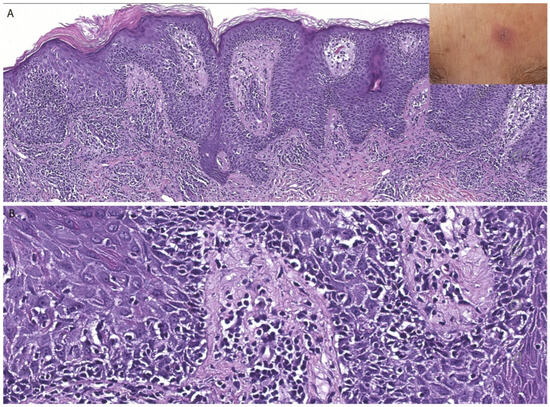
Figure 6.
(A,B) Lichen planus-like keratosis. Inset showing the clinical presentation of a solitary erythematous papule on trunk. This figure is from the corresponding author’s laboratory and illustrates the pathological concept of typical pseudolymphomatous lichen planus-like keratosis.
Recognition of classic interface dermatitis, epidermal hypergranulosis, lack of significant lymphocyte atypia, and absence of reproducible immunophenotypic or molecular aberrations, together with appropriate clinical distribution, is essential for distinguishing pseudolymphomatous LP from CTCL (Table 6) [11,13,48].
Table 6.
Pseudolymphomatous lichen planus: MF-mimicking features and key distinguishing clues.
9. Pityriasis Lichenoides
Pityriasis lichenoides (PL) is an inflammatory dermatosis encompassing a clinical spectrum from pityriasis lichenoides et varioliformis acuta to pityriasis lichenoides chronica, which may exhibit pseudolymphomatous histopathologic features overlapping with CTCL, particularly MF, creating a recognized diagnostic challenge [49,50,51,52,53].
Distinction of PL from MF requires the integration of clinical evolution with crops of lesions, wedge-shaped infiltrates with epidermal necrosis, cytotoxic CD8-positive immunophenotypes, and non-progressive clinical behavior, as molecular clonality alone does not reliably distinguish these entities (Table 7) [49,50,51,52,53].
Table 7.
Pityriasis lichenoides as a mimicker of mycosis fungoides: overlapping and distinguishing features.
10. Annular Lichenoid Dermatitis of Youth
Annular lichenoid dermatitis of youth is an uncommon inflammatory dermatosis primarily affecting children and adolescents that may mimic CTCL, particularly hypopigmented or annular variants of MF, constituting a recognized diagnostic pitfall (Figure 7) [54,55,56,57].
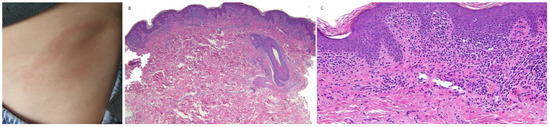
Figure 7.
(A–C) Annular lichenoid dermatitis of youth. (A) Clinical presentation, (B,C) histology exhibiting dense focally lichenoid infiltrate centered at rete ridge tips. This figure is from the corresponding author’s laboratory and illustrates the pathological concept of typical pseudolymphomatous annular lichenoid dermatitis of youth.
Recognition of keratinocyte apoptosis confined to rete ridge tips, absence of cytologic atypia or papillary dermal fibrosis, polyclonal T-cell receptor gene rearrangement, and benign clinical course is essential for distinguishing the annular lichenoid dermatitis of youth from early MF and avoiding the overdiagnosis of CTCL (Table 8) [54,55,56,57].
Table 8.
Annular lichenoid dermatitis of youth as a mimicker of mycosis fungoides: overlapping and distinguishing features.
11. Contact Dermatitis
Contact dermatitis, particularly lymphomatoid contact dermatitis, is a delayed-type hypersensitivity reaction that may develop pseudolymphomatous histopathologic features closely mimicking CTCL/MF, resulting in significant diagnostic difficulty (Figure 8) [17,18,19,20,58].
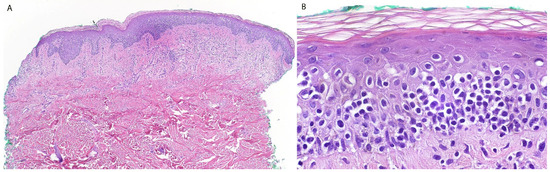
Figure 8.
(A,B) Pseudolymphomatous contact dermatitis. This figure is from the corresponding author’s laboratory and illustrates the pathological concept of typical pseudolymphomatous contact dermatitis.
Common causes of contact dermatitis include rubber compounds, nickel, methylchoroisothiazolinone/methylisothiazolinone, topical medications, and paraphenylenediamine correlation [59]. Correlation of exposure history, presence of spongiosis and eosinophils, preserved T-cell immunophenotype, and rapid clinical improvement following allergen avoidance is essential for distinguishing lymphomatoid contact dermatitis from MF/CTCL (Table 9) [17,18,19,20,58,59,60,61].
Table 9.
Lymphomatoid contact dermatitis as a mimicker of mycosis fungoides: overlapping and distinguishing features.
Hyperkeratotic palmoplantar eczema represents an additional important clinical and histopathologic mimicker of MF, particularly in acral sites. Histologically, features such as clustered intraepidermal lymphocytes and Langerhans cell microgranulomas favor an eczematous process over MF [60].
12. Actinic Reticuloid
Actinic reticuloid, also called chronic actinic dermatitis, is a severe photosensitive inflammatory dermatosis that may demonstrate pseudolymphomatous histopathologic features closely mimicking CTCL/MF [3,62,63,64].
Integration of marked photosensitivity, eczematous epidermal changes, CD8-predominant immunophenotype, and polyclonal molecular findings, together with clinical phototesting when available, is essential for distinguishing actinic reticuloid from MF/CTCL (Table 10) [3,62,63,64,65].
Table 10.
Actinic reticuloid as a mimicker of mycosis fungoides: overlapping and distinguishing features.
13. Arthropod Bite Reactions
Arthropod bite reactions may occasionally elicit a pseudolymphomatous cutaneous lymphoid infiltrate that mimics CTCL and represent a well-recognized cause of diagnostic confusion within the spectrum of cutaneous pseudolymphomas [66,67,68,69,70]. In such cases, including tick bites, deeper histologic sections may reveal the inciting associated changes, highlighting the importance of thorough tissue evaluation and clinicopathologic correlation [70]. They may more frequently mimic other cutaneous lymphoproliferative disorders such as lymphomatoid papulosis or primary cutaneous CD4-positive small/medium T-cell lymphoproliferative disorder. Nonetheless, overlap with MF may arise in cases with dense lymphoid infiltrates and limited epidermotropism, warranting careful clinicopathologic correlation [71].
Recognition of a polymorphous inflammatory infiltrate rich in eosinophils, together with appropriate clinical distribution, preserved immunophenotype, and benign clinical evolution, is essential for distinguishing arthropod bite reactions from CTCL (Table 11) [66,67,68,69,70].
