
Rewiring Mood: Precision Psychobiotics as Adjunct or Stand-Alone Therapy in Depression Using Insights from 19 Randomized Controlled Trials in Adults

 , , and
, , and 
Abstract
1. Introduction
2. Materials and Methods
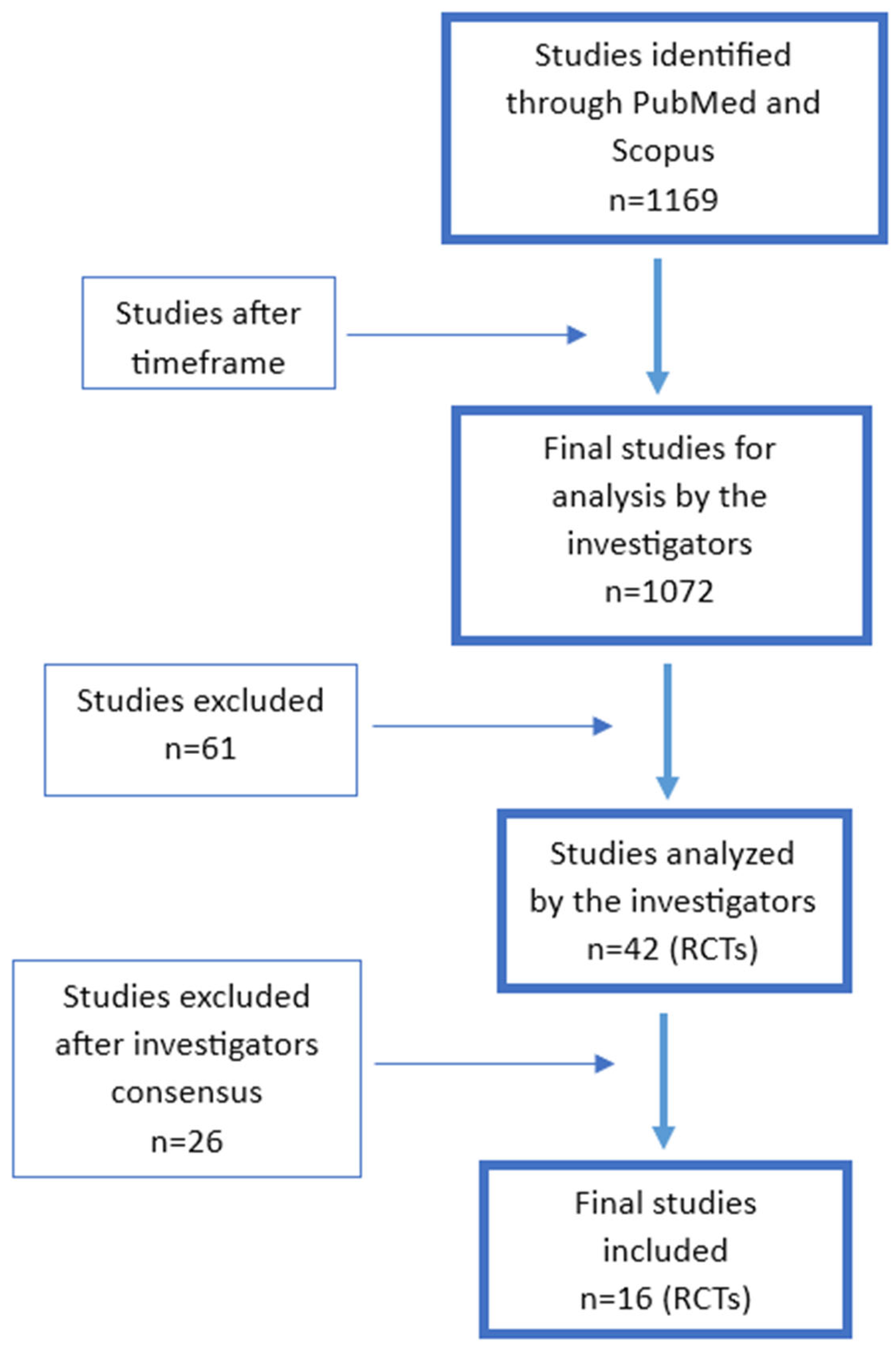
2.1. Search Strategies
2.2. Eligibility Criteria
2.3. Data Extraction
3. Results
3.1. Methodological Considerations
3.2. Overview of Studies (Table 1 and Table 2)

{kind=link}
| Authors, Year, [Ref] | Country | N | Depression Status | Diagnosis Based on | Co-Morbidity | Duration [Weeks] | Antidepressants | Probiotic Strains | Co-Treatment | Dose [cfu/d] | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1. | Akkasheh, G. et al., 2016 [42] | Iran | 40 | MDD | DSM-IV | _ | 8 | not reported | L. acidophilus, L. casei, B. bifidum | 6 × 109 | |
| 2. | Pinto-Sanchez, M.I. et al., 2017 [67] | Switzerland | 44 | D | HAD | IBS | 6 | excluded | B. longum NCC3001 | 1 × 1010 | |
| 3. | Ghorbani, Z. et al., 2018 [61] | Iran | 40 | mD | DSM-V | _ | 6 | add-on | Familact®: L. casei, L. acidophilus, L. bulgaricus, L. rhamnosus, B. breve, B. longum, S. thermophilus | FOS | 8.6 × 109 |
| 4. | Chahwan, B. et al., 2019 [55] | Australia Netherlands | 71 | D | BDI-II | _ | 8 | excluded | Ecologic® Barrier: B. bifidum W23, B. lactis W51, B. lactis W52, L. acidophilus W37, L. brevis W63, L. casei W56, L. salivarius W24, Lc. lactis W19, Lc. lactis W58 | 1 × 1010 | |
| 5. | Kazemi, A et al., 2019 [62] | Iran | 110 | MDD | BDI | _ | 8 | add-on | L. helveticus R0052, B. longum R0175 [CNCM strain I-3470] | 1 × 1010 | |
| 6. | Saccarello, A et al., 2020 [68] | Italy | 90 | D | Z-SDS | _ | 6 | add-on | L. plantarum HEAL9 | SAMe | 1 × 109 |
| 7. | Schaub, A.C. et al., 2022 [53] | Switzerland | 60 | MDD | HAM-D | _ | 4 | add-on | Vivomixx®: Streptococcus thermophilus NCIMB 30438, B. breve NCIMB 30441, B. longum NCIMB 30435, B. infantis NCIMB 30436, L. acidophilus NCIMB 30442, L. plantarum NCIMB 30437, L. paracasei NCIMB 30439, L. delbrueckii ssp. Bulgaricus NCIMB 30440 | 9 × 1011 | |
| 8. | Tian, P. et al., 2022 [27] | China | 45 | MDD | HDRS-24, MADRS, | _ | 4 | no restriction | B. breve CCFM1025 | 1 × 1010 | |
| 9. | Ullah, H. et al., 2022 [69] | Italy | 80 | SD | PHQ-, | _ | 38 | add-on | L. helveticus Rosell®-52, B. longum Rosell®-175 | SAMe | 3 × 109 |
| 10. | Moludi, J. et al., 2022 [70] | Iran | 96 | D | BDI-II | CAD | 8 | excluded | L. rhamnosus GG | 1.9 × 109 | |
| 11. | Nikolova, V.L. et al., 202, [54] | Poland | 50 | MDD | HAMD-17 | _ | 8 | add-on | BioKult Advanced®: L. paracasei PXN37, L. plantarum PXN47, L. rhamnosus PXN54, B. subtilis PXN21, B. bifidum PXN23, B. breve PXN25, B. longum PXN30, L. helveticus PXN35, L. lactis ssp. lactis PXN63, S. thermophilus PXN66, B. infantis PXN27, L. delbruecklii ssp. bulgaricus PXN39, L. helveticus PXN45, L. salivarius PXN57 | 8 × 109 | |
| 12. | Strodl, E. et al., 2024 [71] | Australia | 120 | MDD | DSM-V, BDI-II | _ | 8 | no restriction | NRGBiotic®: L. acidophilus, B. bifidum, S. thermophilus | 8 × 1010 | |
| 13. | Tzikos, G. et al., 2025 [72] | Greece | 266 | D | BDI-II, HDRS-17 | SOP | 4 | excluded | B. animalis subsp. lactis LMG P-21384, B. breve DSM 16604, B. longum DSM 16603, L. rhamnosus ATCC 53103 | 1.76 × 1011 | |
| 14. | Elahinejad, V. et al., 2025 [73] | Iran | 50 | MDD | DSM-IV, HDRS-24 | _ | 8 | add-on | L. helveticus Rosell®-52, B. longum Rosell®-175 | 6 × 109 |
