The Functional Relevance of Diffusion Tensor Imaging in Patients with Degenerative Cervical Myelopathy

 , ,
, ,  ,
,
Abstract
:1. Introduction
2. Experimental Section
2.1. Participants
2.2. Diffusion Tensor Imaging (DTI) Acquisition and Analysis
2.3. Measurement of Dexterity and Hand Strength
2.4. Statistical Analysis
3. Results
3.1. Baseline Characteristics
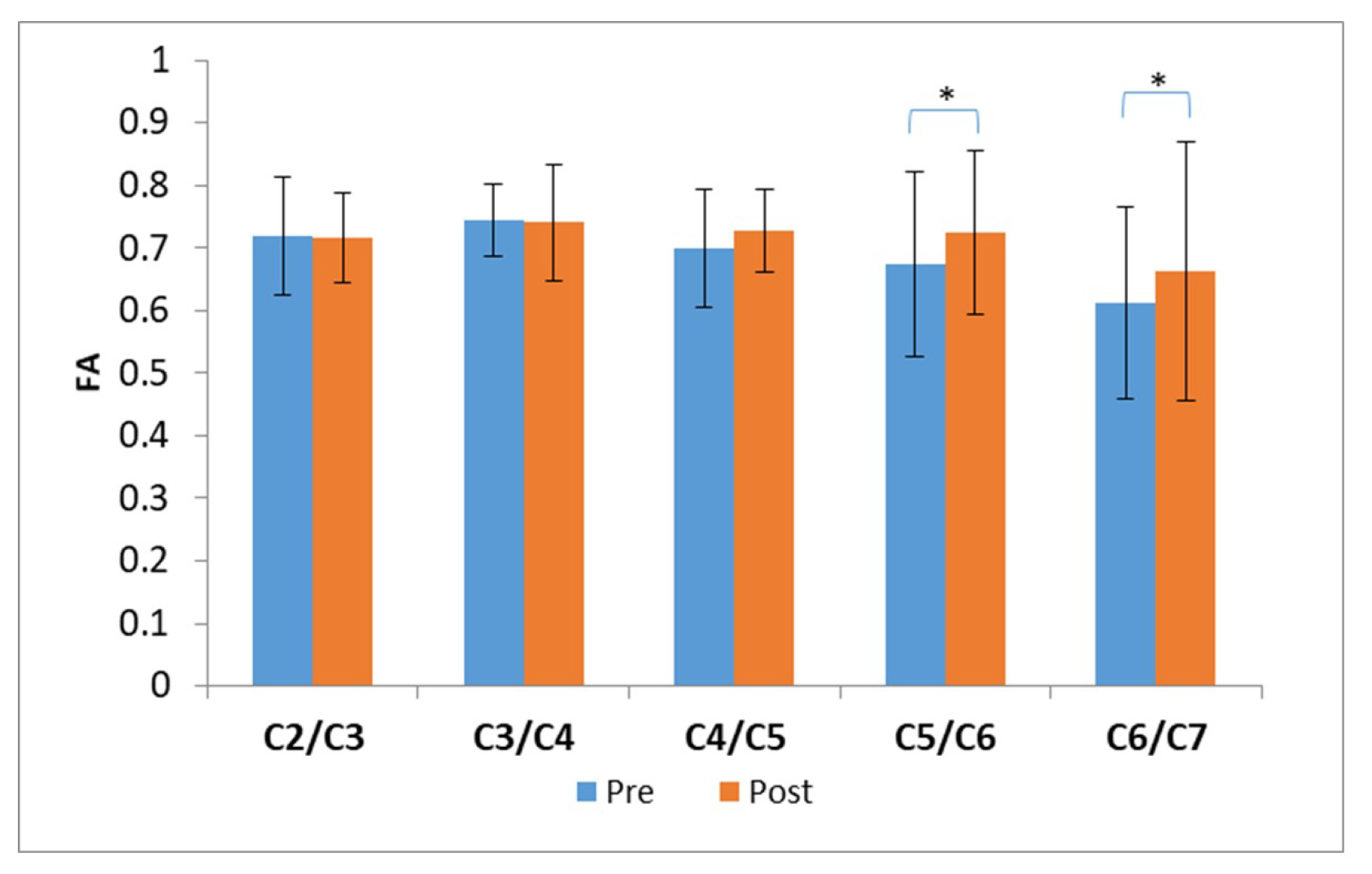
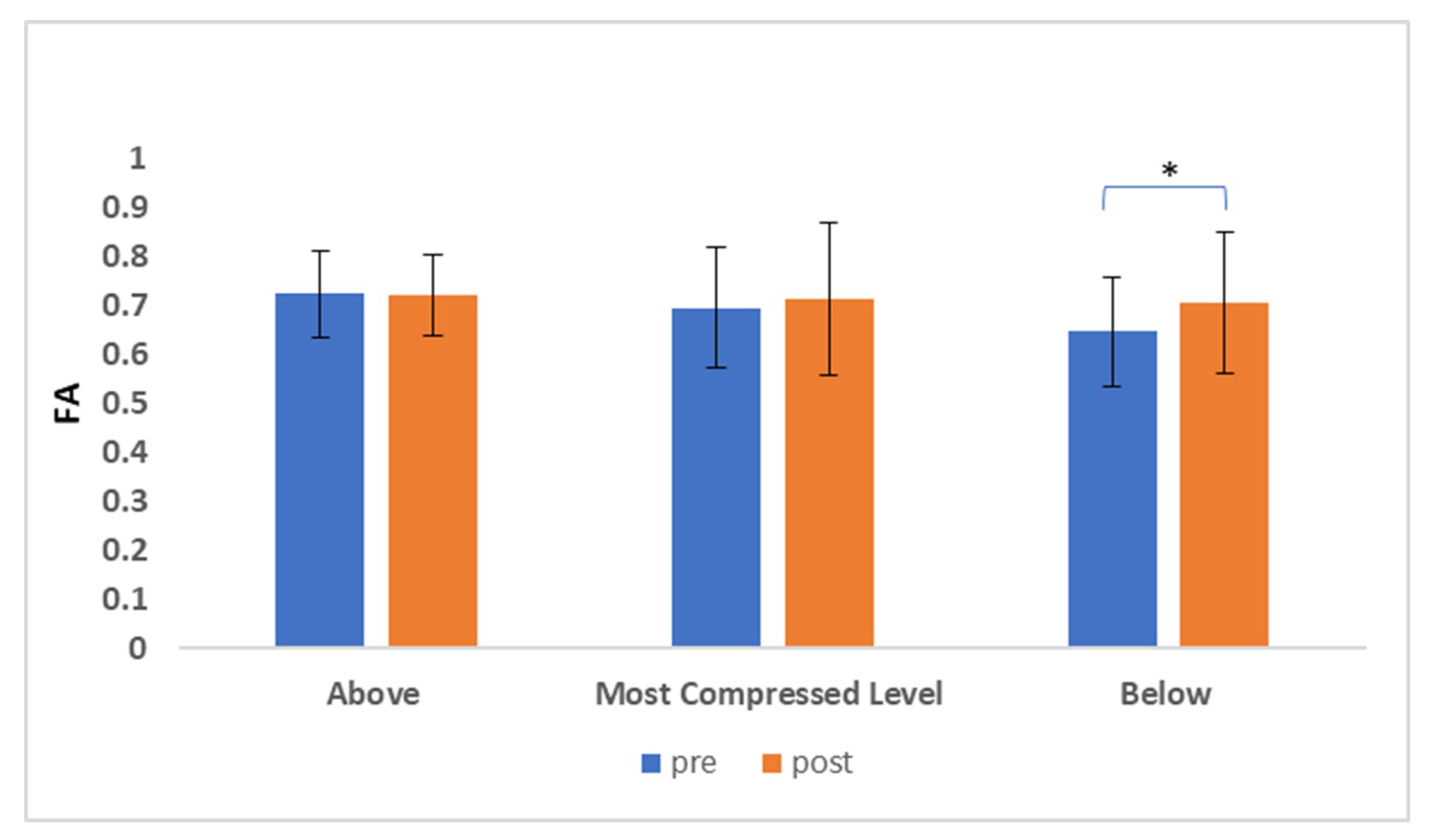
3.2. Diffusion Tensor Imaging (DTI)
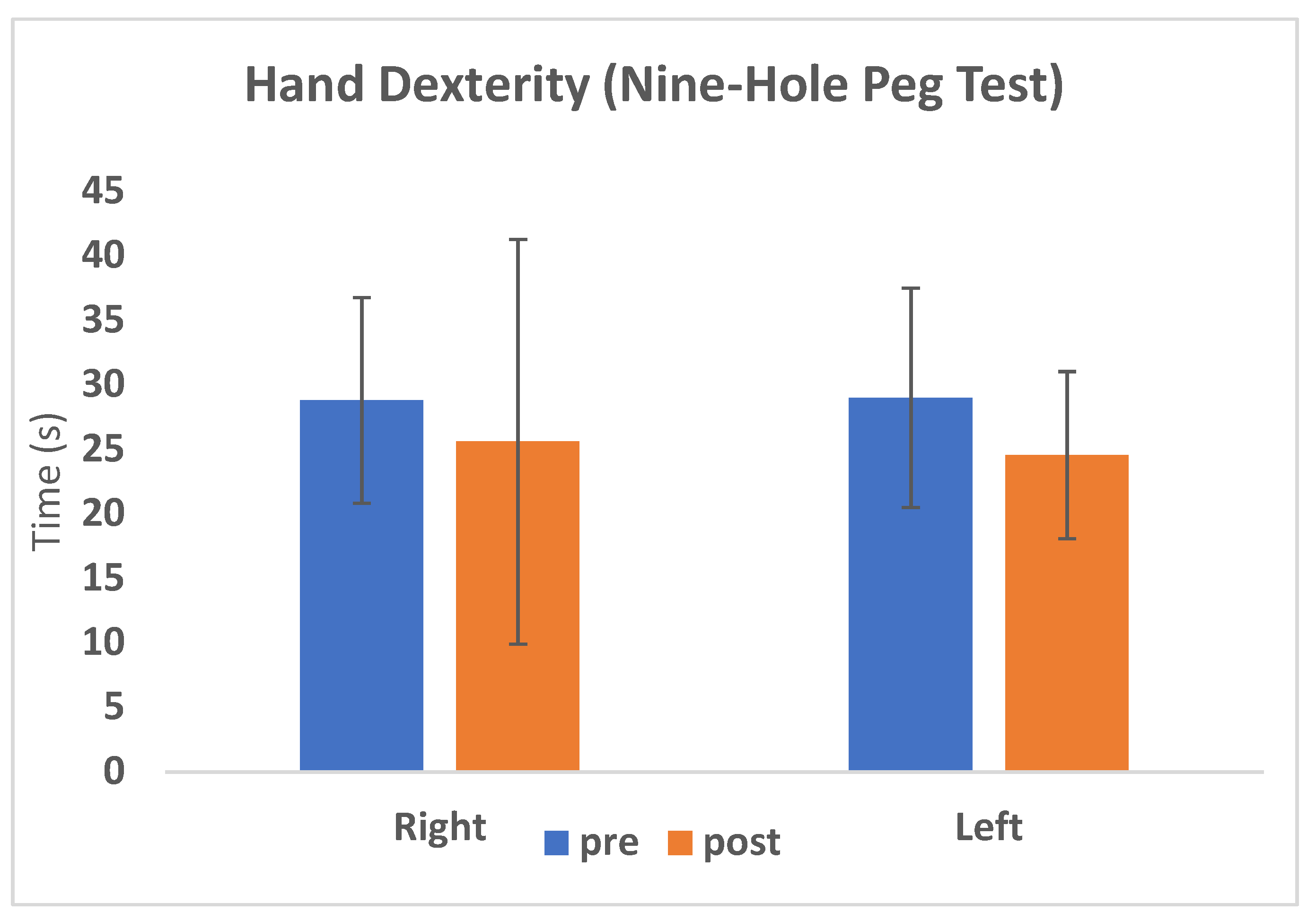
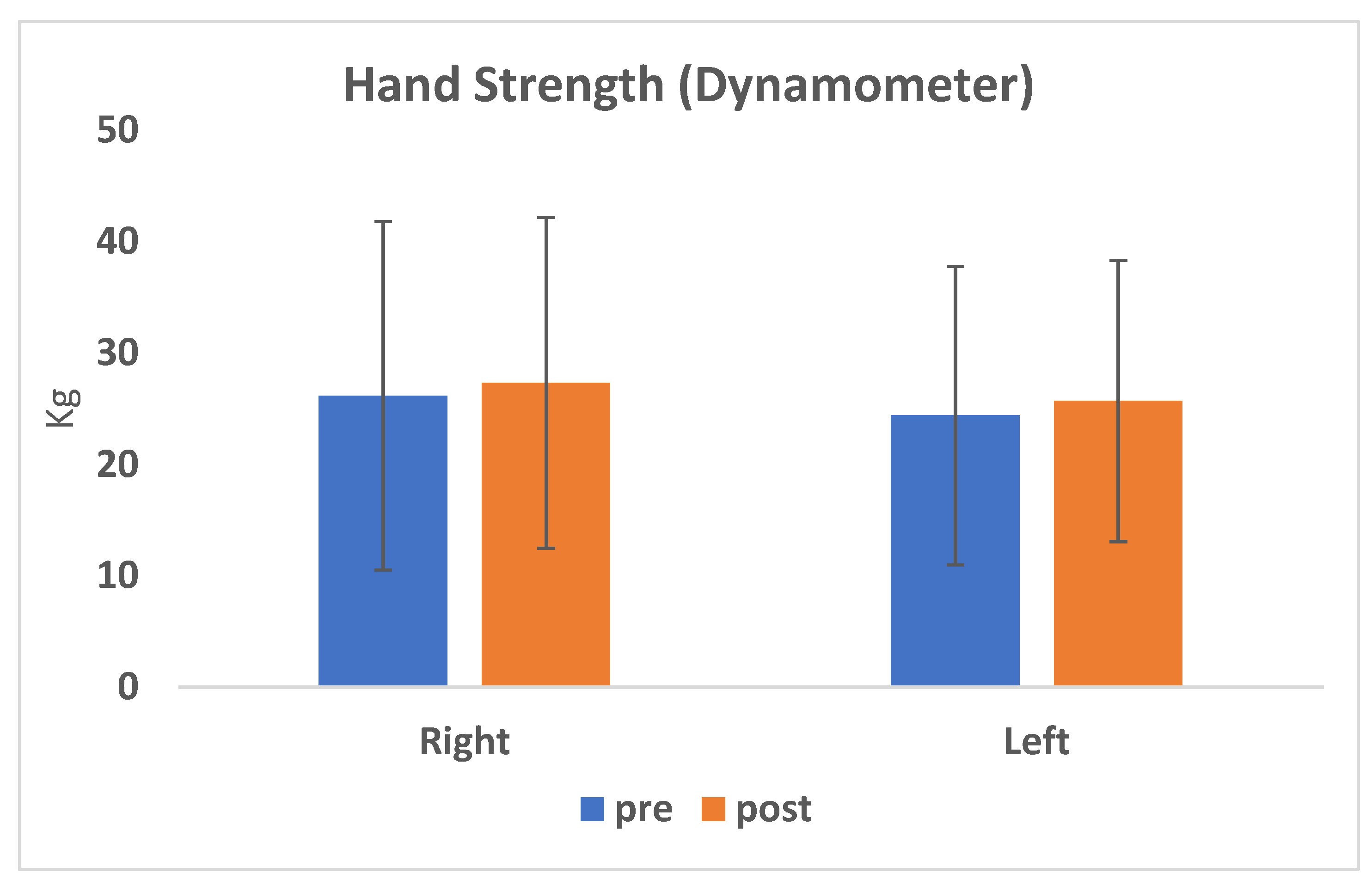
3.3. Dexterity and Hand Strength
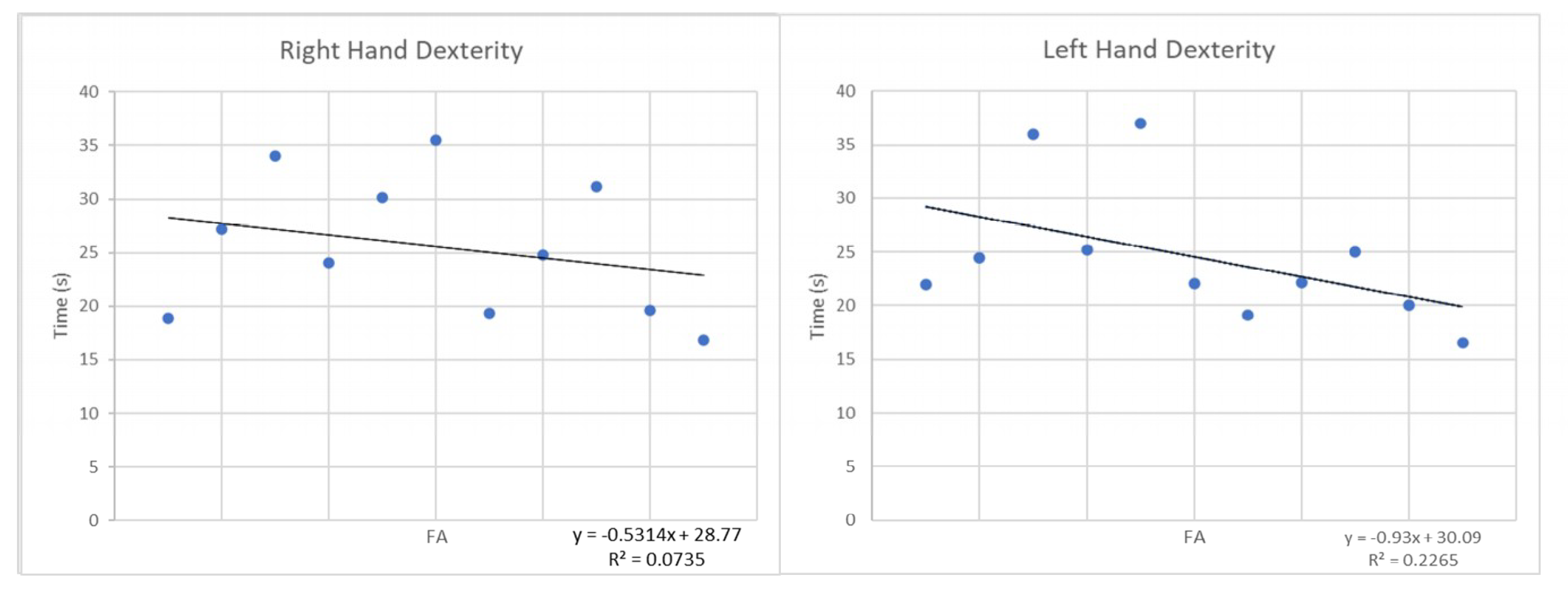
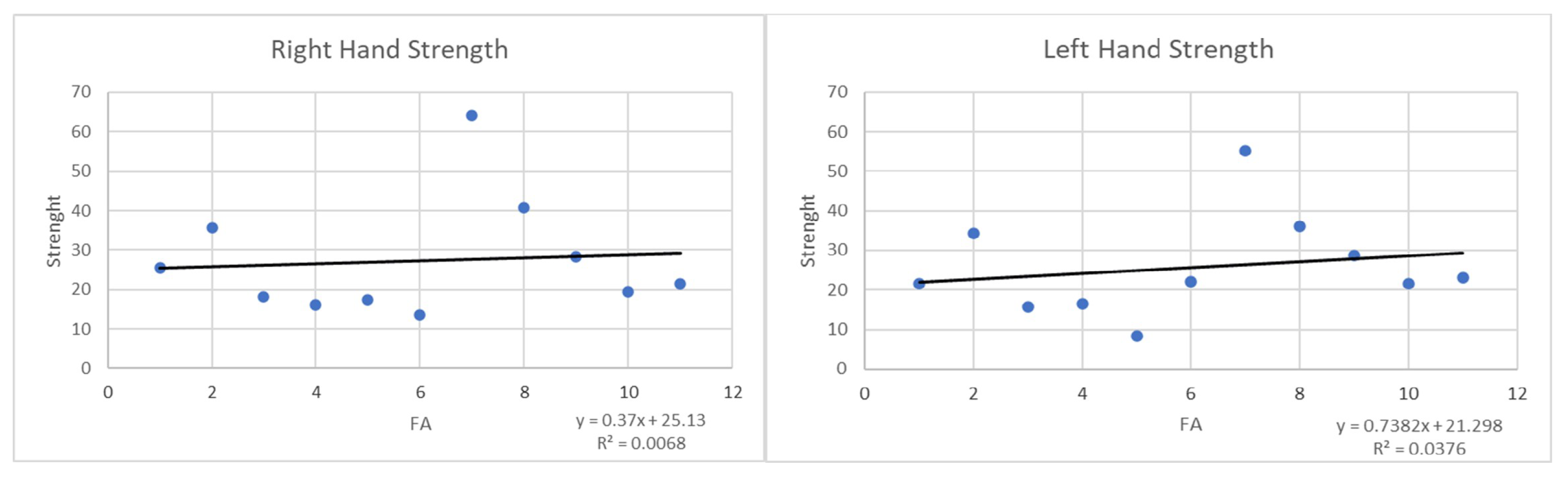
3.4. Correlation between the Postoperative FA Values and Strength and Hand Dexterity
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Wilson, J.R.; Tetreault, L.A.; Kim, J.; Shamji, M.F.; Harrop, J.S.; Mroz, T.; Cho, S.; Fehlings, M.G. State of the Art in Degenerative Cervical Myelopathy: An Update on Current Clinical Evidence. Neurosurgery 2017, 80, S33–S45. [Google Scholar] [CrossRef] [PubMed]
- Karadimas, S.K.; Gatzounis, G.; Fehlings, M.G. Pathobiology of cervical spondylotic myelopathy. Eur. Spine J. 2015, 24, 132–138. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fehlings, M.G.; Tetreault, L. The aging of the global population: The changing epidemiology of disease and spinal disorders. Neurosurgery 2015, 77, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Nouri, A.; Tetreault, L. Degenerative cervical myelopathy: Epidemiology, genetics and pathogenesis. Spine 2015, 40, 675–693. [Google Scholar] [CrossRef] [PubMed]
