
Analysis of Compliance with Proper Nutrition Principles in Patients with a History of Myocardial Infarction

 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Population
2.2. Applied Measurements
2.3. Data Analysis
3. Results
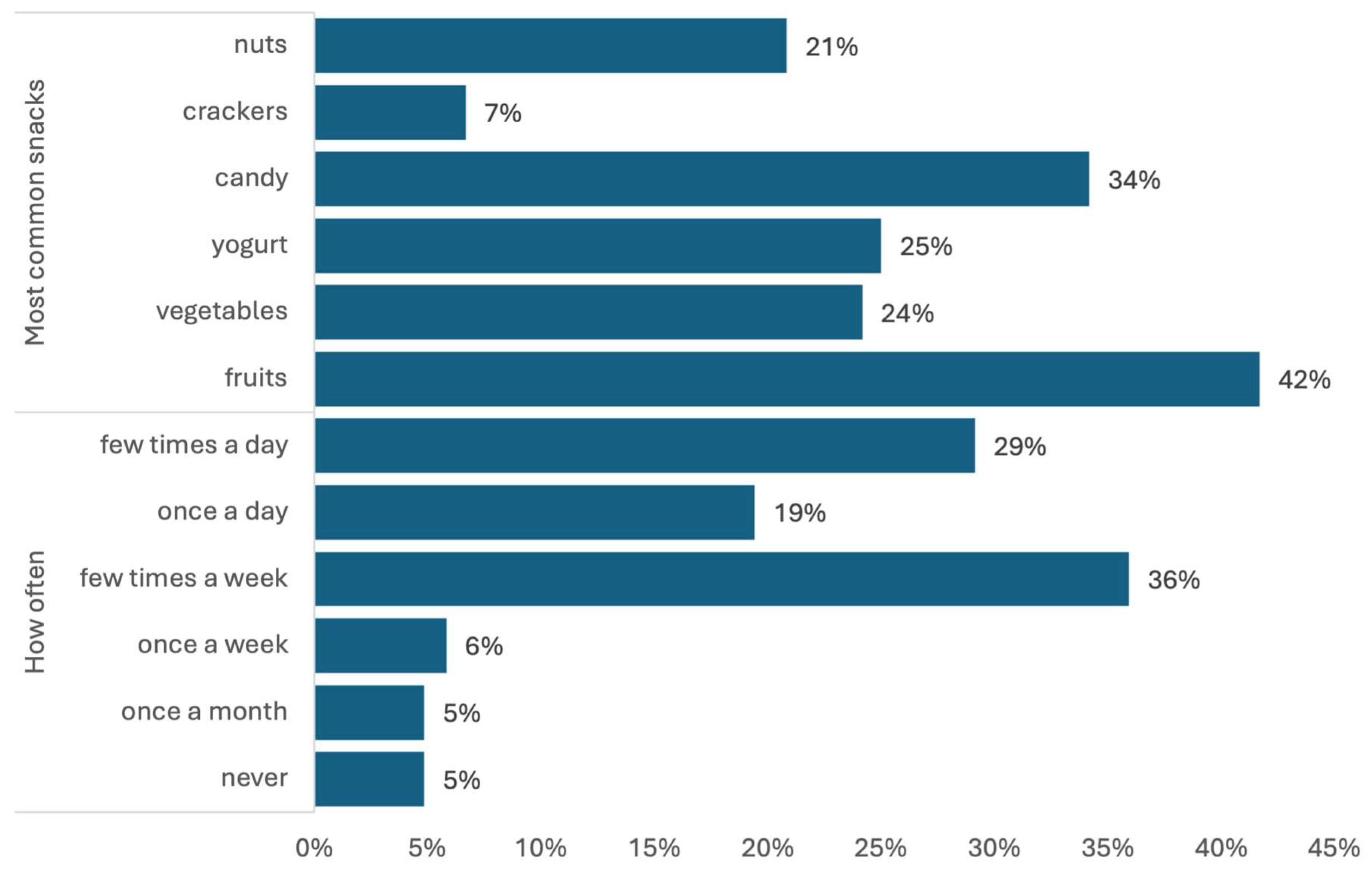
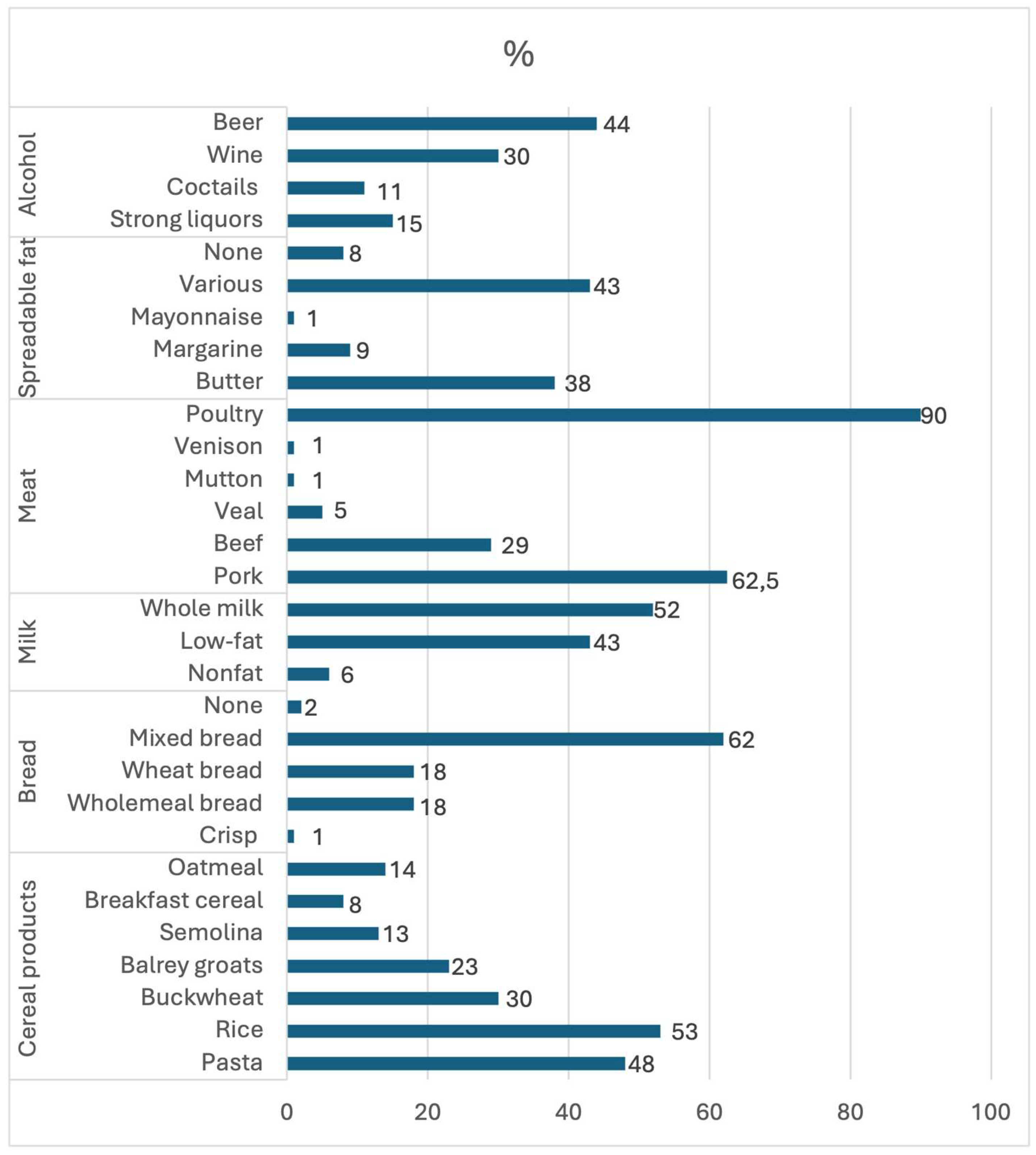
3.1. Analysis of Eating Habits, the Products Consumed, and the Frequency of Consumption
3.2. Respondents’ Knowledge of Nutrition
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Thygesen, K.; Alpert, J.S.; Jaffe, A.S.; Chaitman, B.R.; Bax, J.J.; Morrow, D.A.; White, H.D. Fourth universal definition of myocardial infarction (2018). Circulation 2018, 138, e618–e651. [Google Scholar] [CrossRef] [PubMed]
- Jayaraj, J.C.; Davatyan, K.; Subramanian, S.S.; Pryia, J. Epidemiology of Myocardial Infarction. In Myocardial Infarction; Pamukçu, B., Ed.; IntechOpen: London, UK, 2019; pp. 9–14. ISBN 1789848687/9781789848687. [Google Scholar] [CrossRef]
- Mahajan, S.; Valero-Elizondo, J.; Khera, R.; Desai, N.R.; Blankstein, R.; Blaha, M.J.; Virani, S.S.; Kash, B.A.; Zoghbi, W.A.; Krumholz, H.M.; et al. Variation and Disparities in Awareness of Myocardial Infarction Symptoms among Adults in the United States. JAMA Netw. Open 2019, 2, e1917885. [Google Scholar] [CrossRef] [PubMed]
- Ojha, N.; Dhamoon, A.S. Myocardial Infarction; StatPearls Publishing: Treasure Island, FL, USA, 2024. Available online: https://www.ncbi.nlm.nih.gov/books/NBK537076/ (accessed on 20 May 2024).
