
Beef Consumption Is Associated with Higher Intakes and Adequacy of Key Nutrients in Older Adults Age 60+ Years: National Health and Nutrition Examination Survey 2011–2018 Analysis


Abstract
1. Introduction
2. Materials and Methods
2.1. Database and Study Population
2.2. Dietary Intake
2.3. Beef Intake
2.4. Statistics
3. Results
3.1. Beef Intake
3.2. Demographics
3.3. Nutrient Intakes and Adequacy
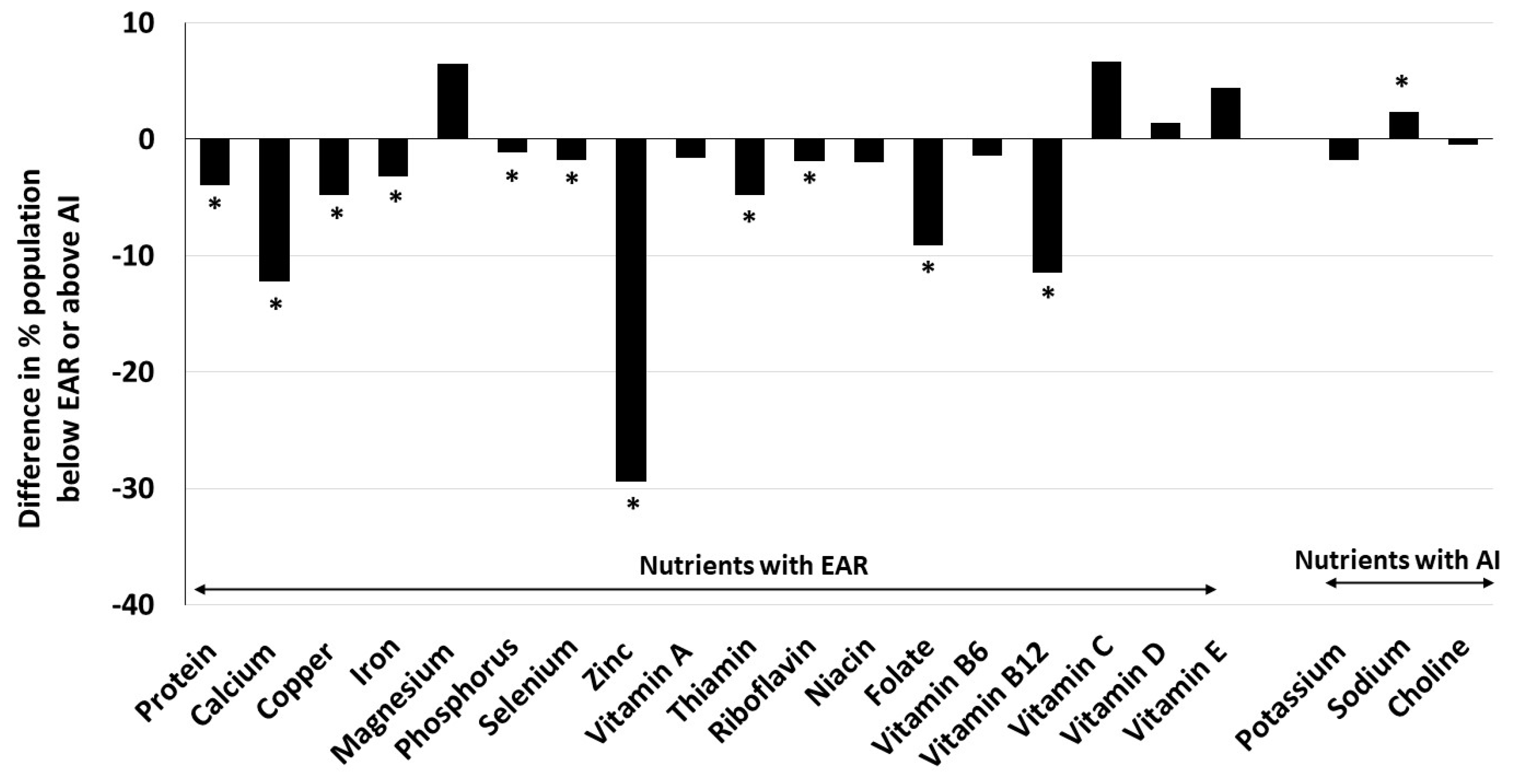
3.4. Association of Beef Intake with Nutrient Intake and Adequacy
3.5. Intake of Different Beef Types
3.6. Effect of Different Beef Types Intake on Nutrient Intake and Adequacy
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- WHO. Ageing. 2024. Available online: https://www.who.int/health-topics/ageing (accessed on 20 April 2024).
- Mather, M.; Scommegna, P. Fact Sheet: Aging in the United States. PRB 2024. Available online: https://www.prb.org/resources/fact-sheet-aging-in-the-united-states/2024 (accessed on 5 March 2024).
