
Nutritional and Lifestyle Therapy for NAFLD in People with HIV
 , ,
, , 
Abstract
1. Introduction
2. Methods
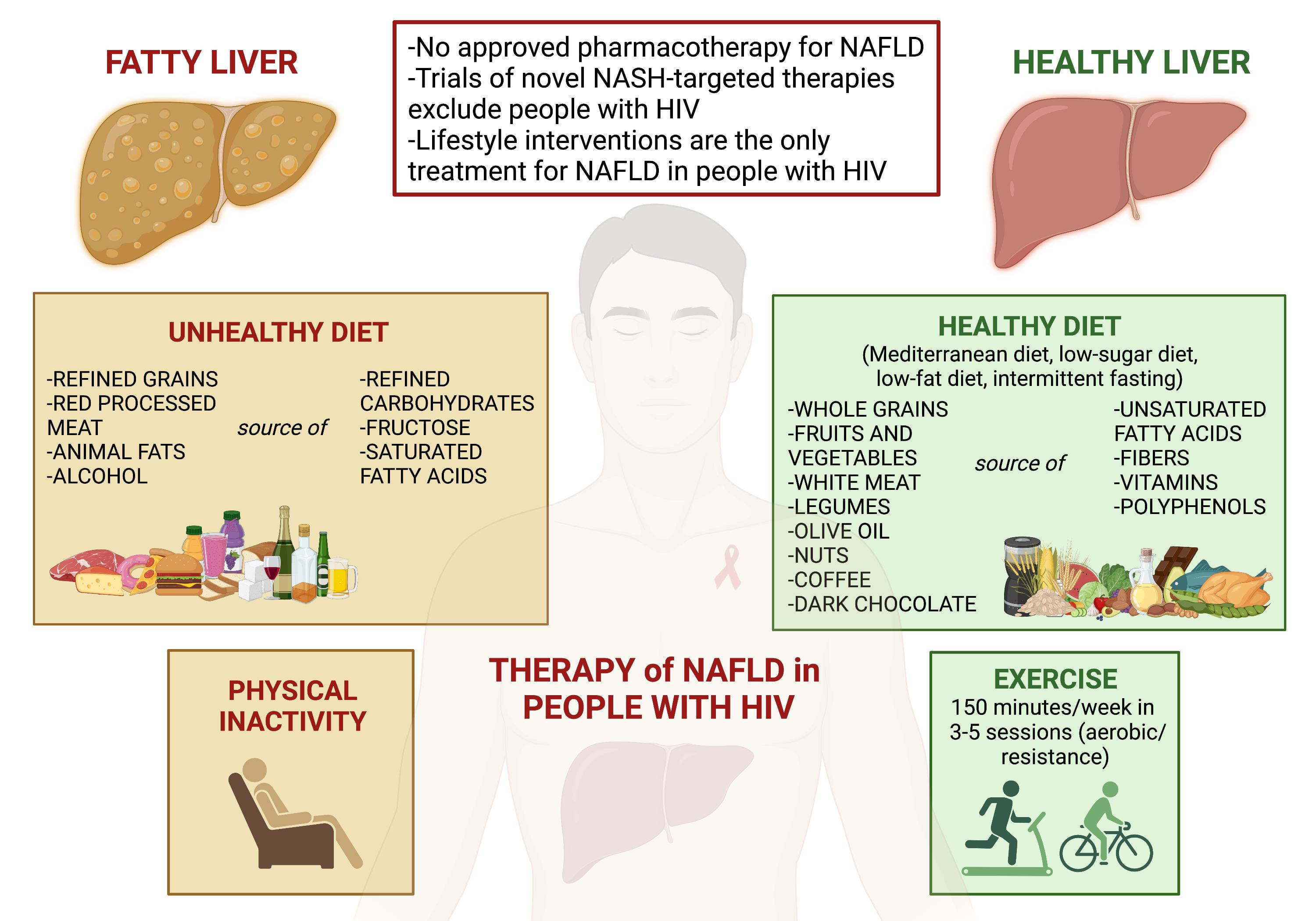
3. The Role of Nutrients in NAFLD in People with HIV
3.1. Nutrients in NAFLD
3.1.1. Macronutrients
Carbohydrates
Lipids
Proteins
Alcohol
Coffee
3.1.2. Micronutrients
Vitamin E
Vitamin D
Polyphenols
Cannabinoid
3.2. Nutrients in NAFLD in People with HIV
3.2.1. Macronutrients
Lipids
Alcohol
Coffee
3.2.2. Micronutrients
Vitamin E
Vitamin D
Cannabinoids
3.3. Food Insecurity
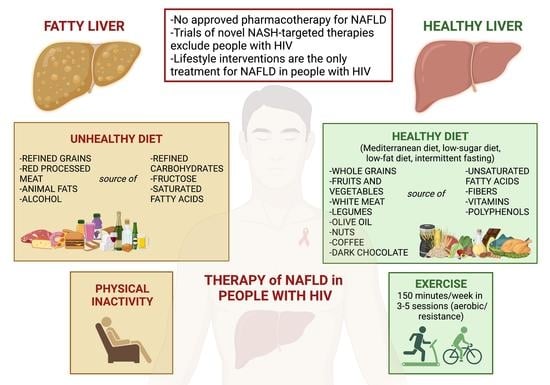
4. Nutrition, Lifestyle and Pharmacotherapy in the Treatment of NAFLD in People with HIV
