
Influence of Adherence to the Mediterranean Diet and Level of Physical Activity with Liver Steatosis in People Aged > 50 Years and with a BMI > 25 kg/m2: Association with Biochemical Markers
 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
- Patients with ultrasound-diagnosed hepatic steatosis: Patients aged over 50 years with a BMI > 25 kg/m2, with an ultrasound diagnosis of hepatic steatosis and who attended primary care.
- Control group of individuals without hepatic steatosis: To assess the effect of adherence to the Mediterranean diet and physical activity, a group of patients aged over 50 years with a BMI > 25 kg/m2 but without ultrasound evidence of hepatic steatosis and who attended the same primary care centers were also included in the study.
2.1. Questionnaires Used
2.2. Calculation of Biochemical Markers of Hepatic Steatosis
- Hepatic Steatosis Index (HSI) = 8 × ALT/AST + BMI (+2 if the patient has DM2; +2 in women).
- AST to platelet ratio index (APRI) = (AST/ALT × 100)/platelet count (109/L).
- Fibrosis-4 (FIB-4) = (age [years] × AST)/(platelet count × ALT)
2.3. Variables
2.4. Statistical Methodology
- Comparison between qualitative variables: When comparing two discrete variables, the Chi-square test was used. When the expected value in any of the boxes of the contingency table was less than 5, it was necessary to use Fisher’s exact test. Relative risk was used to estimate the magnitude of the association.
- Comparison of two normal quantitative variables: Pearson’s comparison method was used. If one or both variables did not have a Gaussian distribution, Spearman’s test was used.
- Comparison of two independent means: Student’s t-test (Mann–Whitney U test for non-Gaussian variables).
- Correlation between quantitative variables: Pearson correlation coefficient (Spearman correlation coefficient for non-Gaussian variables).
2.5. Ethical Aspects
3. Results
3.1. Anthropometric Variables
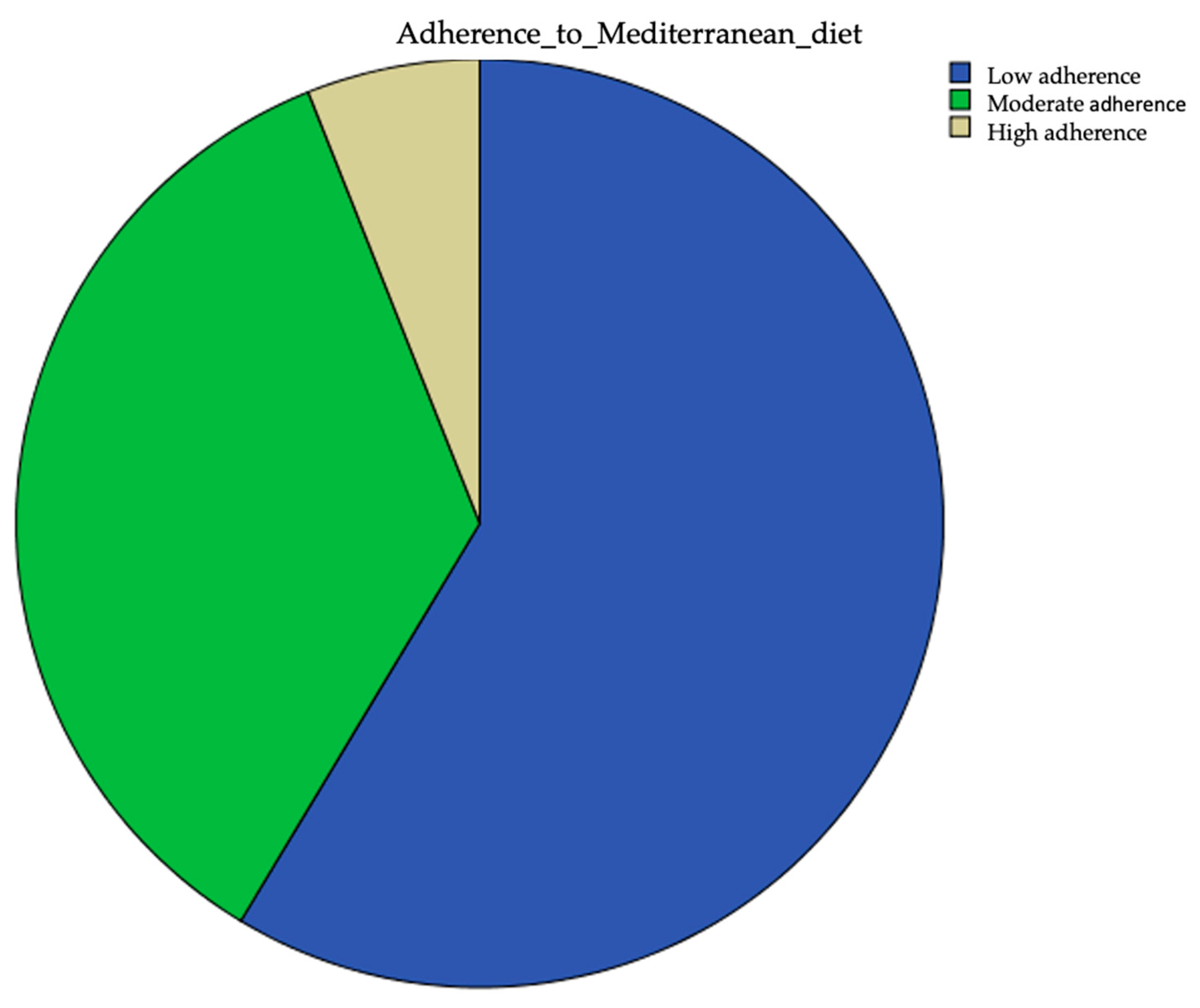
