

Body Weight Loss Efficiency in Overweight and Obese Adults in the Ketogenic Reduction Diet Program—Case Study




Abstract
:Featured Application
Abstract
1. Introduction
2. Materials and Methods
3. Results
3.1. Determining the Level of Nutrition and Eating Habits before Body Weight Reduction Program
3.1.1. Consumption of Different Food Groups
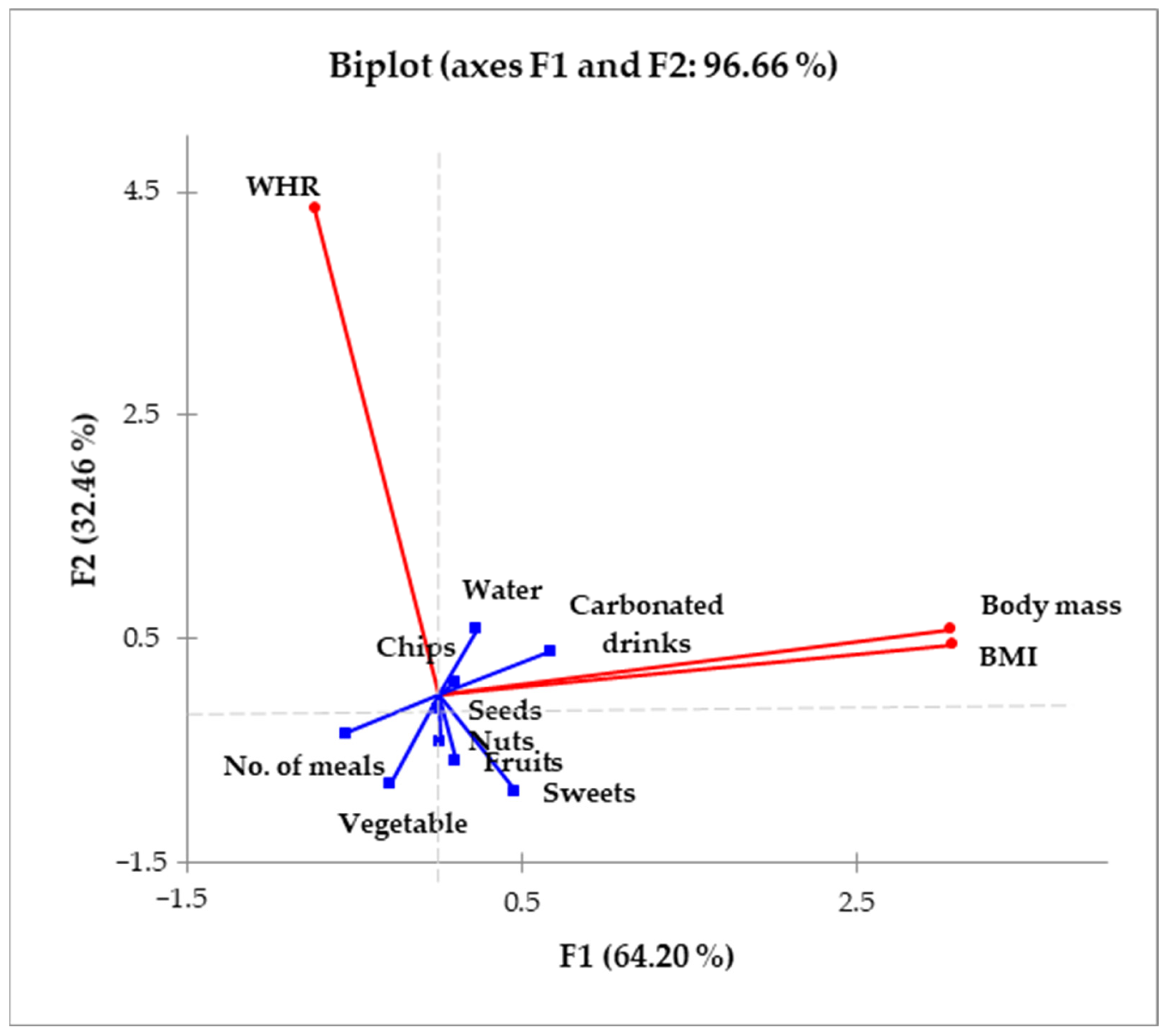
3.1.2. Body Mass Index as the Indicator of Level of Nourishment
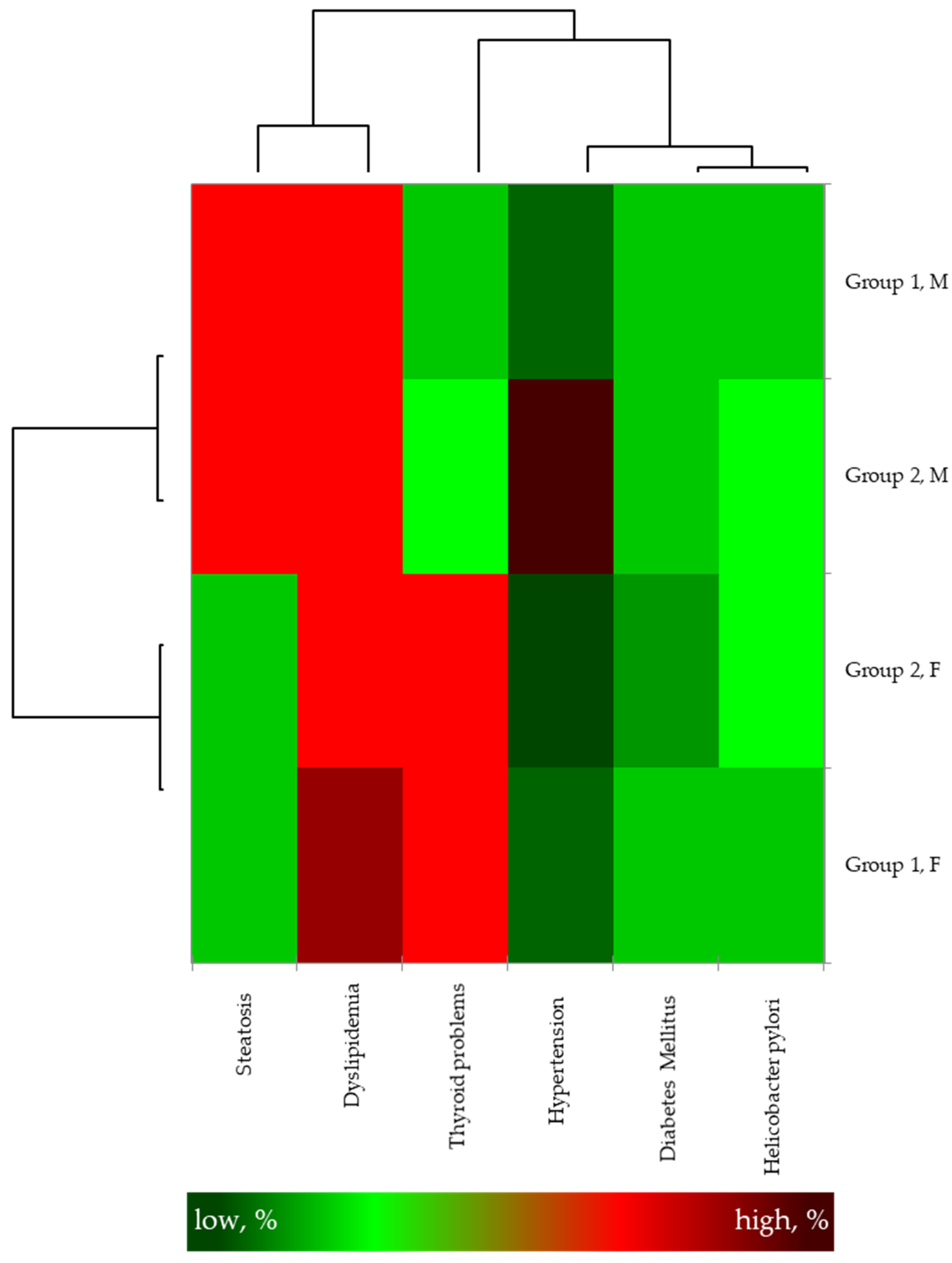
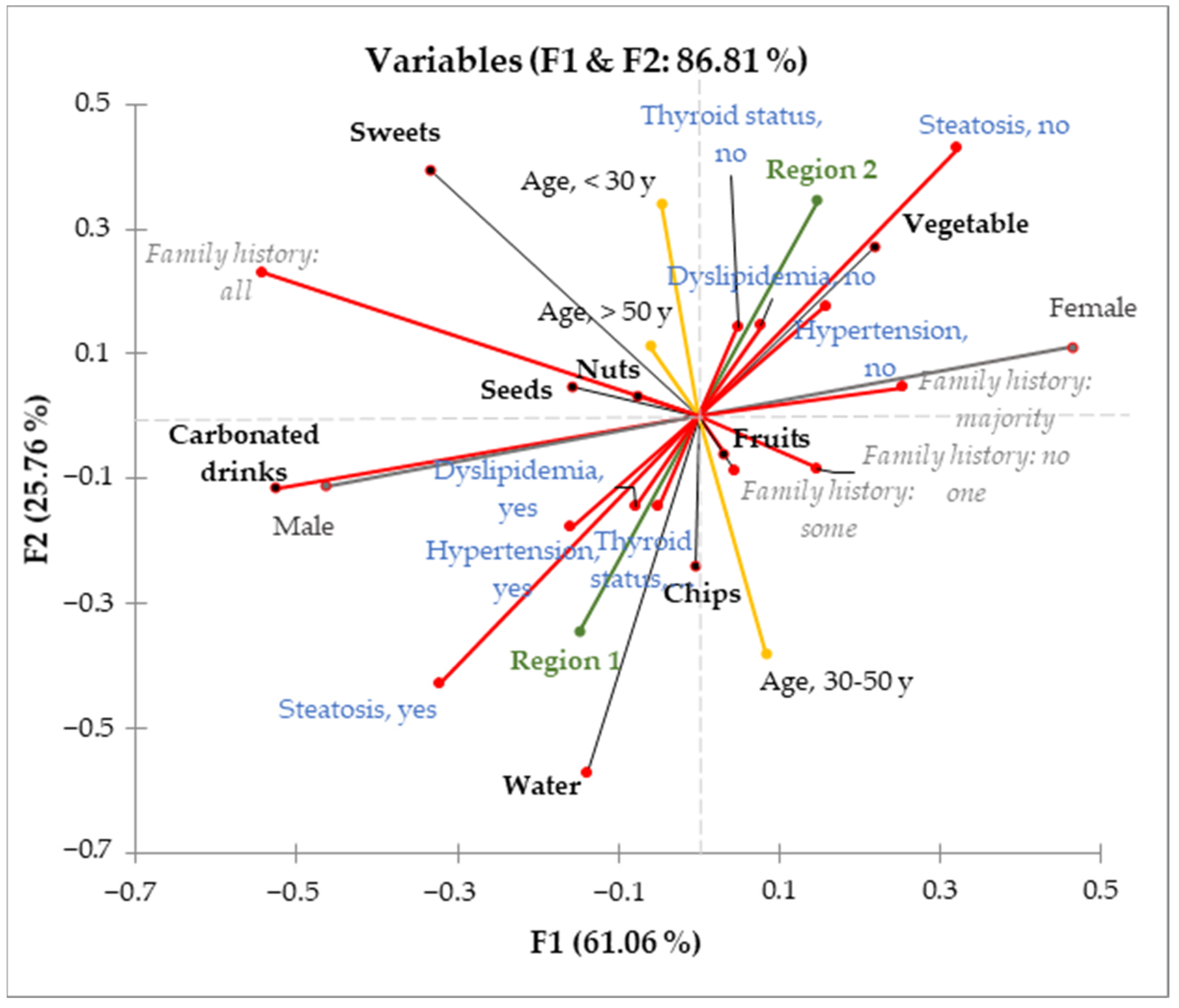
3.2. Relating Overweight/Obesity with Eating Habits
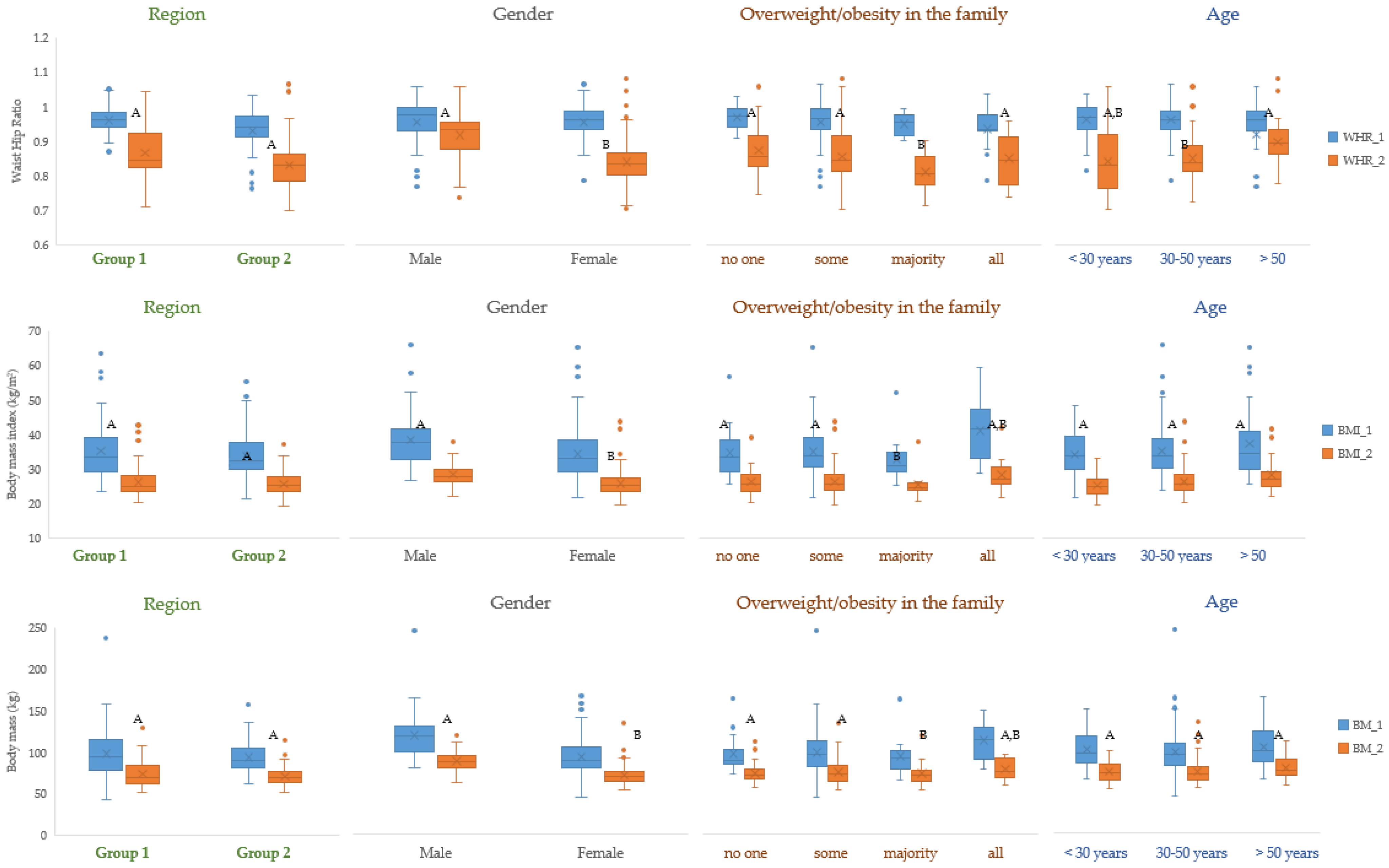
3.3. Successful Implementation of the Body Weight Reduction Program
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Frequency (% per Day) | ||||
|---|---|---|---|---|
| Drink Consumed per Day | Group 1 | Group 2 | ||
| Male | Female | Male | Female | |
| Carbonated drinks | ||||
| 0 L | 25.8 A,a | 39.1 B,a | 30.8 A,a | 32.9 A,a |
| <0.5 L | 12.9 A,a | 29.0 B,a | 38.5 A,b | 17.1 B,b |
| 0.5–1 L | 16.1 A,a | 20.3 A,a | 23.1 A,b | 25.7 A,a |
| 1–2 L | 38.7 A,a | 7.2 B,a | 23.1 A,b | 17.1 A,b |
| >2 L | 6.5 A,a | 4.3 A,a | 15.4 A,b | 7.1 B,a |
| Water | ||||
| 0 L | 74.2 A,a | 56.5 B,a | 75.0 A,a | 88.5 B,b |
| <0.5 L | 19.4 A,a | 33.3 B,a | 0.5 A,b | 2.3 A,b |
| 0.5–1 L | 6.5 A,a | 10.1 A,a | 16.7 A,b | 3.4 A,b |
