

The Association of Vitamin D Levels and Dental Caries in Older Adults: A Cross-Sectional Study
 ,
,  ,
, Highlights
- Vitamin D Deficiency and Dental Caries: The study found that older adults with vitamin D deficiency are more likely to have untreated dental caries and higher DMFT (Decayed, Missing, and Filled Teeth) scores.
- Severe Deficiency: Those with severe vitamin D deficiency showed significantly worse dental health outcomes, with a higher DMFT score by about 13%.
- Public Health: Addressing vitamin D deficiency through screening and supplementation could be crucial in improving dental health in older adults.
- Targeted Interventions: Specific high-risk groups, based on gender and race, may benefit from tailored vitamin D interventions for better oral health outcomes.
Abstract
1. Introduction
2. Methods
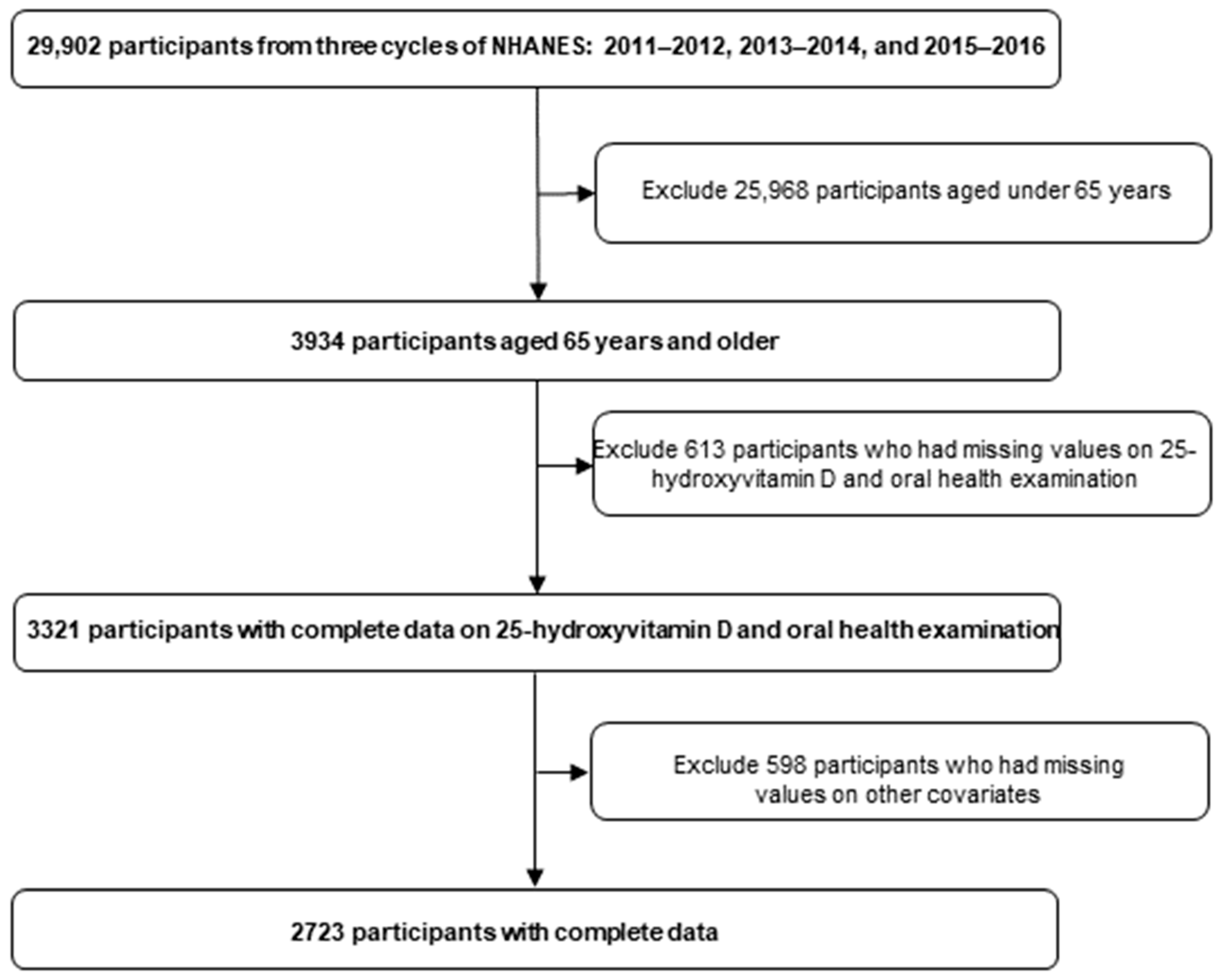
2.1. Data Source
2.2. Measures
2.3. Statistical Analyses
3. Results
4. Discussion
4.1. Strengths and Limitations
4.2. Public Health Implications and Future Research
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Rathee, M.; Sapra, A. Dental Caries. In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2023. [Google Scholar]
- Zhang, J.S.; Chu, C.-H.; Yu, O.Y. Oral Microbiome and Dental Caries Development. Dent. J. 2022, 10, 184. [Google Scholar] [CrossRef] [PubMed]
- Harper, R.A.; Shelton, R.M.; James, J.D.; Salvati, E.; Besnard, C.; Korsunsky, A.M.; Landini, G. Acid-induced demineralisation of human enamel as a function of time and pH observed using X-ray and polarised light imaging. Acta Biomater. 2021, 120, 240–248. [Google Scholar] [CrossRef] [PubMed]
- Angarita-Díaz, M.D.P.; Fong, C.; Bedoya-Correa, C.M.; Cabrera-Arango, C.L. Does high sugar intake really alter the oral microbiota?: A systematic review. Clin. Exp. Dent. Res. 2022, 8, 1376–1390. [Google Scholar] [CrossRef] [PubMed]
- Selwitz, R.H.; Ismail, A.I.; Pitts, N.B. Dental caries. Lancet 2007, 369, 51–59. [Google Scholar] [CrossRef] [PubMed]
- Featherstone, J. Dental caries: A dynamic disease process. Aust. Dent. J. 2008, 53, 286–291. [Google Scholar] [CrossRef] [PubMed]