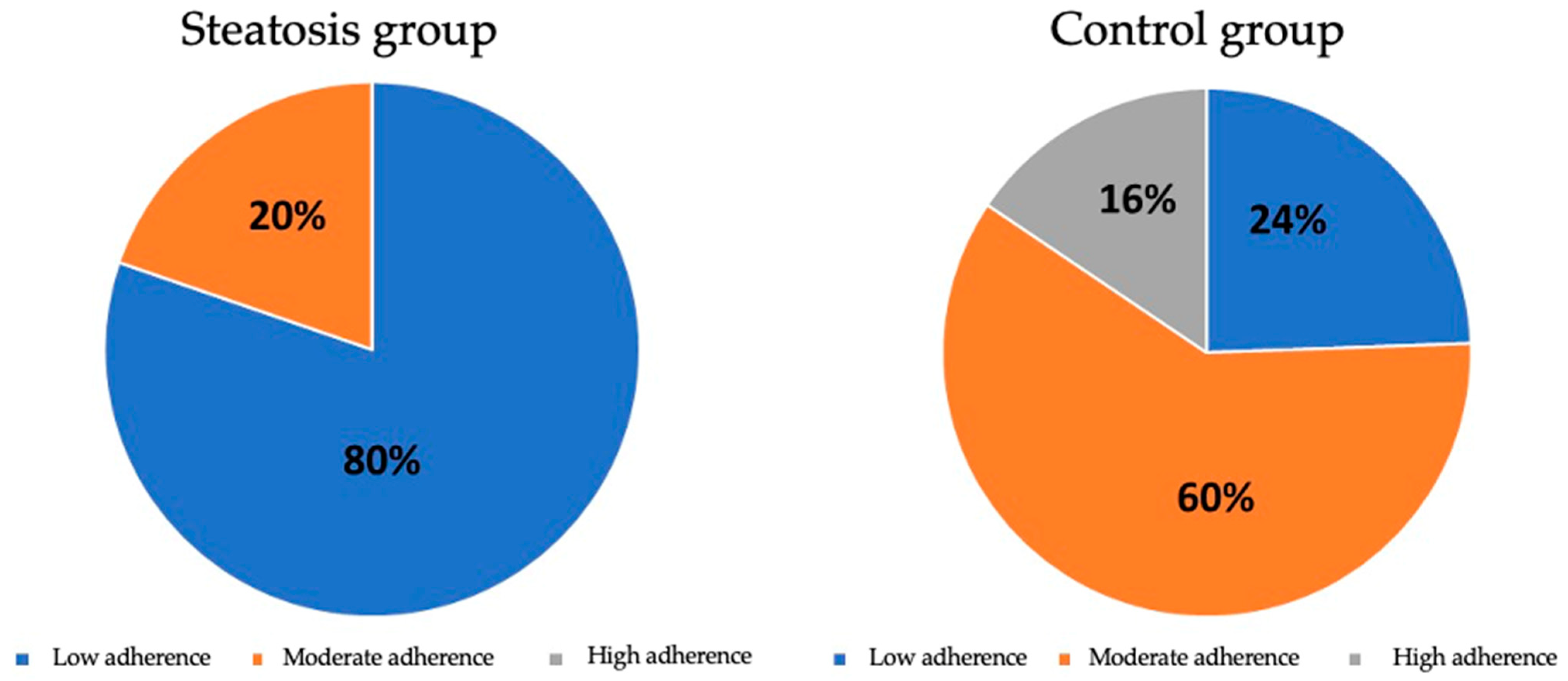
3.2. Adherence to the Mediterranean Diet
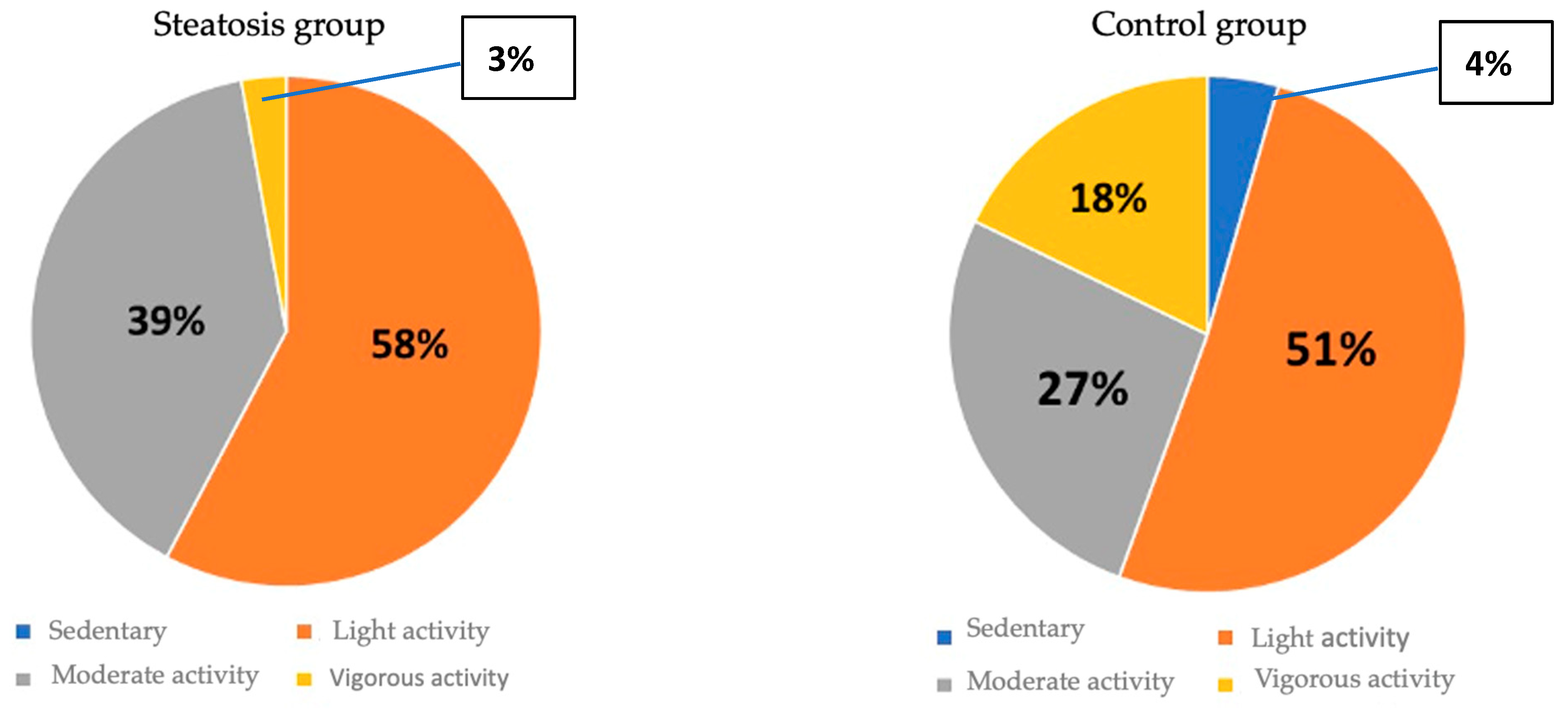
3.3. Physical Activity Level
3.4. Biochemical Markers of Hepatic Steatosis
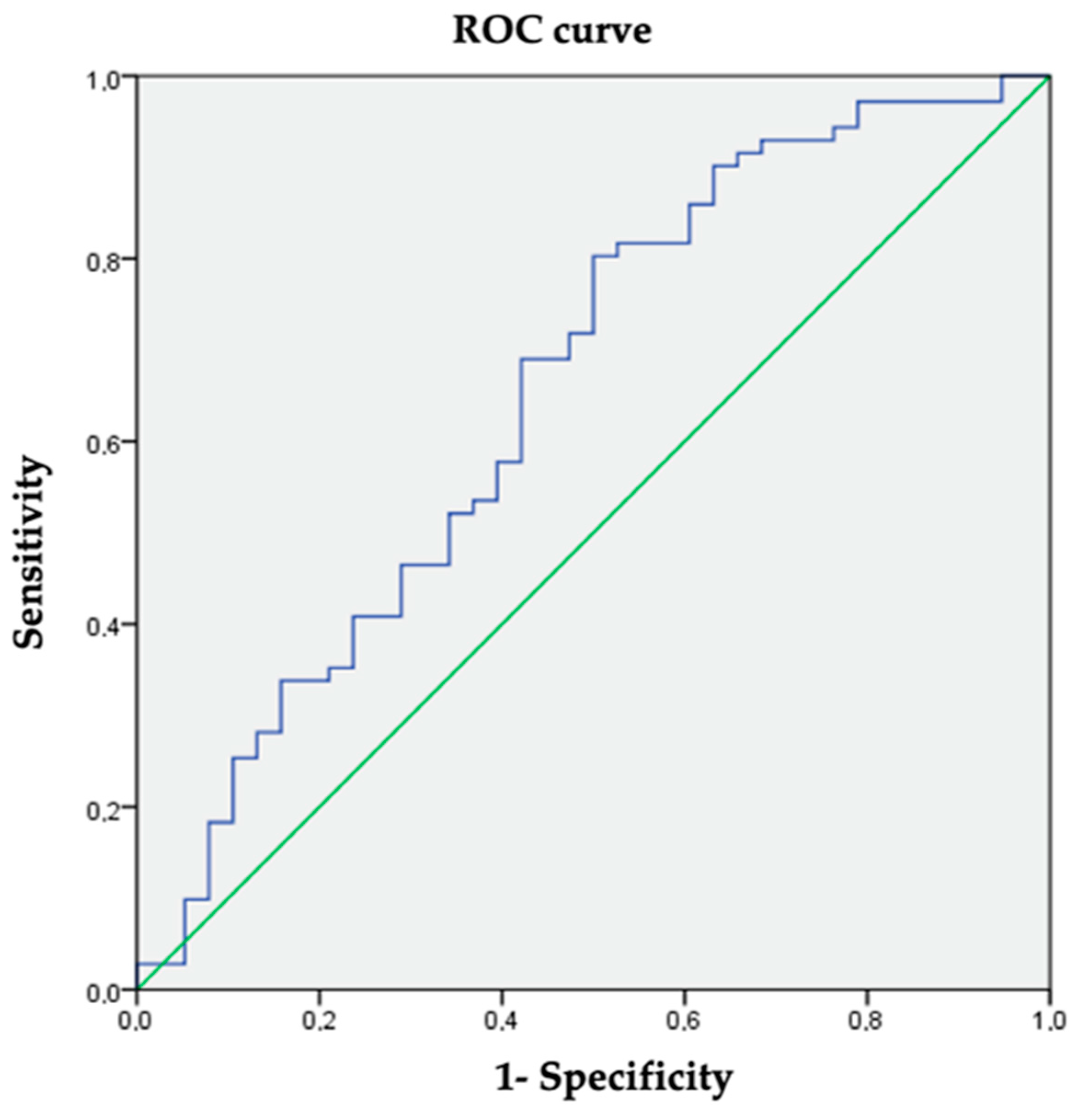
3.5. Correlation between Hepatic Steatosis and Adherence to the Mediterranean Diet
3.6. Association between Hepatic Steatosis and Level of Physical Activity
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Abdelmalek, M.F.; Mae Diehl, A. Hepatopatía grasa no alcohólica y esteatohepatitis no alcohólica. In Harrison Principios De Medicina Interna, 20th ed.; McGraw-Hill Education: New York, NY, USA, 2018; Volume 2, pp. 2401–2405. [Google Scholar]
- Flier, J.S.; Maratos-Flier, E. Biopatología de la obesidad. In Harrison Principios De Medicina Interna, 20th ed.; McGraw-Hill Education: New York, NY, USA, 2018; pp. 2837–2843. [Google Scholar]