- Prince, M.J.; Wu, F.; Guo, Y.; Gutierrez Robledo, L.M.; O’Donnell, M.; Sullivan, R.; Yusuf, S. The burden of disease in older people and implications for health policy and practice. Lancet 2015, 385, 549–562. [Google Scholar] [CrossRef] [PubMed]
- Institute of Medicine. Nutrition Concerns for Aging Populations—Providing Healthy and Safe Foods as We Age; National Academies Press: Washington, DC, USA, 2010. [Google Scholar]
- Morley, J.E. Undernutrition in older adults. Fam. Pract. 2012, 29, i89–i93. [Google Scholar] [CrossRef] [PubMed]
- Stalling, I.; Albrecht, B.M.; Foettinger, L.; Recke, C.; Bammann, K. Meal patterns of older adults: Results from the OUTDOOR ACTIVE study. Nutrients 2022, 14, 2784. [Google Scholar] [CrossRef] [PubMed]
- Roberts, S.B.; Silver, R.E.; Das, S.K.; Fielding, R.A.; Gilhooly, C.H.; Jacques, P.F.; Kelly, J.M.; Mason, J.B.; McKeown, N.M.; Reardon, M.A.; et al. Healthy aging-nutrition matters: Start early and screen sften. Adv. Nutr. 2021, 12, 1438–1448. [Google Scholar] [CrossRef] [PubMed]
- USDA/DHHS. Dietary Guidelines for Americans 2020–2025, 9th ed.; USDA/DHHS: Lincoln, NE, USA, 2020. Available online: https://www.dietaryguidelines.gov/sites/default/files/2021-03/Dietary_Guidelines_for_Americans-2020-2025.pdf (accessed on 5 March 2024).
- Biesalski, H.K. Meat as a component of a healthy diet—Are there any risks or benefits if meat is avoided in the diet? Meat Sci. 2005, 70, 509–524. [Google Scholar] [CrossRef] [PubMed]
- Klurfeld, D.M. Research gaps in evaluating the relationship of meat and health. Meat Sci. 2015, 109, 86–95. [Google Scholar] [CrossRef] [PubMed]
- Pereira, P.M.; Vicente, A.F. Meat nutritional composition and nutritive role in the human diet. Meat Sci. 2013, 93, 586–592. [Google Scholar] [CrossRef] [PubMed]
- Wyness, L.; Weichselbaum, E.; O’Connor, A.; Williams, E.B.; Benelam, B.; Riley, H.; Stanner, S. Red meat in the diet: An update. Nutr. Bull. 2011, 36, 34–77. [Google Scholar] [CrossRef]
- Zanovec, M.; O’Neil, C.E.; Keast, D.R.; Fulgoni, V.L.3rd; Nicklas, T.A. Lean beef contributes significant amounts of key nutrients to the diets of US adults: National Health and Nutrition Examination Survey 1999–2004. Nutr. Res. 2010, 30, 375–381. [Google Scholar] [CrossRef]
- Nicklas, T.A.; O’Neil, C.E.; Zanovec, M.; Keast, D.R.; Fulgoni, V.L. Contribution of beef consumption to nutrient intake, diet quality, and food patterns in the diets of the US population. Meat Sci. 2012, 90, 152–158. [Google Scholar] [CrossRef]
- An, R.; Nickols-Richardson, S.; Alston, R.; Shen, S.; Clarke, C. Total, fresh, lean, and fresh lean beef consumption in relation to nutrient intakes and diet quality among U.S. adults, 2005–2016. Nutrients 2019, 11, 563. [Google Scholar] [CrossRef]
- Agarwal, S.; Fulgoni, V.L. Contribution of beef to key nutrient intakes in American adults: An updated analysis with NHANES 2011–2018. Nutr. Res. 2022, 105, 105–112. [Google Scholar] [CrossRef] [PubMed]
- Beal, T.; Gardner, C.D.; Herrero, M.; Iannotti, L.L.; Merbold, L.; Nordhagen, S.; Mottet, A. Friend or foe? The role of animal-source foods in healthy and environmentally sustainable diets. J. Nutr. 2023, 153, 409–425. [Google Scholar] [CrossRef] [PubMed]
- CDC. National Health and Nutrition Examination Survey. Hyattsville, MD. 2021. Available online: https://www.cdc.gov/nchs/nhanes/index.htm (accessed on 10 December 2023).
- Raper, N.; Perloff, B.; Ingwersen, L.; Steinfeldt, L.; Anand, J. An overview of USDA’s dietary intake data system. J. Food Comp. Anal. 2004, 17, 545–555. [Google Scholar] [CrossRef]
- USDA/ARS. Food and Nutrient Database for Dietary Studies. Food Surveys Research Group Home Page 2023. Available online: http://www.ars.usda.gov/nea/bhnrc/fsrg (accessed on 10 December 2023).