- Pitts, N.B.; Zero, D.T.; Marsh, P.D.; Ekstrand, K.; Weintraub, J.A.; Ramos-Gomez, F.; Tagami, J.; Twetman, S.; Tsakos, G.; Ismail, A. Dental caries. Nat. Rev. Dis. Primers 2017, 3, 17030. [Google Scholar] [CrossRef] [PubMed]
- Al Saffan, A.D. Current Approaches to Diagnosis of Early Proximal Carious Lesion: A Literature Review. Cureus 2023, 15, e43489. [Google Scholar] [CrossRef]
- Maheswari, S.U.; Raja, J.; Kumar, A.; Seelan, R.G. Caries management by risk assessment: A review on current strategies for caries prevention and management. J. Pharm. Bioallied Sci. 2015, 7, S320–S324. [Google Scholar] [CrossRef] [PubMed]
- Petersen, P.E. The World Oral Health Report 2003, continuous improvement of oral health in the 21st century—The approach of the WHO Global Oral Health Programme. Community Dent. Oral Epidemiol. 2003, 31, 3–23. [Google Scholar]
- Lips, P. Vitamin D physiology. Prog. Biophys. Mol. Biol. 2006, 92, 4–8. [Google Scholar] [CrossRef]
- Holick, M.F. Vitamin D deficiency. N. Engl. J. Med. 2007, 357, 266–281. [Google Scholar] [CrossRef] [PubMed]
- Li, Z.; Wei, X.; Shao, Z.; Liu, H.; Bai, S. Correlation between vitamin D levels in serum and the risk of dental caries in children: A systematic review and meta-analysis. BMC Oral. Health 2023, 23, 768. [Google Scholar] [CrossRef] [PubMed]
- Mahmood, M.; Tassery, H.; Tardivo, D.; Lan, R. Association between Vitamin D Levels and Dental Caries: A Systematic Review and Dose-Response Meta-Analysis of Cross-Sectional Studies. Appl. Sci. 2023, 13, 9883. [Google Scholar] [CrossRef]
- Moneem Alhelfi, N.; Mohammed Hoobi, N. Effect of Vitamin D Deficiency on Dental Caries and Salivary Parameters. J. Med. Chem. Sci. 2023, 6, 1362–1369. [Google Scholar] [CrossRef]
- Machado, V.; Lobo, S.; Proença, L.; Mendes, J.J.; Botelho, J. Vitamin D and Periodontitis: A Systematic Review and Meta-Analysis. Nutrients 2020, 12, 2177. [Google Scholar] [CrossRef] [PubMed]
- Schroth, R.J.; Lavelle, C.; Tate, R.; Bruce, S.; Billings, R.J.; Moffatt, M.E.K. Prenatal vitamin D and dental caries in infants. Pediatrics 2014, 133, e1277–e1284. [Google Scholar] [CrossRef] [PubMed]
- Jagelavičienė, E.; Vaitkevičienė, I.; Šilingaitė, D.; Šinkūnaitė, E.; Daugėlaitė, G. The Relationship between Vitamin D and Periodontal Pathology. Medicina 2018, 54, 45. [Google Scholar] [CrossRef] [PubMed]