- Graffigna, M.; Catoira, N.; Soutelo, J.; Azpelicueta, A.; Berg, G.; Perel, C.; Migliano, M.E.; Aranguren, M.; Musso, C.; Farias, J. Diagnóstico de esteatosis hepática por métodos clínicos, bioquímicos y por imágenes. Rev. Argent. Endocrinol. Metab. 2017, 54, 37–46. [Google Scholar] [CrossRef]
- García-Gómez-Heras, S. Biochemical markers. In Liver Steatosis and Bariatric Surgery; Ruiz-Tovar, J., Ed.; Nova Science Publishers, Inc.: New York, NY, USA, 2019; p. 314. [Google Scholar]
- European Association for the Study of the Liver. EASL Clinical Practice Guidelines on non-invasive tests for evaluation of liver disease severity and prognosis-2021 update. J. Hepatol. 2021, 75, 659–689. [Google Scholar] [CrossRef]
- Ruiz-Tovar, J.; Zubiaga, L. Validation of biochemical scores for liver steatosis before and 1 year after sleeve gastrectomy. Surg. Obes. Relat. Dis. 2019, 15, 1447–1453. [Google Scholar] [CrossRef] [PubMed]
- García-Gavilán, J.; Nishi, S.K.; Paz-Graniel, I.; Guasch-Ferré, M.; Razquin, C.; Clish, C.B.; Toledo, E.; Ruiz-Canela, M.; Corella, D.; Deik, A.; et al. Plasma