| Authors, Year, [Ref] | Country | N | Depression Status | Diagnosis Based on | Co-Morbidity | Duration [Weeks] | Antidepressants | Probiotic Strains | Co-Treatment | Dose [cfu/d] | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1. | Rudzki, L. et al., 2019 [59] | Scotland, UK, and Poland | 60 | MDD | DSM-IV-R | _ | 8 | add-on | Lactobacillus Plantarum 299v (LP299v) | - | 2 × 1010 |
| 2. | Reininghaus EZ et al., 2020 [33] | Austria | 82 | D | MINI | _ | 4 | add-on | OMNi-BiOTiC® Stress Repair: B. bifidum W23, B. lactis W51, B. lactis W52, L. acidophilus W22, L. casei W56, L. paracasei W20, L. plantarum W62, L. salivarius W24, L. lactis W19 | Biotin | 7.5 × 109 |
| 3. | Gawlik-Kotel-nicka, O. et al., 2024 [2] | Poland | 116 | D | MADRS | AO/MeS | 8 | no restriction | L. helveticus Rosell®-52, B. longum Rosell®-175 | - | 3 × 109 |
| 4. | Sarkawi, M. et al., 2024 [74] | Malaysia | 124 | SD | CESD-R | IBS | 12 | excluded | Lactobacillus acidophilus LA-5, Lactobacillus paracasei L. CASEI-01 | - | 2 × 109 |
| 5. | Lin, S.K. et al., 2024 [75] | Malaysia | 32 | MDD | DSM-V, HAMD-17, DSSS | 8 | add-on | L. plantarum PS128 | - | 3 × 1010 |
3.3. Additional Benefits
| Improvements | Psychobiotic Strains |
|---|---|
| Cognitive function |
|
| Anxiety status |
|
| Emotional status |
|
| Affect brain structure and function |
|
| Increase in 5-HT and metabolites | |
| Enhance SSRI effects |
|
| Regulation of appetite [ghrelin, leptin] |
|
| Enhance immune activity |
|
3.4. Gut Microbiome Changes and Depression Amelioration
4. Discussion
5. Final Thoughts and Future Perspectives
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| BAI | Beck Anxiety Inventory |
| BDI | Beck Depression Inventory Score |
| CESD-R | Center for Epidemiologic Studies Depression Revised questionnaire |
| DSM-5 | Diagnostic and Statistical Manual of Mental Disorders |
| GAD-7 | General Anxiety Disorder |
| GSRS | Gastrointestinal Symptom Rating Scale |
| HADRS-24 | Hamilton Depression Rating Scale—24 item |
| HADS | Hospital Anxiety and Depression Scale |
| HAM-D-17 | Hamilton Rating Scale for Depression |
| HAMA | Hamilton Anxiety Rating Scale |
| IDS | Inventory of Depressive Symptoms-Clinician rated |
| MADRS | Montgomery–Asberg Depression Rating Scale |
| MDD | Major Depression Disorder |
| PHW-9 | Patient Health Questionnaire-9 |
| SCID-5-RV | Structured Clinical Interview |
| SCL-90 | Symptom Checklist-90-Revised |
| STAI | State–Trait Anxiety Inventory |
| VLMT | Verbal Learning Memory Test |
| Z-SDS | Zung Self-Rating Depression Scale |
References
- Whiteford, H.A.; Degenhardt, L.; Rehm, J.; Baxter, A.J.; Ferrari, A.J.; Erskine, H.E.; Charlson, F.J.; Norman, R.E.; Flaxman, A.D.; Johns, N.; et al. Global burden of disease attributable to mental and substance use disorders: Findings from the Global Burden of Disease Study 2010. Lancet 2013, 382, 1575–1586. [Google Scholar] [CrossRef] [PubMed]
- Gawlik-Kotelnicka, O.; Margulska, A.; Płeska, K.; Skowrońska, A.; Strzelecki, D. Metabolic Status Influences Probiotic Efficacy for Depression-PRO-DEMET Randomized Clinical Trial Results. Nutrients 2024, 16, 1389. [Google Scholar] [CrossRef] [PubMed]
- World-Health-Organization. Depression and Other Common Mental Disorders: Global Health Estimates. Available online: http://apps.who.int/iris/bitstream/10665/254610/1/WHO-MSD-MER-2017.2-eng.pdf (accessed on 22 April 2025).
