
Awareness of Eating Disorders, Nutritional Knowledge, and Emotionally Driven Eating Among Polish Adolescents Aged 15–17—A Pilot Study



Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Research Tools and Data Collection
- (a)
- Knowledge and awareness of disordered eating behaviors: anorexia nervosa (AN), bulimia nervosa (BN), binge eating disorder (BED), and avoidant/restrictive food intake disorder (ARFID).
- (b)
- Attitudes toward body image and body satisfaction.
- (c)
- Perceptions of healthy eating and understanding of concepts such as BMI and the Healthy Eating Plate.
- (d)
- The influence of emotions on food choices and the perceived impact of family, peers, and media.
- (e)
- Awareness of the importance of regular meal consumption and healthy food intake.
2.3. Statistical Analysis
3. Results
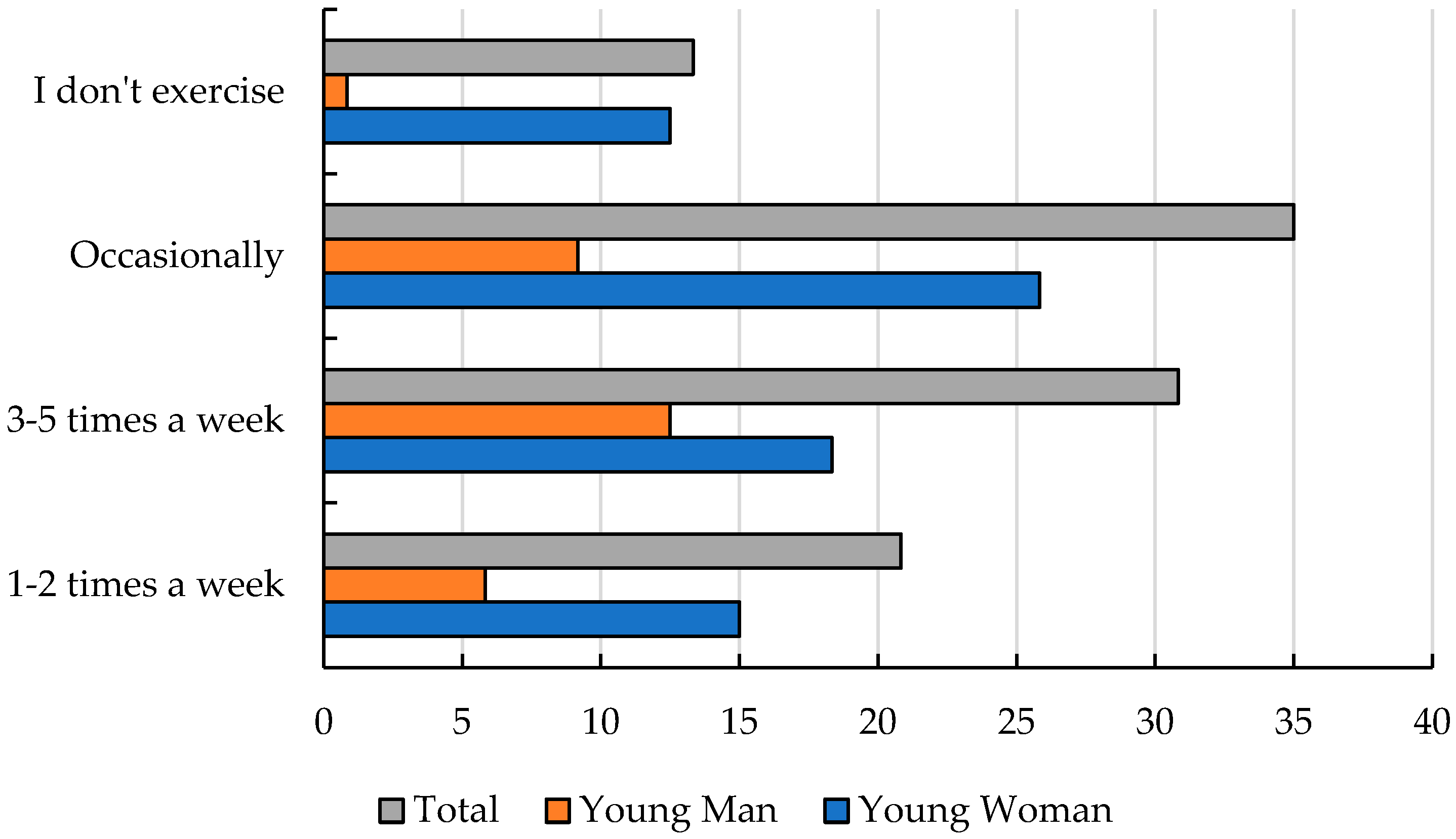
3.1. Healthy Eating and Lifestyle as a Value for Adolescents
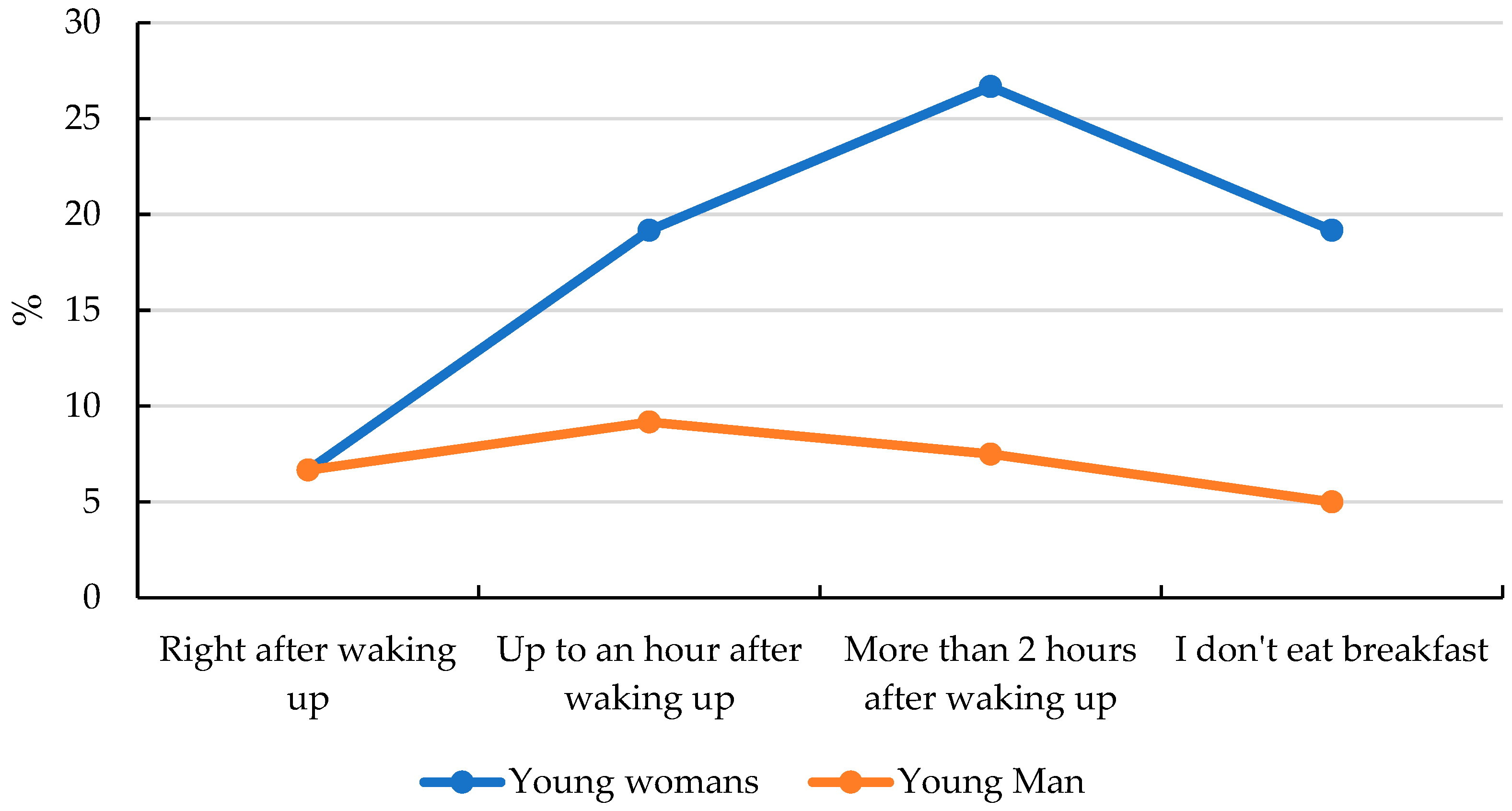
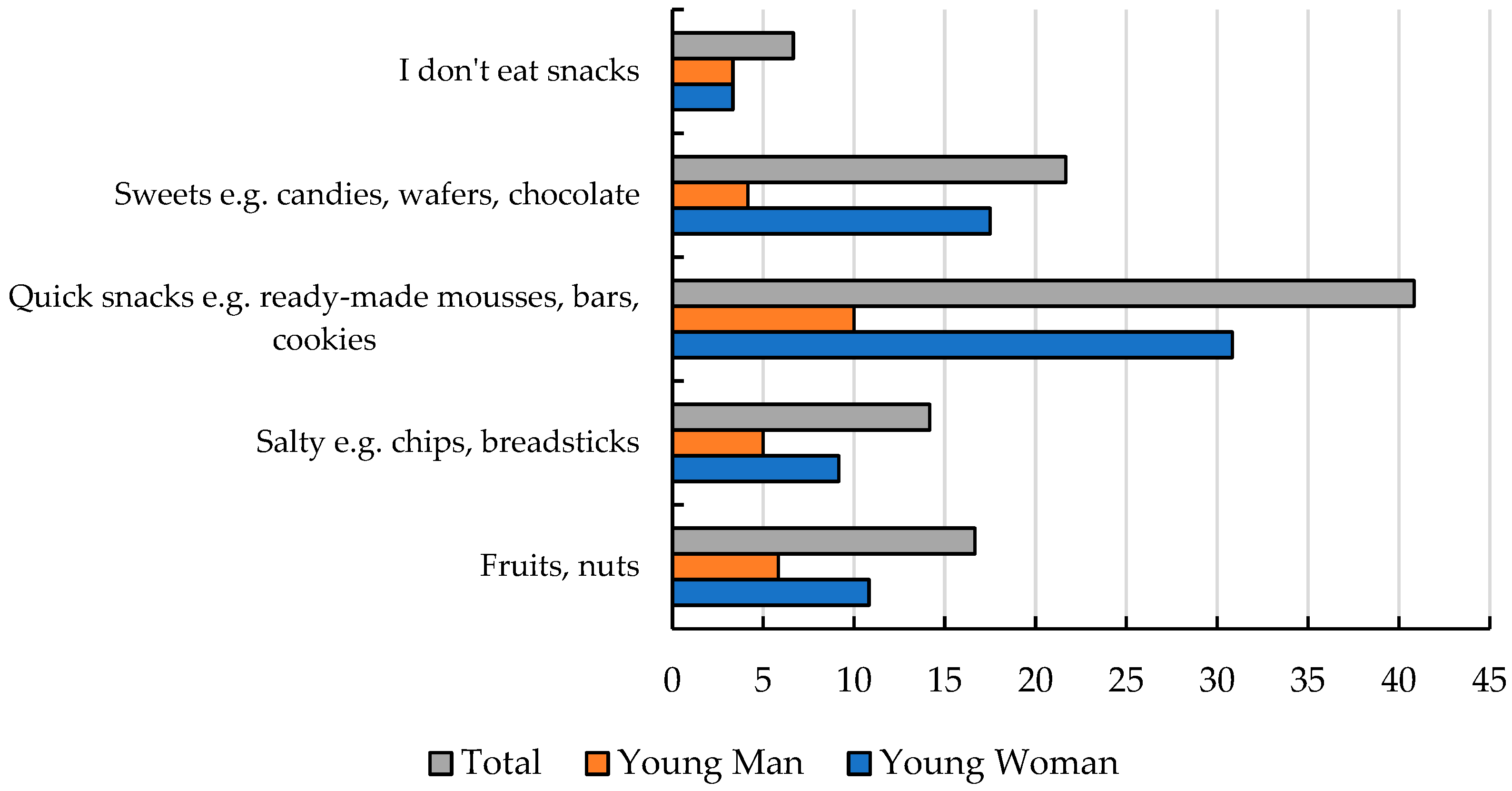
3.2. Adolescents’ Eating Behaviors and Their Attitudes Toward Nutrition
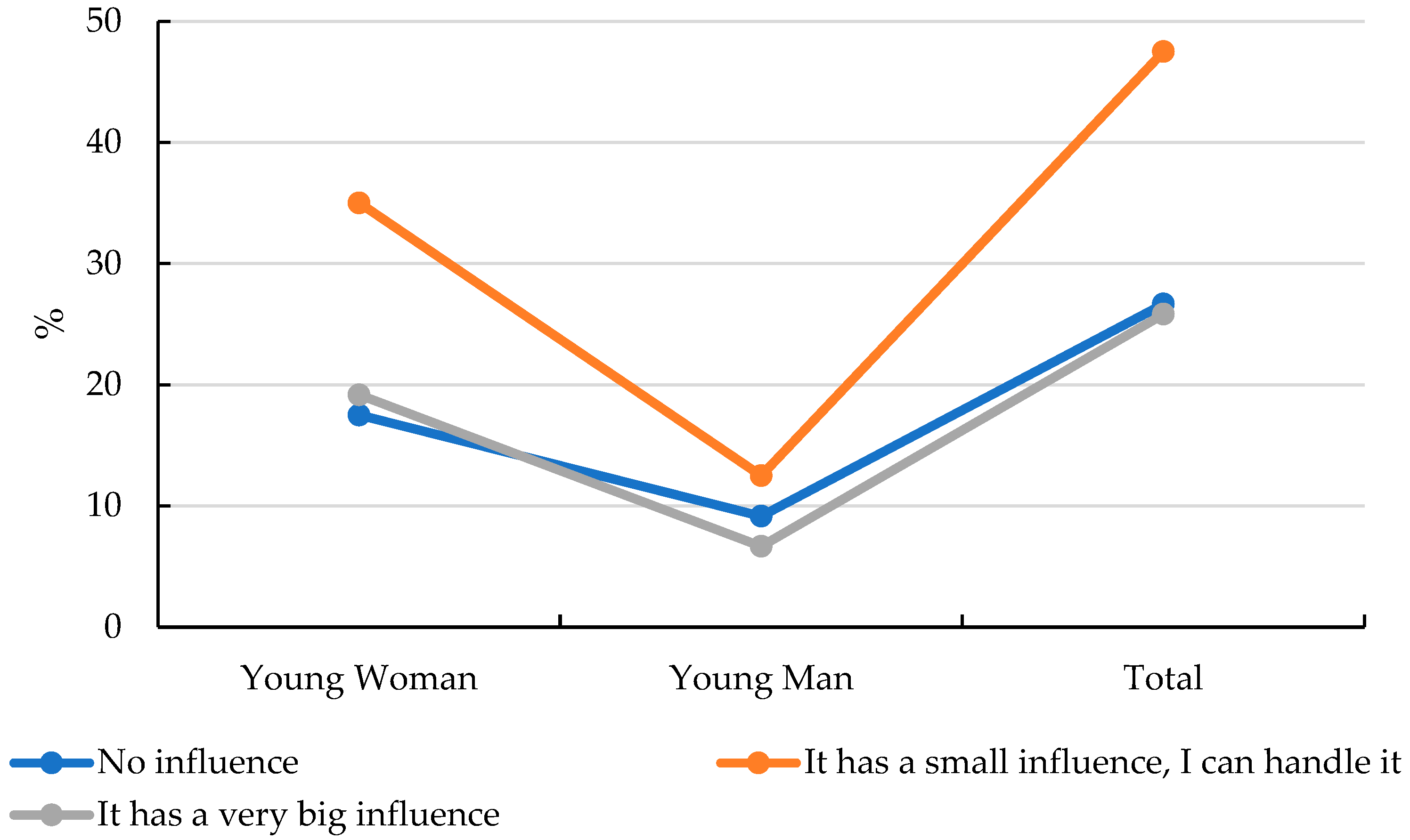
3.3. Emotionally Driven Eating and Disordered Behaviors Among Adolescents
3.4. Adolescents and Awareness of the Basics of Healthy Nutrition
4. Discussion
5. Limitation Study
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Skolmowska, D.; Głąbska, D.; Guzek, D. Relationship between food preferences and eating habits during the COVID-19 pandemic among Polish adolescents (PLACE-19 Study). Nutrients 2021, 13, 2640. [Google Scholar]
- Wawrzyniak, A.; Myszkowska-Ryciak, J.; Harton, A.; Lange, E.; Laskowski, W.; Hamulka, J.; Gajewska, D. Body dissatisfaction among Polish adolescents is associated with unhealthy dietary behaviors. Nutrients 2020, 12, 2648. [Google Scholar] [CrossRef] [PubMed]
- Friedman, V.J.; Wright, C.J.; Molenaar, A.; McCaffrey, T.; Brennan, L.; Lim, M.S. The use of social media as a persuasive platform to facilitate nutrition and health behavior change in young adults: Web-based conversation study. J. Med. Internet Res. 2022, 24, e28063. [Google Scholar] [CrossRef]