Table 11.
Pseudolymphomatous arthropod bite reactions: MF-mimicking features and key distinguishing clues.
14. Drug Reactions
Pseudolymphomatous drug reactions represent benign, medication-induced lymphoid proliferations that clinically and histopathologically resemble cutaneous lymphomas, particularly MF. These reactions may arise in classic drug-induced pseudolymphoma syndromes or within variants such as fixed drug eruptions (FDEs), where dense epidermotropic lymphoid infiltrates can simulate MF. Clinically, patients may present with persistent or recurrent patches or plaques that may be localized or generalized, showing a chronicity, distribution pattern, or morphology that overlaps with early CTCL [22,72,73]. The latency between drug initiation and eruption is variable, typically ranging from days to several weeks, although longer intervals have been reported, while resolution is generally observed within weeks after discontinuation of the offending agent [58].
Histopathologically, drug eruptions exhibit a lichenoid or interface dermatitis with basal vacuolar degeneration, necrotic keratinocytes, and a superficial perivascular lymphocytic infiltrate, often with eosinophils or neutrophils. FDEs, in particular, demonstrate recurrent lesions at identical sites upon re-exposure and may show intraepidermal vesiculation, pigment incontinence, and a CD8-predominant epidermotropic infiltrate. The localization and persistence of intraepidermal CD8+ memory T cells explain both the fixed nature of these eruptions and their histologic resemblance to CD8+ lymphoproliferative disorders, including MF mimickers. Such overlap has been highlighted in reported cases of generalized FDE, including amlodipine-triggered disease, where plaques were clinically indistinguishable from MF prior to drug withdrawal [22]. In addition to FDE, commonly implicated agents in pseudolymphomatous reactions include anticonvulsants (e.g., phenytoin, carbamazepine), antibiotics, antihypertensives, and biologic agents [58].
The pseudolymphomatous variant is identified when the inflammatory infiltrate becomes sufficiently dense, band-like, epidermotropic, or cytologically atypical to simulate MF. Drug-induced pseudolymphoma may demonstrate Pautrier-like collections, cerebriform lymphocytes, and either CD4- or CD8-predominant phenotypes that closely parallel CTCL. Importantly, T-cell receptor gene rearrangement studies may show clonality, which does not exclude a drug etiology. Clonality has been repeatedly documented in reactive drug eruptions, especially in FDE, and must therefore be interpreted with clinical correlation rather than used alone to establish malignancy [72]. Cases of multifocal or generalized FDE induced by drugs such as NSAIDs or amlodipine have closely mimicked MF before the drug trigger was identified [22,72,73].
Drug reaction with eosinophilia and systemic symptoms (DRESS), also referred to as drug-induced hypersensitivity syndrome, may also present with dense lymphoid infiltrates and atypical lymphocytes, occasionally mimicking CTCL both clinically and histopathologically [74].
Additionally, rare MF-like lymphomatoid reactions have been reported following vaccination, including COVID-19 vaccines [75].
Features supporting a drug-related process include a clear temporal relationship between medication exposure and lesion appearance, recurrence of identical lesions with re-challenge, presence of eosinophils or neutrophils within the infiltrate, and complete or near-complete resolution after discontinuation of the suspected agent [72,73].
15. Tattoo-Related Pseudolymphoma
Tattoo-related pseudolymphoma refers to a benign lymphoid proliferation that develops within a tattoo, typically months to years after placement. Clinically, these lesions often arise as pruritic or asymptomatic erythematous plaques or nodules restricted to specific pigment colors, most notably red, which commonly contains mercury sulfide. Although most cases are localized, they may cause significant diagnostic concern due to their resemblance to cutaneous lymphomas and their sometimes indolent but persistent clinical course [76].
Typical histopathology shows a dense lymphoid infiltrate involving the upper and mid-dermis, often with a top-heavy pattern and a preserved or partial grenz zone. Epidermal changes may include acanthosis, parakeratosis, spongiosis, or focal interface dermatitis. Pigment granules (commonly red or black) are frequently identified. The infiltrate may display a mixture of small and medium lymphocytes with scattered histiocytes and plasma cells, and granulomatous aggregates can be present. Immunophenotyping often reveals a predominance of T lymphocytes (CD2+, CD3+, and CD4+), though B-cell-rich patterns also occur. Importantly, T-cell-predominant lesions remain polyclonal, supporting a reactive process [23,24,76]. In some cases, atypical lymphocytes may express CD30, raising a differential diagnosis of lymphomatoid papulosis [2].
The pseudolymphomatous variant becomes diagnostically challenging, because its dense, sometimes atypical lymphoid infiltrate and epidermotropism may simulate CTCL. Loss of pan-T markers such as CD7, irregular nuclear contours, and infiltration between collagen bundles can further mimic lymphoma histologically [23]. However, several key features favor pseudolymphoma, like the presence of abundant tattoo pigment within the infiltrate, confinement of inflammation to the pigmented areas, especially red pigment, and a polyclonal lymphoid population on molecular studies [23,24]. The latency between tattooing and lesion onset can range from months to decades, with occasional reports of flares triggered by sunlight or sweating, underscoring the role of delayed hypersensitivity reactions to metallic pigments [23,24,76].
16. Pseudolymphomatous Folliculitis
Folliculitis is an inflammatory disorder of the hair follicle that clinically presents as follicular papules or nodules and histologically as perifollicular and intrafollicular inflammatory infiltrates without cytologic atypia [77]. Pseudolymphomatous folliculitis (PLF) is a rare benign cutaneous pseudolymphoma characterized by a dense lymphoid infiltrate centered on and invading hair follicles, often presenting as a solitary papule or nodule on the face, scalp, or nose. An initial case series established PLF as a distinct entity defined by a deep, folliculocentric, polymorphous lymphoid infiltrate that closely mimics cutaneous lymphoma but lacks cytologic features (Figure 9) [78]. A rare variant of follicular mycosis fungoides can elicit comedones, clinically and histologically, whereas this feature is absent in pseudolymphomatous folliculitis [79]. Subsequent reports expanded the morphologic spectrum of PLF, demonstrating that lesions may show marked folliculotropism and even focal epidermotropism [80,81,82].
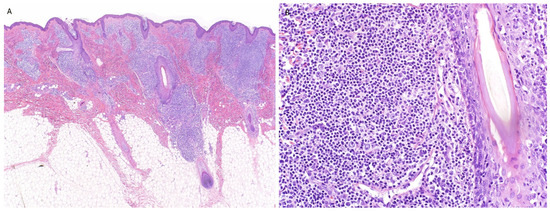
Figure 9.
(A,B) Pseudolymphomatous folliculitis exhibiting dense folliculocentric lymphoid infiltrate. This figure is from the corresponding author’s laboratory and illustrates the pathological concept of typical pseudolymphomatous folliculitis.