- Madi, M.; Pavlic, V.; Alammar, S.M.; Alsulaimi, L.M.; Alotaibi, R.S.; AlOtaibi, G.M.; Zakaria, O. The association between vitamin D level and periodontal disease in Saudi population, a preliminary study. Saudi Dent. J. 2021, 33, 595–600. [Google Scholar] [CrossRef]
- Ketterl, W. Age-induced changes in the teeth and their attachment apparatus. Int. Dent. J. 1983, 33, 262–271. [Google Scholar]
- Arola, D.; Reprogel, R.K. Effects of aging on the mechanical behavior of human dentin. Biomaterials 2005, 26, 4051–4061. [Google Scholar] [CrossRef]
- Botelho, J.; Machado, V.; Proença, L.; Delgado, A.S.; Mendes, J.J. Vitamin D Deficiency and Oral Health: A Comprehensive Review. Nutrients 2020, 12, 1471. [Google Scholar] [CrossRef] [PubMed]
- Hung, M.; Patel, H.; Lee, S.; Nguyen, J.; Mohajeri, A. The Influence of Vitamin D Levels on Dental Caries: A Retrospective Study of the United States Population. Nutrients 2024, 16, 1572. [Google Scholar] [CrossRef]
- Asante, E.O.; Chen, Y.; Eldholm, R.S.; Høvik, H.; Kolberg, M.; Skjellegrind, H.K.; Torabi-Gaarden, R.; Mai, X.-M. Associations of Serum Vitamin D with Dental Caries and Periodontitis: The HUNT Study. Int. Dent. J. 2024, 74, 500–509. [Google Scholar] [CrossRef] [PubMed]
- Hujoel, P.P. Vitamin D and dental caries in controlled clinical trials: Systematic review and meta-analysis. Nutr. Rev. 2013, 71, 88–97. [Google Scholar] [CrossRef] [PubMed]
- Rødseth, S.C.; Høvik, H.; Schuller, A.A.; Bjertness, E.; Skudutyte-Rysstad, R. Dental caries in a Norwegian adult population, the HUNT4 oral health study; prevalence, distribution and 45-year trends. Acta Odontol. Scand. 2023, 81, 202–210. [Google Scholar] [CrossRef] [PubMed]
- Center for Disease Control and Prevention. NCHS Ethics Review Board (ERB) Approval. Updated 24 August 2022. Available online: https://www.cdc.gov/nchs/nhanes/irba98.htm (accessed on 16 June 2024).
- Center for Disease Control and Prevention. National Health and Nutritional Examination Survey. Updated 30 May 2024. Available online: https://www.cdc.gov/nchs/nhanes/ (accessed on 16 June 2024).