- Härter, M.; Klesse, C.; Bermejo, I.; Schneider, F.; Berger, M. Unipolar depression: Diagnostic and therapeutic recommendations from the current S3/National Clinical Practice Guideline. Dtsch. Arztebl. Int. 2010, 107, 700–708. [Google Scholar] [CrossRef] [PubMed]
- Abdoli, N.; Salari, N.; Darvishi, N.; Jafarpour, S.; Solaymani, M.; Mohammadi, M.; Shohaimi, S. The global prevalence of major depressive disorder (MDD) among the elderly: A systematic review and meta-analysis. Neurosci. Biobehav. Rev. 2022, 132, 1067–1073. [Google Scholar] [CrossRef]
- Zhang, X.; Chen, S.; Zhang, M.; Ren, F.; Ren, Y.; Li, Y.; Liu, N.; Zhang, Y.; Zhang, Q.; Wang, R. Effects of Fermented Milk Containing Lacticaseibacillus paracasei Strain Shirota on Constipation in Patients with Depression: A Randomized, Double-Blind, Placebo-Controlled Trial. Nutrients 2021, 13, 2238. [Google Scholar] [CrossRef]
- Hashemi-Mohammadabad, N.; Taghavi, S.A.; Lambert, N.; Moshtaghi, R.; Bazarganipour, F.; Sharifi, M. Adjuvant administration of probiotic effects on sexual function in depressant women undergoing SSRIs treatment: A double-blinded randomized controlled trial. BMC Psychiatry 2024, 24, 44. [Google Scholar] [CrossRef]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Association Publishing: Washington, DC, USA, 2022. [Google Scholar]
- Lai, W.; Liao, Y.; Zhang, H.; Zhao, H.; Li, Y.; Chen, R.; Shi, G.; Liu, Y.; Hao, J.; Li, Z.; et al. The trajectory of depressive symptoms and the association with quality of life and suicidal ideation in patients with major depressive disorder. BMC Psychiatry 2025, 25, 310. [Google Scholar] [CrossRef]
- Gao, K.; Su, M.; Sweet, J.; Calabrese, J.R. Correlation between depression/anxiety symptom severity and quality of life in patients with major depressive disorder or bipolar disorder. J. Affect. Disord. 2019, 244, 9–15. [Google Scholar] [CrossRef]
- National Institute for Health and Care Excellence: Guidelines. In Depression in Adults: Treatment and Management; National Institute for Health and Care Excellence (NICE) Copyright © NICE 2022: London, UK, 2022.
- Rush, A.J.; Trivedi, M.H.; Wisniewski, S.R.; Nierenberg, A.A.; Stewart, J.W.; Warden, D.; Niederehe, G.; Thase, M.E.; Lavori, P.W.; Lebowitz, B.D.; et al. Acute and longer-term outcomes in depressed outpatients requiring one or several treatment steps: A STAR*D report. Am. J. Psychiatry 2006, 163, 1905–1917. [Google Scholar] [CrossRef]
- Al-Harbi, K.S. Treatment-resistant depression: Therapeutic trends, challenges, and future directions. Patient Prefer. Adherence 2012, 6, 369–388. [Google Scholar] [CrossRef]
- Barlati, S.; Minelli, A.; Nibbio, G.; Bertoni, L.; Necchini, N.; Paolini, S.; Muscarella, A.; Ubertino, U.B.; Calzavara-Pinton, I.; Vita, A.; et al. The role of pharmacogenetics in the treatment of major depressive disorder: A critical review. Front. Psychiatry 2023, 14, 1307473. [Google Scholar] [CrossRef] [PubMed]
- Gadad, B.S.; Jha, M.K.; Czysz, A.; Furman, J.L.; Mayes, T.L.; Emslie, M.P.; Trivedi, M.H. Peripheral biomarkers of major depression and antidepressant treatment response: Current knowledge and future outlooks. J. Affect. Disord. 2018, 233, 3–14. [Google Scholar] [CrossRef] [PubMed]
- MacDonald, K.; Krishnan, A.; Cervenka, E.; Hu, G.; Guadagno, E.; Trakadis, Y. Biomarkers for major depressive and bipolar disorders using metabolomics: A systematic review. Am. J. Med. Genet. B Neuropsychiatr. Genet. 2019, 180, 122–137. [Google Scholar] [CrossRef] [PubMed]
- Pedrini, M.; Cao, B.; Nani, J.V.S.; Cerqueira, R.O.; Mansur, R.B.; Tasic, L.; Hayashi, M.A.F.; McIntyre, R.S.; Brietzke, E. Advances and challenges in development of precision psychiatry through clinical metabolomics on mood and psychotic disorders. Prog. Neuropsychopharmacol. Biol. Psychiatry 2019, 93, 182–188. [Google Scholar] [CrossRef]
- Martin, C.R.; Osadchiy, V.; Kalani, A.; Mayer, E.A. The Brain-Gut-Microbiome Axis. Cell Mol. Gastroenterol. Hepatol. 2018, 6, 133–148. [Google Scholar] [CrossRef]
- Cryan, J.F.; Dinan, T.G. Mind-altering microorganisms: The impact of the gut microbiota on brain and behaviour. Nat. Rev. Neurosci. 2012, 13, 701–712. [Google Scholar] [CrossRef]
- Dinan, T.G.; Cryan, J.F. Gut instincts: Microbiota as a key regulator of brain development, ageing and neurodegeneration. J. Physiol. 2017, 595, 489–503. [Google Scholar] [CrossRef]
- Zhu, F.; Tu, H.; Chen, T. The Microbiota-Gut-Brain Axis in Depression: The Potential Pathophysiological Mechanisms and Microbiota Combined Antidepression Effect. Nutrients 2022, 14, 2081. [Google Scholar] [CrossRef]
- Zhang, Y.; Li, Y.; Yuan, Y.; Wang, J.; Zhang, S.; Zhu, R.; Wang, Y.; Wu, Y.; Liao, X.; Mi, J. Reducing light exposure enhances the circadian rhythm of the biological clock through interactions with the gut microbiota. Sci. Total Environ. 2023, 858, 160041. [Google Scholar] [CrossRef]
- Nikolova, V.L.; Smith, M.R.B.; Hall, L.J.; Cleare, A.J.; Stone, J.M.; Young, A.H. Perturbations in Gut Microbiota Composition in Psychiatric Disorders: A Review and Meta-analysis. JAMA Psychiatry 2021, 78, 1343–1354. [Google Scholar] [CrossRef]