- Gurnam, V. Cervical Myelopathy: Pathophysiology, Diagnosis, and Management. Spine Res. 2017, 3, 2–12. [Google Scholar]
- Fujiyoshi, T.; Yamazaki, M. Static versus dynamic factors for the developmentof myelopathy in patients with cervical ossification of the posterior longitudinal ligament. J. Clin. Neurosci. 2010, 17, 320–324. [Google Scholar] [CrossRef]
- Fujiyoshi, T.; Yamazaki, M.; Okawa, A.; Kawabe, J.; Hayashi, K.; Endo, T.; Cho, S.; Fehlings, M.G. A Clinical Practice Guideline for the Management of Degenerative Cervical Myelopathy: Introduction, Rationale and Scope. Glob. Spine J. 2017, 7, 21–27. [Google Scholar]
- Alian, J.; Micev, M.D. Cervical Radiculophaty and Myelopathy: Presentations in the Hand. J. Hand Am. 2013, 38, 2478–2481. [Google Scholar]
- Ono, K.; Ebara, S.; Fuji, T.A.K.E.S.H.I.; Yonenobu, K.A.Z.U.O.; Fujiwara, K.E.I.J.U.; Yamashita, K.A.Z.U.O. Myelopathy hand: New clinical signs of cervical cord damage. J. Bone Jt. Surg. Br. 1987, 69, 215–219. [Google Scholar] [CrossRef] [Green Version]
- Hosono, N.; Makino, T.; Sakaura, H.; Mukai, Y.; Fuji, T.; Yoshikawa, H. Myelopathy hand: New evidence of the classical sign. Spine 2010, 35, 273–277. [Google Scholar] [CrossRef] [PubMed]
- Yukawa, Y.; Nakashima, H. Quantifiable tests for cervical myelopathy; 10-s grip and release test and 10-s step test: Standard values and aging variation from healthy volunteers. J. Orthop. Sci. 2013, 18, 509–513. [Google Scholar] [CrossRef]
- Nouri, A.; Martin, A.R. Magnetic resonance imaging assessment of degenerative cervical myelopathy: A review of structural changes and measurement techniques. Neurosurg. Focus 2016, 40, 5–12. [Google Scholar] [CrossRef] [PubMed]