- USDA/ARS. Food Products Equivalents Database. 2021. Available online: https://www.ars.usda.gov/northeast-area/beltsville-md-bhnrc/beltsville-human-nutrition-research-center/food-surveys-research-group/docs/fped-databases/ (accessed on 10 December 2023).
- Tooze, J.A.; Kipnis, V.; Buckman, D.W.; Carroll, R.J.; Freedman, L.S.; Guenther, P.M.; Krebs-Smith, S.M.; Subar, A.F.; Dodd, K.W. A mixed-effects model approach for estimating the distribution of usual intake of nutrients: The NCI method. Stat. Med. 2010, 29, 2857–2868. [Google Scholar] [CrossRef]
- Institute of Medicine. Dietary Reference Intakes: Applications in Dietary Assessment; National Academies Press: Washington, DC, USA, 2000. [Google Scholar]
- Lau, C.S.; Fulgoni, V.L.; Van Elswyk, M.E.; McNeill, S.H. Trends in beef intake in the United States: Analysis of the National Health and Nutrition Examination Survey, 2001–2018. Nutrients 2023, 15, 2475. [Google Scholar] [CrossRef] [PubMed]
- Asamane, E.A.; Greig, C.A.; Thompson, J.L. The association between nutrient intake, nutritional status and physical function of community-dwelling ethnically diverse older adults. BMC Nutr. 2020, 6, 36. [Google Scholar] [CrossRef] [PubMed]
- Conzade, R.; Koenig, W.; Heier, M.; Schneider, A.; Grill, E.; Peters, A.; Thorand, B. Prevalence and predictors of subclinical micronutrient deficiency in German older adults: Results from the population-based KORA-Age Study. Nutrients 2017, 9, 1276. [Google Scholar] [CrossRef]
- Jun, S.; Cowan, A.E.; Bhadra, A.; Dodd, K.W.; Dwyer, J.T.; Eicher-Miller, H.A.; Gahche, J.J.; Guenther, P.M.; Potischman, N.; Tooze, J.A.; et al. Older adults with obesity have higher risks of some micronutrient inadequacies and lower overall dietary quality compared to peers with a healthy weight, National Health and Nutrition Examination Surveys (NHANES), 2011–2014. Public Health Nutr. 2020, 23, 2268–2279. [Google Scholar] [CrossRef]
- Roman Vinas, B.; Ribas Barba, L.; Ngo, J.; Gurinovic, M.; Novakovic, R.; Cavelaars, A.; de Groot, L.C.; van’t Veer, P.; Matthys, C.; Serra Majem, L. Projected prevalence of inadequate nutrient intakes in Europe. Ann. Nutr. Metab. 2011, 59, 84–95. [Google Scholar] [CrossRef]
- Bartali, B.; Frongillo, E.A.; Guralnik, J.M.; Stipanuk, M.H.; Allore, H.G.; Cherubini, A.; Bandinelli, S.; Ferrucci, L.; Gill, T.M. Serum micronutrient concentrations and decline in physical function among older persons. JAMA 2008, 299, 308–315. [Google Scholar] [CrossRef] [PubMed]
- Hamer, D.H.; Sempertegui, F.; Estrella, B.; Tucker, K.L.; Rodríguez, A.; Egas, J.; Dallal, G.E.; Selhub, J.; Griffiths, J.K.; Meydani, S.N. Micronutrient deficiencies are associated with impaired immune response and higher burden of respiratory infections in elderly Ecuadorians. J. Nutr. 2009, 139, 113–119. [Google Scholar] [CrossRef] [PubMed]