- Valles-Colomer, M.; Falony, G.; Darzi, Y.; Tigchelaar, E.F.; Wang, J.; Tito, R.Y.; Schiweck, C.; Kurilshikov, A.; Joossens, M.; Wijmenga, C.; et al. The neuroactive potential of the human gut microbiota in quality of life and depression. Nat. Microbiol. 2019, 4, 623–632. [Google Scholar] [CrossRef] [PubMed]
- McGuinness, A.J.; Davis, J.A.; Dawson, S.L.; Loughman, A.; Collier, F.; O‘Hely, M.; Simpson, C.A.; Green, J.; Marx, W.; Hair, C.; et al. A systematic review of gut microbiota composition in observational studies of major depressive disorder, bipolar disorder and schizophrenia. Mol. Psychiatry 2022, 27, 1920–1935. [Google Scholar] [CrossRef] [PubMed]
- Donoso, F.; Cryan, J.F.; Olavarría-Ramírez, L.; Nolan, Y.M.; Clarke, G. Inflammation, Lifestyle Factors, and the Microbiome-Gut-Brain Axis: Relevance to Depression and Antidepressant Action. Clin. Pharmacol. Ther. 2023, 113, 246–259. [Google Scholar] [CrossRef] [PubMed]
- Tian, P.; Chen, Y.; Zhu, H.; Wang, L.; Qian, X.; Zou, R.; Zhao, J.; Zhang, H.; Qian, L.; Wang, Q.; et al. Bifidobacterium breve CCFM1025 attenuates major depression disorder via regulating gut microbiome and tryptophan metabolism: A randomized clinical trial. Brain Behav. Immun. 2022, 100, 233–241. [Google Scholar] [CrossRef]
- Kelly, J.R.; Borre, Y.; O’Brien, C.; Patterson, E.; El Aidy, S.; Deane, J.; Kennedy, P.J.; Beers, S.; Scott, K.; Moloney, G.; et al. Transferring the blues: Depression-associated gut microbiota induces neurobehavioural changes in the rat. J. Psychiatr. Res. 2016, 82, 109–118. [Google Scholar] [CrossRef]
- Cryan, J.F.; Dinan, T.G. Gut microbiota: Microbiota and neuroimmune signalling-Metchnikoff to microglia. Nat. Rev. Gastroenterol. Hepatol. 2015, 12, 494–496. [Google Scholar] [CrossRef]
- Hsiao, E.Y.; McBride, S.W.; Hsien, S.; Sharon, G.; Hyde, E.R.; McCue, T.; Codelli, J.A.; Chow, J.; Reisman, S.E.; Petrosino, J.F.; et al. Microbiota modulate behavioral and physiological abnormalities associated with neurodevelopmental disorders. Cell 2013, 155, 1451–1463. [Google Scholar] [CrossRef]
- Sarkar, A.; Lehto, S.M.; Harty, S.; Dinan, T.G.; Cryan, J.F.; Burnet, P.W.J. Psychobiotics and the Manipulation of Bacteria-Gut-Brain Signals. Trends Neurosci. 2016, 39, 763–781. [Google Scholar] [CrossRef]
- Dinan, T.G.; Stanton, C.; Cryan, J.F. Psychobiotics: A novel class of psychotropic. Biol. Psychiatry 2013, 74, 720–726. [Google Scholar] [CrossRef]
- Reininghaus, E.Z.; Platzer, M.; Kohlhammer-Dohr, A.; Hamm, C.; Mörkl, S.; Bengesser, S.A.; Fellendorf, F.T.; Lahousen-Luxenberger, T.; Leitner-Afschar, B.; Schöggl, H.; et al. PROVIT: Supplementary Probiotic Treatment and Vitamin B7 in Depression-A Randomized Controlled Trial. Nutrients 2020, 12, 3422. [Google Scholar] [CrossRef]
- O‘Mahony, S.M.; Clarke, G.; Borre, Y.E.; Dinan, T.G.; Cryan, J.F. Serotonin, tryptophan metabolism and the brain-gut-microbiome axis. Behav. Brain Res. 2015, 277, 32–48. [Google Scholar] [CrossRef] [PubMed]
- Berding, K.; Bastiaanssen, T.F.S.; Moloney, G.M.; Boscaini, S.; Strain, C.R.; Anesi, A.; Long-Smith, C.; Mattivi, F.; Stanton, C.; Clarke, G.; et al. Feed your microbes to deal with stress: A psychobiotic diet impacts microbial stability and perceived stress in a healthy adult population. Mol. Psychiatry 2023, 28, 601–610. [Google Scholar] [CrossRef] [PubMed]
- Sanada, K.; Nakajima, S.; Kurokawa, S.; Barceló-Soler, A.; Ikuse, D.; Hirata, A.; Yoshizawa, A.; Tomizawa, Y.; Salas-Valero, M.; Noda, Y.; et al. Gut microbiota and major depressive disorder: A systematic review and meta-analysis. J. Affect. Disord. 2020, 266, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Ma, Q.; Xing, C.; Long, W.; Wang, H.Y.; Liu, Q.; Wang, R.F. Impact of microbiota on central nervous system and neurological diseases: The gut-brain axis. J. Neuroinflammation 2019, 16, 53. [Google Scholar] [CrossRef]
- Messaoudi, M.; Lalonde, R.; Violle, N.; Javelot, H.; Desor, D.; Nejdi, A.; Bisson, J.F.; Rougeot, C.; Pichelin, M.; Cazaubiel, M.; et al. Assessment of psychotropic-like properties of a probiotic formulation (Lactobacillus helveticus R0052 and Bifidobacterium longum R0175) in rats and human subjects. Br. J. Nutr. 2011, 105, 755–764. [Google Scholar] [CrossRef]
- Wauters, L.; Van Oudenhove, L.; Accarie, A.; Geboers, K.; Geysen, H.; Toth, J.; Luypaerts, A.; Verbeke, K.; Smokvina, T.; Raes, J.; et al. Lactobacillus rhamnosus CNCM I-3690 decreases subjective academic stress in healthy adults: A randomized placebo-controlled trial. Gut Microbes 2022, 14, 2031695. [Google Scholar] [CrossRef]
- Le Morvan de Sequeira, C.; Hengstberger, C.; Enck, P.; Mack, I. Effect of Probiotics on Psychiatric Symptoms and Central Nervous System Functions in Human Health and Disease: A Systematic Review and Meta-Analysis. Nutrients 2022, 14, 621. [Google Scholar] [CrossRef]
- Akbari, E.; Asemi, Z.; Daneshvar Kakhaki, R.; Bahmani, F.; Kouchaki, E.; Tamtaji, O.R.; Hamidi, G.A.; Salami, M. Effect of Probiotic Supplementation on Cognitive Function and Metabolic Status in Alzheimer’s Disease: A Randomized, Double-Blind and Controlled Trial. Front. Aging Neurosci. 2016, 8, 256. [Google Scholar] [CrossRef]
- Akkasheh, G.; Kashani-Poor, Z.; Tajabadi-Ebrahimi, M.; Jafari, P.; Akbari, H.; Taghizadeh, M.; Memarzadeh, M.R.; Asemi, Z.; Esmaillzadeh, A. Clinical and metabolic response to probiotic administration in patients with major depressive disorder: A randomized, double-blind, placebo-controlled trial. Nutrition 2016, 32, 315–320. [Google Scholar] [CrossRef]