- Ciborowska, H.; Rudnicka, A. Dietetyka. In Żywienie Zdrowego i Chorego Człowieka; PZWL: Warszawa, Poland, 2007; pp. 359, 465–469. [Google Scholar]
- Jarosz, M.; Rychlik, E.; Stoś, K.; Charzewska, J. Normy Żywienia dla Populacji Polski i ich Zastosowanie; Narodowy Instytut Zdrowia Publicznego—Państwowy Zakład Higieny: Warsaw, Poland, 2020; p. 83. [Google Scholar]
- Bottin, J.H.; Morin, C.; Guelinckx, I.; Perrier, E.T. Hydration in children: What do we know and why does it matter? Ann. Nutr. Metab. 2019, 74 (Suppl. S3), 11–18. [Google Scholar] [CrossRef] [PubMed]
- James, A.; Lawrence, B.; O’Connor, M. Healthy eating as a new way of life: A qualitative study of successful long-term diet change. Inquiry 2022, 59, 00469580221090397. [Google Scholar] [CrossRef] [PubMed]
- Garaulet, M.; Canteras, M.; Morales, E.; López-Guimera, G.; Sanchez-Carracedo, D. Validation of the Emotional Eating Questionnaire (EEQ) for use in cases of obesity. Nutr. Hosp. 2012, 27, 645–651. [Google Scholar]
- Ioannidis, K.; Hook, R.W.; Grant, J.E.; Czabanowska, K.; Roman-Urrestarazu, A.; Chamberlain, S.R. Eating disorders with over-exercise: A cross-sectional analysis of the mediational role of problematic usage of the internet in young people. J. Psychiatr. Res. 2021, 132, 215–222. [Google Scholar] [CrossRef]
- Christensen, K.; Forbush, K.; Richson, B.; Thomeczek, M.; Perko, V.; Bjorlie, K.; Christian, K.; Ayres, J.; Wildes, J.; Chana, S. Food insecurity associated with elevated eating disorder symptoms, impairment, and eating disorder diagnoses in an American University student sample before and during the beginning of the COVID-19 pandemic. Int. J. Eat. Disord. 2021, 54, 1213–1223. [Google Scholar] [CrossRef]
- Stice, E.; Desjardins, C.D.; Rohde, P.; Shaw, H. Sequencing of symptom emergence in anorexia nervosa, bulimia nervosa, binge eating disorder, and purging disorder and relations of prodromal symptoms to future onset of these disorders. J. Abnorm. Psychol. 2021, 130, 377–389. [Google Scholar] [CrossRef]
- Sfärlea, A.; Radix, A.K.; Schulte-Körne, G.; Legenbauer, T.; Platt, B. Attention biases for eating disorder-related stimuli versus social stimuli in adolescents with anorexia nervosa–An eye-tracking study. Res. Child Adolesc. Psychopathol. 2023, 51, 541–555. [Google Scholar] [CrossRef]