| 1–2 L | 0.0 A,a | 0.0 A,a | 0.0 A,a | 2.3 A,b |
| >2 L | 0.0 A,a | 0.0 A,a | 8.3 A,b | 3.4 A,b |
| Family Incidence of Overweight/Obesity | Group 1 | Group 2 | Total | |||
|---|---|---|---|---|---|---|
| Male | Female | Male | Female | Male | Female | |
| No one | 16.1 A,a | 17.2 A,a | 7.7 A,b | 22.1 A,a | 11.9 | 19.7 |
| Some | 77.4 A,a | 73.4 A,a | 46.2 A,b | 65.1 A,b | 61.8 | 69.3 |
| Majority | 3.2 A,a | 1.6 A,a | 23.1 A,b | 5.8 B,a | 13.2 | 3.7 |
| All | 3.2 A,a | 7.8 A,a | 23.1 A,b | 7.0 B,a | 13.2 | 7.4 |
| Basic Information | Group 1 | Group 2 | ||
|---|---|---|---|---|
| Male (n = 31) | Female (n = 69) | Male (n = 13) | Female (n = 87) | |
| Body mass (kg) | 85.4 (60.3–107.7) | 68.1 (50.7–129.1) | 84.5 (68.0–114.8) | 68.5 (51.1–89.6) |
| Body mass index (kg/m2) | 27.8 (21.6–38.2) | 25.4 (20.0–42.6) | 27.9 (23.4–37.1) | 25.1 (19.2–33.7) |
| Consumed meals per day (No.) | 2.6 (1–5) | 2.8 (1–6) | 2.5 (2–4) | 2.5 (1–5) |
| Waist Circumference (cm) | 86.7 (72–114) | 80.2 (71–120) | 84.3 (66–102) | 79.1 (58–84) |
| Waist-to-hip ratio | 0.92 | 0.84 | 0.88 | 0.82 |
| (0.82–1.04) | (0.71–0.93) | (0.71–1) | (0.70–0.91) | |
References
- Meldrum, D.R.; Morris, M.A.; Gambone, J.C. Obesity pandemic: Causes, consequences, and solutions-but do we have the will? Fertil. Steril. 2017, 107, 833–839. [Google Scholar] [CrossRef]