- Kochar, A.; Chen, A.Y.; Sharma, P.P.; Pagidipati, N.J.; Fonarow, G.C.; Cowper, P.A.; Roe, M.T.; Peterson, E.D.; Wang, T.Y. Long-Term Mortality of Older Patients with Acute Myocardial Infarction Treated in US Clinical Practice. J. Am. Heart Assoc. 2018, 7, e007230. [Google Scholar] [CrossRef] [PubMed]
- Szczepańska, E.; Białek-Dratwa, A.; Filipów, K.; Kowalski, O. Lifestyle and the risk of acute coronary event: A retrospective study of patients after myocardial infarction. Front. Nutr. 2023, 10, 1203841. [Google Scholar] [CrossRef]
- Almazán-Ávila, M.A. Cardiovascular risk factors in young Mexican adults. Arch. Cardiol. Méx. 2020, 90, 427–435. [Google Scholar] [CrossRef]
- Cardiovascular Diseases (CVDs). World Health Organisation. 2021. Available online: https://www.who.int/news-room/fact-sheets/detail/cardiovascular-diseases-(cvds) (accessed on 20 May 2024).
- Bortkiewicz, A.; Gadzicka, E.; Siedlecka, J.; Szyjkowska, A.; Viebig, P.; Wranicz, J.K.; Kurpesa, M.; Trzos, E.; Makowiec-Dąbrowska, T. Dietary Habits and Myocardial Infarction in Occupationally Active Men. Int. J. Occup. Med. Environ. Health 2019, 32, 853–863. [Google Scholar] [CrossRef]
- Mizia, S.; Felińczak, A.; Włodarek, D.; Syrkiewicz-Świtała, M. Evaluation of Eating Habits and Their Impact on Health among Adolescents and Young Adults: A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2021, 18, 3996. [Google Scholar] [CrossRef]
- Waldowska, A.; Stasiewicz, B. Procedura Opracowania Danych Żywieniowych z Kwestionariusza QEB. 2014. Available online: https://www.researchgate.net/publication/271653184_Procedura_opracowania_danych_zywieniowych_z_kwestionariusza_QEB (accessed on 2 August 2024).