Distinction from CTCL, particularly folliculotropic MF, relies on architectural, cytologic, immunophenotypic, and molecular features. PLF shows a polymorphous infiltrate with the preservation of follicular structures, retention of pan–T-cell antigens, and polyclonal T-cell receptor gene rearrangements [78,80,81]. In contrast, CTCL demonstrates monomorphic atypical lymphocytes with cerebriform nuclei, true follicular epidermotropism, aberrant antigen loss (e.g., CD7), and clonal T-cell receptor rearrangements [83].
17. Syphilis
Syphilis is a well-known clinical and histologic imitator of CTCL, and both primary and secondary stages may closely resemble cutaneous or mucosal lymphoproliferative disorders. Typical lesions show dense lymphoplasmacytic infiltrates in lichenoid or perivascular patterns, and this inflammatory richness, especially when plasma cells are abundant, can create concern for lymphoma [84]. Unusual presentations such as oral ulcerations or nodular secondary syphilis intensify this difficulty, as these lesions may be persistent, indurated, or architecturally complex. Several reports have highlighted that secondary and malignant syphilis, particularly in the setting of human immunodeficiency virus (HIV) coinfection, may closely mimic cutaneous T-cell lymphoma both clinically and histologically, with features including epidermotropism, CD8-predominant infiltrates, cytologic atypia, and even monoclonal T-cell receptor rearrangements, which emphasizes that clonality and atypia do not exclude an infectious etiology and must be interpreted alongside serologic and clinical data [85,86,87,88].
Histologically, syphilis may display dense lymphoid aggregates, germinal-center-like structures, or prominent epidermotropism, all of which may mimic MF or B-cell lymphomas. Nodular secondary syphilis has been documented with cerebriform lymphocytes, folliculotropism, and band-like infiltrates that strongly resemble CTCL. Yet the polyclonal nature of the infiltrate, mixed B- and T-cell populations, and especially the presence of numerous plasma cells help distinguish syphilis from true lymphoma [3,25].
Distinguishing syphilis-induced pseudolymphoma from true lymphoma requires careful clinicopathologic correlation. Polyclonality of plasma cells, equal κ and λ light-chain expression, and the presence of both CD20+ B cells and CD3+ T cells contrast with the monotypic or aberrant profiles seen in neoplastic lymphoproliferations. The identification of Treponema pallidum by immunohistochemistry or serologic confirmation is critical, especially when histology is misleading, as serologic tests may be initially nonreactive in primary disease or affected by the prozone phenomenon [25,84]. Importantly, prompt resolution of lesions following penicillin therapy strongly supports a syphilitic pseudolymphomatous process [3,25,84].
18. Borrelia
Borrelial lymphocytoma is a cutaneous pseudolymphoma triggered by Borrelia burgdorferi and presents as a solitary red violaceous nodule or plaque, most often on the nipple, earlobe, or genital area in endemic regions [27]. It usually appears weeks to months after a tick bite and typically resolves completely after appropriate antibiotic therapy. Although lesions may arise at the site of the initial tick bite, they are not strictly confined to it and can occur at distant cutaneous locations, reflecting the disseminated nature of Borrelia infection [89].
Histopathology shows dense dermal lymphoid infiltrates with prominent germinal centers, which may appear blastic, confluent, or lack mantle zones, which are architectural patterns that can resemble B-cell lymphoma (). Plasma cells and eosinophils are commonly present, and germinal centers characteristically express CD10 and BCL6 while lacking BCL2, a profile favoring a reactive rather than neoplastic process [27]. In addition to the classic B-cell-rich infiltrates, cutaneous borreliosis may also present with T-cell-predominant infiltrates that show epidermotropism, cytologic atypia, and band-like patterns, raising concern for MF [30]. However, the presence of mixed inflammatory cells, polytypic plasma cells, tingible body macrophages, and appropriate anatomic distribution strongly support a reactive Borrelia-associated process [27,30].
Detection of Borrelia may aid in confirming the diagnosis. Serologic testing and tissue-based methods such as polymerase chain reaction (PCR) can be helpful; however, the organism is not always demonstrable, and a negative result does not exclude the diagnosis in the appropriate clinicopathologic context [30].
19. Molluscum Contagiosum, Milker’s Nodules, and Orf
Molluscum contagiosum (MC) may rarely trigger a pseudolymphomatous reaction. Typical MC shows a lobulated endophytic proliferation with molluscum bodies in keratinocytes, but in atypical presentations, especially in older adults, unusual locations, or inflamed lesions, the dermal response may be unusually dense [90]. Recognition of molluscum bodies is the key diagnostic clue. The pseudolymphomatous variant of MC typically shows a predominance of CD3+ T cells, often CD4-biased, with scattered CD20+ cells and occasional CD30 expression [26,90]. Despite alarming atypia, clonal TCR rearrangements are consistently absent, and lesions resolve after excision or spontaneously, supporting their reactive nature.
Milker’s nodules, caused by Parapoxvirus (pseudocowpox), are zoonotic infections producing solitary or multiple tender nodules on the hands after exposure to infected cattle. Histopathology shows epidermal necrosis, ballooning degeneration, and a dermal mixed infiltrate composed of lymphocytes, histiocytes, and eosinophils. Rare reports document exuberant lymphoid hyperplasia with atypical lymphocytes simulating lymphoma, but absence of clonality and the presence of viral cytopathic changes favor a reactive interpretation [91]. Lesions resolve spontaneously within 4–6 weeks, supporting their benign nature.
Orf (ecthyma contagiosum), caused by the related Parapoxvirus of sheep and goats, can trigger pseudolymphoma. Orf-related pseudolymphoma presents as persistent nodules with a dense dermal lymphocytic infiltrate, often with germinal center formation and features resembling cutaneous B-cell pseudolymphoma. Histopathology may show epidermal acanthosis, ballooning degeneration, and viral inclusions, but deeper sections reveal lymphoid follicles with polyclonal B cells and mixed T cells [72]. The key distinguishing features are the presence of viral changes in the epidermis, a polymorphous and polyclonal infiltrate, and complete resolution over weeks.
20. Herpetic Infections
Herpes simplex virus (HSV-1/2) and varicella zoster virus (VZV) can occasionally produce atypical lesions that lack vesicles and instead present as plaques or nodules that are clinically suspicious for lymphoma. In these situations, biopsies may reveal dense lymphoid infiltrates with cytologic atypia that closely mimic CTCL or CD30+ lymphoproliferative disorders [28,29,92,93].