- Ahluwalia, M.K. Chrononutrition—When We Eat Is of the Essence in Tackling obesity. Nutrients 2022, 14, 5080. [Google Scholar] [CrossRef]
- Di Rosa, C.; Lattanzi, G.; Taylor, S.F.; Manfrini, S.; Khazrai, Y.M. Very low calorie ketogenic diets in overweight and obesity treatment: Effects on anthropometric parameters, body composition, satiety, lipid profile and microbiota. Obes. Res. Clin. Pract. 2020, 14, 491–503. [Google Scholar] [CrossRef]
- Tham, K.W.; Abdul Ghani, R.; Cua, S.C.; Deerochanawong, C.; Fojas, M.; Hocking, S.; Lee, J.; Nam, T.Q.; Pathan, F.; Saboo, B.; et al. Obesity in South and Southeast Asia-A new consensus on care and management. Obes. Rev. 2023, 24, e13520. [Google Scholar] [CrossRef]
- Zavala, G.A.; Kolovos, S.; Chiarotto, A.; Chiarotto, A.; Bosmans, J.E.; Campos-Ponce, M.; Rosado, J.L.; Garcia, O.P. Association between obesity and depressive symptoms in Mexican population. Soc. Psychiatry Psychiatr. Epidemiol. 2018, 53, 639–646. [Google Scholar] [CrossRef]
- Berry, E.M. The Obesity Pandemic-Whose Responsibility? No Blame, No Shame, Not More of the Same. Front. Nutr. 2020, 7, 2. [Google Scholar] [CrossRef]
- Vasileva, L.V.; Marchev, A.S.; Georgiev, M.I. Causes and solutions to “globesity”: The new FA(S)T alarming global epidemic. Food Chem. Toxicol. 2018, 121, 173–193. [Google Scholar] [CrossRef]