- Huang, R.; Wang, K.; Hu, J. Effect of Probiotics on Depression: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Nutrients 2016, 8, 483. [Google Scholar] [CrossRef]
- Rao, A.V.; Bested, A.C.; Beaulne, T.M.; Katzman, M.A.; Iorio, C.; Berardi, J.M.; Logan, A.C. A randomized, double-blind, placebo-controlled pilot study of a probiotic in emotional symptoms of chronic fatigue syndrome. Gut Pathog. 2009, 1, 6. [Google Scholar] [CrossRef] [PubMed]
- Mörkl, S.; Butler, M.I.; Holl, A.; Cryan, J.F.; Dinan, T.G. Probiotics and the Microbiota-Gut-Brain Axis: Focus on Psychiatry. Curr. Nutr. Rep. 2020, 9, 171–182. [Google Scholar] [CrossRef] [PubMed]
- Misera, A.; Liśkiewicz, P.; Łoniewski, I.; Skonieczna-Żydecka, K.; Samochowiec, J. Effect of Psychobiotics on Psychometric Tests and Inflammatory Markers in Major Depressive Disorder: Meta-Analysis of Randomized Controlled Trials with Meta-Regression. Pharmaceuticals 2021, 14, 952. [Google Scholar] [CrossRef] [PubMed]
- Goh, K.K.; Liu, Y.W.; Kuo, P.H.; Chung, Y.E.; Lu, M.L.; Chen, C.H. Effect of probiotics on depressive symptoms: A meta-analysis of human studies. Psychiatry Res. 2019, 282, 112568. [Google Scholar] [CrossRef]
- Liu, R.T.; Walsh, R.F.L.; Sheehan, A.E. Prebiotics and probiotics for depression and anxiety: A systematic review and meta-analysis of controlled clinical trials. Neurosci. Biobehav. Rev. 2019, 102, 13–23. [Google Scholar] [CrossRef]
- Ng, Q.X.; Peters, C.; Ho, C.Y.X.; Lim, D.Y.; Yeo, W.S. A meta-analysis of the use of probiotics to alleviate depressive symptoms. J. Affect. Disord. 2018, 228, 13–19. [Google Scholar] [CrossRef]
- Nikolova, V.L.; Cleare, A.J.; Young, A.H.; Stone, J.M. Updated Review and Meta-Analysis of Probiotics for the Treatment of Clinical Depression: Adjunctive vs. Stand-Alone Treatment. J. Clin. Med. 2021, 10, 647. [Google Scholar] [CrossRef]
- Alli, S.R.; Gorbovskaya, I.; Liu, J.C.W.; Kolla, N.J.; Brown, L.; Müller, D.J. The Gut Microbiome in Depression and Potential Benefit of Prebiotics, Probiotics and Synbiotics: A Systematic Review of Clinical Trials and Observational Studies. Int. J. Mol. Sci. 2022, 23, 4494. [Google Scholar] [CrossRef]
- Skowron, K.; Budzyńska, A.; Wiktorczyk-Kapischke, N.; Chomacka, K.; Grudlewska-Buda, K.; Wilk, M.; Wałecka-Zacharska, E.; Andrzejewska, M.; Gospodarek-Komkowska, E. The Role of Psychobiotics in Supporting the Treatment of Disturbances in the Functioning of the Nervous System-A Systematic Review. Int. J. Mol. Sci. 2022, 23, 7820. [Google Scholar] [CrossRef]
- Schaub, A.-C.; Schneider, E.; Vazquez-Castellanos, J.F.; Schweinfurth, N.; Kettelhack, C.; Doll, J.P.K.; Yamanbaeva, G.; Mählmann, L.; Brand, S.; Beglinger, C.; et al. Clinical, gut microbial and neural effects of a probiotic add-on therapy in depressed patients: A randomized controlled trial. Transl. Psychiatry 2022, 12, 227. [Google Scholar] [CrossRef]
- Nikolova, V.L.; Cleare, A.J.; Young, A.H.; Stone, J.M. Acceptability, Tolerability, and Estimates of Putative Treatment Effects of Probiotics as Adjunctive Treatment in Patients With Depression: A Randomized Clinical Trial. JAMA Psychiatry 2023, 80, 842–847. [Google Scholar] [CrossRef] [PubMed]
- Chahwan, B.; Kwan, S.; Isik, A.; van Hemert, S.; Burke, C.; Roberts, L. Gut feelings: A randomised, triple-blind, placebo-controlled trial of probiotics for depressive symptoms. J. Affect. Disord. 2019, 253, 317–326. [Google Scholar] [CrossRef] [PubMed]
- Johnson, D.; Thurairajasingam, S.; Letchumanan, V.; Chan, K.G.; Lee, L.H. Exploring the Role and Potential of Probiotics in the Field of Mental Health: Major Depressive Disorder. Nutrients 2021, 13, 1728. [Google Scholar] [CrossRef] [PubMed]
- Yong, S.J.; Tong, T.; Chew, J.; Lim, W.L. Antidepressive Mechanisms of Probiotics and Their Therapeutic Potential. Front. Neurosci. 2019, 13, 1361. [Google Scholar] [CrossRef]
- Naseribafrouei, A.; Hestad, K.; Avershina, E.; Sekelja, M.; Linløkken, A.; Wilson, R.; Rudi, K. Correlation between the human fecal microbiota and depression. Neurogastroenterol. Motil. 2014, 26, 1155–1162. [Google Scholar] [CrossRef]
- Rudzki, L.; Ostrowska, L.; Pawlak, D.; Małus, A.; Pawlak, K.; Waszkiewicz, N.; Szulc, A. Probiotic Lactobacillus Plantarum 299v decreases kynurenine concentration and improves cognitive functions in patients with major depression: A double-blind, randomized, placebo controlled study. Psychoneuroendocrinology 2019, 100, 213–222. [Google Scholar] [CrossRef]
- Lee, H.J.; Hong, J.K.; Kim, J.K.; Kim, D.H.; Jang, S.W.; Han, S.W.; Yoon, I.Y. Effects of Probiotic NVP-1704 on Mental Health and Sleep in Healthy Adults: An 8-Week Randomized, Double-Blind, Placebo-Controlled Trial. Nutrients 2021, 13, 2660. [Google Scholar] [CrossRef]
- Ghorbani, Z.; Nazari, S.; Etesam, F.; Nourimajd, S.; Ahmadpanah, M.; Razeghi, S. The Effect of Synbiotic as an Adjuvant Therapy to Fluoxetine in Moderate Depression: A Randomized Multicenter Trial. Arch. Neurosci. 2018, 5, e60507. [Google Scholar] [CrossRef]