- Szałachowski, R.R.; Tuszyńska-Bogucka, W. “Yes, in Crisis, We Pray.” The role of prayer in coping with pandemic fears. Religions 2021, 12, 824. [Google Scholar] [CrossRef]
- Eddy, K.T.; Lawson, E.A.; Hartmann, A.S.; Mancuso, C.J.; Misra, M.; Becker, K.R.; Thomas, J.J.; Plessow, F.; Slattery, M.; Murray, H.B.; et al. Implicit attitudes toward dieting and thinness distinguish fat-phobic and non-fat-phobic anorexia nervosa from avoidant/restrictive food intake disorder in adolescents. Int. J. Eat. Disord. 2019, 52, 419–427. [Google Scholar]
- Franko, D.L.; Eddy, K.T.; Liebman, R.E.; Keshishian, A.C.; Coniglio, K.A.; Wang, S.B.; Thomas, J.J.; Becker, K.R. Impact of expanded diagnostic criteria for avoidant/restrictive food intake disorder on clinical comparisons with anorexia nervosa. Int. J. Eat. Disord. 2019, 52, 230–238. [Google Scholar]
- Karakuła-Juchnowicz, H.; Pankowicz, H.; Juchnowicz, D.; Piedra, J.L.V.; Małecka-Massalska, T. Gut microbiota—The key to understanding the pathophysiology of anorexia nervosa. Psychiatr. Pol. 2017, 51, 859–870. [Google Scholar] [CrossRef]
- Garber, A.K.; Cheng, J.; Accurso, E.C.; Adams, S.H.; Buckelew, S.M.; Kapphahn, C.J.; Kreiter, A.; Le Grange, D.; Machen, V.I.; Moscicki, A.B.; et al. Short-term outcomes of the study of refeeding to optimize inpatient gains for patients with anorexia nervosa: A multicenter randomized clinical trial. JAMA Pediatr. 2021, 175, 19–27. [Google Scholar] [CrossRef] [PubMed]
- Pettersson, C.; Svedlund, A.; Wallengren, O.; Swolin-Eide, D.; Karlsson, G.P.; Ellegård, L. Dietary intake and nutritional status in adolescents and young adults with anorexia nervosa: A 3-year follow-up study. Clin. Nutr. 2021, 40, 5391–5398. [Google Scholar] [CrossRef] [PubMed]
- Malara, B.; Jośko, J.; Kasperczyk, J.; Kamecka-Krupa, J. Rozpowszechnienie zaburzeń odżywiania wśród młodzieży w wybranych miastach województwa śląskiego. Probl. Hig. Epidemiol. 2010, 91, 388–392. [Google Scholar]