- Markovikj, G.; Knights, V.; Kljusurić, J.G. Ketogenic Diet Applied in Weight Reduction of Overweight and Obese Individuals with Progress Prediction by Use of the Modified Wishnofsky Equation. Nutrients 2023, 15, 927. [Google Scholar] [CrossRef]
- Frank, J.W. Controlling the obesity pandemic: Geoffrey Rose revisited. Can. J. Public Health 2022, 113, 736–742. [Google Scholar] [CrossRef]
- Abarca-Gomez, L.; NCD Risk Factor Collaboration. Worldwide trends in body-mass index, underweight, overweight, and obesity from 1975 to 2016: A pooled analysis of 2416 population-based measurement studies in 128·9 million children, adolescents, and adults. Lancet 2017, 390, 2627–2642. [Google Scholar] [CrossRef]
- Pandita, A.; Sharma, D.; Pandita, D.; Pawar, S.; Tariq, M.; Kaul, A. Childhood obesity: Prevention is better than cure. Diabetes Metab. Syndr. Obes. 2016, 9, 83–89. [Google Scholar] [CrossRef]
- Flegal, K.M.; Ogden, C.L.; Fryar, C.; Afful, J.; Klein, R.; Huang, D. Comparisons of Self-Reported and Measured Height and Weight, BMI, and Obesity Prevalence from National Surveys: 1999–2016. Obesity 2019, 27, 1711–1719. [Google Scholar] [CrossRef] [PubMed]
- CDC. National Health and Nutrition Examination Survey 1999–2016 Survey Content Brochure. Available online: https://www.cdc.gov/nchs/nhanes/index.htm (accessed on 7 June 2023).