4.1. Lifestyle Interventions in NAFLD in People with HIV
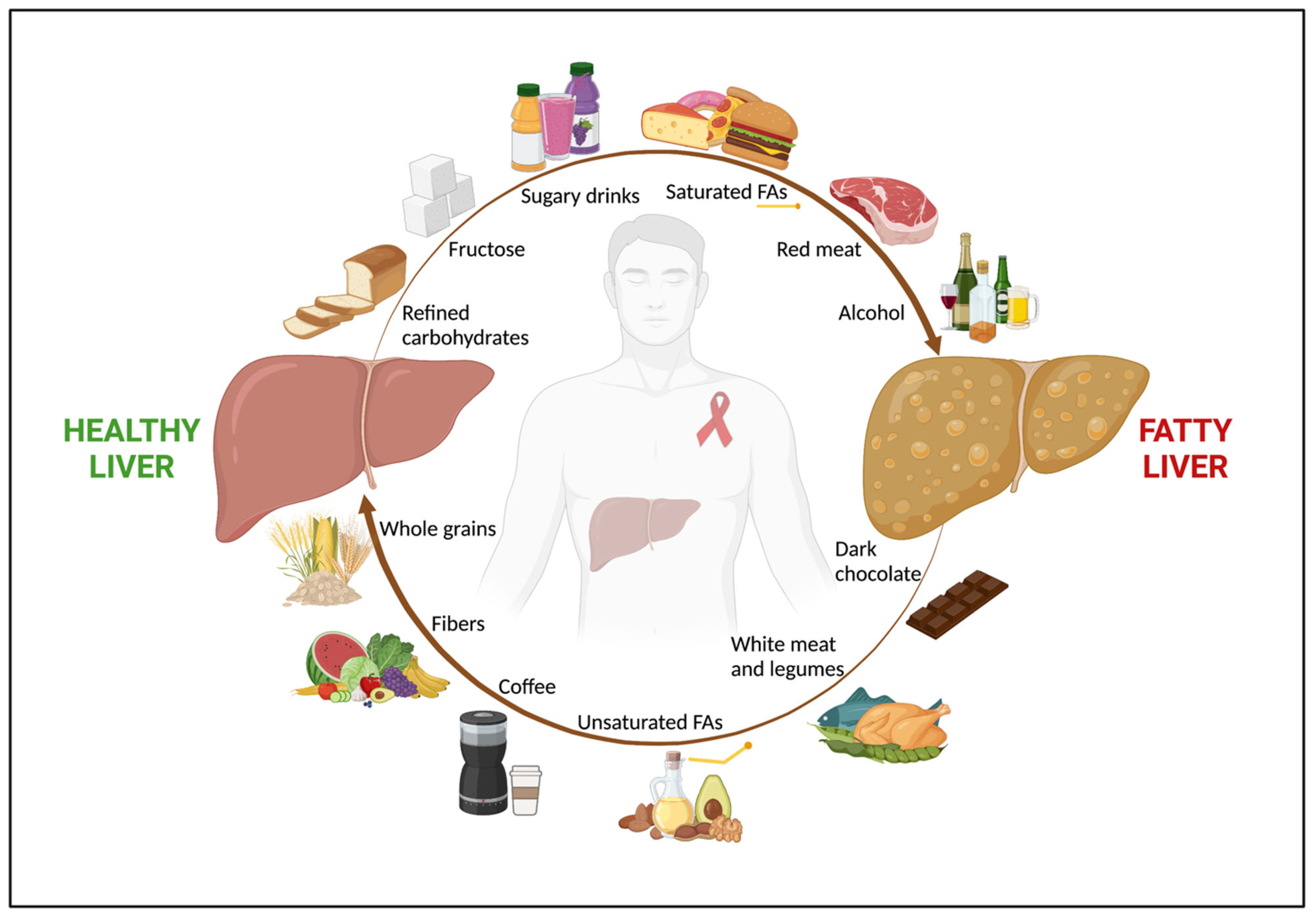
4.1.1. Lifestyle Treatment of NAFLD
4.1.2. Lifestyle Treatment of NAFLD in People with HIV
4.2. The State of the Art NAFLD Pharmacotherapy in People with HIV
4.3. Lifestyle Treatment of Lean NAFLD in People with HIV
4.4. The Role of Gut Microbiota in Lifestyle Treatment of NAFLD in People with HIV
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Global HIV & AIDS Statistics—Fact Sheet. Available online: https://www.unaids.org/en/resources/fact-sheet (accessed on 28 January 2023).