The typical histopathology of herpes infections includes ballooning degeneration, necrotic keratinocytes, and multinucleated keratinocytes with margination, but in atypical cases, these epidermal changes may be subtle or absent. The pseudolymphomatous variant is characterized by dense, often superficial, and deep perivascular and periadnexal lymphoid infiltrates with atypical lymphocytes, angiotropism or angiodestruction, and at times, extension into the subcutis [28,92]. Immunohistochemically, these infiltrates are typically T-cell-predominant (CD3+) and often CD4-skewed, with variable numbers of CD30+ and CD56+ cells; in some cases, CD30+ cells form clusters that are virtually indistinguishable from CD30+ lymphoproliferative disorders [28,92]. Rarely, the PCR for T-cell receptor genes reveals a monoclonal band [28]. Cases of herpes folliculitis with dense atypical infiltrates and CD56+ cells have been initially interpreted as angiocentric lymphoma before deeper or additional sections revealed herpetic cytopathic changes [29,92].
21. Scabies
Scabies, especially its nodular form, can mimic cutaneous lymphoma [3]. On routine histology, typical scabies show epidermal spongiosis, parakeratosis, eosinophils, and sometimes mites in the stratum corneum. However, nodular lesions instead reveal a deep, dense, T-cell-rich infiltrate with eosinophils and plasma cells, occasionally accompanied by epidermotropism or Pautrier-like collections [3,94]. In some cases, activated large atypical lymphocytes may express CD30, raising concern for lymphomatoid papulosis (LyP) or other CD30+ lymphoproliferative disorders [95].
Molecular studies are generally polyclonal, though occasional oligoclonal or faint clonal T-cell receptor rearrangements have been reported [3,69,95]. While the identification of mites or their products can be helpful, particularly with deeper sections, nodular scabies lesions often represent a hypersensitivity reaction, and the organism may not be demonstrable [95].
Distinguishing scabies-associated pseudolymphoma requires recognizing a mixed infiltrate with eosinophils and plasma cells and integrating clinical clues such as intense pruritus, affected household members, or lesions in genital or axillary regions, and/or improvement after scabicidal therapy [3,69,95].
22. Nevoid Hyperkeratosis of the Nipple/Areola
Nevoid hyperkeratosis of the nipple and areola (NHNA) is a rare benign disorder presenting as verrucous or velvety plaques on the nipple–areolar complex, most commonly in women, and often associated with hormonal changes such as puberty, pregnancy, or estrogen exposure [96,97]. Histopathology typically reveals marked hyperkeratosis, papillomatosis, acanthosis, and keratin plugging with only a mild superficial dermal infiltrate [96,97].
Rarely, NHNA exhibits epidermotropic lymphocytes with a CD3+- and CD4-predominant immunophenotype and partial CD7 loss [96,97,98]. The superficial dermal sclerosis, thickened collagen, and stellate fibroblasts sometimes observed in NHNA [96,97] can further complicate the picture by resembling fibrosing variants of CTCL [96,99]. However, key distinguishing features include the preservation of epidermal architecture [96,98], lymphocytes lacking significant cytologic atypia [96,99], polyclonal or indeterminate TCR gene rearrangement patterns [96,99], and the strict anatomic confinement of lesions to the nipple–areolar complex.
23. Conclusions
CTCLs, especially MF, represent one of the most challenging diagnoses in dermatology, because their presentations substantially histologically overlap with a wide spectrum of benign inflammatory and infectious dermatoses. This review underlines the crucial importance of clinicopathologic correlation and the judicious use of immunohistochemistry and molecular studies to distinguish CTCL from the other entities that mimic it, including multiple common autoimmune and infectious diseases.
Author Contributions
Conceptualization, O.A.; methodology, validation, formal analysis, resources, data curation, writing—original draft preparation, J.N.E. and E.E.T.; writing—review and editing, supervision, and project administration, O.A. and J.B. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
No new data were created or analysed in this study. Further inquiries can be directed to the corresponding author.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Bergman, R. Pseudolymphoma and Cutaneous Lymphoma: Facts and Controversies. Clin. Dermatol. 2010, 28, 568–574. [Google Scholar] [CrossRef]
- Mitteldorf, C. Inflammatory and Infectious Skin Diseases Presenting as Cutaneous Pseudolymphoma. Diagn. Histopathol. 2021, 27, 42–52. [Google Scholar] [CrossRef]
- Reddy, K.; Bhawan, J. Histologic Mimickers of Mycosis Fungoides: A Review. J. Cutan. Pathol. 2007, 34, 519–525. [Google Scholar] [CrossRef]
- Arps, D.P.; Chen, S.; Fullen, D.R.; Hristov, A.C. Selected Inflammatory Imitators of Mycosis Fungoides: Histologic Features and Utility of Ancillary Studies. Arch. Pathol. Lab. Med. 2014, 138, 1319–1327. [Google Scholar] [CrossRef]
- Suchak, R.; Verdolini, R.; Robson, A.; Stefanato, C.M. Extragenital Lichen Sclerosus et Atrophicus Mimicking Cutaneous T-cell Lymphoma: Report of a Case. J. Cutan. Pathol. 2010, 37, 982–986. [Google Scholar] [CrossRef]