- CDC. National Center for Health Statistics- National Health Intervju Survey. Available online: https://www.cdc.gov/nchs/nhis/index.htm (accessed on 7 June 2023).
- CDC. Behavioral Risk Factor Surveillance System. Available online: https://www.cdc.gov/brfss/index.html (accessed on 7 June 2023).
- Contreras, R.E.; Schriever, S.C.; Pfluger, P.T. Physiological and Epigenetic Features of Yoyo Dieting and Weight Control. Front. Genet. 2019, 10, 1015. [Google Scholar] [CrossRef]
- Drabińska, N.; Wiczkowski, W.; Piskuła, M.K. Recent advances in the application of a ketogenic diet for obesity management. Trends Food Sci. Technol. 2021, 110, 28–38. [Google Scholar] [CrossRef]
- Dowis, K.; Banga, S. The Potential Health Benefits of the Ketogenic Diet: A Narrative Review. Nutrients 2021, 13, 1654. [Google Scholar] [CrossRef] [PubMed]
- Knights, V.; Kolak, M.; Markovikj, G.; Gajdoš Kljusurić, J. Modeling and Optimization with Artificial Intelligence in Nutrition. Appl. Sci. 2023, 13, 7835. [Google Scholar] [CrossRef]
- Papadaki, A.; Linardakis, M.; Plada, M.; Larsen, T.M.; van Baak, M.A.; Lindroos, A.K.; Pfeiffer, A.F.; Martinez, J.A.; Handjieva-Darlenska, T.; Kunešová, M.; et al. A multicentre weight loss study using a low-calorie diet over 8 weeks: Regional differences in efficacy across eight European cities. Swiss Med. Wkly. 2013, 143, w13721. [Google Scholar] [CrossRef]
- Sreenivas, S. Keto Diet for Beginners—Nourish byWebMD. Available online: https://www.webmd.com/diet/keto-diet-forbeginners (accessed on 4 July 2022).
- Maltarić, M.; Ruščić, P.; Kolak, M.; Bender, D.V.; Kolarić, B.; Ćorić, T.; Hoejskov, P.S.; Bošnir, J.; Kljusurić, J.G. Adherence to the Mediterranean Diet Related to the Health Related and Well-Being Outcomes of European Mature Adults and Elderly, with an Additional Reference to Croatia. Int. J. Environ. Res. Public Health 2023, 20, 4893. [Google Scholar] [CrossRef]
- Fatsecret. Green Peppers—Nutrition Facts. Available online: https://www.fatsecret.com/calories-nutrition/usda/green-peppers (accessed on 30 August 2023).
- Fatsecret. Hot & Sweet Peppers Stuffed with Cheese—Nutrition Facts. Available online: https://www.eatthismuch.com/food/nutrition/hot-sweet-peppers-stuffed-with-cheese,2508247/ (accessed on 30 August 2023).
- Dodevska, M.; Kukic Markovic, J.; Sofrenic, I.; Tesevic, V.; Jankovic, M.; Djordjevic, B.; Ivanovic, N.D. Similarities and differences in the nutritional composition of nuts and seeds in Serbia. Front. Nutr. 2022, 9, 1003125. [Google Scholar] [CrossRef] [PubMed]
- Weir, C.B.; Jan, A. BMI Classification Percentile and Cut Off Points. [Updated 2023 Jun 26]. Available online: https://www.ncbi.nlm.nih.gov/books/NBK541070/ (accessed on 16 August 2023).