- Palella, F.J.; Loveless, M.O.; Holmberg, S.D. Declining Morbidity and Mortality among Patients with Advanced Human Immunodeficiency Virus Infection. N. Engl. J. Med. 1998, 383, 853–860. [Google Scholar] [CrossRef] [PubMed]
- Xia, Q.; Maduro, G.A.; Li, W.; Huynh, M.; Torian, L.V. Life Expectancy Among People with HIV in New York City, 2009–2018. JAIDS J. Acquir. Immune Defic. Syndr. 2022, 91, 434–438. [Google Scholar] [CrossRef] [PubMed]
- Croxford, S.; Kitching, A.; Desai, S.; Kall, M.; Edelstein, M.; Skingsley, A.; Burns, F.; Copas, A.; Brown, A.E.; Sullivan, A.K.; et al. Mortality and Causes of Death in People Diagnosed with HIV in the Era of Highly Active Antiretroviral Therapy Compared with the General Population: An Analysis of a National Observational Cohort. Lancet Public Health 2017, 2, e35–e46. [Google Scholar] [CrossRef] [PubMed]
- Guaraldi, G.; Milic, J.; Mussini, C. Aging with HIV. Curr. HIV/AIDS Rep. 2019, 16, 475–481. [Google Scholar] [CrossRef] [PubMed]
- Guaraldi, G.; Orlando, G.; Zona, S.; Menozzi, M.; Carli, F.; Garlassi, E.; Berti, A.; Rossi, E.; Roverato, A.; Palella, F. Premature Age-Related Comorbidities Among HIV-Infected Persons Compared with the General Population. Clin. Infect. Dis. 2011, 53, 1120–1126. [Google Scholar] [CrossRef]
- Ghosn, J.; Taiwo, B.; Seedat, S.; Autran, B.; Katlama, C. HIV. The Lancet 2018, 392, 685–697. [Google Scholar] [CrossRef]
- Kaspar, M.B.; Sterling, R.K. Mechanisms of Liver Disease in Patients Infected with HIV. BMJ Open Gastroenterol. 2017, 4, e000166. [Google Scholar] [CrossRef]
- Younossi, Z.; Anstee, Q.M.; Marietti, M.; Hardy, T.; Henry, L.; Eslam, M.; George, J.; Bugianesi, E. Global Burden of NAFLD and NASH: Trends, Predictions, Risk Factors and Prevention. Nat. Rev. Gastroenterol. Hepatol. 2018, 15, 11–20. [Google Scholar] [CrossRef]
- Rinella, M.E.; Neuschwander-Tetri, B.A.; Siddiqui, M.S.; Abdelmalek, M.F.; Caldwell, S.; Barb, D.; Kleiner, D.E.; Loomba, R. AASLD Practice Guidance on the Clinical Assessment and Management of Nonalcoholic Fatty Liver Disease. Hepatology 2023. [Google Scholar] [CrossRef]
- Pais, R.; Maurel, T. Natural History of NAFLD. J. Clin. Med. 2021, 10, 1161. [Google Scholar] [CrossRef]
- Younossi, Z.M.; Golabi, P.; de Avila, L.; Paik, J.M.; Srishord, M.; Fukui, N.; Qiu, Y.; Burns, L.; Afendy, A.; Nader, F. The Global Epidemiology of NAFLD and NASH in Patients with Type 2 Diabetes: A Systematic Review and Meta-Analysis. J. Hepatol. 2019, 71, 793–801. [Google Scholar] [CrossRef]
- Eslam, M.; Sanyal, A.J.; George, J.; Sanyal, A.; Neuschwander-Tetri, B.; Tiribelli, C.; Kleiner, D.E.; Brunt, E.; Bugianesi, E.; Yki-Järvinen, H.; et al. MAFLD: A Consensus-Driven Proposed Nomenclature for Metabolic Associated Fatty Liver Disease. Gastroenterology 2020, 158, 1999–2014.e1. [Google Scholar] [CrossRef] [PubMed]
- Eslam, M.; Newsome, P.N.; Sarin, S.K.; Anstee, Q.M.; Targher, G.; Romero-Gomez, M.; Zelber-Sagi, S.; Wai-Sun Wong, V.; Dufour, J.-F.; Schattenberg, J.M.; et al. A New Definition for Metabolic Dysfunction-Associated Fatty Liver Disease: An International Expert Consensus Statement. J. Hepatol. 2020, 73, 202–209. [Google Scholar] [CrossRef]