- Kazemi, A.; Noorbala, A.A.; Azam, K.; Eskandari, M.H.; Djafarian, K. Effect of probiotic and prebiotic vs placebo on psychological outcomes in patients with major depressive disorder: A randomized clinical trial. Clin. Nutr. 2019, 38, 522–528. [Google Scholar] [CrossRef]
- Wallace, C.J.K.; Milev, R. The effects of probiotics on depressive symptoms in humans: A systematic review. Ann. Gen. Psychiatry 2017, 16, 14. [Google Scholar] [CrossRef]
- Mangiola, F.; Ianiro, G.; Franceschi, F.; Fagiuoli, S.; Gasbarrini, G.; Gasbarrini, A. Gut microbiota in autism and mood disorders. World J. Gastroenterol. 2016, 22, 361–368. [Google Scholar] [CrossRef] [PubMed]
- Gawlik-Kotelnicka, O.; Margulska, A.; Skowrońska, A.; Strzelecki, D. PRO-DEMET Randomized Controlled Trial on Probiotics in Depression-Pilot Study Results. Nutrients 2023, 15, 1400. [Google Scholar] [CrossRef] [PubMed]
- Salminen, S.; Collado, M.C.; Endo, A.; Hill, C.; Lebeer, S.; Quigley, E.M.M.; Sanders, M.E.; Shamir, R.; Swann, J.R.; Szajewska, H.; et al. Author Correction: The International Scientific Association of Probiotics and Prebiotics (ISAPP) consensus statement on the definition and scope of postbiotics. Nat. Rev. Gastroenterol. Hepatol. 2022, 19, 551. [Google Scholar] [CrossRef] [PubMed]
- Pinto-Sanchez, M.I.; Hall, G.B.; Ghajar, K.; Nardelli, A.; Bolino, C.; Lau, J.T.; Martin, F.P.; Cominetti, O.; Welsh, C.; Rieder, A.; et al. Probiotic Bifidobacterium longum NCC3001 Reduces Depression Scores and Alters Brain Activity: A Pilot Study in Patients With Irritable Bowel Syndrome. Gastroenterology 2017, 153, 448–459.e448. [Google Scholar] [CrossRef]
- Saccarello, A.; Montarsolo, P.; Massardo, I.; Picciotto, R.; Pedemonte, A.; Castagnaro, R.; Brasesco, P.C.; Guida, V.; Picco, P.; Fioravanti, P.; et al. Oral Administration of S-Adenosylmethionine (SAMe) and Lactobacillus Plantarum HEAL9 Improves the Mild-To-Moderate Symptoms of Depression: A Randomized, Double-Blind, Placebo-Controlled Study. Prim. Care Companion CNS Disord. 2020, 22, 19m02578. [Google Scholar] [CrossRef]
- Ullah, H.; Di Minno, A.; Esposito, C.; El-Seedi, H.R.; Khalifa, S.A.M.; Baldi, A.; Greco, A.; Santonastaso, S.; Cioffi, V.; Sperandeo, R.; et al. Efficacy of a food supplement based on S-adenosyl methionine and probiotic strains in subjects with subthreshold depression and mild-to-moderate depression: A monocentric, randomized, cross-over, double-blind, placebo-controlled clinical trial. Biomed. Pharmacother. 2022, 156, 113930. [Google Scholar] [CrossRef]
- Moludi, J.; Khedmatgozar, H.; Nachvak, S.M.; Abdollahzad, H.; Moradinazar, M.; Sadeghpour Tabaei, A. The effects of co-administration of probiotics and prebiotics on chronic inflammation, and depression symptoms in patients with coronary artery diseases: A randomized clinical trial. Nutr. Neurosci. 2022, 25, 1659–1668. [Google Scholar] [CrossRef]
- Strodl, E.; Bambling, M.; Parnam, S.; Ritchie, G.; Cramb, S.; Vitetta, L. Probiotics and magnesium orotate for the treatment of major depressive disorder: A randomised double blind controlled trial. Sci. Rep. 2024, 14, 20841. [Google Scholar] [CrossRef]
- Tzikos, G.; Chamalidou, E.; Christopoulou, D.; Apostolopoulou, A.; Gkarmiri, S.; Pertsikapa, M.; Menni, A.E.; Theodorou, I.M.; Stavrou, G.; Doutsini, N.D.; et al. Psychobiotics Ameliorate Depression and Anxiety Status in Surgical Oncology Patients: Results from the ProDeCa Study. Nutrients 2025, 17, 857. [Google Scholar] [CrossRef]
- Elahinejad, V.; Khorasanian, A.S.; Tehrani-Doost, M.; Khosravi-Darani, K.; Mirsepasi, Z.; Effatpanah, M.; Askari-Rabori, R.; Tajadod, S.; Jazayeri, S. Effects of Probiotics as Adjunctive Therapy to Fluoxetine on Depression Severity and Serum Brain-Derived Neurotrophic Factor, Cortisol, and Adrenocorticotropic Hormone in Patients With Major Depressive Disorder: A Randomized, Double-Blind, Placebo-Controlled Trial. Food Sci. Nutr. 2025, 13, e4698. [Google Scholar] [CrossRef]
- Sarkawi, M.; Raja Ali, R.A.; Abdul Wahab, N.; Abdul Rathi, N.D.; Mokhtar, N.M. A randomized, double-blinded, placebo-controlled clinical trial on Lactobacillus-containing cultured milk drink as adjuvant therapy for depression in irritable bowel syndrome. Sci. Rep. 2024, 14, 9478. [Google Scholar] [CrossRef] [PubMed]
- Lin, S.K.; Kuo, P.H.; Hsu, C.Y.; Chiu, Y.H.; Chen, C.H. The effects of Lactobacillus plantarum PS128 in patients with major depressive disorder: An eight-week double-blind, placebo-controlled study. Asian J. Psychiatr. 2024, 101, 104210. [Google Scholar] [CrossRef] [PubMed]
- Godzien, J.; Kalaska, B.; Rudzki, L.; Barbas-Bernardos, C.; Swieton, J.; Lopez-Gonzalvez, A.; Ostrowska, L.; Szulc, A.; Waszkiewicz, N.; Ciborowski, M.; et al. Probiotic Lactobacillus plantarum 299v supplementation in patients with major depression in a double-blind, randomized, placebo-controlled trial: A metabolomics study. J. Affect. Disord. 2025, 368, 180–190. [Google Scholar] [CrossRef] [PubMed]
- Schneider, E.; Doll, J.P.K.; Schweinfurth, N.; Kettelhack, C.; Schaub, A.C.; Yamanbaeva, G.; Varghese, N.; Mählmann, L.; Brand, S.; Eckert, A.; et al. Effect of short-term, high-dose probiotic supplementation on cognition, related brain functions and BDNF in patients with depression: A secondary analysis of a randomized controlled trial. J. Psychiatry Neurosci. 2023, 48, E23–E33. [Google Scholar] [CrossRef]