- Alanazi, A.; Alghanim, M.H.; Alamer, A.J.; Alshaqaqiq, M.A.; Al Busaeed, M.M.; Alahmed, A.H.; Alali, A.I.; Almazyadi, H.; Alharbi, W.F.; Nasser, I.A.; et al. Acute Myocardial Infarction Patients’ Knowledge Regarding the Modifiable Risk Factors of Heart Disease. Int. J. Pharm. Res. Allied Sci. 2020, 9, 210–216. [Google Scholar]
- Luhana, R.B. Evaluation of compliance to “Discharge Instruction” among Post Myocardial Infarction Patients at Teaching Hospital Hyberabad, Pakistan. J. Univ. Med. Dent. Coll. 2023, 15, 775–780. [Google Scholar] [CrossRef]
- Lee, Y.; Kim, R.B.; Lee, H.J.; Kim, K.; Shin, M.; Park, H.; Ahn, S.-K.; Kim, S.Y.; Lee, Y.-H.; Kim, B.-G.; et al. Relationships among medication adherence, lifestyle modification, and health-related quality of life in patients with acute myocardial infarction: A cross-sectional study. Health Qual. Life Outcomes 2018, 16, 100. [Google Scholar] [CrossRef]
- Strömbäck, U.; Vikman, I.; Lundblad, D.; Lundqvist, R.; Engström, Å. The second myocardial infarction: Higher risk factor burden and earlier second myocardial infarction in women compared with men. The Northern Sweden MONICA study. Eur. J. Cardiovasc. Nurs. 2017, 16, 418–424. [Google Scholar] [CrossRef] [PubMed]
- Pakhare, M.; Anjankar, A. Critical Correlation Between Obesity and Cardiovascular Diseases and Recent Advancements in Obesity. Cureus 2024, 16, e51681. [Google Scholar] [CrossRef] [PubMed]
- Otterstad, J.E.; Munkhaugen, J.; Ruddox, V.; Edvardsen, T.; Hjelmesaeth, J. Association of normal body mass index and weight loss with long-term major cardiovascular events after PCI for myocardial infarction. Scand. Cardiovasc. J. 2024, 58, 2386984. [Google Scholar] [CrossRef] [PubMed]
- Park, S.; Kim, D.-W.; Lee, K.; Park, M.; Chang, K.; Jeong, M.H.; Ahn, Y.K.; Chae, S.C.; Ahn, T.H.; Rha, S.W.; et al. Association between body mass index and three-year outcome of acute myocardial infarction. Sci. Rep. 2024, 14, 365. [Google Scholar] [CrossRef] [PubMed]
- Taftian, M.; Sasanfar, B.; Sarebanhassanabadi, M.; Seyedhosseini, S.; Khayyatzadeh, S.S.; Madadizadeh, F.; Motallaei, M.; Beigrezaei, S.; Golvardi-Yazdi, F.; Mirjalili, F.; et al. The association between dietary meal intake habits and coronary artery stenosis and cardio-metabolic risk factors. BMC Nutr. 2024, 10, 86. [Google Scholar] [CrossRef]
- Li, K.; Song, H.; Wei, F.; Liu, D.; Zhao, Y.; Yin, H.; Cui, Y.; Zhang, H.; Liu, Z. High salt intake damages myocardial viability and induces cardiac remodeling via chronic inflammation in the elderly. Front. Cardiovasc. Med. 2022, 9, 952691. [Google Scholar] [CrossRef]
- Almohammadi, R.A. A Predictor for Decreased Left Ventricular Ejection Fraction in Patients Present to the Emergency Room with Non St Segment Elevation Myocardial Infarction. Cardiol. Cardiovasc. Med. 2024, 8, 89–93. [Google Scholar] [CrossRef]
- Nikiforov, I.; Shah, C.; Kanukuntla, A.K.; Vanjarapu, J.M.R.; Singh, P.; Tadepalii, S.; Cheriyath, P.; Nookala, V. Salt Consumption and Myocardial Infarction: Is Limited Salt Intake Beneficial? Cureus 2021, 13, e13072. [Google Scholar] [CrossRef]
- Bodén, S.; Wennberg, M.; Van Guelpen, B.; Johansson, I.; Lindahl, B.; Andersson, J. Dietary inflammatory index and risk of first myocardial infarction; a prospective population-based study. Nutr. J. 2017, 16, 21. [Google Scholar] [CrossRef]