- Lonardo, A.; Leoni, S.; Alswat, K.A.; Fouad, Y. History of Nonalcoholic Fatty Liver Disease. Int. J. Mol. Sci. 2020, 21, 5888. [Google Scholar] [CrossRef]
- Cervo, A.; Shengir, M.; Patel, K.; Sebastiani, G. NASH in HIV. Curr. HIV/AIDS Rep. 2020, 17, 601–614. [Google Scholar] [CrossRef]
- Maurice, J.B.; Patel, A.; Scott, A.J.; Patel, K.; Thursz, M.; Lemoine, M. Prevalence and Risk Factors of Nonalcoholic Fatty Liver Disease in HIV-Monoinfection. AIDS 2017, 31, 1621–1632. [Google Scholar] [CrossRef]
- Kalligeros, M.; Vassilopoulos, A.; Shehadeh, F.; Vassilopoulos, S.; Lazaridou, I.; Mylonakis, E.; Promrat, K.; Wands, J.R. Prevalence and Characteristics of Nonalcoholic Fatty Liver Disease and Fibrosis in People Living with HIV Monoinfection: A Systematic Review and Meta-Analysis. Clin. Gastroenterol. Hepatol. 2023. [Google Scholar] [CrossRef]
- Verna, E.C. Non-Alcoholic Fatty Liver Disease and Non-Alcoholic Steatohepatitis in Patients with HIV. Lancet Gastroenterol. Hepatol. 2017, 2, 211–223. [Google Scholar] [CrossRef]
- Guaraldi, G.; Lonardo, A.; Maia, L.; Palella, F.J. Metabolic Concerns in Aging HIV-Infected Persons: From Serum Lipid Phenotype to Fatty Liver. AIDS 2017, 31, S147–S156. [Google Scholar] [CrossRef]
- Zelber-Sagi, S. Nutrition and Physical Activity in NAFLD: An Overview of the Epidemiological Evidence. WJG 2011, 17, 3377. [Google Scholar] [CrossRef]
- EASL–EASD–EASO. Clinical Practice Guidelines for the Management of Non-Alcoholic Fatty Liver Disease. J. Hepatol. 2016, 64, 1388–1402. [Google Scholar] [CrossRef] [PubMed]
- Chakravarthy, M.V.; Waddell, T.; Banerjee, R.; Guess, N. Nutrition and Nonalcoholic Fatty Liver Disease. Gastroenterol. Clin. North Am. 2020, 49, 63–94. [Google Scholar] [CrossRef] [PubMed]
- Sevastianova, K.; Santos, A.; Kotronen, A.; Hakkarainen, A.; Makkonen, J.; Silander, K.; Peltonen, M.; Romeo, S.; Lundbom, J.; Lundbom, N.; et al. Effect of Short-Term Carbohydrate Overfeeding and Long-Term Weight Loss on Liver Fat in Overweight Humans. Am. J. Clin. Nutr. 2012, 96, 727–734. [Google Scholar] [CrossRef] [PubMed]
- Nseir, W.; Nassar, F.; Assy, N. Soft Drinks Consumption and Nonalcoholic Fatty Liver Disease. World J. Gastroenterol. 2010, 16, 2579–2588. [Google Scholar] [CrossRef]
- Abid, A.; Taha, O.; Nseir, W.; Farah, R.; Grosovski, M.; Assy, N. Soft Drink Consumption Is Associated with Fatty Liver Disease Independent of Metabolic Syndrome. J. Hepatol. 2009, 51, 918–924. [Google Scholar] [CrossRef]
- Zhao, H.; Yang, A.; Mao, L.; Quan, Y.; Cui, J.; Sun, Y. Association Between Dietary Fiber Intake and Non-Alcoholic Fatty Liver Disease in Adults. Front. Nutr. 2020, 7, 593735. [Google Scholar] [CrossRef]
- Zolfaghari, H.; Askari, G.; Siassi, F.; Feizi, A.; Sotoudeh, G. Intake of Nutrients, Fiber, and Sugar in Patients with Nonalcoholic Fatty Liver Disease in Comparison to Healthy Individuals. Int. J. Prev. Med. 2016, 7, 98. [Google Scholar] [CrossRef]