- Cowley, P. Neuroimaging of Spinal Canal Stenosis. Magn. Reson. Imaging Clin. N. Am. 2016, 24, 523–539. [Google Scholar] [CrossRef] [PubMed]
- Tetreault, L.A.; Dettori, J.R. Systematic review of magnetic resonance imaging characteristics that affect treatment decision making and predict clinical outcome in patients with cervical spondylotic myelopathy. Spine 2013, 38, 89–110. [Google Scholar] [CrossRef] [PubMed]
- Karpova, A.; Arun, R. Do quantitative magnetic resonance imaging parameters correlate with the clinical presentation and functional outcomes after surgery in cervical spondylotic myelopathy? A prospective multicenter study. Spine 2014, 39, 1488–1497. [Google Scholar] [CrossRef] [PubMed]
- Li, F.; Chen, Z. A meta-analysis showing that high signal intensity on T2-weighted MRI is associated with poor prognosis for patients with cervical spondylotic myelopathy. J. Clin. Neurosci. 2011, 18, 1592–1595. [Google Scholar] [CrossRef] [PubMed]
- Nouri, A.; Martin, A.R. The relationship between MRI signal intensity changes, clinical presentation, and surgical outcome in degenerative cervical myelopathy: Analysis of a global cohort. Spine 2017, 42, 1851–1858. [Google Scholar] [CrossRef]
- Guan, X.; Fan, G. Diffusion tensor imaging studies of cervical spondylotic myelophaty: A systemic review and meta-analysis. PLoS ONE 2015, 10, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Song, T.; Chen, V.J. Diffusion tensor imaging in the cervical spinal cord. Eur. Spine J. 2011, 20, 422–428. [Google Scholar] [CrossRef] [Green Version]
- Dong, F.; Wu, F. A preliminary study of 3.0-T magnetic resonance diffusion tensor imaging in cervical spondylotic myelopathy. Eur. Spine J. 2018, 27, 1839–1845. [Google Scholar] [CrossRef]