- World Medical Association. World Medical Association Declaration of Helsinki: Ethical principles for medical research involving human subjects. JAMA 2013, 310, 2191–2194. [Google Scholar] [CrossRef]
- Suhag, K.; Rauniyar, S. The influence of social media on eating disorders and body image in young adolescents. Cureus 2024, 16, e58674. [Google Scholar]
- Guzek, D.; Głąbska, D.; Skolmowska, D. Emotional eating among Polish adolescents and its association with the COVID-19 pandemic. Nutrients 2021, 13, 1022. [Google Scholar]
- Kotowska, A.; Sochacka, K.; Wiśniewski, R.; Lachowicz-Wiśniewska, S. Dietary habits of young Poles and their selected determinants: A review and implications for public health. Nutrients 2024, 16, 3561. [Google Scholar] [CrossRef] [PubMed]
- Jeżewska-Zychowicz, M.; Małachowska, A.; Sajdakowska, M.; Żybula, Z. Childhood dietary restrictions for health and weight control and their associations with restrained eating and excessive body weight in young adults in Poland—A cross-sectional study. Nutrients 2024, 16, 450. [Google Scholar]
- López-Gil, J.; García-Hermoso, A.; Smitch, L. Global Proportion of Disordered Eating in Children and Adolescents: A Systematic Review and Meta-analysis. JAMA Pediatr. 2023, 177, 363–372. [Google Scholar] [CrossRef]
- Olsen, E.; Koch, S.; Skovgaard, A.; Strandberg-Larsen, K. Self-reported binge eating symptoms among adolescents in a community-based Danish cohort: Prevalence, correlates, and impact. Int. J. Eat. Disord. 2020, 53, 1272–1283. [Google Scholar] [CrossRef]
- Al-Sheyab, N.; Gharaibeh, T.; Kheirallah, K.A. Peer pressure and risk of disordered eating among adolescents in Jordan. J. Obes. 2018, 2018, 6747649. [Google Scholar] [CrossRef]
- Kovács-Tóth, B.; Oláh, B.; Szabó, I.; Túry, F. Adverse childhood experiences increase the risk of eating disorders among adolescents. Front. Psychol. 2022, 13, 902137. [Google Scholar] [CrossRef] [PubMed]
- Ispas, A.; Forray, A.; Lacurezeeanu, A.; Petreus, D.; Gavrillas, L.; Chereches, R. Eating Disorder Risk Among Adolescents: The Influence of Dietary Patterns, Physical Activity, and BMI. Nutrients 2025, 17, 1067. [Google Scholar] [CrossRef]