- Yamanbaeva, G.; Schaub, A.C.; Schneider, E.; Schweinfurth, N.; Kettelhack, C.; Doll, J.P.K.; Mählmann, L.; Brand, S.; Beglinger, C.; Borgwardt, S.; et al. Effects of a probiotic add-on treatment on fronto-limbic brain structure, function, and perfusion in depression: Secondary neuroimaging findings of a randomized controlled trial. J. Affect. Disord. 2023, 324, 529–538. [Google Scholar] [CrossRef]
- Tian, P.; O‘Riordan, K.J.; Lee, Y.K.; Wang, G.; Zhao, J.; Zhang, H.; Cryan, J.F.; Chen, W. Towards a psychobiotic therapy for depression: Bifidobacterium breve CCFM1025 reverses chronic stress-induced depressive symptoms and gut microbial abnormalities in mice. Neurobiol. Stress. 2020, 12, 100216. [Google Scholar] [CrossRef]
- Kazemi, A.; Noorbala, A.A.; Djafarian, K. Effect of probiotic and prebiotic versus placebo on appetite in patients with major depressive disorder: Post hoc analysis of a randomised clinical trial. J. Hum. Nutr. Diet. 2020, 33, 56–65. [Google Scholar] [CrossRef]
- Sempach, L.; Doll, J.P.K.; Limbach, V.; Marzetta, F.; Schaub, A.C.; Schneider, E.; Kettelhack, C.; Mählmann, L.; Schweinfurth-Keck, N.; Ibberson, M.; et al. Examining immune-inflammatory mechanisms of probiotic supplementation in depression: Secondary findings from a randomized clinical trial. Transl. Psychiatry 2024, 14, 305. [Google Scholar] [CrossRef]
- Simpson, C.A.; Diaz-Arteche, C.; Eliby, D.; Schwartz, O.S.; Simmons, J.G.; Cowan, C.S.M. The gut microbiota in anxiety and depression—A systematic review. Clin. Psychol. Rev. 2021, 83, 101943. [Google Scholar] [CrossRef]
- Liu, L.; Wang, H.; Chen, X.; Zhang, Y.; Zhang, H.; Xie, P. Gut microbiota and its metabolites in depression: From pathogenesis to treatment. EBioMedicine 2023, 90, 104527. [Google Scholar] [CrossRef]
- Nikolova, V.L.; Cleare, A.J.; Young, A.H.; Stone, J.M. Exploring the mechanisms of action of probiotics in depression: Results from a randomized controlled pilot trial. J. Affect. Disord. 2025, 376, 241–250. [Google Scholar] [CrossRef] [PubMed]
- Hill, C.; Guarner, F.; Reid, G.; Gibson, G.R.; Merenstein, D.J.; Pot, B.; Morelli, L.; Canani, R.B.; Flint, H.J.; Salminen, S.; et al. Expert consensus document. The International Scientific Association for Probiotics and Prebiotics consensus statement on the scope and appropriate use of the term probiotic. Nat. Rev. Gastroenterol. Hepatol. 2014, 11, 506–514. [Google Scholar] [CrossRef] [PubMed]
- Sanders, M. How do we know when something called "probiotic" is really a probiotic? A guideline for consumers and health care professionals. Funct. Food Rev. 2009, 1, 3–12. [Google Scholar]
- Barrio, C.; Arias-Sánchez, S.; Martín-Monzón, I. The gut microbiota-brain axis, psychobiotics and its influence on brain and behaviour: A systematic review. Psychoneuroendocrinology 2022, 137, 105640. [Google Scholar] [CrossRef]
- Smythies, J.R. The role of the one-carbon cycle in neuropsychiatric disease. Biol. Psychiatry 1984, 19, 755–758. [Google Scholar]
- Tillmann, S.; Awwad, H.M.; MacPherson, C.W.; Happ, D.F.; Treccani, G.; Geisel, J.; Tompkins, T.A.; Ueland, P.M.; Wegener, G.; Obeid, R. The Kynurenine Pathway Is Upregulated by Methyl-deficient Diet and Changes Are Averted by Probiotics. Mol. Nutr. Food Res. 2021, 65, e2100078. [Google Scholar] [CrossRef]
- Wang, Q.; Hu, Y.; Li, F.; Hu, L.; Zhang, Y.; Qiao, Y.; Tang, C.; Wang, R. MgSO4 alleviates hippocampal neuroinflammation and BBB damage to resist CMS-induced depression. Front. Nutr. 2025, 12, 1470505. [Google Scholar] [CrossRef]
- Rodríguez-Morán, M.; Guerrero-Romero, F.; Barragán-Zuñiga, J.; Gamboa-Gómez, C.I.; Weyman-Vela, Y.; Arce-Quiñones, M.; Simental-Mendía, L.E.; Martínez-Aguilar, G. Combined oral supplementation with magnesium plus vitamin D alleviates mild to moderate depressive symptoms related to long-COVID: An open-label randomized, controlled clinical trial. Magnes. Res. 2024, 37, 49–57. [Google Scholar] [CrossRef]
- Bertazzoni, E.; Donelli, G.; Midtvedt, T.; Nicoli, J.; Sanz, Y. Probiotics and clinical effects: Is the number what counts? J. Chemother. 2013, 25, 193–212. [Google Scholar] [CrossRef]
- Önning, G.; Montelius, C.; Hillman, M.; Larsson, N. Intake of Lactiplantibacillus plantarum HEAL9 Improves Cognition in Moderately Stressed Subjects: A Randomized Controlled Study. Nutrients 2023, 15, 3466. [Google Scholar] [CrossRef]
- Wu, S.I.; Wu, C.C.; Tsai, P.J.; Cheng, L.H.; Hsu, C.C.; Shan, I.K.; Chan, P.Y.; Lin, T.W.; Ko, C.J.; Chen, W.L.; et al. Psychobiotic Supplementation of PS128(TM) Improves Stress, Anxiety, and Insomnia in Highly Stressed Information Technology Specialists: A Pilot Study. Front. Nutr. 2021, 8, 614105. [Google Scholar] [CrossRef] [PubMed]
- Schwarcz, R.; Bruno, J.P.; Muchowski, P.J.; Wu, H.Q. Kynurenines in the mammalian brain: When physiology meets pathology. Nat. Rev. Neurosci. 2012, 13, 465–477. [Google Scholar] [CrossRef] [PubMed]
- Mörkl, S.; Narrath, M.; Schlotmann, D.; Sallmutter, M.T.; Putz, J.; Lang, J.; Brandstätter, A.; Pilz, R.; Karl Lackner, H.; Goswami, N.; et al. Multi-species probiotic supplement enhances vagal nerve function—Results of a randomized controlled trial in patients with depression and healthy controls. Gut Microbes 2025, 17, 2492377. [Google Scholar] [CrossRef] [PubMed]