- Fulgoni, K.; Fulgoni, V.L. Beef intake is associated with higher nutrient intake and nutrient adequacy in U.S. adolescents, NHANES 2001–2018. Nutrients 2023, 15, 4996. [Google Scholar] [CrossRef]
- Asp, M.L.; Richardson, J.R.; Collene, A.L.; Droll, K.R.; Belury, M.A. Dietary protein and beef consumption predict for markers of muscle mass and nutrition status in older adults. J. Nutr. Health Aging 2012, 16, 784–790. [Google Scholar] [CrossRef]
- Subar, A.F.; Freedman, L.S.; Tooze, J.A.; Kirkpatrick, S.I.; Boushey, C.; Neuhouser, M.L. Addressing current criticism regarding the value of self-report dietary data. J. Nutr. 2015, 145, 2639–2645. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Total Population | Beef | |||
|---|---|---|---|---|
| Non-Consumers | Consumers | p Value | ||
| Sample N | 5868 | 2072 | 3796 | |
| Population N | 63,614,931 | 20,160,054 | 43,454,877 | |
| Age (mean) | 69.6 ± 0.2 | 70.0 ± 0.3 | 69.4 ± 0.2 | 0.1011 |
| Gender (% Male) | 46.4 ± 0.8 | 38.8 ± 1.5 | 49.9 ± 1.3 | <0.0001 |
| Ethnicity | ||||
| Hispanic (%) | 7.95 ± 0.87 | 9.37 ± 1.04 | 7.29 ± 0.92 | 0.0203 |
| Non-Hispanic White (%) | 77.6 ± 1.5 | 72.1 ± 2.1 | 80.2 ± 1.6 | <0.0001 |
| Non-Hispanic Black (%) | 8.49 ± 0.86 | 10.16 ± 1.11 | 7.71 ± 0.86 | 0.0073 |
| Non-Hispanic Asian (%) | 3.92 ± 0.41 | 6.72 ± 0.84 | 2.63 ± 0.33 | <0.0001 |
| Other (%) | 2.00 ± 0.28 | 1.64 ± 0.33 | 2.16 ± 0.40 | 0.3410 |
| Poverty Income Ratio (PIR) | ||||
| <1.35 (%) | 17.4 ± 1.0 | 20.4 ± 1.5 | 16.1 ± 1.0 | 0.0033 |
| 1.35 ≤ 1.85 (%) | 11.1 ± 0.9 | 10.2 ± 0.9 | 11.4 ± 1.1 | 0.3171 |
| >1.85 (%) | 71.5 ± 1.5 | 69.4 ± 1.9 | 72.5 ± 1.7 | 0.1112 |
| Education | ||||
| ≤High School (%) | 38.3 ± 1.3 | 38.0 ± 1.5 | 38.5 ± 1.5 | 0.7879 |
| Some post-high school education (%) | 29.8 ± 1.3 | 29.0 ± 1.7 | 30.2 ± 1.4 | 0.5153 |
| ≥Bachelor’s degree (%) | 31.9 ± 1.7 | 33.0 ± 1.9 | 31.4 ± 2.1 | 0.4636 |
| Physical Activity | ||||
| Sedentary (%) | 30.8 ± 1.1 | 31.7 ± 1.7 | 30.5 ± 1.3 | 0.5373 |
| Moderate (%) | 43.6 ± 1.2 | 43.5 ± 1.9 | 43.7 ± 1.4 | 0.9392 |
| Vigorous (%) | 25.5 ± 1.1 | 24.8 ± 1.6 | 25.8 ± 1.3 | 0.6037 |
| Smoking Never (%) | 49.8 ± 1.1 | 53.3 ± 1.8 | 48.2 ± 1.2 | 0.0125 |
| Smoking Current (%) | 11.6 ± 0.6 | 9.7 ± 1.0 | 12.5 ± 0.7 | 0.0244 |
| Overweight (%) | 35.4 ± 1.2 | 33.0 ± 1.7 | 36.5 ± 1.4 | 0.1046 |
| Obese (%) | 40.5 ± 1.4 | 39.2 ± 2.1 | 41.1 ± 1.6 | 0.4506 |
| Usual Intake | % Below EAR or Above AI | |
|---|---|---|
| Energy (kcal) | 1936 ± 15 | |
| EAR nutrients | ||
| Protein (g) | 74.2 ± 0.7 | 2.68 ± 0.43 |
| Calcium (mg) | 877 ± 12 | 63.0 ± 1.6 |