- Chagawa, K.; Nishijima, S. Normal values of diffusion tensor magnetic resonance imaging parameters in the cervical spinal cord. Asian Spine J. 2015, 9, 541–547. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wei, L.F.; Wang, S.S. Analysis of the diffusion tensor imaging parameters of a normal cervical spinal cord in healthy population. J. Spinal Cord Med. 2017, 40, 338–345. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shen, C.; Xu, H. Value of conventional MRI and DTI parameters in predicting surgical outcome in patients with DCM. J. Back Musculoskelet. Rehabil. 2018, 31, 525–532. [Google Scholar] [CrossRef]
- Wang, K.; Chen, Z. Evaluation of DTI parameter ratio and diffusion tensor tractography grading in the diagnosis and prognosis prediction of cervical spondylotic myelopathy. Spine 2017, 42, 202–210. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.M.; Yoo, W.K. The functional relevance of diffusion tensor imaging in comparison to conventional MRI in patients with cervical compressive myelopathy. Skeletal Radiol. 2017. [Google Scholar] [CrossRef] [PubMed]
- Landi, A.; Innocenzi, G. Diagnostic potential of the diffusion tensor tractography with fractional anisotropy in the diagnosis and treatment of cervical spondylotic and posttraumatic myelopathy. Surg. Neurol. Int. 2016, 7, 705–707. [Google Scholar] [CrossRef] [Green Version]
- Tetreault, L.; Kopjar, B. The modified Japanese Orthopaedic Association scale: Establishing criteria for mild, moderate and severe impairment in patients with degenerative cervical myelopathy. Eur. Spine J. 2017, 26, 78–84. [Google Scholar] [CrossRef]