Metabolite Profiles Associated with the Amount and Source of Meat and Fish Consumption and the Risk of Type 2 Diabetes. Mol. Nutr. Food Res. 2022, 10, e2200145. [Google Scholar] [CrossRef] [PubMed]
- Zapata, I.; Maté-Muñoz, J.L.; Higueras, A.; Hernández-Lougedo, J.; Martín-Fidalgo, N.; García-Fernández, P.; Redondo-Vega, M.V.; Ruiz-Tovar, J. Toxic habits and well-being measures in Spanish Healthcare University Students during the COVID-19 pandemic. Int. J. Environ. Res. Public Health 2022, 19, 13213. [Google Scholar] [CrossRef] [PubMed]
- Zubiaga Toro, L.; Ruiz-Tovar, J.; Diez-Tabernilla, M.; Bernal, L.G.; Sebastián, A.A.; Rico, R.C. Fórmula CUN-BAE y factores bioquímicos como marcadores predictivos de obesidad y enfermedad cardiovascular en pacientes pre y post gastrectomía vertical. Nutr. Hosp. 2014, 30, 281–286. [Google Scholar] [PubMed]
- UCLA. Statistical Methods and Data Analytics. Available online: https://stats.oarc.ucla.edu/other/gpower/ (accessed on 28 November 2023).