| Copper (mg) | 1.23 ± 0.01 | 7.22 ± 0.65 |
| Iron (mg) | 14.2 ± 0.1 | 1.08 ± 0.23 |
| Magnesium (mg) | 291 ± 3 | 60.2 ± 1.3 |
| Phosphorus (mg) | 1277 ± 13 | 1.20 ± 0.27 |
| Selenium (µg) | 104 ± 1 | 0.85 ± 0.20 |
| Zinc (mg) | 10.4 ± 0.1 | 21.5 ± 1.6 |
| Vitamin A, RAE (µg) | 668 ± 14 | 38.9 ± 2.4 |
| Thiamin (mg) | 1.53 ± 0.02 | 7.89 ± 0.85 |
| Riboflavin (mg) | 2.04 ± 0.02 | 2.94 ± 0.41 |
| Niacin (mg) | 23.0 ± 0.3 | 1.89 ± 0.43 |
| Folate, DFE (µg) | 496 ± 6 | 15.2 ± 1.2 |
| Vitamin B6 (mg) | 1.92 ± 0.03 | 19.2 ± 1.5 |
| Vitamin B12 (µg) | 4.67 ± 0.10 | 5.59 ± 0.85 |
| Vitamin C (mg) | 80.8 ± 1.8 | 46.2 ± 1.6 |
| Vitamin D (µg) | 4.66 ± 0.11 | 95.6 ± 0.7 |
| Vitamin E, ATE (mg) | 8.72 ± 0.15 | 84.4 ± 1.3 |
| AI nutrients | ||
| Potassium (mg) | 2626 ± 23 | 29.9 ± 1.2 |
| Sodium (mg) | 3157 ± 28 | 98.5 ± 0.3 |
| Choline (mg) | 316 ± 3 | 3.78 ± 0.61 |
| Usual Intakes | % Meeting Recommendations | |||||
|---|---|---|---|---|---|---|
| Beef Non-Consumers | Beef Consumers | p Value | Beef Non-Consumers | Beef Consumers | p Value | |
| Energy (kcal) | 1775 ± 30 | 2008 ± 22 | <0.0001 | |||
| EAR nutrients | % Below EAR | |||||
| Protein (g) | 68.7 ± 1.4 | 76.7 ± 0.9 | <0.0001 | 5.34 ± 1.09 | 1.34 ± 0.45 | 0.0007 |
| Calcium (mg) | 813 ± 18 | 905 ± 15 | 0.0001 | 71.3 ± 2.0 | 59.1 ± 2.1 | <0.0001 |
| Copper (mg) | 1.21 ± 0.03 | 1.23 ± 0.02 | 0.5427 | 10.4 ± 1.3 | 5.61 ± 0.87 | 0.0016 |
| Iron (mg) | 13.2 ± 0.3 | 14.6 ± 0.2 | <0.0001 | 3.42 ± 0.63 | <1.00 | <0.0001 |
| Magnesium (mg) | 294 ± 6 | 289 ± 4 | 0.5003 | 56.1 ± 2.4 | 62.6 ± 1.6 | 0.0236 |
| Phosphorus (mg) | 1218 ± 22 | 1302 ± 15 | 0.0019 | 1.99 ± 0.43 | <1.00 | 0.0444 |
| Selenium (µg) | 97.5 ± 2.1 | 107 ± 2 | 0.0002 | 2.10 ± 0.53 | <1.00 | 0.0015 |
| Zinc (mg) | 8.82 ± 0.21 | 11.2 ± 0.1 | <0.0001 | 41.5 ± 2.3 | 12.1 ± 1.9 | <0.0001 |
| Vitamin A, RAE (µg) | 662 ± 19 | 670 ± 17 | 0.7599 | 40.1 ± 2.9 | 38.5 ± 3.2 | 0.7120 |
| Thiamin (mg) | 1.46 ± 0.03 | 1.56 ± 0.02 | 0.0169 | 11.3 ± 1.6 | 6.45 ± 1.08 | 0.0135 |
| Riboflavin (mg) | 1.92 ± 0.04 | 2.10 ± 0.03 | 0.0001 | 4.31 ± 0.69 | 2.38 ± 0.50 | 0.0227 |
| Niacin (mg) | 21.8 ± 0.7 | 23.6 ± 0.3 | 0.0174 | 3.22 ± 1.04 | 1.20 ± 0.47 | 0.0765 |
| Folate, DFE (µg) | 488 ± 10 | 499 ± 8 | 0.4247 | 21.3 ± 1.8 | 12.2 ± 1.4 | 0.0001 |
| Vitamin B6 (mg) | 1.92 ± 0.08 | 1.92 ± 0.04 | 0.9565 | 20.4 ± 3.2 | 19.0 ± 1.8 | 0.6847 |
| Vitamin B12 (µg) | 4.03 ± 0.14 | 4.97 ± 0.13 | <0.0001 | 13.4 ± 2.1 | 1.94 ± 0.76 | <0.0001 |
| Vitamin C (mg) | 86.3 ± 3.2 | 78.0 ± 2.3 | 0.0340 | 41.9 ± 2.8 | 48.6 ± 2.0 | 0.0489 |
| Vitamin D (µg) | 4.93 ± 0.15 | 4.54 ± 0.14 | 0.0557 | 94.6 ± 0.9 | 96.0 ± 0.9 | 0.2916 |
| Vitamin E, ATE (mg) | 8.72 ± 0.24 | 8.71 ± 0.19 | 0.9853 | 81.5 ± 1.8 | 85.9 ± 1.8 | 0.0834 |