- Fedorov, A.; Beichel, R. 3D Slicer as an Image Computing Platform for the Quantitative Imaging Network. Magn. Reson. Imaging 2012, 30, 1323–1341. [Google Scholar] [CrossRef] [Green Version]
- Basser, P.J.; Mattiello, J.; LeBihan, D. MR diffusion tensor spectroscopy and imaging. Biophys. J. 1994, 66, 259–267. [Google Scholar] [CrossRef] [Green Version]
- Westin, C.F.; Maier, S.E. Processing and visualization for diffusion tensor MRI. Med. Image Anal. 2002, 6, 93–108. [Google Scholar] [CrossRef]
- Thurnher, M.M.; Mueller, M.C. Diffusion tensor MR imaging (DTI) metrics in the cervical spinal cord in asymptomatic HIV-positive patients. Neuroradiology 2011, 53, 585–592. [Google Scholar]
- Olindo, S.; Signate, A. Quantitative assessment of hand disability by the Nine-Hole-Peg test (9-HPT) in cervical spondyloticmyelophaty. J. Neurol. Neurosurg. Psychiatry 2008, 79, 965–967. [Google Scholar]
- Silberberg, N.; Kellor, M. Hand strenght and dexterity. Am. J. Occup. Ther. 1971, 25, 77–83. [Google Scholar]
- Martin, A.R.; De Leener, B.; Cohen-Adad, J.; Cadotte, D.W.; Nouri, A.; Wilson, J.R.; Tetreault, L.; Crawley, A.P.; Mikulis, D.J.; Ginsberg, H.; et al. Can microstructural MRI detect subclinical tissue injury in subjects with asymptomatic cervical spinal cord compression? A prospective cohort study. BMJ Open 2018, 8, e019809. [Google Scholar] [CrossRef] [PubMed]
- Clark, C.A.; Barker, G.J. Magnetic resonance diffusion imaging of the human cervical spinal cord in vivo. Magn. Reson. Med. 1999, 41, 1269–1273. [Google Scholar] [CrossRef] [Green Version]
- Rajasekaran, S.; Kanna, R. Efficacy of Diffusion Tensor Imaging indices in assessing postoperative neural recovery in cervical spondylotic myelopathy. Spine 2016, 42, 8–13. [Google Scholar] [CrossRef] [PubMed]