- Katzman, D.K. The COVID-19 pandemic and eating disorders: A warning about the future. J. Adolesc. Health 2021, 68, 5–6. [Google Scholar]
- Sung, J.; Hong, J.; Kim, J.; Jung, J.; Choi, S.; Kang, J.; Han, M. Watching Mukbang and Cookbang and dietary behaviors among Korean adolescents. Nutr. Res. Pract. 2024, 18, 523–533. [Google Scholar] [CrossRef]
- Park, E.; Hwang, S.; Lee, M.; Bhang, S. Does food addiction and emotional eating behavior co-exist with smartphone use problems among adolescents? Int. J. Environ. Res. Public Health 2022, 19, 4939. [Google Scholar] [CrossRef]
- Nawaz, F.; Riaz, M.; Banday, N.U.A.; Singh, A.; Arshad, Z.; Derby, H.; Sultan, M. Social media use among adolescents with eating disorders: A double-edged sword. Front. Psychiatry 2024, 15, 123456. [Google Scholar] [CrossRef] [PubMed]
- Jośko, J.; Kamecka-Krupa, J. Czynniki kulturowe i społeczne predysponujące do zaburzeń odżywiania u młodzieży szkolnej w wybranych miastach województwa śląskiego. Probl. Hig. Epidemiol. 2007, 88, 320–326. [Google Scholar]
- Trafalska, E.; Niedźwiedzka, M.; Nowacka, E. Czynniki ryzyka zaburzeń odżywiania wśród młodzieży łódzkiej—Postrzeganie i kontrola masy ciała. Probl. Hig. Epidemiol. 2010, 91, 602–605. [Google Scholar]
- Sochacka-Tatara, E.; Stypuła, A. Zaburzenia odżywiania wśród młodzieży uczniów szkół krakowskich—Część ogólnopolskich badań zaburzeń odżywiania wśród młodzieży. Probl. Hig. Epidemiol. 2010, 91, 591–595. [Google Scholar]
- Saitz, R.; Horton, N.J.; Sullivan, L.M.; Moskowitz, M.A.; Samet, J.H. Addressing Alcohol Problems in Primary Care: A Cluster Randomized, Controlled Trial of a Systems Intervention. Ann. Intern. Med. 2003, 138, 372–382. [Google Scholar] [CrossRef] [PubMed]
- Bilson, J.; Sethi, J.K.; Byrne, C.D. Non-Alcoholic Fatty Liver Disease: A Multi-System Disease Influenced by Ageing and Sex, and Affected by Adipose Tissue and Intestinal Function. Proc. Nutr. Soc. 2022, 81, 146–161. [Google Scholar] [CrossRef] [PubMed]
- Pelc, A.; Winiarska, M.; Polak-Szczybyło, E.; Godula, J.; Stępień, A. Low self-esteem and life satisfaction as significant risk factors of eating disorders among adolescents. Nutrients 2023, 15, 1832. [Google Scholar] [CrossRef]