| AI nutrients | % Above AI | |||||
| Potassium (mg) | 2568 ± 47 | 2656 ± 28 | 0.1065 | 31.3 ± 2.2 | 29.5 ± 1.5 | 0.5117 |
| Sodium (mg) | 2831 ± 51 | 3310 ± 38 | <0.0001 | 96.9 ± 0.8 | 99.2 ± 0.3 | 0.0062 |
| Choline (mg) | 300 ± 6 | 324 ± 4 | 0.0010 | 4.23 ± 1.16 | 3.71 ± 0.70 | 0.6965 |
| Usual Intakes | % Meeting Recommendations | |||||
|---|---|---|---|---|---|---|
| Fresh Beef Non-Consumers | Fresh Beef Consumers | p Value | Fresh Beef Non-Consumers | Fresh Beef Consumers | p Value | |
| Energy (kcal) | 1812 ± 28 | 2017 ± 23 | <0.0001 | |||
| EAR nutrients | % Below EAR | |||||
| Protein (g) | 69.2 ± 1.3 | 77.5 ± 0.9 | <0.0001 | 4.96 ± 0.96 | 1.00 ± 0.36 | 0.0001 |
| Calcium (mg) | 835 ± 17 | 904 ± 16 | 0.0032 | 68.8 ± 1.9 | 59.3 ± 2.3 | 0.0017 |
| Copper (mg) | 1.19 ± 0.02 | 1.25 ± 0.02 | 0.0865 | 10.8 ± 1.1 | 4.87 ± 0.92 | <0.0001 |
| Iron (mg) | 13.2 ± 0.2 | 14.8 ± 0.2 | <0.0001 | 2.83 ± 0.47 | <1.00 | <0.0001 |
| Magnesium (mg) | 288 ± 5 | 292 ± 4 | 0.5622 | 58.5 ± 2.0 | 61.5 ± 1.9 | 0.2655 |
| Phosphorus (mg) | 1226 ± 21 | 1308 ± 16 | 0.0020 | 1.95 ± 0.47 | <1.00 | 0.0170 |
| Selenium (µg) | 98.6 ± 1.9 | 108 ± 2 | 0.0003 | 1.89 ± 0.54 | <1.00 | 0.0022 |
| Zinc (mg) | 8.87 ± 0.17 | 11.5 ± 0.2 | <0.0001 | 40.8 ± 2.0 | 7.99 ± 1.90 | <0.0001 |
| Vitamin A, RAE (µg) | 665 ± 16 | 670 ± 18 | 0.8359 | 39.4 ± 2.7 | 39.1 ± 3.2 | 0.9465 |
| Thiamin (mg) | 1.47 ± 0.03 | 1.57 ± 0.03 | 0.0091 | 10.9 ± 1.4 | 5.80 ± 1.05 | 0.0038 |
| Riboflavin (mg) | 1.92 ± 0.03 | 2.13 ± 0.03 | <0.0001 | 4.29 ± 0.68 | 1.96 ± 0.49 | 0.0055 |
| Niacin (mg) | 21.9 ± 0.6 | 23.8 ± 0.4 | 0.0042 | 3.48 ± 1.01 | <1.00 | 0.0127 |
| Folate, DFE (µg) | 485 ± 9 | 503 ± 9 | 0.1539 | 20.8 ± 1.8 | 11.2 ± 1.4 | <0.0001 |
| Vitamin B6 (mg) | 1.87 ± 0.07 | 1.95 ± 0.04 | 0.2749 | 21.8 ± 3.1 | 17.0 ± 1.6 | 0.1704 |
| Vitamin B12 (µg) | 4.05 ± 0.11 | 5.08 ± 0.15 | <0.0001 | 12.1 ± 1.6 | 1.41 ± 0.69 | <0.0001 |
| Vitamin C (mg) | 83.7 ± 2.8 | 79.0 ± 2.4 | 0.2069 | 44.2 ± 2.5 | 47.4 ± 2.0 | 0.3094 |
| Vitamin D (µg) | 4.84 ± 0.14 | 4.55 ± 0.15 | 0.1467 | 95.4 ± 0.9 | 95.7 ± 1.0 | 0.8196 |
| Vitamin E, ATE (mg) | 8.63 ± 0.21 | 8.76 ± 0.21 | 0.6730 | 82.5 ± 1.6 | 85.7 ± 2.0 | 0.2184 |
| AI nutrients | % Above AI | |||||
| Potassium (mg) | 2540 ± 40 | 2690 ± 31 | 0.0032 | 29.4 ± 1.8 | 30.7 ± 1.7 | 0.6006 |
| Sodium (mg) | 2914 ± 48 | 3321 ± 42 | <0.0001 | 97.3 ± 0.7 | 99.2 ± 0.3 | 0.0070 |
| Choline (mg) | 297 ± 5 | 328 ± 4 | <0.0001 | 3.25 ± 0.78 | 4.03 ± 0.85 | 0.4974 |
| Usual Intakes | % Meeting Recommendations | |||||
|---|---|---|---|---|---|---|
| Ground Beef Non-Consumers | Ground Beef Consumers | p Value | Ground Beef Non-Consumers | Ground Beef Consumers | p Value | |