- Chen, S.J.T.; Tse, J.Y.; Harms, P.W.; Hristov, A.C.; Chan, M.P. Utility of CD 123 Immunohistochemistry in Differentiating Lupus Erythematosus from Cutaneous T Cell Lymphoma. Histopathology 2019, 74, 908–916. [Google Scholar] [CrossRef]
- Tallon, B.; Kaddu, S.; Cerroni, L.; Kerl, H.; Aberer, E. Pseudolymphomatous Tumid Lupus Erythematosus of the Oral Mucosa. Am. J. Dermatopathol. 2010, 32, 704–707. [Google Scholar] [CrossRef] [PubMed]
- Umeda, Y.; Ito, K.; Ansai, S.; Hoashi, T.; Saeki, H.; Kanda, N. Lupus Erythematosus Tumidus with Pseudolymphomatous Infiltrates: A Case Report. J. Nippon Med. Sch. 2020, 87, 100–103. [Google Scholar] [CrossRef] [PubMed]
- Roda, Â.; Travassos, A.R.; Soares-de-Almeida, L.; Kutzner, H. Lupus Erythematosus Mimicking Mycosis Fungoides: CD123+ Plasmacytoid Dendritic Cells as a Useful Diagnostic Clue. J. Cutan. Pathol. 2019, 46, 167–170. [Google Scholar] [CrossRef]
- Leoni, E.; Kempf, W.; Cerroni, L. Lichen Sclerosus et Atrophicus With Histopathologic Features Mimicking Mycosis Fungoides: A Large Series of Cases Comparing Genital With Extragenital Lichen Sclerosus. Am. J. Surg. Pathol. 2022, 46, 83–88. [Google Scholar] [CrossRef] [PubMed]
- Mohaghegh, F.; Khodashenas, Z.; Saber, M.; Sohrabi, H. Syringotropic Lichen Planus: An Unusual Presentation of a Common Dermatosis—A Report of 2 Cases. Case Rep. Dermatol. 2024, 16, 226–233. [Google Scholar] [CrossRef]
- Go, J.; Wu, Y. Generalized Early Inflammatory Morphea Mimicking Interstitial T-cell Lymphoma: A Diagnostic Pitfall. J. Cutan. Pathol. 2024, 51, 34–39. [Google Scholar] [CrossRef]
- Mazzeo, M.; Saggini, A.; Rocco, T.; Fargnoli, M.C.; Cerroni, L. Syringotropic Lichen Planus: A Potential Histopathologic Mimicker of Syringotropic Mycosis Fungoides. Am. J. Dermatopathol. 2019, 41, e50–e53. [Google Scholar] [CrossRef]
- Wang, L.; Chen, F.; Liu, Y.; Gao, T.; Wang, G. Lichen Striatus with Syringotropism and Hyperplasia of Eccrine Gland Cells: A Rare Phenomenon That Should Not Be Confused with Syringotropic Mycosis Fungoides. J. Cutan. Pathol. 2016, 43, 927–931. [Google Scholar] [CrossRef]
- Hignett, E.; Seminario-Vidal, L.; Shulman, K.; Sami, N. Cutaneous T-cell Lymphoma Mimicking Palmoplantar Pustular Psoriasis: A Rare Variant. Australas. J. Dermatol. 2021, 62, E280–E282. [Google Scholar] [CrossRef] [PubMed]
- Vaudreuil, A.M.; Stroud, C.M.; Hsu, S. Psoriasis Mimicking Mycosis Fungoides Clinically. Dermatol. Online J. 2017, 23, 16. [Google Scholar] [CrossRef]
- Ezzedine, K.; Rafii, N.; Heenen, M. Lymphomatoid Contact Dermatitis to an Exotic Wood: A Very Harmful Toilet Seat. Contact Dermat. 2007, 57, 128–130. [Google Scholar] [CrossRef]
- Knackstedt, T.J.; Zug, K.A. T Cell Lymphomatoid Contact Dermatitis: A Challenging Case and Review of the Literature. Contact Dermat. 2015, 72, 65–74. [Google Scholar] [CrossRef]
- Gatica-Ortega, M.; Pastor-Nieto, M.; Schoendorff-Ortega, C.; Mollejo-Villanueva, M.; Giménez-Arnau, A. Lymphomatoid Contact Dermatitis Caused by Limonene Hydroperoxides Confirmed by an Exposure Provocation Test with the Involved Personal Hygiene Products. Contact Dermat. 2018, 78, 230–233. [Google Scholar] [CrossRef] [PubMed]
- Mendese, G. Lymphomatoid Contact Dermatitis to Baby Wipes. Arch. Dermatol. 2010, 146, 918. [Google Scholar] [CrossRef]
- Jacobsen, E.; Tarabadkar, E.S.; Shinohara, M.M. Generalized Fixed Drug Eruption Mimicking CD8+ Cutaneous T-cell Lymphoma in HIV. J. Cutan. Pathol. 2019, 46, 134–137. [Google Scholar] [CrossRef]
- Çetinarslan, T.; Ermertcan, A.T.; Temiz, P. Amlodipine-induced Generalized Fixed Drug Eruption Clinically Mimicking Mycosis Fungoides. Dermatol. Ther. 2021, 34, e14775. [Google Scholar] [CrossRef] [PubMed]
- Souza, E.S.; Rocha, B.D.O.; Batista, E.D.S.; Oliveira, R.F.D.; Farre, L.; Bittencourt, A.L. T-Cell-Predominant Lymphoid Hyperplasia in a Tattoo. An. Bras. Dermatol. 2014, 89, 1019–1021. [Google Scholar] [CrossRef]
- Camilot, D.; Arnez, Z.M.; Luzar, B.; Pižem, J.; Žgavec, B.; Falconieri, G. Cutaneous Pseudolymphoma Following Tattoo Application: Report of Two New Cases of a Potential Lymphoma Mimicker. Int. J. Surg. Pathol. 2012, 20, 311–315. [Google Scholar] [CrossRef]
- McComb, M.E.; Telang, G.H.; Vonderheid, E.C. Secondary Syphilis Presenting as Pseudolymphoma of the Skin. J. Am. Acad. Dermatol. 2003, 49, 174–176. [Google Scholar] [CrossRef]
- Del Boz González, J.; Sanz, A.; Martín, T.; Samaniego, E.; Martínez, S.; Crespo, V. Cutaneous Pseudolymphoma Associated with Molluscum Contagiosum: A Case Report. Int. J. Dermatol. 2008, 47, 502–504. [Google Scholar] [CrossRef]
- Colli, C.; Leinweber, B.; Müllegger, R.; Chott, A.; Kerl, H.; Cerroni, L. Borrelia burgdorferi-associated Lymphocytoma Cutis: Clinicopathologic, Immunophenotypic, and Molecular Study of 106 Cases. J. Cutan. Pathol. 2004, 31, 232–240. [Google Scholar] [CrossRef]
- Leinweber, B.; Kerl, H.; Cerroni, L. Histopathologic Features of Cutaneous Herpes Virus Infections (Herpes Simplex, Herpes Varicella/Zoster): A Broad Spectrum of Presentations With Common Pseudolymphomatous Aspects. Am. J. Surg. Pathol. 2006, 30, 50–58. [Google Scholar] [CrossRef]