- Maraschim, J.; Honicky, M.; Moreno, Y.M.F.; Hinnig, P.d.F.; Cardoso, S.M.; Back, I.d.C.; Vieira, F.G.K. Consumption and Breakfast Patterns in Children and Adolescents with Congenital Heart Disease. Int. J. Environ. Res. Public Health 2023, 20, 5146. [Google Scholar] [CrossRef] [PubMed]
- Addas, A. Understanding the Relationship between Urban Biophysical Composition and Land Surface Temperature in a Hot Desert Megacity (Saudi Arabia). Int. J. Environ. Res. Public Health 2023, 20, 5025. [Google Scholar] [CrossRef]
- Plura, J.; Vykydal, D.; Tošenovský, F.; Klaput, P. Graphical Tools for Increasing the Effectiveness of Gage Repeatability and Reproducibility Analysis. Process. 2023, 11, 1. [Google Scholar] [CrossRef]
- Fiore, G.; Pascuzzi, M.C.; Di Profio, E.; Corsello, A.; Agostinelli, M.; La Mendola, A.; Milanta, C.; Campoy, C.; Calcaterra, V.; Zuccotti, G.; et al. Bioactive compounds in childhood obesity and associated metabolic complications: Current evidence, controversies and perspectives. Pharmacol. Res. 2023, 187, 106599. [Google Scholar] [CrossRef] [PubMed]
- Buckley, J.P.; Kim, H.; Wong, E.; Rebholz, C.M. Ultra-processed food consumption and exposure to phthalates and bisphenols in the US National Health and Nutrition Examination Survey, 2013–2014. Environ. Int. 2019, 131, 105057. [Google Scholar] [CrossRef] [PubMed]
- Anderson, B.; Rafferty, A.P.; Lyon-Callo, S.; Fussman, C.; Imes, G. Fast-food consumption and obesity among Michigan adults. Prev. Chronic Dis. 2011, 8, A71. [Google Scholar]
- Vetrani, C.; Di Nisio, A.; Paschou, S.A.; Barrea, L.; Muscogiuri, G.; Graziadio, C.; Savastano, S.; Colao, A.; on behalf of the Obesity Programs of Nutrition, Education, Research and Assessment (OPERA) Group. From Gut Microbiota through Low-Grade Inflammation to Obesity: Key Players and Potential Targets. Nutrients 2022, 14, 2103. [Google Scholar] [CrossRef]
- Xu, Y.-S.; Liu, X.-J.; Liu, X.-X.; Chen, D.; Wang, M.-M.; Jiang, X.; Xiong, Z.-F. The Roles of the Gut Microbiota and Chronic Low-Grade Inflammation in Older Adults with Frailty. Front. Cell. Infect. Microbiol. 2021, 11, 675414. [Google Scholar] [CrossRef]
- Cheng, Z.; Zheng, L.; Almeida, F.A. Epigenetic reprogramming in metabolic disorders: Nutritional factors and beyond. J. Nutr. Biochem. 2018, 54, 1–10. [Google Scholar] [CrossRef]
- González-Muniesa, P.; Mártinez-González, M.A.; Hu, F.B.; Després, J.P.; Matsuzawa, Y.; Loos, R.J.F.; Moreno, L.A.; Bray, G.A.; Martinez, J.A. Obesity. Nat. Rev. Dis. Prim. 2017, 3, 17034. [Google Scholar] [CrossRef]
- Stelmach-Mardas, M.; Rodacki, T.; Dobrowolska-Iwanek, J.; Brzozowska, A.; Walkowiak, J.; Wojtanowska-Krosniak, A.; Zagrodzki, P.; Bechthold, A.; Mardas, M.; Boeing, H. Link between Food Energy Density and Body Weight Changes in Obese Adults. Nutrients 2016, 8, 229. [Google Scholar] [CrossRef]
- Tristan Asensi, M.; Napoletano, A.; Sofi, F.; Dinu, M. Low-Grade Inflammation and Ultra-Processed Foods Consumption: A Review. Nutrients 2023, 15, 1546. [Google Scholar] [CrossRef]
- Wu, E.; Ni, J.; Zhou, W.; You, L.; Tao, L.; Xie, T. Consumption of fruits, vegetables, and legumes are associated with overweight/obesity in the middle- and old-aged Chongqing residents: A case-control study. Medicine 2022, 101, e29749. [Google Scholar] [CrossRef] [PubMed]
- Nour, M.; Lutze, S.A.; Grech, A.; Allman-Farinelli, M. The Relationship between Vegetable Intake and Weight Outcomes: A Systematic Review of Cohort Studies. Nutrients 2018, 10, 1626. [Google Scholar] [CrossRef] [PubMed]
- Kelly, R.K.; Calhoun, J.; Hanus, A.; Payne-Foster, P.; Stout, R.; Sherman, B.W. Increased dietary fiber is associated with weight loss among Full Plate Living program participants. Front. Nutr. 2023, 10, 1110748. [Google Scholar] [CrossRef]
- Jorge, T.; Sousa, S.; do Carmo, I.; Lunet, N.; Padrão, P. Accuracy of Assessing Weight Status in Adults by Structured Observation. Appl. Sci. 2023, 13, 8185. [Google Scholar] [CrossRef]
- Pedrianes-Martin, P.B.; Perez-Valera, M.; Morales-Alamo, D.; Martin-Rincon, M.; Perez-Suarez, I.; Serrano-Sanchez, J.A.; Gonzalez-Henriquez, J.J.; Galvan-Alvarez, V.; Acosta, C.; Curtelin, D.; et al. Resting metabolic rate is increased in hypertensive patients with overweight or obesity: Potential mechanisms. Scand. J. Med. Sci. Sport. 2021, 31, 1461–1470. [Google Scholar] [CrossRef]
- Baradaran, A.; Dehghanbanadaki, H.; Naderpour, S.; Pirkashani, L.M.; Rajabi, A.; Rashti, R.; Riahifar, S.; Moradi, Y. The association between Helicobacter pylori and obesity: A systematic review and meta-analysis of case–control studies. Clin. Diabetes Endocrinol. 2021, 7, 15. [Google Scholar] [CrossRef]
- Crane, M.M.; Jeffery, R.W.; Sherwood, N.E. Exploring Gender Differences in a Randomized Trial of Weight Loss Maintenance. Am. J. Men’s Health 2017, 11, 369–375. [Google Scholar] [CrossRef]
- Kim, J.Y. Optimal Diet Strategies for Weight Loss and Weight Loss Maintenance. J. Obes. Metab. Syndr. 2021, 30, 20–31. [Google Scholar] [CrossRef]
- Harvard Health Publishing. Should you Try the Keto Diet? Available online: https://www.health.harvard.edu/staying-healthy/should-you-try-the-keto-diet (accessed on 18 September 2023).