| Energy (kcal) | 1836 ± 23 | 2087 ± 31 | <0.0001 | |||
| EAR nutrients | % Below EAR | |||||
| Protein (gm) | 71.3 ± 1.0 | 78.6 ± 1.1 | <0.0001 | 3.03 ± 0.72 | 1.14 ± 0.39 | 0.0205 |
| Calcium (mg) | 831 ± 14 | 944 ± 19 | <0.0001 | 68.6 ± 1.5 | 54.7 ± 3.1 | 0.0001 |
| Copper (mg) | 1.19 ± 0.02 | 1.28 ± 0.03 | 0.0039 | 9.41 ± 0.92 | 4.32 ± 0.82 | <0.0001 |
| Iron (mg) | 13.5 ± 0.2 | 15.3 ± 0.3 | <0.0001 | 1.79 ± 0.38 | <1.00 | <0.0001 |
| Magnesium (mg) | 285 ± 4 | 299 ± 5 | 0.0244 | 61.0 ± 1.6 | 58.0 ± 2.2 | 0.2721 |
| Phosphorus (mg) | 1234 ± 16 | 1341 ± 19 | <0.0001 | 1.64 ± 0.41 | <1.00 | 0.0138 |
| Selenium (mcg) | 101 ± 1 | 110 ± 2 | 0.0004 | 1.15 ± 0.40 | <1.00 | 0.0238 |
| Zinc (mg) | 9.54 ± 0.13 | 11.8 ± 0.2 | <0.0001 | 32.3 ± 2.0 | 8.17 ± 2.12 | <0.0001 |
| Vitamin A, RAE (µg) | 669 ± 14 | 667 ± 22 | 0.9468 | 38.7 ± 2.7 | 40.4 ± 3.7 | 0.7108 |
| Thiamin (mg) | 1.47 ± 0.02 | 1.62 ± 0.3 | 0.0001 | 10.4 ± 1.1 | 4.26 ± 0.83 | <0.0001 |
| Riboflavin (mg) | 1.96 ± 0.02 | 2.17 ± 0.04 | <0.0001 | 3.49 ± 0.55 | 1.84 ± 0.51 | 0.0272 |
| Niacin (mg) | 22.2 ± 0.4 | 24.3 ± 0.4 | 0.0002 | 2.72 ± 0.67 | <1.00 | 0.0054 |
| Folate, DFE (µg) | 480 ± 7 | 521 ± 12 | 0.0028 | 19.7 ± 1.6 | 8.31 ± 1.41 | <0.0001 |
| Vitamin B6 (mg) | 1.90 ± 0.04 | 1.95 ± 0.05 | 0.4765 | 20.3 ± 2.2 | 17.2 ± 2.2 | 0.3272 |
| Vitamin B12 (mcg) | 4.31 ± 0.10 | 5.25 ± 0.18 | <0.0001 | 7.98 ± 1.44 | 1.49 ± 0.61 | <0.0001 |
| Vitamin C (mg) | 81.4 ± 2.2 | 79.8 ± 2.9 | 0.6566 | 45.3 ± 1.9 | 47.7 ± 2.4 | 0.4382 |
| Vitamin D (µg) | 4.74 ± 0.15 | 4.54 ± 0.15 | 0.3240 | 95.4 ± 1.0 | 96.1 ± 1.0 | 0.6296 |
| Vitamin E, ATE (mg) | 8.46 ± 0.17 | 9.07 ± 0.26 | 0.0524 | 85.1 ± 1.4 | 82.8 ± 2.5 | 0.4225 |
| AI nutrients | % Above AI | |||||
| Potassium (mg) | 2561 ± 30 | 2732 ± 35 | 0.0002 | 28.4 ± 1.6 | 33.1 ± 1.8 | 0.0462 |
| Sodium (mg) | 2975 ± 34 | 3433 ± 56 | <0.0001 | 97.8 ± 0.5 | 99.5 ± 0.2 | 0.0007 |
| Choline (mg) | 307 ± 4 | 330 ± 6 | 0.0012 | 3.26 ± 0.70 | 4.66 ± 1.12 | 0.2895 |
| Usual Intakes | % Meeting Recommendations | |||||
|---|---|---|---|---|---|---|
| Processed Beef Non-Consumers | Processed Beef Consumers | p Value | Processed Beef Non-Consumers | Processed Beef Consumers | p Value | |
| Energy (kcal) | 1887 ± 17 | 2094 ± 37 | <0.0001 | |||
| EAR nutrients | % Below EAR | |||||
| Protein (g) | 73.1 ± 0.9 | 77.6 ± 1.6 | 0.0138 | 3.02 ± 0.51 | 1.02 ± 0.62 | 0.0129 |
| Calcium (mg) | 860 ± 15 | 925 ± 23 | 0.0178 | 65.4 ± 1.8 | 56.1 ± 3.0 | 0.0089 |
| Copper (mg) | 1.22 ± 0.02 | 1.25 ± 0.04 | 0.4341 | 7.54 ± 0.79 | 6.54 ± 1.43 | 0.5384 |
| Iron (mg) | 13.9 ± 0.2 | 15.0 ± 0.3 | 0.0025 | 1.09 ± 0.27 | <1.00 | 0.0223 |
| Magnesium (mg) | 293 ± 4 | 283 ± 7 | 0.1997 | 58.0 ± 1.6 | 67.0 ± 2.7 | 0.0041 |