- Center for Disease Control and Prevention. National Health and Nutrition Examination Survey: Oral Health Examiners Manual. Updated January 2020. Available online: https://wwwn.cdc.gov/nchs/data/nhanes/2019-2020/manuals/2020-Oral-Health-Examiners-Manual-508.pdf (accessed on 25 July 2023).
- Center for Disease Control and Prevention. Laboratory Procedure Manual: 25-Hydroxyvitamin D3, C3-epimer-25Hydroxyvitamin D3, and 25-Hydroxyvitamin D2. Updated 20 September 2010. Available online: https://wwwn.cdc.gov/nchs/data/nhanes/2009-2010/labmethods/VID_F_met_vitamin_D.pdf (accessed on 16 June 2024).
- Pu, R.; Fu, M.; Li, N.; Jiang, Z. A certain protective effect of vitamin D against dental caries in US children and youth: A cross-sectional study. J. Public. Health Dent. 2023, 83, 231–238. [Google Scholar] [CrossRef] [PubMed]
- Martens, P.-J.; Gysemans, C.; Verstuyf, A.; Mathieu, C. Vitamin D’s Effect on Immune Function. Nutrients 2020, 12, 1248. [Google Scholar] [CrossRef] [PubMed]
- Youssef, D.A.; Miller, C.W.; El-Abbassi, A.M.; Cutchins, D.C.; Cutchins, C.; Grant, W.B.; Peiris, A.N. Antimicrobial implications of vitamin D. Derm. Endocrinol. 2011, 3, 220–229. [Google Scholar] [CrossRef] [PubMed]
- Kamycheva, E.; Sundsfjord, J.; Jorde, R. Serum parathyroid hormone level is associated with body mass index. The 5th Tromsø study. Eur. J. Endocrinol. 2004, 151, 167–172. [Google Scholar] [CrossRef]
- Ginde, A.A.; Liu, M.C.; Camargo, C.A., Jr. Demographic differences and trends of vitamin D insufficiency in the US population, 1988–2004. Arch. Intern. Med. 2009, 169, 626–632. [Google Scholar] [CrossRef]
- Petersen, P.E.; Yamamoto, T. Improving the oral health of older people: The approach of the WHO Global Oral Health Programme. Community Dent. Oral. Epidemiol. 2005, 33, 81–92. [Google Scholar] [CrossRef] [PubMed]
- Lipsky, M.S.; Singh, T.; Zakeri, G.; Hung, M. Oral Health and Older Adults: A Narrative Review. Dent. J. 2024, 12, 30. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Variables | All Participants | Participants with Untreated Caries Mean ± SD N (%) | Untreated Caries p-Value | Participants DMFT Score Mean ± SD | DMFT p-Value |
|---|---|---|---|---|---|
| Age (years) | 73.07 ± 5.35 | 72.54 ± 5.31 | -- | 73.16 ± 5.35 | <0.001 b |
| Sex | |||||
| Female | 1362 (50%) | 437 (32.10%) | 0.008 a | 17.63 ± 8.27 | 0.58 c |
| Male | 1361 (50%) | 519 (38.10%) | 17.82 ± 8.40 | ||
| Race and Ethnicity | |||||
| Mexican American | 265 (9.70%) | 129 (48.70%) | <0.001 a | 15.17 ± 8.45 | <0.001 d |
| Other Hispanic | 278 (10.20%) | 104 (37.40%) | 18.03 ± 8.16 | ||
| Non-Hispanic white | 1434 (52.70%) | 450 (31.40%) | 17.93 ± 8.24 | ||
| Non-Hispanic Black | 502 (18.40%) | 194 (38.60%) | 19.11 ± 7.88 | ||