- Tian, H.-H.; Aziz, A.-R.; Png, W.; Wahid, M.F.; Yeo, D.; Png, A.-L.C. Effects of Fasting During Ramadan on Cognitive Function in Muslim Athletes. Asian J. Sports Med. 2011, 2, 145–153. [Google Scholar] [CrossRef]
- Schroder, H.; Zomeno, M.D.; Martinez-Gonzalez, M.A.; Salas-Salvado, J.; Corella, D.; Vioque, J.; Romaguera, D.; Martínez, J.A.; Tinahones, F.J.; Miranda, J.L.; et al. Validity of the Energy-Restricted Mediterranean Diet Adherence Screener. Clin. Nutr. 2021, 40, 4971–4979. [Google Scholar] [CrossRef]
- Kasperczyk, J.; Jośko, J.; Bilska, J. Eating habits and selected healthy lifestyle factors among secondary school students. Probl. Hig. Epidemiol. 2007, 88, 157–161. [Google Scholar]
- Mizia, S.; Felinczak, A.; Włodarek, D.; Syrkiewicz-Świtała, M. Evaluation of eating habits and their impact on health among adolescents and young adults: A cross-sectional study. Int. J. Environ. Res. Public Health 2021, 18, 3996. [Google Scholar] [CrossRef] [PubMed]
- Białek-Dratwa, A.; Staśkiewicz-Bartecka, W.; Kiciak, A.; Wardyniec, A.; Grajek, M.; Aktaç, Ş.; Çelik, Z.; Sabuncular, G.; İslamoğlu, A.; Kowalski, O. Food neophobia and avoidance/restriction of food intake among adults and associated factors. Nutrients 2024, 16, 850. [Google Scholar] [CrossRef]
- Vilagut, G.; Ferrer, M.; Rajmil, L.; Rebollo, P.; Permanyer-Miralda, G.; Quintana, J.M.; Santed, R.; Valderas, J.M.; Ribera, A.; Domingo-Salvany, A.; et al. The Spanish version of the SF-36 Health Questionnaire: A decade of experience and new developments. Gac. Sanit. 2005, 19, 135–150. [Google Scholar] [CrossRef] [PubMed]
- Wawrzyniak, A.; Pietruszka, B. Dietary habits and nutritional status of different population groups in relation to lifestyle factors and nutritional knowledge. Nutrients 2023, 15, 4609. [Google Scholar] [CrossRef] [PubMed]
- Liu, T.; Li, N.; Hou, Z.; Liu, L.; Gao, L.; Wang, L.; Tan, J. Nutrition and Exercise Interventions Could Ameliorate Age-Related Cognitive Decline: A Meta-Analysis of Randomized Controlled Trials. Aging Clin. Exp. Res. 2021, 33, 1799–1809. [Google Scholar] [CrossRef]