- Krawczyk, M.; Maciejewska, D.; Ryterska, K.; Czerwińka-Rogowska, M.; Jamioł-Milc, D.; Skonieczna-Żydecka, K.; Milkiewicz, P.; Raszeja-Wyszomirska, J.; Stachowska, E. Gut Permeability Might Be Improved by Dietary Fiber in Individuals with Nonalcoholic Fatty Liver Disease (NAFLD) Undergoing Weight Reduction. Nutrients 2018, 10, 1793. [Google Scholar] [CrossRef]
- Barber, T.M.; Kabisch, S.; Pfeiffer, A.F.H.; Weickert, M.O. The Health Benefits of Dietary Fibre. Nutrients 2020, 12, 3209. [Google Scholar] [CrossRef]
- Ahmadi, S.; Mainali, R.; Nagpal, R.; Sheikh-Zeinoddin, M.; Soleimanian-Zad, S.; Wang, S.; Deep, G.; Kumar Mishra, S.; Yadav, H. Dietary Polysaccharides in the Amelioration of Gut Microbiome Dysbiosis and Metabolic Diseases. Obes. Control Ther. 2017, 4, 7058–7069. [Google Scholar] [CrossRef]
- Parry, S.A.; Hodson, L. Influence of Dietary Macronutrients on Liver Fat Accumulation and Metabolism. J. Investig. Med. 2017, 65, 1102–1115. [Google Scholar] [CrossRef]
- Errazuriz, I.; Dube, S.; Slama, M.; Visentin, R.; Nayar, S.; O’Connor, H.; Cobelli, C.; Das, S.K.; Basu, A.; Kremers, W.K.; et al. Randomized Controlled Trial of a MUFA or Fiber-Rich Diet on Hepatic Fat in Prediabetes. J. Clin. Endocrinol. Metab. 2017, 102, 1765–1774. [Google Scholar] [CrossRef]
- Capanni, M.; Calella, F.; Biagini, M.R.; Genise, S.; Raimondi, L.; Bedogni, G.; Svegliati-Baroni, G.; Sofi, F.; Milani, S.; Abbate, R.; et al. Prolonged N-3 Polyunsaturated Fatty Acid Supplementation Ameliorates Hepatic Steatosis in Patients with Non-Alcoholic Fatty Liver Disease: A Pilot Study. Aliment. Pharmacol. Ther. 2006, 23, 1143–1151. [Google Scholar] [CrossRef]
- Cortez-Pinto, H.; Jesus, L.; Barros, H.; Lopes, C.; Moura, M.C.; Camilo, M.E. How Different Is the Dietary Pattern in Non-Alcoholic Steatohepatitis Patients? Clin. Nutr. 2006, 25, 816–823. [Google Scholar] [CrossRef]
- Tricò, D.; Biancalana, E.; Solini, A. Protein and Amino Acids in Nonalcoholic Fatty Liver Disease. Curr. Opin. Clin. Nutr. Metab. Care 2021, 24, 96–101. [Google Scholar] [CrossRef] [PubMed]
- Zelber-Sagi, S.; Ivancovsky-Wajcman, D.; Fliss Isakov, N.; Webb, M.; Orenstein, D.; Shibolet, O.; Kariv, R. High Red and Processed Meat Consumption Is Associated with Non-Alcoholic Fatty Liver Disease and Insulin Resistance. J. Hepatol. 2018, 68, 1239–1246. [Google Scholar] [CrossRef] [PubMed]
- Hashemian, M.; Merat, S.; Poustchi, H.; Jafari, E.; Radmard, A.-R.; Kamangar, F.; Freedman, N.; Hekmatdoost, A.; Sheikh, M.; Boffetta, P.; et al. Red Meat Consumption and Risk of Nonalcoholic Fatty Liver Disease in a Population with Low Meat Consumption: The Golestan Cohort Study. Am. J. Gastroenterol. 2021, 116, 1667–1675. [Google Scholar] [CrossRef]
- Dunn, W.; Sanyal, A.J.; Brunt, E.M.; Unalp-Arida, A.; Donohue, M.; McCullough, A.J.; Schwimmer, J.B. Modest Alcohol Consumption Is Associated with Decreased Prevalence of Steatohepatitis in Patients with Nonalcoholic Fatty Liver Disease (NAFLD). J. Hepatol. 2012, 57, 384–391. [Google Scholar] [CrossRef]