| Non-Hispanic Asian | 189 (6.90%) | 59 (31.20%) | 14.98 ± 8.90 | ||
| Other Race * | 55 (2%) | 20 (36.4%) | 19.87 ± 8.73 | ||
| Birth country | |||||
| United States | 2088 (76.70%) | 730 (35%) | <0.001 a | 18.06 ± 8.22 | <0.001 c |
| Others | 635 (23.30%) | 226 (35.60%) | 16.64 ± 8.64 | ||
| 25(OH)D (nmol/mL) | |||||
| Normal (≥75) | 1428 (52.40%) | 463 (32.40%) | <0.001 a | 17.41 ± 8.24 | 0.002 d |
| Insufficient (50–74.9) | 835 (30.70%) | 305 (36.50%) | 17.58 ± 8.45 | ||
| Deficient (25–49.9) | 411 (15.10%) | 168 (40.90%) | 18.96 ± 8.30 | ||
| Severely deficient (<25) | 49 (1.8%) | 20 (40.80%) | 19.33 ± 8.56 |
| Variables | Severely Deficient (<25 nmol/L) | Deficient (25–49.9 nmol/L) | Insufficient (50–74.9 nmol/L) | Normal (≥75 nmol/L) | p-Value |
|---|---|---|---|---|---|
| Untreated caries | |||||
| Yes | 20 (2.10%) | 168 (17.60%) | 305 (31.90%) | 463 (48.40%) | 0.008 a |
| No | 29 (1.60%) | 243 (13.80%) | 530 (30%) | 965 (54.60%) | |
| DMFT Scores | 18.94 ± 8.91 | 18.96 ± 8.30 | 17.58 ± 8.45 | 17.41 ± 8.24 | 0.002 b |
| Variables | Model I 1 | Model II 2 |
|---|---|---|
| Untreated Caries | OR [95% CI] | OR [95% CI] |
| Normal (≥75 nmol/L) | Reference | Reference |
| Insufficient (50–74.9 nmol/L) | 1.20 [1.00–1.44] * | 1.07 [0.89–1.29] |
| Deficient (25–49.9 nmol/L) | 1.44 [1.15–1.81] * | 1.23 [0.97–1.55] |
| Severely deficient (<25 nmol/L) | 1.44 [0.81–2.57] | 1.20 [0.66–2.18] |
| DMFT Scores | RR [95% CI] | RR [95% CI] |
| Normal (≥75 nmol/L) | Reference | Reference |
| Insufficient (50–74.9 nmol/L) | 1.03 [1.00–1.05] * | 1.04 [1.02–1.06] * |
| Deficient (25–49.9 nmol/L) | 1.08 [1.05–1.11] * | 1.09 [1.07–1.12] * |
| Severely deficient (<25 nmol/L) | 1.13 [1.06–1.20] * | 1.12 [1.05–1.20] * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hung, M.; Mohajeri, A.; Sadri, M.; Khodabandeh, E.; Zeitoun, I.; Lipsky, M.S. The Association of Vitamin D Levels and Dental Caries in Older Adults: A Cross-Sectional Study. Nutrients 2024, 16, 2307. https://doi.org/10.3390/nu16142307
Hung M, Mohajeri A, Sadri M, Khodabandeh E, Zeitoun I, Lipsky MS. The Association of Vitamin D Levels and Dental Caries in Older Adults: A Cross-Sectional Study. Nutrients. 2024; 16(14):2307. https://doi.org/10.3390/nu16142307
Chicago/Turabian StyleHung, Man, Amir Mohajeri, Mahsa Sadri, Elahe Khodabandeh, Ibrahim Zeitoun, and Martin S. Lipsky. 2024. "The Association of Vitamin D Levels and Dental Caries in Older Adults: A Cross-Sectional Study" Nutrients 16, no. 14: 2307. https://doi.org/10.3390/nu16142307
APA StyleHung, M., Mohajeri, A., Sadri, M., Khodabandeh, E., Zeitoun, I., & Lipsky, M. S. (2024). The Association of Vitamin D Levels and Dental Caries in Older Adults: A Cross-Sectional Study. Nutrients, 16(14), 2307. https://doi.org/10.3390/nu16142307