- Carreño Enciso, L.; de Mateo Silleras, B.; de la Cruz Marcos, S.; Redondo Del Río, P. Social Media for Nutrition Education-A Randomized Controlled Trial to Promote Fruit and Vegetable Intake in a University Setting: “The University of Valladolid Community Eats Healthy” Study. Nutrients 2024, 16, 1308. [Google Scholar] [CrossRef] [PubMed]
- Wilhelm, R.A.; Lacey, M.F.; Masters, S.L.; Breeden, C.J.; Mann, E.; MacDonald, H.V.; Gable, P.A.; White, E.J.; Stewart, J.L. Greater weekly physical activity linked to left resting frontal alpha asymmetry in women: A study on gender differences in highly active young adults. Psychol. Sport Exerc. 2024, 74, 102679. [Google Scholar] [CrossRef] [PubMed]
- Misciagna, G.; Del Pilar Diaz, M.; Caramia, D.V.; Bonfiglio, C.; Franco, I.; Noviello, M.R.; Chiloiro, M.; Abbrescia, D.I.; Mirizzi, A.; Tanzi, M.; et al. Effect of a Low Glycemic Index Mediterranean Diet on Non-Alcoholic Fatty Liver Disease. A Randomized Controlled Clinici Trial. J. Nutr. Health Aging 2017, 21, 404–412. [Google Scholar] [CrossRef]
- Estruch, R.; Ros, E.; Salas-Salvadó, J.; Covas, M.-I.; Corella, D.; Arós, F.; Gómez-Gracia, E.; Ruiz-Gutiérrez, V.; Fiol, M.; Lapetra, J.; et al. Primary prevention of cardiovascular disease with a Mediterranean diet. N. Engl. J. Med. 2018, 378, e34. [Google Scholar] [CrossRef]
- Costarelli, V.; Koretsi, E.; Georgitsogianni, E. Health-related quality of life of Greek adolescents: The role of the Mediterranean diet. Qual. Life Res. 2013, 22, 951–956. [Google Scholar] [CrossRef] [PubMed]
- Mamplekou, E.; Bountziouka, V.; Psaltopoulou, T.; Zeimbekis, A.; Tsakoundakis, N.; Papaerakleous, N.; Gotsis, E.; Metallinos, G.; Pounis, G.; Polychronopoulos, E.; et al. Urban environment, physical inactivity and unhealthy dietary habits correlate to depression among elderly livingin Eastern Mediterranean Islands: The MEDIS (Mediterranean Islands Elderly) study. J. Nutr. Health Aging 2010, 14, 449–455. [Google Scholar] [CrossRef] [PubMed]
- Sofi, F.; Cesari, F.; Abbate, R.; Gensini, G.F.; Casini, A. Adherence to Mediterranean diet and Health status: Meta-analysis. BMJ. 2008, 337, a1344. [Google Scholar] [CrossRef] [PubMed]
- Mente, A.; de Koning, L.; Shannon, H.S.; Anand, S.S. A systematic review of the evidence supporting a causal link between dietary factors and coronary heart disease. Arch. Intern. Med. 2009, 169, 659–669. [Google Scholar] [CrossRef] [PubMed]
- Willett, W.C.; Sacks, F.; Trichopoulou, A.; Drescher, G.; Ferro-Luzzi, A.; Helsing, E.; Trichopoulos, D. Mediterranean diet pyramid: A cultural model for healthy eating. Am. J. Clin. Nutr. 1995, 61, 1402S–1406S. [Google Scholar] [CrossRef] [PubMed]
- Tosti, V.; Bertozzi, B.; Fontana, L. Health benefits of the Mediterranean diet: Metabolic and molecular mechanisms. J. Gerontol. A Biol. Sci. Med. Sci. 2018, 73, 318–326. [Google Scholar] [CrossRef] [PubMed]
- Dernini, S.; Berry, E.M.; Serra-Majem, L.; La Vecchia, C.; Capone, R.; Medina, F.; Aranceta-Bartrina, J.; Belahsen, R.; Burlingame, B.; Calabrese, G. Med Diet 4.0: The Mediterranean diet with four sustainable benefits. Public Health Nutr. 2017, 20, 1322–1330. [Google Scholar] [CrossRef] [PubMed]
- Sánchez-Villegas, A.; Martinez, J.A.; De Irala I y Martinez-González, M.A. Determinants of the adherence to an “a priori” defined Mediterranean dietary pattern. Eur. J. Nutr. 2002, 41, 249–257. [Google Scholar] [CrossRef]