- Jones, J.G.; Cen, S.Y. Diffusion tensor imaging correlates with the clinical assessment of disease severity in cervical spondilotic myelopathy and predicts outcome following surgery. AJNR Am. J. Neuroradiol. 2013, 34, 471–478. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Severino, R.; Nouri, A.; Tessitore, E. Degenerative cervical myelopathy: How to Identify the best responders to surgery? J. Clin. Med. 2020, 9, 759. [Google Scholar] [CrossRef] [Green Version]
- Doita, M.; Sakai, H. Evaluation of impairment of hand function in patients with cervical myelophaty. J. Spinal Disord. 2006, 19, 276–280. [Google Scholar] [CrossRef]
- Murphy, R.K.; Sun, P. Fractional anisotropy to quantify cervical spondylotic myelophaty severity. J. Neurosurg. Sci. 2018, 62, 406–412. [Google Scholar]
- Smith, Z.A.; Barry, A.J.; Paliwal, M.; Hopkins, B.S.; Cantrell, D.; Dhaher, Y. Assessing hand dysfunction in cervical spondylotic myelopathy. PLoS ONE 2019, 14, e0223009. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Case | Gender | Surgical Level | Age | T2 Hyperintensity Signal | Most Compressed Level | mJOA Pre-op |
|---|---|---|---|---|---|---|
| 1 | F | 2 | 57 | + | C5-C6 | 13 |
| 2 | M | 2 | 66 | + | C3-C4 | 12 |
| 3 | F | 1 | 75 | - | C5-C6 | 11 |
| 4 | M | 2 | 55 | - | C5-C6 | 9 |
| 5 | F | 2 | 56 | + | C5-C6 | 16 |
| 6 | F | 1 | 59 | + | C3-C4 | 12 |
| 7 | M | 2 | 38 | + | C5-C6 | 11 |
| 8 | M | 1 | 56 | + | C5-C6 | 14 |
| 9 | M | 1 | 67 | + | C5-C6 | 14 |
| 10 | F | 2 | 62 | - | C4-C5 | 17 |
| 11 | F | 1 | 43 | - | C5-C6 | 17 |
| FA | C2/C3 | C3/C4 | C4/C5 | C5/C6 | C6/C7 |
|---|---|---|---|---|---|