- Batch, J.T.; Lamsal, S.P.; Adkins, M.; Sultan, S.; Ramirez, M.N. Advantages and Disadvantages of the Ketogenic Diet: A Review Article. Cureus 2020, 12, e9639. [Google Scholar] [CrossRef]
- Clark, J.E. Diet, exercise or diet with exercise: Comparing the effectiveness of treatment options for weight-loss and changes in fitness for adults (18–65 years old) who are overfat, or obese; systematic review and meta-analysis. J. Diabetes Metab. Disord. 2015, 14, 31, Erratum in J. Diabetes Metab. Disord. 2015, 14, 73. [Google Scholar] [CrossRef] [PubMed]
- Gerić, M.; Matković, K.; Gajski, G.; Rumbak, I.; Štancl, P.; Karlić, R.; Bituh, M. Adherence to Mediterranean Diet in Croatia: Lessons Learned Today for a Brighter Tomorrow. Nutrients 2022, 14, 3725. [Google Scholar] [CrossRef] [PubMed]
- Ayele, G.M.; Atalay, R.T.; Mamo, R.T.; Hussien, S.; Fissha, A.; Michael, M.B.; Nigussie, B.G.; Behailu, A. Is Losing Weight Worth Losing Your Kidney: Keto Diet Resulting in Renal Failure. Cureus 2023, 15, e36546. [Google Scholar] [CrossRef] [PubMed]
- Gomez-Arbelaez, D.; Bellido, D.; Castro, A.I.; Ordonez-Mayan, L.; Carreira, J.; Galban, C.; Martinez-Olmos, A.A.; Crujeiras, A.B.; Sajoux, I.; Casenueva, F.F. Body composition changes after very-low-calorie ketogenic diet in obesity evaluated by 3 standardized methods. J. Clin. Endocrinol. Metab. 2017, 102, 488–498. [Google Scholar] [CrossRef]
- Gomez-Arbelaez, D.; Crujeiras, A.B.; Castro, A.I.; Goday, A.; Mas-Lorenzo, A.; Bellon, A.; Tejera, C.; Bellido, D.; Galban, C.; Sajoux, I.; et al. Acid–base safety during the course of a very low-calorie-ketogenic diet. Endocrine 2017, 58, 81–90. [Google Scholar] [CrossRef]

| Basic Information | Group 1 | Group 2 | ||
|---|---|---|---|---|
| Male (n = 31) | Female (n = 69) | Male (n = 13) | Female (n = 87) | |
| Age (years) | 35.3 (18–569) | 37.6 (18–68) | 41.8 (18–57) | 38 (18–67) |
| Body mass (kg) | 103.3 (60.3–237) | 78.8 (50.7–152.5) | 108.4 (85.1–157.6) | 91.3 (62.5–161.2) |
| Body height (m) | 1.76 (1.62–1.92) | 1.64 (1.47–1.84) | 1.74 (1.55–1.85) | 1.65 (1.52–1.83) |
| Body mass index (kg/m2) | 38.3 (26.3–64.3) | 33.6 (25.4–63.5) | 35 (28–49) | 32.8 (25.1–54.5) |
| Consumed meals per day (No.) | 2.5 (1–4) | 2.1 (1–4) | 2.5 (2–4) | 2.6 (1–5) |
| Waist Circumference (cm) | 110.7 (80–164) | 100.9 (75–162) | 105.4 (77–138) | 101.3 (66–166) |
| Waist-to-hip ratio | 0.97 | 0.95 | 0.94 | 0.95 |
| (0.91–1.05) | (0.89–1.05) | (0.85–1) | (0.85–1.03) | |
| Controlled Dietary Parameters | Content |
|---|---|
| Energy, kJ | 6280 ± 210 |
| Proteins #, g | 136 ± 5.6 |
| Fats #, g | 95 ± 4.3 |
| Carbohydrates #, g | 360 ± 1.9 |
| Vitamins | |
| Thiamine (vit. B1), mg | 1.4 ± 0.02 |
| Riboflavin (vit. B2), mg | 1.6 ± 0.03 |
| Niacin (vit. B3), mg NE | 18 ± 0.8 |
| Pantothenic acid (vit. B5), mg | 6 ± 0.3 |
| Vitamin B6, mg | 2 ± 0.08 |
| Biotin (vit. B7), μg | 150 ± 6.2 |
| Folic acid (vit. B9), μg | 200 ± 10.4 |
| Vitamin B12, μg | 1 ± 0.2 |
| Vitamin C, mg | 60 ± 2.7 |
| Vitamin D, μg | 5 ± 0.25 |
| Vitamin E, mg | 7.4 ± 0.4 |
| Vitamin K, μg | 30 ± 1.1 |
| Vitamin A, μg RE | 800 ± 32.7 |
| Minerals | |
| Calcium, mg | 360 ± 17.8 |
| Chromium, μg | 25 ± 0.9 |
| Cupper, mg | 1 ± 0.01 |
| Iodine, μg | 100 ± 4.2 |
| Iron, mg | 8 ± 2.1 |
| Magnesium, mg | 360 ± 15.9 |
| Manganese, mg | 1 ± 0.03 |
| Molybdenum, μg | 25 ± 1.1 |
| Potassium, mg | 1200 ± 48.3 |
| Selenium, μg | 25 ± 1.3 |
| Sodium, mg | 1200 ± 44.2 |
| Zinc, mg | 10 ± 0.9 |
