Abstract
Due to its high morbidity and mortality, myocardial infarction is the leading cause of death worldwide. Against this background, rapid diagnosis is of immense importance. Especially in case of an atypical course, the correct diagnosis may be delayed and thus lead to increased mortality rates. In this report, we present a complex case of acute coronary syndrome. A triple-rule-out CT examination was performed in dual-energy CT (DECT) mode. While pulmonary artery embolism and aortic dissection could be ruled out with conventional CT series, the presence of anterior wall infarction was only detectable on DECT reconstructions. Subsequently, adequate and rapid therapy was then initiated leading to survival of the patient.

Figure 1.
Conventional arterial paratransversal CT series (A) and reconstructions (B,C) show multiple soft and calcified plaques in the LAD (RIVA) in the context of CAD. However, the presence of contrast material in the distal course of the LAD remains questionable and cannot be assessed with high diagnostic confidence by conventional CT imaging due to significant image noise and consecutive low image quality.

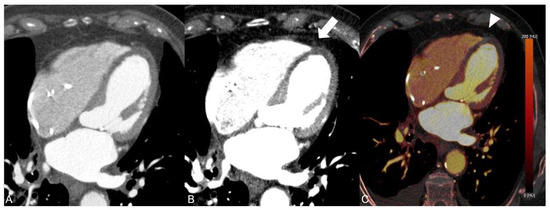
Figure 2.
In comparison with the conventional arterial CT image (A), the complete lack of iodine in the distal course of the LAD can be visualized by application of dual-energy CT-based virtual monoenergetic images at 55 keV (B, arrow) and corresponding iodine maps (C, arrowhead).
Furthermore, the DECT-based iodine maps demonstrated significant hypoperfusion of the anterior wall and anterior septum suggestive for an acute anterior wall infarction, which was missed on conventional CT series (Figure 3). Pulmonary artery embolism and aortic dissection were excluded.
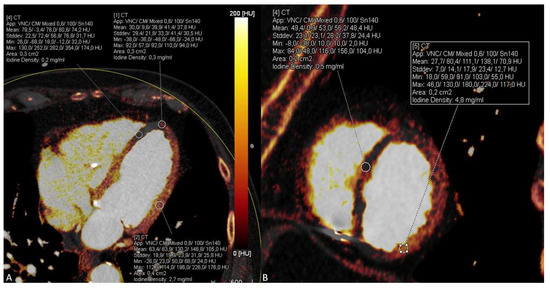
Figure 3.
Significant hypoperfusion of the anterior wall and anterior septum is visible and can be quantified on dual-energy CT iodine maps using the four chamber view (A) and short axis view (B) indicating acute myocardial infarction in this area due to the LAD occlusion.
To initiate significant treatment of the patient, percutaneous transluminal coronary angioplasty (PTCA) was subsequently planned and mechanical recanalization with implantation of double stents in the LAD and LCX was performed. Postinterventional echocardiography revealed an ejection fraction of 35%, indicating continuing moderately reduced systolic left ventricular function. In addition to dual antiplatelet therapy and heart failure therapy, an upgrade to an implantable cardioverter defibrillator (ICD) was initiated. The nasal bone fracture caused by the syncope was treated conservatively during the inpatient stay. In order to detect long-term complications, the patient was scheduled for a second coronary angiography four months later and was subsequently transferred to successful geriatric rehabilitation. Follow-up coronary angiography revealed restenosis of the previously deployed stent in the midportion of the LAD. A stent-in-stent deployment was initiated to redilate the stenosis. As a result, left ventricular function also improved. No further complications occurred in the patient.
Globally, myocardial infarction is the leading cause of death due to its high morbidity and mortality. According to recent data [1], there is an incidence of 290 myocardial infarctions per 100,000 inhibitors, while the mortality rate is about 60 out of 100,000 inhibitants. In order to increase the chances of a person’s survival, it is of enormous importance for to begin treatment as soon as possible after an appropriate diagnosis [2]. Occlusion of the coronary arteries can result in cardiac arrest and functional disorders and lead to death if no adequate treatment is initiated. An anterior wall infarction can affect a large area of the heart [3]. The symptoms of anterior wall infarction are not always pathognomonic and cannot be distinguished from the symptoms of pulmonary artery embolism and aortic dissection or gastritis in certain cases. In addition, other heart diseases such as myocarditis can be the cause of the symptoms. In this context, myocardial anterior wall infarction not infrequently causes diagnostic difficulties but requires rapid workup because of its high lethality [4]. The conventional diagnosis of acute myocardial infarction is usually made with the help of laboratory tests, ECG, and, if necessary, echocardiography. If these examinations do not provide sufficient information about the present disease and do not allow the exclusion of other diseases, a non-invasive CT scan of the heart can be conducted in stable patients if no invasive coronary angiography is performed. In addition, cardiac MRI may be considered as cross-sectional imaging technique for myocardial tissue assessment and functional/volumetric imaging in stable situations, particularly in follow-up [5]. However, this imaging modality is not performed in the acute setting. In the present case, the incident occurred at least 24 to 48 h ago. The performed laboratory tests and the clinical presentation were not strictly specific for a myocardial infarction. Pulmonary embolism and aortic dissection could not be excluded with certainty based on the laboratory results and clinical features. Because of the patient’s hemodynamically stable condition, a DECT scan was preferred over an initial invasive coronary angiography. The DECT examination is our department´s key standard protocol for eliminating differential diagnoses if a final diagnosis of myocardial infarction, pulmonary