- Tessitore, E.; Branca, M.; Heg, D.; Nanchen, D.; Auer, R.; Räber, L.; Klingenberg, R.; Windecker, S.; Lüscher, T.F.; Carballo, S.; et al. Drinking patterns of alcohol and risk of major adverse cardiovascular events after an acute coronary syndrome. Eur. J. Prev. Cardiol. 2024, 31, 845–855. [Google Scholar] [CrossRef]
- Dahanayake, D.N.; Yoosoof, F.; Chathuranga, K.M.N.T.; Jayakody, C.P.; Janadari, W.D.B.C.; Pelden, K.; Saranapala, I.U.; Ruwanpathirana, G.K.; Shamith, M.L.M. A cross-sectional study of the knowledge of post-myocardial infarction patients in a low-middle-income country regarding myocardial infarction and adherence to secondary preventive strategies practices. Indian J. Med. Sci. 2022, 75, 29–37. [Google Scholar] [CrossRef]
- Ghisi, G.L.D.M.; Rouleaus, F.; Ross, M.-K.; Dufour-Doiron, M.; Bellivea, S.L.; Brideua, J.-R.; Aultman, C.; Thomas, S.; Colella, T.; Oh, P. Effectiveness of an Education Intervention among Cardiac Rehabilitation Patients in Canada: A Multi-Site Study. CJC Open 2020, 2, 214–221. [Google Scholar] [CrossRef] [PubMed]
- Dandan, C.; Zhang, H.; Shao, J.; Tang, L.; Cui, N.; Wang, X.; Wu, J.; Wang, D.; Ye, Z. Determinants of adherence to diet and exercise behaviours among individuals with metabolic syndrome based on the Capability, Opportunity, Motivation, and Behaviour model: A cross-sectional study. Eur. J. Cardiovasc. Nurs. 2023, 22, 193–200. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Variables | n (%) | |
|---|---|---|
| Gender | Female | 62 (51.67) |
| Male | 58 (48.33) | |
| Marital status | Single/widowed/divorced | 39 (32.5) |
| Married/cohabiting | 81 (67.5) | |
| Education | Primary | 11 (9.17) |
| Vocational | 26 (21.67) | |
| Secondary | 60 (50) | |
| Higher | 23 (19.17) | |
| Employment status | Active | 41 (34.17) |
| Retirement | 74 (61.67) | |
| Pension | 3 (2.50) | |
| Other | 2 (1.67) | |
| Place of residence | City | 86 (71.67) |
| Countryside | 34 (28.33) | |
| Living with family | Yes | 96 (80.0) |
| No | 24 (20.0) | |
| Age, m (SD) | 65, 12 (10.56) | |
| Height, m (SD) | 168, 92 (9.12) | |
| Weight, m (SD) | 81, 27 (15.98) | |
| BMI, m (SD) | 28, 39 (4.72) | |
| Most common comorbidities | ||
| Circulatory System | 70 (58.33) | |
| Respiratory system | 10 (8.33) | |
| Digestive system | 18 (15.0) | |
| Osteoarticular system | 26 (21.67) | |
| Genitourinary system | 23 (19.17) | |
| Neurological | 5 (4.17) | |
| Cancer | 4 (3.33) | |
| Ocular | 26 (21.67) | |
| Auditory | 13 (10.83) | |
| Metabolic | 18 (15.0) | |
| Other | 5 (4.17) | |
| None | 17 (14.17) | |
| Patients’ Cardiac Details | n (%) | ||
|---|---|---|---|
| Number of MIs | One | 106 (88.33) | |
| Two | 11 (9.17) | ||
| More than two | 3 (2.50) | ||
| Time since first MI | Up to six months | 67 (55.83) | |
| A year | 27 (22.5) | ||
| Over a year | 14 (11.67) | ||
| Several years | 12 (10.0) | ||
| Cardiac rehabilitation | Yes | 47 (39.17) | |
| No | 73 (60.83) | ||
| Cardiac interventions performed within a year | Angioplasty | 15 (12.5) | |
| Pharmacotherapy | 22 (18.33) | ||
| Pacemaker | 2 (1.67) | ||
| PCI | 81 (67.5) | ||
| Compliance to recommendations | If feeling unwell | 41 (34.17) | |
| Consistently | 79 (65.83) | ||
| Self-measurement of blood pressure | Yes | 63 (52.5) | |
| No | 57 (47.5) | ||
| Variables | n = 120 | |
|---|---|---|
| Number of meals per day, % | 1 | 1 |
| 2 | 5 | |
| 3 | 33 | |
| 4 | 51 | |
| 5 or more | 10 | |
| Eating at regular times, % | Yes, always | 14 |
| Yes, some meals | 38 | |
| No | 48 | |
| Snacking, % | Yes | 81 |
| No | 19 | |
| Adding salt to dishes, % | Yes | 8 |