| polyunsaturated fats | |
| Omega-3, mg | 1000 ± 30 |
| Amount of Daily Consumed Foods | Frequency (% per Day or per Week #) | |||
|---|---|---|---|---|
| Group 1 | Group 2 | |||
| Male | Female | Male | Female | |
| Sweets | ||||
| 0 g | 9.7 A,a | 5.8 B,a | 0.0 A,b | 0.0 A,b |
| <50 g | 38.7 A,a | 26.1 B,a | 25.0 A,b | 18.2 B,b |
| 50–100 g | 16.1 A,a | 23.2 A,a | 8.3 A,b | 28.6 B,a |
| 101–200 g | 16.1 A,a | 37.7 B,a | 0.0 A,b | 23.4 B,b |
| >200 g | 19.4 A,a | 7.2 B,a | 66.7 A,b | 29.9 B,b |
| Chips | ||||
| 0 g | 35.5 A,a | 18.8 B,a | 25.0 A,b | 29.9 A,a |
| <50 g | 25.8 A,a | 33.3 B,a | 16.7 A,b | 26.0 B,b |
| 50–100 g | 19.4 A,a | 30.4 B,a | 41.7 A,b | 35.1 B,a |
| 101–200 g | 9.7 A,a | 13.0 A,a | 8.3 A,a | 6.5 A,b |
| >200 g | 9.7 A,a | 4.3 A,a | 8.3 A,a | 2.6 B,a |
| Vegetables | ||||
| 0 g | 12.9 A,a | 10.1 A,a | 0.0 A,b | 4.0 B,a |
| <500 g | 87.1 A,a | 88.4 A,a | 0.0 A,b | 12.0 B,b |
| 500–1000 g | 0.0 A,a | 1.4 A,a | 91.7 A,b | 70.7 B,b |
| 1001–1500 g | 0.0 A,a | 0.0 A,a | 0.0 A,a | 4.0 B,b |
| >1500 g | 0.0 A,a | 0.0 A,a | 8.3 A,b | 9.3 A,b |
| Fruits | ||||
| 0 g | 19.4 A,a | 17.4 A,a | 0.0 A,b | 2.6 A,b |
| <500 g | 54.8 A,a | 49.3 A,a | 36.4 A,b | 46.1 B,a |
| 500–1000 g | 16.1 A,a | 18.8 A,a | 36.4 A,b | 31.6 A,b |
| 1001–1500 g | 6.5 A,a | 8.7 A,a | 18.2 A,b | 11.8 A,a |
| >1500 g | 3.2 A,a | 5.8 A,a | 9.1 A,b | 7.9 A,a |
| Nuts # | ||||
| 0 g | 22.6 A,a | 26.1 A,a | 45.5 A,b | 16.2 B,b |
| <500 g | 32.3 A,a | 31.9 A,a | 9.1 A,b | 29.7 B,a |
| 500–1000 g | 9.7 A,a | 13.0 A,a | 36.4 A,b | 39.2 A,b |
| 1001–1500 g | 22.6 A,a | 26.1 A,a | 0.0 A,b | 9.5 B,b |
| 200–500 g | 12.9 A,a | 2.9 B,a | 9.1 A,a | 5.4 A,a |
| >500 g | 0.0 A,a | 0.0 A,a | 9.1 A,b | 2.7 B,b |
| Seeds # | ||||
| 0.0 g | 54.8 A,a | 56.5 A,a | 33.3 A,a | 24.7 A,a |
| <500 g | 22.6 A,a | 21.7 A,a | 25.0 A,a | 23.3 A,a |
| 500–1000 g | 6.5 A,a | 4.3 A,a | 41.7 A,a | 43.8 A,a |
| 1001–1500 g | 16.1 A,a | 17.4 A,a | 0.0 A,a | 6.8 A,a |
| >1500 g | 0.0 A,a | 0.0 A,a | 0.0 A,a | 1.4 A,a |
| Participants | BMI | WHR | |||
|---|---|---|---|---|---|
| in the Healthy Range | Average ± SD | in the Healthy Range | Average ± SD | ||
| (%) | (kg/m2) | (%) | (kg/m2) | ||
| Group 1 | Male | 35.71 | 27.76 ± 3.44 | 35.71 | 0.92 ± 0.05 |
| Female | 73.91 | 25.41 ± 4.35 | 69.57 | 0.84 ± 0.06 | |
| Group 2 | Male | 30.77 | 27.9 ± 3.37 | 46.15 | 0.88 ± 0.09 |
| Female | 81.69 | 25.14 ± 3.06 | 98.59 | 0.82 ± 0.06 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Markovikj, G.; Knights, V.; Gajdoš Kljusurić, J. Body Weight Loss Efficiency in Overweight and Obese Adults in the Ketogenic Reduction Diet Program—Case Study. Appl. Sci. 2023, 13, 10704. https://doi.org/10.3390/app131910704
Markovikj G, Knights V, Gajdoš Kljusurić J. Body Weight Loss Efficiency in Overweight and Obese Adults in the Ketogenic Reduction Diet Program—Case Study. Applied Sciences. 2023; 13(19):10704. https://doi.org/10.3390/app131910704
Chicago/Turabian StyleMarkovikj, Gordana, Vesna Knights, and Jasenka Gajdoš Kljusurić. 2023. "Body Weight Loss Efficiency in Overweight and Obese Adults in the Ketogenic Reduction Diet Program—Case Study" Applied Sciences 13, no. 19: 10704. https://doi.org/10.3390/app131910704
APA StyleMarkovikj, G., Knights, V., & Gajdoš Kljusurić, J. (2023). Body Weight Loss Efficiency in Overweight and Obese Adults in the Ketogenic Reduction Diet Program—Case Study. Applied Sciences, 13(19), 10704. https://doi.org/10.3390/app131910704