| PRE | 0.72 | 0.74 | 0.70 | 0.67 | 0.61 |
| POST | 0.72 | 0.74 | 0.73 | 0.72 | 0.66 |
| Pre-Surgery (24–48 h) | Post-Surgery (Mean Follow-up 12 ± 2 Weeks) | |||||
|---|---|---|---|---|---|---|
| Case | Above FA | Most Compressed Level FA | Below FA | Above FA | Most Compressed Level FA | Below FA |
| 1. | 0.69 | 0.51 | 0.57 | 0.76 | 0.56 | 0.420 |
| 2. | 0.63 | 0.76 | 0.70 | 0.60 | 0.71 | 0.66 |
| 3. | 0.81 | 0.73 | 0.73 | 0.85 | 0.85 | 0.82 |
| 4. | 0.70 | 0.79 | 0.72 | 0.71 | 0.84 | 0.82 |
| 5. | 0.65 | 0.62 | 0.67 | 0.65 | 0.90 | 0.67 |
| 6. | 0.82 | 0.73 | 0.73 | 0.72 | 0.52 | 0.60 |
| 7. | 0.80 | 0.88 | 0.50 | 0.78 | 0.82 | 0.66 |
| 8. | 0.63 | 0.59 | 0.63 | 0.72 | 0.59 | 0.89 |
| 9. | 0.85 | 0.84 | 0.76 | 0.72 | 0.54 | 0.42 |
| 10. | 0.77 | 0.54 | 0.40 | 0.78 | 0.74 | 0.59 |
| 11. | 0.61 | 0.66 | 0.71 | 0.75 | 0.71 | 0.75 |
| Mean | 0.72 ± 0.08 | 0.69 ± 0.12 | 0.64 ± 0.11 | 0.72 ± 0.08 | 0.71 ± 0.15 | 0.70 ± 0.14 |
| Right Hand | Left Hand | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| NHPT | Hand Strength | NHPT | Hand Strength | |||||||||
| pre | post | % | pre | post | % | pre | post | % | pre | post | % | |
| 1 | 24.0 | 18.9 | −21.3 | 23.4 | 25.6 | 9.4 | 26.4 | 22.0 | −16.7 | 20.9 | 21.6 | 3.3 |
| 2 | 38.1 | 27.2 | −28.6 | 31.3 | 35.8 | 14.4 | 33.1 | 24.5 | −26.0 | 35.4 | 34.3 | −3.1 |
| 3 | 32.4 | 34.0 | 5.1 | 15.1 | 18.2 | 20.6 | 39.2 | 36.0 | −8.2 | 8.9 | 15.7 | 76.4 |
| 4 | 31.2 | 24.0 | −23.0 | 18.5 | 16.2 | −12.4 | 27.7 | 25.2 | −9.0 | 20.1 | 16.5 | −17.9 |
| 5 | 34.7 | 30.1 | −13.3 | 14.1 | 17.4 | 23.4 | 47.4 | 37.0 | −22.0 | 6.9 | 8.4 | 21.9 |
| 6 | 43.1 | 35.5 | −17.6 | 12.0 | 13.5 | 13.0 | 28.8 | 22.1 | −23.1 | 23.1 | 22.1 | −4.3 |