embolism and aortic dissection has not been made. Using the TRO method, DECT has the advantage that possible differential diagnoses can be successfully excluded. In the context of the presented DECT application, simultaneous visualization of coronary arteries, pulmonary arteries and thoracic aorta in arterial and venous contrast phases, as well as reconstruction of iodine maps and monoenergetic images, allowed the exclusion of pulmonary artery embolism and aortic dissection. Compared with CT angiography, the use of venous-phase DECT as an accurate imaging method for the diagnosis of pulmonary artery embolism has already been significantly demonstrated and represents an additional benefit of DECT in acute coronary pain [6]. While the diagnosis of LAD occlusion and acute anterior wall infarction could not be made with conventional CT images, DECT-based VMI series and iodine maps enabled the prompt detection and therapy initiation of an acute wall infarction due to LAD occlusion. Compared with single-energy CT, DECT has been shown to allow for better tissue differentiation and assessment through the application of a second X-ray spectrum and dedicated postprocessing algorithms [7,8]. In this context, VMI series at low keV levels, such as 55 keV, allow for an increased iodine signal, particularly in vessels, while iodine maps show the direct iodine uptake in tissue without unenhanced background density [9,10]. DECT has made enormous progress in the imaging of cardiovascular diseases in recent years and promises a comprehensive, noninvasive examination of patients in the acute setting [11]. By using CT imaging, nontraumatic as well as traumatic diseases of the chest can be detected. In this context, the combined usage of DECT postprocessing algorithms led to a prompt diagnosis and therapy initiation in our case. However, only very few studies have evaluated the DECT technique and its algorithms in acute myocardial infarction, as well as the significance of iodine mapping for the detection of myocardial perfusion defects to date. In our patient, myocardial infarction and infarct location were reliably diagnosed by DECT, whereas laboratory examination and ECG were nonspecific. In addition, DECT facilitated a prompt diagnosis with high diagnostic confidence compared to conventional CT in our case. Therefore, our recommendation is to perform CT scans in dual-energy mode if technically possible to obtain a rapid and correct diagnosis in comparable circumstances.
Funding
This research received no external funding.
Institutional Review Board Statement
The manuscript contains an account of descriptions of diagnostic tests on a selected patient; the work does not describe a medical experiment-no opinion of the Bioethics Committee was required.
Informed Consent Statement
This is not applicable. Patient´s personal information was not identified in a retrospective study, so informed consent was waived.
Data Availability Statement
In this article, all relevant data are presented. Further inquiries can be directed to the corresponding author.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Statistics on Myocardial Infarctions 2020; The National Board of Health and Welfare: Stockholm County, Sweden, 2021.
- Reed, G.W.; Rossi, J.E.; Cannon, C.P. Acute myocardial infarction. Lancet 2017, 389, 197–210. [Google Scholar] [CrossRef] [PubMed]
- Stone, P.H.; Raabe, D.S.; Jaffe, A.S.; Gustafson, N.; E Muller, J.; Turi, Z.G.; Rutherford, J.D.; Poole, W.; Passamani, E.; Willerson, J.T.; et al. Prognostic significance of location and type of myocardial infarction: Independent adverse outcome associated with anterior location. J. Am. Coll. Cardiol. 1988, 11, 453–463. [Google Scholar] [CrossRef] [PubMed]
- Kennedy, H.L.; Goldberg, R.J.; Szklo, M.; Tonascia, J.A. The prognosis of anterior myocardial infarction revisited: A community-wide study. Clin. Cardiol. 1979, 2, 455–460. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, N.; Carrick, D.; Layland, J.; Oldroyd, K.G.; Berry, C. The role of cardiac magnetic resonance imaging (MRI) in acute myocardial infarction (AMI). Hear. Lung Circ. 2013, 22, 243–255. [Google Scholar] [CrossRef] [PubMed]
- Foti, G.; Silva, R.; Faccioli, N.; Fighera, A.; Menghini, R.; Campagnola, A.; Carbognin, G. Identification of pulmonary embolism: Diagnostic accuracy of venous-phase dual-energy CT in comparison to pulmonary arteries CT angiography. Eur. Radiol. 2021, 31, 1923–1931. [Google Scholar] [CrossRef] [PubMed]
- McCollough, C.H.; Leng, S.; Yu, L.; Fletcher, J.G. Dual- and Multi-Energy CT: Principles, Technical Approaches, and Clinical Applications. Radiology 2015, 276, 637–653. [Google Scholar] [CrossRef] [PubMed]
- Vulasala, S.S.R.; Wynn, G.C.; Hernandez, M.; Kadambi, I.; Gopireddy, D.R.; Bhosale, P.; Virarkar, M.K. Dual-Energy Imaging of the Chest. Semin. Ultrasound CT MRI 2022, 43, 311–319. [Google Scholar] [CrossRef] [PubMed]
- D’Angelo, T. Dual energy computed tomography virtual monoenergetic imaging: Technique and clinical applications. Br. J. Radiol. 2019, 92, 20180546. [Google Scholar] [CrossRef] [PubMed]
- Tatsugami, F.; Higaki, T.; Nakamura, Y.; Honda, Y.; Awai, K. Dual-energy CT: Minimal essentials for radiologists. Jpn. J. Radiol. 2022, 40, 547–559. [Google Scholar] [CrossRef] [PubMed]
- Vliegenthart, R.; Pelgrim, G.J.; Ebersberger, U.; Rowe, G.W.; Oudkerk, M.; Schoepf, U.J. Dual-energy CT of the heart. AJR Am. J. Roentgenol. 2012, 199, S54–S63. [Google Scholar] [CrossRef] [PubMed]


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).