| Phosphorus (mg) | 1261 ± 15 | 1323 ± 2.8 | 0.0495 | 1.35 ± 0.28 | <1.00 | 0.1154 |
| Selenium (µg) | 102 ± 1 | 112 ± 3 | 0.0016 | 1.03 ± 0.28 | <1.00 | 0.0032 |
| Zinc (mg) | 10.2 ± 0.1 | 11.1 ± 0.2 | 0.0013 | 24.7 ± 1.6 | 15.2 ± 3.4 | 0.0109 |
| Vitamin A, RAE (µg) | 669 ± 14 | 671 ± 35 | 0.9388 | 39.5 ± 2.4 | 36.9 ± 6.6 | 0.7085 |
| Thiamin (mg) | 1.51 ± 0.02 | 1.60 ± 0.5 | 0.0463 | 8.70 ± 0.93 | 5.64 ± 1.79 | 0.1294 |
| Riboflavin (mg) | 2.02 ± 0.002 | 2.13 ± 0.05 | 0.0359 | 3.19 ± 0.49 | 2.29 ± 0.68 | 0.2827 |
| Niacin (mg) | 22.7 ± 0.4 | 24.0 ± 0.7 | 0.0867 | 1.87 ± 0.45 | 1.76 ± 0.95 | 0.9200 |
| Folate, DFE (µg) | 491 ± 7 | 514 ± 16 | 0.1868 | 16.4 ± 1.3 | 11.9 ± 2.3 | 0.0851 |
| Vitamin B6 (mg) | 1.94 ± 0.04 | 1.85 ± 0.06 | 0.1700 | 18.7 ± 1.7 | 21.1 ± 4.1 | 0.5952 |
| Vitamin B12 (µg) | 4.54 ± 0.12 | 5.09 ± 0.23 | 0.0368 | 6.62 ± 1.22 | 1.93 ± 1.01 | 0.0030 |
| Vitamin C (mg) | 83.7 ± 2.1 | 72.0 ± 3.8 | 0.0065 | 43.1 ± 1.8 | 56.3 ± 3.1 | 0.0002 |
| Vitamin D (µg) | 4.76 ± 0.14 | 4.36 ± 0.22 | 0.1194 | 94.8 ± 0.9 | 98.3 ± 1.2 | 0.0169 |
| Vitamin E, ATE (mg) | 8.67 ± 0.17 | 8.88 ± 0.29 | 0.5221 | 83.9 ± 1.4 | 84.4 ± 3.0 | 0.8716 |
| AI nutrients | % Above AI | |||||
| Potassium (mg) | 2635 ± 29 | 2618 ± 51 | 0.7648 | 31.7 ± 1.4 | 25.0 ± 2.4 | 0.0180 |
| Sodium (mg) | 3036 ± 33 | 3553 ± 86 | <0.0001 | 98.0 ± 0.4 | 99.8 ± 0.2 | <0.0001 |
| Choline (mg) | 311 ± 4 | 330 ± 8 | 0.0322 | 3.97 ± 0.71 | 2.95 ± 1.28 | 0.4898 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Agarwal, S.; Fulgoni, V.L., III. Beef Consumption Is Associated with Higher Intakes and Adequacy of Key Nutrients in Older Adults Age 60+ Years: National Health and Nutrition Examination Survey 2011–2018 Analysis. Nutrients 2024, 16, 1779. https://doi.org/10.3390/nu16111779
Agarwal S, Fulgoni VL III. Beef Consumption Is Associated with Higher Intakes and Adequacy of Key Nutrients in Older Adults Age 60+ Years: National Health and Nutrition Examination Survey 2011–2018 Analysis. Nutrients. 2024; 16(11):1779. https://doi.org/10.3390/nu16111779
Chicago/Turabian StyleAgarwal, Sanjiv, and Victor L. Fulgoni, III. 2024. "Beef Consumption Is Associated with Higher Intakes and Adequacy of Key Nutrients in Older Adults Age 60+ Years: National Health and Nutrition Examination Survey 2011–2018 Analysis" Nutrients 16, no. 11: 1779. https://doi.org/10.3390/nu16111779
APA StyleAgarwal, S., & Fulgoni, V. L., III. (2024). Beef Consumption Is Associated with Higher Intakes and Adequacy of Key Nutrients in Older Adults Age 60+ Years: National Health and Nutrition Examination Survey 2011–2018 Analysis. Nutrients, 16(11), 1779. https://doi.org/10.3390/nu16111779