- Całyniuk, B.; Górski, M.; Garbicz, J.; Grochowska-Niedworok, E. Nutrition knowledgle of people with etaing disorders. Rocz. Państwowego Zakładu Higieny 2019, 70, 41–48. [Google Scholar] [CrossRef]
- Mushtaq, T.; Aszraf, S.; Hameed, H.; Irfan, A.; Szahid, M.; Kanwal, R.; Aslam, M.; Szahid, H.; Noor, K.; Shazly, G.; et al. Prevalence of Eating Disorders and Their Association with Social Media Addiction among Youths. Nutrients 2023, 15, 4687. [Google Scholar] [CrossRef]
- Stich, F.M.; Huwiler, S.; D’Hulst, G.; Lustenberger, C. The Potential Role of Sleep in Promoting a Healthy Body Composition: Underlying Mechanisms Determining Muscle, Fat, and Bone Mass and Their Association with Sleep. Neuroendocrinology 2021, 112, 673–701. [Google Scholar] [CrossRef]
- Larsson, S.; Agneta, A.; Wolk, A. Sweetened Beverage Consumption Is Associated with Increased Risk of Stroke in Women and Men. J. Nutr. 2014, 144, 856–860. [Google Scholar] [CrossRef]
- Thompson, A.; Moughan, P. Innovation in the Food Industry: Functional Foods. Innov. Manag. Policy Pract. 2008, 10, 61–73. [Google Scholar] [CrossRef]
- Mohamed, O.G.; Fareen, M.F.K.; Zaman, S.; Salmasi, A.M.; Tsilidis, K.; Dehghan, A. Intermittent fasting for the prevention of cardiovascular disease. Cochrane Database Syst. Rev. 2021, 1, CD013496. [Google Scholar]
- Innes, J.K.; Calder, P.C. Marine Omega-3 (N-3) Fatty Acids for Cardiovascular Health: An Update for 2020. Int. J. Mol. Sci. 2020, 21, 1362. [Google Scholar] [CrossRef] [PubMed]
- Grabe, S.; Ward, L.M.; Hyde, J.S. The Role of the Media in Body Image Concerns Among Women: A Meta-Analysis of Experimental and Correlational Studies. Psychol. Bull. 2008, 134, 460–476. [Google Scholar] [CrossRef] [PubMed]
- Kahleova, H.; Belinova, L.; Malinska, H.; Oliyarnyk, O.; Trnovska, J.; Skop, V.; Kazdova, L.; Dezortova, M.; Hajek, M.; Tura, A.; et al. Eating Two Larger Meals a Day (Breakfast and Lunch) Is More Effective than Six Smaller Meals in a Reduced-Energy Regimen for Patients with Type 2 Diabetes: A Randomised Crossover Study. Diabetologia 2014, 57, 1552–1556. [Google Scholar] [CrossRef]