- Bae-Harboe, Y.-S.C.; Bhawan, J.; Demierre, M.-F.; Goldberg, L.J. Herpes Folliculitis Masquerading as Cutaneous Lymphoma. Am. J. Dermatopathol. 2013, 35, 663–665. [Google Scholar] [CrossRef] [PubMed]
- Kempf, W.; Kazakov, D.V.; Hübscher, E.; Gugerli, O.; Gerbig, A.W.; Schmid, R.; Palmedo, G.; Kutzner, H. Cutaneous Borreliosis Associated with T Cell–Predominant Infiltrates: A Diagnostic Challenge. J. Am. Acad. Dermatol. 2015, 72, 683–689. [Google Scholar] [CrossRef] [PubMed]
- Pereira, A.; Ferrara, G.; Calamaro, P.; Cota, C.; Massone, C.; Boggio, F.; Prieto-Torres, L.; Cerroni, L. The Histopathological Spectrum of Pseudolymphomatous Infiltrates in Cutaneous Lupus Erythematosus. Am. J. Dermatopathol. 2018, 40, 247–253. [Google Scholar] [CrossRef]
- Bardawil, T.; Khalil, S.; Kurban, M.; Abbas, O. Diagnostic Utility of Plasmacytoid Dendritic Cells in Dermatopathology. Indian J. Dermatol. Venereol. Leprol. 2021, 87, 3–13. [Google Scholar] [CrossRef]
- Miyagaki, T. Diagnosis of Early Mycosis Fungoides. Diagnostics 2021, 11, 1721. [Google Scholar] [CrossRef]
- Citarella, L.; Massone, C.; Kerl, H.; Cerroni, L. Lichen Sclerosus with Histopathologic Features Simulating Early Mycosis Fungoides. Am. J. Dermatopathol. 2003, 25, 463–465. [Google Scholar] [CrossRef]
- Parera, E.; Toll, A.; Gallardo, F.; Bellosillo, B.; Pujol, R.M.; Martí, R. Lichen Sclerosus et Atrophicus-like Lesions in Mycosis Fungoides. Br. J. Dermatol. 2007, 157, 411–413. [Google Scholar] [CrossRef]
- Regauer, S.; Reich, O.; Beham-Schmid, C. Monoclonal γ-T-Cell Receptor Rearrangement in Vulvar Lichen Sclerosus and Squamous Cell Carcinomas. Am. J. Pathol. 2002, 160, 1035–1045. [Google Scholar] [CrossRef]
- Regauer, S.; Beham-Schmid, C. Detailed Analysis of the T-cell Lymphocytic Infiltrate in Penile Lichen Sclerosus: An Immunohistochemical and Molecular Investigation. Histopathology 2006, 48, 730–735. [Google Scholar] [CrossRef]
- Lukowsky, A.; Muche, J.M.; Sterry, W.; Audring, H. Detection of Expanded T Cell Clones in Skin Biopsy Samples of Patients with Lichen Sclerosus et Atrophicus by T Cell Receptor-γ Polymerase Chain Reaction Assays. J. Investig. Dermatol. 2000, 115, 254–259. [Google Scholar] [CrossRef]
- Saadeh, D.; Kurban, M.; Abbas, O. Update on the Role of Plasmacytoid Dendritic Cells in Inflammatory/Autoimmune Skin Diseases. Exp. Dermatol. 2016, 25, 415–421. [Google Scholar] [CrossRef]
- Gomez-Moyano, E.; Vera-Casaño, A.; Gamero, A.H.; Sanz-Trelles, A.; Crespo-Erchiga, V. Inflammatory Vitiligo or Hypopigmented Mycosis Fungoides? J. Pediatr. Hematol./Oncol. 2010, 32, 338–339. [Google Scholar] [CrossRef]
- Xavier-Júnior, J.C.C.; Ocanha-Xavier, J.P.; Domingos, M.R.; D’Ávilla, S.C.G.P. Lichen Aureus with Pseudolymphomatous Infiltrate: Other Histopathological Aspects and the Importance of Clinical-pathological Correlation. J. Cutan. Pathol. 2021, 48, 1101–1102. [Google Scholar] [CrossRef]
- Kolm, I.; Buset, C.; Flury, U.; Nosek, D.; Kazakov, D.V.; Kempf, W. Lichen Aureus with Pseudolymphomatous Infiltrate. J. Cutan. Pathol. 2021, 48, 669–673. [Google Scholar] [CrossRef]
- Lor, P.; Krueger, U.; Kempf, W.; Burg, G.; Nestle, F.O. Monoclonal Rearrangement of the T Cell Receptor Gamma-Chain in Lichenoid Pigmented Purpuric Dermatitis of Gougerot-Blum Responding to Topical Corticosteroid Therapy. Dermatology 2002, 205, 191–193. [Google Scholar] [CrossRef]
- Spigariolo, C.B.; Giacalone, S.; Nazzaro, G. Pigmented Purpuric Dermatoses: A Complete Narrative Review. J. Clin. Med. 2021, 10, 2283. [Google Scholar] [CrossRef]
- Riyaz, N.; Sasidharanpillai, S.; Abdul Latheef, E.; Davul, H.; Ashraf, F. Pigmented Purpuric Dermatosis or Mycosis Fungoides: A Diagnostic Dilemma. Indian. Dermatol. Online J. 2016, 7, 183. [Google Scholar] [CrossRef]
- Ghasemi Basir, H.R.; Alirezaei, P.; Rezanejad, A.; Daneshyar, S. Early Morphea Simulating Patch-Stage Mycosis Fungoides in Two Cases. Dermatol. Rep. 2018, 10, 7471. [Google Scholar] [CrossRef]
- Kazmi, A.; Feuerhake, T.; Zidan, A.; Frewen, J.; Carmichael, A.; Ross, J.; Orteu, C.H.; Calonje, E. Morphoea Presenting Histopathologically as Mycosis Fungoides: An Illustrative Series of Four Cases. Histopathology 2024, 85, 353–358. [Google Scholar] [CrossRef]
- Mascolo, M.; Russo, D.; Scalvenzi, M.; Di Lorenzo, P.; Cerroni, L. Lichen Striatus Histopathologically Mimicking Mycosis Fungoides. J. Dtsch. Dermatol. Ges. 2014, 12, 1048–1050. [Google Scholar] [CrossRef][Green Version]
- Bowers, S.; Warshaw, E.M. Pityriasis Lichenoides and Its Subtypes. J. Am. Acad. Dermatol. 2006, 55, 557–572. [Google Scholar] [CrossRef]
- Borra, T.; Custrin, A.; Saggini, A.; Fink-Puches, R.; Cota, C.; Vermi, W.; Facchetti, F.; Cerroni, L. Pityriasis Lichenoides, Atypical Pityriasis Lichenoides, and Related Conditions: A Study of 66 Cases. Am. J. Surg. Pathol. 2018, 42, 1101–1112. [Google Scholar] [CrossRef]
- Tomasini, D.; Tomasini, C.F.; Cerri, A.; Sangalli, G.; Palmedo, G.; Hantschke, M.; Kutzner, H. Pityriasis Lichenoides: A Cytotoxic T-cell-mediated Skin Disorder. Evidence of Human Parvovirus B19 DNA in Nine Cases. J. Cutan. Pathol. 2004, 31, 531–538. [Google Scholar] [CrossRef]
- De Unamuno Bustos, B.; Ferriols, A.P.; Sánchez, R.B.; Rabasco, A.G.; Vela, C.G.; Piris, M.A.; Alegre De Míquel, V. Adult Pityriasis Lichenoides-like Mycosis Fungoides: A Clinical Variant of Mycosis Fungoides. Int. J. Dermatol. 2014, 53, 1331–1338. [Google Scholar] [CrossRef]