- Lydakis, C.; Stefanaki, E.; Stefanaki, S.; Thalassinos, E.; Kavousanaki, M.; Lydaki, D. Correlation of blood pressure, obesity and adherence to the Mediterranean diet with indices of arterial stiffness in children. Eur. J. Pediatr. 2012, 171, 1373–1382. [Google Scholar] [CrossRef]
- Ryan, M.C.; Itsiopoulos, C.; Thodis, T.; Ward, G.; Trost, N.; Hofferberth, S.; O’dea, K.; Desmond, P.V.; Johnson, N.A.; Wilson, A.M. The Mediterranean diet improves hepatic steatosis and insulin sensitivity in individuals with non-alcoholic fatty liver disease. J. Hepatol. 2013, 59, 138–143. [Google Scholar] [CrossRef]
- Velasco, N.; Contreras, A.; Grassi, B. The Mediterranean diet, hepatic steatosis and nonalcoholic fatty liver disease. Curr. Opin. Clin. Nutr. Metab. Care 2014, 17, 453–457. [Google Scholar] [CrossRef]
- Karković Marković, A.; Torić, J.; Barbarić, M.; Jakobušić Brala, C. Hydroxytyrosol, tyrosol and derivatives and their potential effects on human health. Molecules 2019, 24, 2001. [Google Scholar] [CrossRef] [PubMed]
- Carnevale, R.; Silvestri, R.; Loffredo, L.; Novo, M.; Cammisotto, V.; Castellani, V.; Bartimoccia, S.; Nocella, C.; Violi, F. Oleuropein, a component of extra virgin olive oil, lowers postprandial glycaemia in healthy subjects. Br. J. Clin. Pharmacol. 2018, 84, 1566–1574. [Google Scholar] [CrossRef] [PubMed]
- Wu, L.; Velander, P.; Liu, D.; Xu, B. Olive component oleuropein promotes β-cell insulin secretion and protects β-cells from amylin amyloid-induced cytotoxicity. Biochemistry 2017, 56, 5035–5039. [Google Scholar] [CrossRef] [PubMed]
- Godos, J.; Federico, A.; Dallio, M.; Scazzina, F. Mediterranean diet and nonalcoholic fatty liver disease: Molecular mechanisms of protection. Int. J. Food Sci. Nutr. 2017, 68, 18–27. [Google Scholar] [CrossRef] [PubMed]
- Saavedra, Y.; Mena, V.; Priken, K. Effect of the Mediterranean diet on histological indicators and imaging tests in non-alcoholic fatty liver disease. Gastroenterol. Hepatol. 2022, 45, 350–360. [Google Scholar] [CrossRef] [PubMed]
- Teixeira, B.; Afonso, C.; Severo, M.; Carvalho, C.; Torres, D.; Lopes, C.; Oliveira, A. Exploring dietary patterns and their association with environmental sustainability and body mass index in children and adolescents: Insights from the National Food, nutrition and physical activity survey 2015–2016. Sci. Total Environ. 2024, 15, 174051. [Google Scholar] [CrossRef]
- Hallsworth, M.; Berry, D.; Sanders, M.; Sallis, A.; King, D.; Vlaev, I.; Darzi, A. Stating Appointment Costs in SMS Reminders Reduces Missed Hospital Appointments: Findings from Two Randomised Controlled Trials. Clin. Sci. 2015, 129, 1097–1105. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Wang, X.; Fang, Z. Evaluating the impact of exercise on intermediate disease markers in overweight and obese individuals through a network meta-analysis of randomized controlled trials. Sci. Rep. 2024, 14, 12137. [Google Scholar] [CrossRef]
- García-Gavilán, J.F.; Atzeni, A.; Babio, N.; Liang, L.; Belzer, C.; Vioque, J.; Corella, D.; Fitó, M.; Vidal, J.; Moreno-Indias, I.; et al. Effect of 1-year lifestyle intervention with energy-reduced Mediterranean diet and physical activity promotion on the gut metabolome and microbiota: A randomized clinical trial. Am. J. Clin. Nutr. 2024, 119, 1143–1154. [Google Scholar] [CrossRef]