| 7 | 20.0 | 19.3 | −3.5 | 66.3 | 64.3 | −3.1 | 21.3 | 19.1 | −10.1 | 54.5 | 55.2 | 1.3 |
| 8 | 20.2 | 24.8 | 22.8 | 39.4 | 40.7 | 3.3 | 22.3 | 22.2 | −0.7 | 34.0 | 36.0 | 5.9 |
| 9 | 23.1 | 31.2 | 35.1 | 29.3 | 28.4 | −3.2 | 23.9 | 25.1 | 5.0 | 27.6 | 28.7 | 4.0 |
| 10 | 30.0 | 19.7 | −34.5 | 18.0 | 19.5 | 8.3 | 30.5 | 20.0 | −34.4 | 15.0 | 21.5 | 43.3 |
| 11 | 19.8 | 16.8 | −14.9 | 20.9 | 21.5 | 2.9 | 18.1 | 16.5 | −8.8 | 22.3 | 23.2 | 3.8 |
| Mean | 28.8 | 25.6 | −11.1 | 26.2 | 27.4 | 4.4 | 29.0 | 24.5 | −15.4 | 24.4 | 25.7 | 5.4 |
| p-value | 0.057 | 0.055 | 0.002 | 0.068 | ||||||||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
d’Avanzo, S.; Ciavarro, M.; Pavone, L.; Pasqua, G.; Ricciardi, F.; Bartolo, M.; Solari, D.; Somma, T.; de Divitiis, O.; Cappabianca, P.; et al. The Functional Relevance of Diffusion Tensor Imaging in Patients with Degenerative Cervical Myelopathy. J. Clin. Med. 2020, 9, 1828. https://doi.org/10.3390/jcm9061828
d’Avanzo S, Ciavarro M, Pavone L, Pasqua G, Ricciardi F, Bartolo M, Solari D, Somma T, de Divitiis O, Cappabianca P, et al. The Functional Relevance of Diffusion Tensor Imaging in Patients with Degenerative Cervical Myelopathy. Journal of Clinical Medicine. 2020; 9(6):1828. https://doi.org/10.3390/jcm9061828
Chicago/Turabian Styled’Avanzo, Stefania, Marco Ciavarro, Luigi Pavone, Gabriele Pasqua, Francesco Ricciardi, Marcello Bartolo, Domenico Solari, Teresa Somma, Oreste de Divitiis, Paolo Cappabianca, and et al. 2020. "The Functional Relevance of Diffusion Tensor Imaging in Patients with Degenerative Cervical Myelopathy" Journal of Clinical Medicine 9, no. 6: 1828. https://doi.org/10.3390/jcm9061828