- Kwon, H.K.; Greenson, J.K.; Conjeevaram, H.S. Effect of Lifetime Alcohol Consumption on the Histological Severity of Non-Alcoholic Fatty Liver Disease. Liver Int. 2014, 34, 129–135. [Google Scholar] [CrossRef]
- Kashiwagi, K.; Yamaguchi, A.; Shiba, S.; Taniki, N.; Inoue, N.; Takaishi, H.; Iwao, Y.; Kanai, T. Moderate Alcohol Consumption Is Not Associated with Subclinical Cardiovascular Damage but with Hepatic Fibrosis in Non-Alcoholic Fatty Liver Disease. Alcohol 2020, 89, 1–7. [Google Scholar] [CrossRef]
- Blomdahl, J.; Nasr, P.; Ekstedt, M.; Kechagias, S. Moderate Alcohol Consumption Is Associated with Advanced Fibrosis in Non-Alcoholic Fatty Liver Disease and Shows a Synergistic Effect with Type 2 Diabetes Mellitus. Metabolism 2021, 115, 154439. [Google Scholar] [CrossRef]
- Ascha, M.S.; Hanouneh, I.A.; Lopez, R.; Tamimi, T.A.-R.; Feldstein, A.F.; Zein, N.N. The Incidence and Risk Factors of Hepatocellular Carcinoma in Patients with Nonalcoholic Steatohepatitis. Hepatology 2010, 51, 1972–1978. [Google Scholar] [CrossRef]
- Jarvis, H.; O’Keefe, H.; Craig, D.; Stow, D.; Hanratty, B.; Anstee, Q.M. Does Moderate Alcohol Consumption Accelerate the Progression of Liver Disease in NAFLD? A Systematic Review and Narrative Synthesis. BMJ Open 2022, 12, e049767. [Google Scholar] [CrossRef] [PubMed]
- Sinn, D.H.; Gwak, G.-Y.; Cho, J.; Son, H.J.; Paik, Y.-H.; Choi, M.S.; Lee, J.H.; Koh, K.C.; Paik, S.W.; Yoo, B.C. Modest Alcohol Consumption and Carotid Plaques or Carotid Artery Stenosis in Men with Non-Alcoholic Fatty Liver Disease. Atherosclerosis 2014, 234, 270–275. [Google Scholar] [CrossRef]
- VanWagner, L.B.; Ning, H.; Allen, N.B.; Ajmera, V.; Lewis, C.E.; Carr, J.J.; Lloyd-Jones, D.M.; Terrault, N.A.; Siddique, J. Alcohol Use and Cardiovascular Disease Risk in Patients with Nonalcoholic Fatty Liver Disease. Gastroenterology 2017, 153, 1260–1272.e3. [Google Scholar] [CrossRef]
- Butt, M.S.; Sultan, M.T. Coffee and Its Consumption: Benefits and Risks. Crit. Rev. Food Sci. Nutr. 2011, 51, 363–373. [Google Scholar] [CrossRef]
- Wadhawan, M.; Anand, A.C. Coffee and Liver Disease. J. Clin. Exp. Hepatol. 2016, 6, 40–46. [Google Scholar] [CrossRef]
- Sewter, R.; Heaney, S.; Patterson, A. Coffee Consumption and the Progression of NAFLD: A Systematic Review. Nutrients 2021, 13, 2381. [Google Scholar] [CrossRef]
- Anty, R.; Marjoux, S.; Iannelli, A.; Patouraux, S.; Schneck, A.-S.; Bonnafous, S.; Gire, C.; Amzolini, A.; Ben-Amor, I.; Saint-Paul, M.-C.; et al. Regular Coffee but Not Espresso Drinking Is Protective against Fibrosis in a Cohort Mainly Composed of Morbidly Obese European Women with NAFLD Undergoing Bariatric Surgery. J. Hepatol. 2012, 57, 1090–1096. [Google Scholar] [CrossRef]
- Saab, S.; Mallam, D.; Cox II, G.A.; Tong, M.J. Impact of Coffee on Liver Diseases: A Systematic Review. Liver Int. 2014, 34, 495–504. [Google Scholar] [CrossRef]
- Dranoff, J.A. Coffee Consumption and Prevention of Cirrhosis: In Support of the Caffeine Hypothesis. Gene Expr. 2018, 18, 1–3. [Google Scholar] [CrossRef] [PubMed]