- Jang, M.S.; Kang, D.Y.; Park, J.B.; Kim, J.H.; Park, K.A.; Rim, H.; Suh, K.S. Pityriasis Lichenoides-like Mycosis Fungoides: Clinical and Histologic Features and Response to Phototherapy. Ann. Dermatol. 2016, 28, 540–547. [Google Scholar] [CrossRef] [PubMed]
- Annessi, G.; Paradisi, M.; Angelo, C.; Perez, M.; Puddu, P.; Girolomoni, G. Annular Lichenoid Dermatitis of Youth. J. Am. Acad. Dermatol. 2003, 49, 1029–1036. [Google Scholar] [CrossRef]
- Cesinaro, A.M.; Sighinolfi, P.; Greco, A.; Garagnani, L.; Conti, A.; Fantini, F. Annular Lichenoid Dermatitis of Youth … and Beyond: A Series of 6 Cases. Am. J. Dermatopathol. 2009, 31, 263–267. [Google Scholar] [CrossRef]
- Kazlouskaya, V.; Trager, J.D.K.; Junkins-Hopkins, J.M. Annular Lichenoid Dermatitis of Youth: A Separate Entity or on the Spectrum of Mycosis Fungoides? Case Report and Review of the Literature. J. Cutan. Pathol. 2015, 42, 420–426. [Google Scholar] [CrossRef] [PubMed]
- Di Mercurio, M.; Gisondi, P.; Colato, C.; Schena, D.; Girolomoni, G. Annular Lichenoid Dermatitis of Youth: Report of Six New Cases with Review of the Literature. Dermatology 2015, 231, 195–200. [Google Scholar] [CrossRef]
- Coleman, E.; Bhawan, J. Baby Wet Wipes: An Unusual Culprit of Lymphomatoid Contact Dermatitis Mimicking Mycosis Fungoides. Am. J. Dermatopathol. 2022, 44, 205–206. [Google Scholar] [CrossRef] [PubMed]
- Jones, R.; Horn, H.M. Identifying the Causes of Contact Dermatitis. Practitioner 2014, 258, 27–31, 3. [Google Scholar]
- Kim, S.R.; McNiff, J.M.; Ko, C.J. Clustered Intraepidermal Lymphocytes and Langerhans Cell Microgranulomas Are Consistently Observed in Hyperkeratotic Palmoplantar Eczema Compared with Palmoplantar Psoriasis and Mycosis Fungoides Palmaris et Plantaris. J. Am. Acad. Dermatol. 2022, 87, 884–886. [Google Scholar] [CrossRef]
- Dalton, S.R.; Chandler, W.M.; Abuzeid, M.; Hossler, E.W.; Ferringer, T.; Elston, D.M.; LeBoit, P.E. Eosinophils in Mycosis Fungoides: An Uncommon Finding in the Patch and Plaque Stages. Am. J. Dermatopathol. 2012, 34, 586–591. [Google Scholar] [CrossRef] [PubMed]
- Ive, F.A.; Magnus, I.A.; Wartn, R.P.; Jones, E.W. “Actinic reticuloid”; A chronic dermatosis associated with severe photosensitivity and the histological resemblance to lymphoma. Br. J. Dermatol. 1969, 81, 469–485. [Google Scholar] [CrossRef]
- Bakels, V.; Van Oostveen, J.W.; Preesman, A.H.; Meijer, C.J.; Willemze, R. Differentiation between Actinic Reticuloid and Cutaneous T Cell Lymphoma by T Cell Receptor Gamma Gene Rearrangement Analysis and Immunophenotyping. J. Clin. Pathol. 1998, 51, 154–158. [Google Scholar] [CrossRef]
- Toonstra, J.; Henquet, C.J.; van Weelden, H.; van der Putte, S.C.; van Vloten, W.A. Actinic Reticuloid. A Clinical Photobiologic, Histopathologic, and Follow-u Study of 16 Patients. J. Am. Acad. Dermatol. 1989, 21, 205–214. [Google Scholar]
- Sidiropoulos, M.; Deonizio, J.; Martinez-Escala, M.E.; Gerami, P.; Guitart, J. Chronic Actinic Dermatitis/Actinic Reticuloid: A Clinicopathologic and Immunohistochemical Analysis of 37 Cases. Am. J. Dermatopathol. 2014, 36, 875–881. [Google Scholar] [CrossRef]
- Terhune, M.H. Nodule on the Cheek of an 81-Year-Old Woman. Arch. Dermatol. 1999, 135, 1543-a-1548. [Google Scholar] [CrossRef]
- Choi, M.E.; Lee, K.H.; Lim, D.J.; Won, C.H.; Chang, S.E.; Lee, M.W.; Choi, J.H.; Lee, W.J. Clinical and Histopathological Characteristics of Cutaneous Lymphoid Hyperplasia: A Comparative Study According to Causative Factors. J. Clin. Med. 2020, 9, 1217. [Google Scholar] [CrossRef]
- Alzahrani, A.; Alghamdi, M.K.; Alghamdi, A.S.; Shahbar, S.T. Cutaneous Pseudolymphoma Secondary to Insect Bite: A Case Report. Open Dermatol. J. 2025, 19, e18743722384358. [Google Scholar] [CrossRef]
- Ploysangam, T.; Breneman, D.L.; Mutasim, D.F. Cutaneous Pseudolymphomas. J. Am. Acad. Dermatol. 1998, 38, 877–898. [Google Scholar] [CrossRef] [PubMed]
- Cho, W.C.; Gill, P.; Nagarajan, P.; Aung, P.P.; Torres-Cabala, C.A.; Curry, J.L.; Ivan, D.; Lester, L.; Prieto, V.G. Cutaneous Lymphoid Hyperplasia With T-Cell Clonality and Monotypic Plasma Cells Secondary to a Tick Bite: A Hidden Critter and the Power of Deeper Levels. Am. J. Dermatopathol. 2022, 44, 226–229. [Google Scholar] [CrossRef]
- Verma, D.; Lakhani, R.; Mendiratta, V.; Chatterjee, P. Lymphomatoid Papulosis: A Case Report. Indian Dermatol. Online J. 2024, 15, 95–98. [Google Scholar] [CrossRef]
- Etesami, I.; Kalantari, Y.; Tavakolpour, S.; Mahmoudi, H.; Daneshpazhooh, M. Drug-induced Cutaneous Pseudolymphoma: A Systematic Review of the Literature. Australas. J. Dermatol. 2023, 64, 41–49. [Google Scholar] [CrossRef]
- Guitart, J.; Peduto, M.; Caro, W.A.; Roenigk, H.H. Lichenoid Changes in Mycosis Fungoides. J. Am. Acad. Dermatol. 1997, 36, 417–422. [Google Scholar] [CrossRef]
- Keefe, M.; Buntinx-Krieg, T.; Contestable, J. Angioimmunoblastic T-Cell Lymphoma Mimicking DRESS Syndrome. Cutis 2022, 109, E29–E32. [Google Scholar] [CrossRef] [PubMed]
- Li, H.O.-Y.; Lipson, J. New Mycosis Fungoides-like Lymphomatoid Reaction Following COVID-19 Vaccination: A Case Report. SAGE Open Med. Case Rep. 2022, 10, 2050313X221131859. [Google Scholar] [CrossRef]