| Sometimes | 53 | |
| No | 39 | |
| Diet index, (times/day) M(SD) | Health-promoting | 3.30 (1.38) |
| Unhealthy | 1.65 (1.07) | |
| Intensity of the health-promoting diet index, % | Moderate | 10 |
| Low | 90 | |
| Intensity of the unhealthy diet index, % | Moderate | 2 |
| Low | 98 | |
| Self-assessment of diet, % | Very good | 3 |
| Good | 78 | |
| Bad | 18 | |
| Very bad | 2 | |
| Self-assessment of nutritional knowledge, % | Very good | 2 |
| Good | 34 | |
| Sufficient | 53 | |
| Insufficient | 12 | |
| Nutrition knowledge sources, % | Home | 69 |
| Advertisements | 36 | |
| Internet | 28 | |
| Press | 26 | |
| Radio | 19 | |
| Doctor | 15 | |
| School | 3 | |
| Foods | Frequency of Consumption, % | |||||
|---|---|---|---|---|---|---|
| A Few Times a Day | Once a Day | Several Times a Week | Once a Week | One to Three Times a Month | Never | |
| Vegetables | 14 | 18 | 58 | 6 | 3 | 0 |
| Fruits | 17 | 23 | 52 | 6 | 3 | 0 |
| Legumes | 0 | 2 | 12 | 27 | 57 | 3 |
| Wholemeal bread | 3 | 13 | 17 | 19 | 28 | 21 |
| Canned meat | 1 | 2 | 17 | 13 | 52 | 16 |
| Fish | 0 | 1 | 13 | 23 | 58 | 5 |
| Hard cheeses | 2 | 5 | 51 | 18 | 18 | 8 |
| Quark cheeses | 1 | 4 | 45 | 30 | 18 | 3 |
| Milk | 5 | 9 | 43 | 11 | 17 | 16 |
| Dairy drinks | 0 | 4 | 49 | 25 | 19 | 3 |
| Fried dishes | 0 | 6 | 45 | 22 | 26 | 2 |
| Fast food | 0 | 0 | 5 | 6 | 40 | 49 |
| Preserves | 3 | 11 | 68 | 13 | 5 | 1 |
| Sweets | 3 | 17 | 40 | 18 | 20 | 2 |
| Alcohol | 0 | 2 | 8 | 11 | 52 | 28 |
| Energy drinks | 1 | 0 | 3 | 3 | 5 | 88 |
| Carbonated drinks | 0 | 2 | 13 | 12 | 23 | 51 |
| Fruit juices | 2 | 8 | 32 | 25 | 27 | 7 |
| Average QEB score, m (Mdn) | 11.94 (12) |
| Diet quality index | |
| Index of a healthy diet, m ± SD | 3.30 ± 1.38 |
| Index of an unhealthy diet, m ± SD | 1.65 ± 1.07 |
| Intensity of healthy diet index | |
| Moderate, % | 10 |
| Small, % | 90 |
| Intensity of unhealthy diet index | |
| Moderate, % | 2 |
| Small, % | 98 |
| Kruskal–Wallis Test | H | 9.2423 | |||
| p | 0.0262 | ||||
| Primary | Vocational | Secondary | Higher | ||
| POST HOC (Dunn Bonferroni) | Primary | 1.0000 | 0.2071 | 0.8485 | |
| Vocational | 1.0000 | 0.0628 | 0.7115 | ||
| Secondary | 0.2071 | 0.0628 | 1.0000 | ||
| Higher | 0.8485 | 0.7115 | 1.0000 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Krężel, P.; Kurek, E.; Jurczak, A.; Napieracz-Trzosek, I.; Iłgowska, D.; Młyńska, K.; Wieder-Huszla, S. Analysis of Compliance with Proper Nutrition Principles in Patients with a History of Myocardial Infarction. Nutrients 2024, 16, 3091. https://doi.org/10.3390/nu16183091
Krężel P, Kurek E, Jurczak A, Napieracz-Trzosek I, Iłgowska D, Młyńska K, Wieder-Huszla S. Analysis of Compliance with Proper Nutrition Principles in Patients with a History of Myocardial Infarction. Nutrients. 2024; 16(18):3091. https://doi.org/10.3390/nu16183091
Chicago/Turabian StyleKrężel, Patrycja, Ewa Kurek, Anna Jurczak, Izabela Napieracz-Trzosek, Dorota Iłgowska, Katarzyna Młyńska, and Sylwia Wieder-Huszla. 2024. "Analysis of Compliance with Proper Nutrition Principles in Patients with a History of Myocardial Infarction" Nutrients 16, no. 18: 3091. https://doi.org/10.3390/nu16183091
APA StyleKrężel, P., Kurek, E., Jurczak, A., Napieracz-Trzosek, I., Iłgowska, D., Młyńska, K., & Wieder-Huszla, S. (2024). Analysis of Compliance with Proper Nutrition Principles in Patients with a History of Myocardial Infarction. Nutrients, 16(18), 3091. https://doi.org/10.3390/nu16183091