- Mansour, A.; Mohajeri-Tehrani, M.R.; Samadi, M.; Qorbani, M.; Merat, S.; Adibi, H.; Poustchi, H.; Hekmatdoost, A. Effects of Supplementation with Main Coffee Components Including Caffeine and/or Chlorogenic Acid on Hepatic, Metabolic, and Inflammatory Indices in Patients with Non-Alcoholic Fatty Liver Disease and Type 2 Diabetes: A Randomized, Double-Blind, Placebo-Controlled, Clinical Trial. Nutr. J. 2021, 20, 35. [Google Scholar] [CrossRef] [PubMed]
- Dongiovanni, P.; Lanti, C.; Riso, P.; Valenti, L. Nutritional Therapy for Nonalcoholic Fatty Liver Disease. J. Nutr. Biochem. 2016, 29, 1–11. [Google Scholar] [CrossRef]
- Perumpail, B.; Li, A.; John, N.; Sallam, S.; Shah, N.; Kwong, W.; Cholankeril, G.; Kim, D.; Ahmed, A. The Role of Vitamin E in the Treatment of NAFLD. Diseases 2018, 6, 86. [Google Scholar] [CrossRef]
- Sanyal, A.J.; Chalasani, N.; Kowdley, K.V.; McCullough, A.; Diehl, A.M.; Bass, N.M.; Neuschwander-Tetri, B.A.; Lavine, J.E.; Tonascia, J.; Unalp, A.; et al. Pioglitazone, Vitamin E, or Placebo for Nonalcoholic Steatohepatitis. N. Engl. J. Med. 2010, 362, 1675–1685. [Google Scholar] [CrossRef]
- Lavine, J.E.; Schwimmer, J.B.; Van Natta, M.L.; Molleston, J.P.; Murray, K.F.; Rosenthal, P.; Abrams, S.H.; Scheimann, A.O.; Sanyal, A.J.; Chalasani, N.; et al. Effect of Vitamin E or Metformin for Treatment of Nonalcoholic Fatty Liver Disease in Children and Adolescents. JAMA 2011, 305, 1659–1668. [Google Scholar] [CrossRef]
- Vilar-Gomez, E.; Vuppalanchi, R.; Gawrieh, S.; Ghabril, M.; Saxena, R.; Cummings, O.W.; Chalasani, N. Vitamin E Improves Transplant-Free Survival and Hepatic Decompensation Among Patients with Nonalcoholic Steatohepatitis and Advanced Fibrosis. Hepatology 2020, 71, 495–509. [Google Scholar] [CrossRef]
- Kwok, R.M.; Torres, D.M.; Harrison, S.A. Vitamin D and Nonalcoholic Fatty Liver Disease (NAFLD): Is It More than Just an Association? Hepatology 2013, 58, 1166–1174. [Google Scholar] [CrossRef]
- Kong, M.; Zhu, L.; Bai, L.; Zhang, X.; Chen, Y.; Liu, S.; Zheng, S.; Pandol, S.J.; Han, Y.-P.; Duan, Z. Vitamin D Deficiency Promotes Nonalcoholic Steatohepatitis through Impaired Enterohepatic Circulation in Animal Model. Am. J. Physiol. Gastrointest. Liver Physiol. 2014, 307, G883–G893. [Google Scholar] [CrossRef]
- Ding, N.; Yu, R.T.; Subramaniam, N.; Sherman, M.H.; Wilson, C.; Rao, R.; Leblanc, M.; Coulter, S.; He, M.; Scott, C.; et al. A Vitamin D Receptor/SMAD Genomic Circuit Gates Hepatic Fibrotic Response. Cell 2013, 153, 601–613. [Google Scholar] [CrossRef]
- Eliades, M.; Spyrou, E.; Agrawal, N.; Lazo, M.; Brancati, F.L.; Potter, J.J.; Koteish, A.A.; Clark, J.M.; Guallar, E.; Hernaez, R. Meta-Analysis: Vitamin D and Non-Alcoholic Fatty Liver Disease. Aliment. Pharmacol. Ther. 2013, 38, 246–254. [Google Scholar] [CrossRef] [PubMed]
- Liu, T.; Xu, L.; Chen, F.-H.; Zhou, Y.-B. Association of Serum Vitamin D Level and Nonalcoholic Fatty Liver Disease: A Meta-Analysis. Eur. J. Gastroenterol. Hepatol. 2020, 32, 140–147. [Google Scholar] [CrossRef]
- Pop, T.L.; Sîrbe, C.; Benţa, G.; Mititelu, A.; Grama, A. The Role of Vitamin D and Vitamin D Binding Protein in Chronic Liver Diseases. Int. J. Mol. Sci. 2022, 23, 10705. [Google Scholar] [CrossRef]