- Bahrudin, M.F.; Abdul Rani, R.; Tamil, A.M.; Mokhtar, N.M.; Raja Ali, R.A. Effectiveness of Sterilized Symbiotic Drink Containing Lactobacillus helveticus Comparable to Probiotic Alone in Patients with Constipation-Predominant Irritable Bowel Syndrome. Dig. Dis. Sci. 2020, 65, 541–549. [Google Scholar] [CrossRef]
- Zhang, R.; Peng, X.; Song, X.; Long, J.; Wang, C.; Zhang, C.; Huang, R.; Lee, T.M.C. The prevalence and risk of developing major depression among individuals with subthreshold depression in the general population. Psychol. Med. 2023, 53, 3611–3620. [Google Scholar] [CrossRef]
- Juruena, M.F. Understanding subthreshold depression. Shanghai Arch. Psychiatry 2012, 24, 292–293. [Google Scholar] [CrossRef]
- Hyde, J.; Calnan, M.; Prior, L.; Lewis, G.; Kessler, D.; Sharp, D. A qualitative study exploring how GPs decide to prescribe antidepressants. Br. J. Gen. Pract. 2005, 55, 755–762. [Google Scholar]
- Fournier, J.C.; DeRubeis, R.J.; Hollon, S.D.; Dimidjian, S.; Amsterdam, J.D.; Shelton, R.C.; Fawcett, J. Antidepressant drug effects and depression severity: A patient-level meta-analysis. Jama 2010, 303, 47–53. [Google Scholar] [CrossRef]
- Mokhtar, N.M.; Bahrudin, M.F.; Abd Ghani, N.; Abdul Rani, R.; Raja Ali, R.A. Prevalence of Subthreshold Depression Among Constipation-Predominant Irritable Bowel Syndrome Patients. Front. Psychol. 2020, 11, 1936. [Google Scholar] [CrossRef]
- Altamura, C.; Maes, M.; Dai, J.; Meltzer, H.Y. Plasma concentrations of excitatory amino acids, serine, glycine, taurine and histidine in major depression. Eur. Neuropsychopharmacol. 1995, 5, 71–75. [Google Scholar] [CrossRef]
- Lima, L.; Obregón, F.; Urbina, M.; Carreira, I.; Baccichet, E.; Peña, S. Taurine concentration in human blood peripheral lymphocytes: Major depression and treatment with the antidepressant mirtazapine. Adv. Exp. Med. Biol. 2003, 526, 297–304. [Google Scholar] [PubMed]
- Rayan, N.A.; Aow, J.; Lim, M.G.L.; Arcego, D.M.; Ryan, R.; Nourbakhsh, N.; de Lima, R.M.S.; Craig, K.; Zhang, T.Y.; Goh, Y.T.; et al. Shared and unique transcriptomic signatures of antidepressant and probiotics action in the mammalian brain. Mol. Psychiatry 2024, 29, 3653–3668. [Google Scholar] [CrossRef] [PubMed]
- Kennedy, S.H.; Lam, R.W.; McIntyre, R.S.; Tourjman, S.V.; Bhat, V.; Blier, P.; Hasnain, M.; Jollant, F.; Levitt, A.J.; MacQueen, G.M.; et al. Canadian Network for Mood and Anxiety Treatments (CANMAT) 2016 Clinical Guidelines for the Management of Adults with Major Depressive Disorder: Section 3. Pharmacological Treatments. Can. J. Psychiatry 2016, 61, 540–560. [Google Scholar] [CrossRef] [PubMed]
| Psychobiotic Strains | Gut Microbiome Changes |
|---|---|
| OMNi-BiOTiC® Stress Repair: B. bifidum W23, B. lactis W51, B. lactis W52, L. acidophilus W22, L. casei W56, L. paracasei W20, L. plantarum W62, L. salivarius W24, L. lactis W19 |
|
| Ecologic® Barrier: B. bifidum W23, B. lactis W51, B. lactis W52, L. acidophilus W37, L. brevis W63, L. casei W56, L. salivarius W24, Lc. lactis W19, Lc. lactis W58 |
|
| BioKult Advanced: L. paracasei PXN37, L. plantarum PXN47, L. rhamnosus PXN54, B. subtilis PXN21, B. bifidum PXN23, B. breve PXN25, B. longum PXN30, L. helveticus PXN35, L. lactis ssp. lactis PXN63, S. thermophilus PXN66, B. infantis PXN27, L. delbruecklii ssp. bulgaricus PXN39, L. helveticus PXN45, L. salivarius PXN57 |
|
| Bifidobacterium breve CCFM1025 | |
| L. plantarum PS128 |
|
| Vivomixx®: Streptococcus thermophilus NCIMB 30438, B. breve NCIMB 30441, B. longum NCIMB 30435, B. infantis NCIMB 30436, L. acidophilus NCIMB 30442, L. plantarum NCIMB 30437, L. paracasei NCIMB 30439, L. delbrueckii susp. Bulgaricus NCIMB 30440 |
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Menni, A.-E.; Theodorou, H.; Tzikos, G.; Theodorou, I.M.; Semertzidou, E.; Stelmach, V.; Shrewsbury, A.D.; Stavrou, G.; Kotzampassi, K. Rewiring Mood: Precision Psychobiotics as Adjunct or Stand-Alone Therapy in Depression Using Insights from 19 Randomized Controlled Trials in Adults. Nutrients 2025, 17, 2022. https://doi.org/10.3390/nu17122022
Menni A-E, Theodorou H, Tzikos G, Theodorou IM, Semertzidou E, Stelmach V, Shrewsbury AD, Stavrou G, Kotzampassi K. Rewiring Mood: Precision Psychobiotics as Adjunct or Stand-Alone Therapy in Depression Using Insights from 19 Randomized Controlled Trials in Adults. Nutrients. 2025; 17(12):2022. https://doi.org/10.3390/nu17122022
Chicago/Turabian StyleMenni, Alexandra-Eleftheria, Helen Theodorou, Georgios Tzikos, Ioannis M. Theodorou, Eleni Semertzidou, Veroniki Stelmach, Anne D. Shrewsbury, George Stavrou, and Katerina Kotzampassi. 2025. "Rewiring Mood: Precision Psychobiotics as Adjunct or Stand-Alone Therapy in Depression Using Insights from 19 Randomized Controlled Trials in Adults" Nutrients 17, no. 12: 2022. https://doi.org/10.3390/nu17122022
APA StyleMenni, A.-E., Theodorou, H., Tzikos, G., Theodorou, I. M., Semertzidou, E., Stelmach, V., Shrewsbury, A. D., Stavrou, G., & Kotzampassi, K. (2025). Rewiring Mood: Precision Psychobiotics as Adjunct or Stand-Alone Therapy in Depression Using Insights from 19 Randomized Controlled Trials in Adults. Nutrients, 17(12), 2022. https://doi.org/10.3390/nu17122022