- Lunsford-Avery, J.R. Light Regularity: Illuminating Opportunities to Enhance Adolescent Health. Sleep 2023, 46, zsad086. [Google Scholar] [CrossRef]
- DiNicolantonio, J.J.; O’Keefe, J. The Importance of Maintaining a Low Omega-6/Omega-3 Ratio for Reducing the Risk of Autoimmune Diseases, Asthma, and Allergies. Mo. Med. 2021, 118, 453–459. [Google Scholar]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total | Young Woman | Young Man | ||
|---|---|---|---|---|
| Characteristics | N = 120 | N = 87 | N = 33 | |
| Age | arithmetic mean [years] | 16.2 | 16.2 | 16.2 |
| variance [years] | 0.5 | 0.5 | 0.5 | |
| standard deviation [years] | 0.7 | 0.7 | 0.7 | |
| coefficient of variation [%] | 4.4 | 4.5 | 4.3 | |
| Age distribution | 15 years | 20 | 15 | 5 |
| 16 years | 51 | 35 | 16 | |
| 17 years | 49 | 37 | 12 | |
| Place of residence | village | 45 | 32 | 13 |
| small town | 37 | 28 | 9 | |
| medium-sized town | 33 | 25 | 8 | |
| large city | 5 | 2 | 3 | |
| Body mass index (kg/m2) | <18.0 | 26 | 21 | 5 |
| 18.5–25.0 | 91 | 64 | 27 | |
| >25.0 | 3 | 2 | 1 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zięba, M.; Jaskuła, M.; Lachowicz-Wiśniewska, S. Awareness of Eating Disorders, Nutritional Knowledge, and Emotionally Driven Eating Among Polish Adolescents Aged 15–17—A Pilot Study. Nutrients 2025, 17, 1994. https://doi.org/10.3390/nu17121994
Zięba M, Jaskuła M, Lachowicz-Wiśniewska S. Awareness of Eating Disorders, Nutritional Knowledge, and Emotionally Driven Eating Among Polish Adolescents Aged 15–17—A Pilot Study. Nutrients. 2025; 17(12):1994. https://doi.org/10.3390/nu17121994
Chicago/Turabian StyleZięba, Marlena, Marta Jaskuła, and Sabina Lachowicz-Wiśniewska. 2025. "Awareness of Eating Disorders, Nutritional Knowledge, and Emotionally Driven Eating Among Polish Adolescents Aged 15–17—A Pilot Study" Nutrients 17, no. 12: 1994. https://doi.org/10.3390/nu17121994
APA StyleZięba, M., Jaskuła, M., & Lachowicz-Wiśniewska, S. (2025). Awareness of Eating Disorders, Nutritional Knowledge, and Emotionally Driven Eating Among Polish Adolescents Aged 15–17—A Pilot Study. Nutrients, 17(12), 1994. https://doi.org/10.3390/nu17121994