- Marchesi, A.; Parodi, P.C.; Brioschi, M.; Marchesi, M.; Bruni, B.; Cangi, M.G.; Vaienti, L. Tattoo Ink-Related Cutaneous Pseudolymphoma: A Rare but Significant Complication. Case Report and Review of the Literature. Aesthetic Plast. Surg. 2014, 38, 471–478. [Google Scholar] [CrossRef]
- Biswas, A. Pearls and Pitfalls in Inflammatory Dermatopathology, 1st ed.; Cambridge University Press: Cambridge, UK, 2016. [Google Scholar]
- Arai, E.; Okubo, H.; Tsuchida, T.; Kitamura, K.; Katayama, I. Pseudolymphomatous Folliculitis: A Clinicopathologic Study of 15 Cases of Cutaneous Pseudolymphoma With Follicular Invasion. Am. J. Surg. Pathol. 1999, 23, 1313. [Google Scholar] [CrossRef]
- Paolino, G.; Caputo, V.; Stabile, G.; Bonoldi, E.; Rongioletti, F. Widespread and Eruptive Comedonal Lesions with Alopecia. JAAD Case Rep. 2023, 31, 23–26. [Google Scholar] [CrossRef]
- Petersson, F. Pseudolymphomatous Folliculitis with Marked Lymphocytic Folliculo- and Focal Epidermotropism—Expanding the Morphologic Spectrum. Am. J. Dermatopathol. 2011, 33, 323–325. [Google Scholar] [CrossRef] [PubMed]
- Kakizaki, A.; Fujimura, T.; Numata, I.; Hashimoto, A.; Aiba, S. Pseudolymphomatous Folliculitis on the Nose. Case Rep. Dermatol. 2012, 4, 27–30. [Google Scholar] [CrossRef] [PubMed]
- Roque Quintana, B.; Peñate, Y.; Montenegro Dámaso, T. Pseudolymphomatous Folliculitis. Dermatol. Online J. 2020, 26, 10. [Google Scholar] [CrossRef]
- Willemze, R.; Cerroni, L.; Kempf, W.; Berti, E.; Facchetti, F.; Swerdlow, S.H.; Jaffe, E.S. The 2018 Update of the WHO-EORTC Classification for Primary Cutaneous Lymphomas. Blood 2019, 133, 1703–1714. [Google Scholar] [CrossRef]
- Silva, L.D.D.A.E.; Silva, E.V.; Silveira, H.A.; Silva, H.C.; Chahud, F.; León, J.E.; Mesquita, A.T.M. Intraoral Primary Syphilis Mimicking Lymphoproliferative Disorder. J. Cutan. Pathol. 2024, 51, 209–213. [Google Scholar] [CrossRef]
- Yamashita, M.; Fujii, Y.; Ozaki, K.; Urano, Y.; Iwasa, M.; Nakamura, S.; Fujii, S.; Abe, M.; Sato, Y.; Yoshino, T. Human Immunodeficiency Virus-Positive Secondary Syphilis Mimicking Cutaneous T-Cell Lymphoma. Diagn. Pathol. 2015, 10, 185. [Google Scholar] [CrossRef]
- Laungani, A.; McDonnell, J.; Bergfeld, W.; Sellheyer, K. Secondary Syphilis Presenting as Cutaneous T-Cell Lymphoma in an HIV-Positive Patient. J. Cutan. Pathol. 2005, 32, 69. [Google Scholar] [CrossRef]
- Maci, C.; Canetti, D.; Tassan Din, C.; Bruzzesi, E.; Lucente, M.F.; Badalucco Ciotta, F.; Candela, C.; Ponzoni, M.; Castagna, A.; Nozza, S. Malignant Syphilis Mimicking Lymphoma in HIV: A Challenging Case and a Review of Literature Focusing on the Role of HIV and Syphilis Coinfection. Microorganisms 2025, 13, 968. [Google Scholar] [CrossRef]
- Julius, K.; Schill, T.; Kempf, W.; Schön, M.P.; Mitteldorf, C. Disseminated Erythematous Nodules in a 39-year-old Man. J. Dtsch. Dermatol. Ges. 2025, 23, 246–249. [Google Scholar] [CrossRef]
- Stanek, G.; Strle, F. Lyme Borreliosis–from Tick Bite to Diagnosis and Treatment. FEMS Microbiol. Rev. 2018, 42, 233–258. [Google Scholar] [CrossRef]
- Moreno-Ramírez, D.; García-Escudero, A.; Ríos-Martín, J.J.; Herrera-Saval, A.; Camacho, F. Cutaneous Pseudolymphoma in Association with Molluscum Contagiosum in an Elderly Patient. J. Cutan. Pathol. 2003, 30, 473–475. [Google Scholar] [CrossRef]
- Espósito, A.C.C.; Jorge, M.F.S.; Marques, M.E.A.; Abbade, L.P.F. Milker’s Nodules: Classic Histological Findings. An. Bras. Dermatol. 2017, 92, 838–840. [Google Scholar] [CrossRef]
- Hoyt, B.; Bhawan, J. Histological Spectrum of Cutaneous Herpes Infections. Am. J. Dermatopathol. 2014, 36, 609–619. [Google Scholar] [CrossRef]
- Mitteldorf, C.; Geissinger, E.; Pleimes, M.; Schön, M.P.; Kempf, W. T-cell Pseudolymphoma in Recurrent Herpes Simplex Virus Infection. J. Cutan. Pathol. 2019, 46, 717–722. [Google Scholar] [CrossRef]
- Walton, S.; Bottomley, W.W.; Wyatt, E.H.; Bury, H.P.R. Pseudo T-Cell Lymphoma Due to Scabies in a Patient with Hodgkin’s Disease. Br. J. Dermatol. 1991, 124, 277–278. [Google Scholar] [CrossRef]
- Kataoka, Y.; Nakai, N.; Katoh, N. Histology Resembling Cutaneous T-Cell Lymphoma in Nodular Scabies: A Case Report. Indian J. Dermatol. 2016, 61, 125. [Google Scholar] [CrossRef]
- Rosman, I.S.; Hepper, D.M.; Lind, A.C.; Anadkat, M.J. Nevoid Hyperkeratosis of the Areola Misinterpreted as Mycosis Fungoides. J. Cutan. Pathol. 2012, 39, 545–548. [Google Scholar] [CrossRef]
- Baykal, C.; Bykbabani, N.; Kavak, A.; Alper, M. Nevoid Hyperkeratosis of the Nipple and Areola: A Distinct Entity. J. Am. Acad. Dermatol. 2002, 46, 414–418. [Google Scholar] [CrossRef]
- Roustan, G.; Yus, E.S.; Simón, A. Nevoid Hyperkeratosis of the Areola with Histopathological Features Mimicking Mycosis Fungoides. Eur. J. Dermatol. 2002, 12, 79–81. [Google Scholar]
- Kalajian, A.H.; Waldman, M.; Knable, A.L. Nodular Primary Localized Cutaneous Amyloidosis after Trauma: A Case Report and Discussion of the Rate of Progression to Systemic Amyloidosis. J. Am. Acad. Dermatol. 2007, 57, S26–S29. [Google Scholar] [CrossRef]









Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Published by MDPI on behalf of the European Society of Dermatopathology. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license.