- Lonardo, A.; Nascimbeni, F.; Maurantonio, M. Nonalcoholic fatty liver disease: Evolving paradigms. World J. Gastroenterol. 2017, 23, 6571–6592. [Google Scholar] [CrossRef] [PubMed]
- Arab, J.P.; Barrera, F.; Arrese, M. The evolving role of liver biopsy in nonalcoholic fatty liver disease. Ann. Hepatol. 2018, 17, 899–902. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total | CG | SG | p | |
|---|---|---|---|---|
| Weight (Kg) | 86.6 ± 14.0 | 78.5 ± 14.9 | 91.7 ± 10.7 | 0.000 |
| IMC (Kg/m2) | 31.4 ± 4.3 | 28.5 ± 4.3 | 33.2 ± 3.2 | 0.000 |
| Adiposity (%) | 39.2 ± 7.3 | 37.0 ± 7.4 | 40.6 ± 6.9 | 0.009 |
| Steatosis Group (n = 71) | Control Group (n = 45) | p | |
|---|---|---|---|
| Global obesity according to BMI (%) | 90.1% | 31.1% | 0.000 |
| Global obesity according to adiposity (%) | 100% | 88.9% | 0.008 |
| Frequency | Percentage | |
|---|---|---|
| Sedentary | 2 | 1.7 |
| Light activity | 64 | 55.2 |
| Moderate activity | 40 | 34.5 |
| Vigorous activity | 10 | 8.6 |
| Ultrasound Steatosis | Mean | Standard Deviation | p | |
|---|---|---|---|---|
| HSI | No | 38.3262 | 5.50273 | 0.000 |
| Yes | 43.6782 | 5.23534 | ||
| APRI | No | 0.4568 | 0.21902 | 0.081 |
| Yes | 0.5569 | 0.31134 | ||
| FIB_4 | No | 0.3006 | 0.19029 | 0.039 |
| Yes | 0.3997 | 0.25703 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cano-Lallave, L.; Ruiz-Tovar, J.; Martin-de-Bernardo, L.; Martinez-Oribe, M.; Rodriguez-Obispo, C.; Carrascosa-Corrochano, S.; Martín-Nieto, A.; Baeza, I.; Gonzalez-Ramos, M.; Benito, M.; et al. Influence of Adherence to the Mediterranean Diet and Level of Physical Activity with Liver Steatosis in People Aged > 50 Years and with a BMI > 25 kg/m2: Association with Biochemical Markers. Nutrients 2024, 16, 1996. https://doi.org/10.3390/nu16131996
Cano-Lallave L, Ruiz-Tovar J, Martin-de-Bernardo L, Martinez-Oribe M, Rodriguez-Obispo C, Carrascosa-Corrochano S, Martín-Nieto A, Baeza I, Gonzalez-Ramos M, Benito M, et al. Influence of Adherence to the Mediterranean Diet and Level of Physical Activity with Liver Steatosis in People Aged > 50 Years and with a BMI > 25 kg/m2: Association with Biochemical Markers. Nutrients. 2024; 16(13):1996. https://doi.org/10.3390/nu16131996
Chicago/Turabian StyleCano-Lallave, Laura, Jaime Ruiz-Tovar, Lucia Martin-de-Bernardo, Malena Martinez-Oribe, Cristina Rodriguez-Obispo, Sara Carrascosa-Corrochano, Ana Martín-Nieto, Isabel Baeza, Marta Gonzalez-Ramos, Marta Benito, and et al. 2024. "Influence of Adherence to the Mediterranean Diet and Level of Physical Activity with Liver Steatosis in People Aged > 50 Years and with a BMI > 25 kg/m2: Association with Biochemical Markers" Nutrients 16, no. 13: 1996. https://doi.org/10.3390/nu16131996
APA StyleCano-Lallave, L., Ruiz-Tovar, J., Martin-de-Bernardo, L., Martinez-Oribe, M., Rodriguez-Obispo, C., Carrascosa-Corrochano, S., Martín-Nieto, A., Baeza, I., Gonzalez-Ramos, M., Benito, M., & Olazabal, I. (2024). Influence of Adherence to the Mediterranean Diet and Level of Physical Activity with Liver Steatosis in People Aged > 50 Years and with a BMI > 25 kg/m2: Association with Biochemical Markers. Nutrients, 16(13), 1996. https://doi.org/10.3390/nu16131996