- Jaruvongvanich, V.; Ahuja, W.; Sanguankeo, A.; Wijarnpreecha, K.; Upala, S. Vitamin D and Histologic Severity of Nonalcoholic Fatty Liver Disease: A Systematic Review and Meta-Analysis. Dig. Liver Dis. 2017, 49, 618–622. [Google Scholar] [CrossRef]
- Guo, X.; Wang, C.; Yang, T.; Li, S.; Li, K.; Li, D. Vitamin D and Non-Alcoholic Fatty Liver Disease: A Meta-Analysis of Randomized Controlled Trials. Food Funct. 2020, 11, 7389–7399. [Google Scholar] [CrossRef]
- Eliades, M.; Spyrou, E. Vitamin D: A New Player in Non-Alcoholic Fatty Liver Disease? World J. Gastroenterol. 2015, 21, 1718–1727. [Google Scholar] [CrossRef]
- Abenavoli, L.; Larussa, T.; Corea, A.; Procopio, A.C.; Boccuto, L.; Dallio, M.; Federico, A.; Luzza, F. Dietary Polyphenols and Non-Alcoholic Fatty Liver Disease. Nutrients 2021, 13, 494. [Google Scholar] [CrossRef]
- Rahmani, S.; Asgary, S.; Askari, G.; Keshvari, M.; Hatamipour, M.; Feizi, A.; Sahebkar, A. Treatment of Non-Alcoholic Fatty Liver Disease with Curcumin: A Randomized Placebo-Controlled Trial. Phytother. Res. 2016, 30, 1540–1548. [Google Scholar] [CrossRef]
- Panahi, Y.; Kianpour, P.; Mohtashami, R.; Jafari, R.; Simental-Mendía, L.; Sahebkar, A. Efficacy and Safety of Phytosomal Curcumin in Non-Alcoholic Fatty Liver Disease: A Randomized Controlled Trial. Drug Res. 2017, 67, 244–251. [Google Scholar] [CrossRef]
- Zhong, S.; Fan, Y.; Yan, Q.; Fan, X.; Wu, B.; Han, Y.; Zhang, Y.; Chen, Y.; Zhang, H.; Niu, J. The Therapeutic Effect of Silymarin in the Treatment of Nonalcoholic Fatty Disease. Medicine 2017, 96, e9061. [Google Scholar] [CrossRef]
- Cheraghpour, M.; Imani, H.; Ommi, S.; Alavian, S.M.; Karimi-Shahrbabak, E.; Hedayati, M.; Yari, Z.; Hekmatdoost, A. Hesperidin Improves Hepatic Steatosis, Hepatic Enzymes, and Metabolic and Inflammatory Parameters in Patients with Nonalcoholic Fatty Liver Disease: A Randomized, Placebo-controlled, Double-blind Clinical Trial. Phytother. Res. 2019, 33, 2118–2125. [Google Scholar] [CrossRef] [PubMed]
- Jakubczyk, K.; Skonieczna-Żydecka, K.; Kałduńska, J.; Stachowska, E.; Gutowska, I.; Janda, K. Effects of Resveratrol Supplementation in Patients with Non-Alcoholic Fatty Liver Disease—A Meta-Analysis. Nutrients 2020, 12, 2435. [Google Scholar] [CrossRef] [PubMed]
- Mboumba Bouassa, R.-S.; Sebastiani, G.; Di Marzo, V.; Jenabian, M.-A.; Costiniuk, C.T. Cannabinoids and Chronic Liver Diseases. Int. J. Mol. Sci. 2022, 23, 9423. [Google Scholar] [CrossRef] [PubMed]
- Adejumo, A.C.; Alliu, S.; Ajayi, T.O.; Adejumo, K.L.; Adegbala, O.M.; Onyeakusi, N.E.; Akinjero, A.M.; Durojaiye, M.; Bukong, T.N. Cannabis Use Is Associated with Reduced Prevalence of Non-Alcoholic Fatty Liver Disease: A Cross-Sectional Study. PLoS ONE 2017, 12, e0176416. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.; Kim, W.; Kwak, M.-S.; Chung, G.E.; Yim, J.Y.; Ahmed, A. Inverse Association of Marijuana Use with Nonalcoholic Fatty Liver Disease among Adults in the United States. PLoS ONE 2017, 12, e0186702. [Google Scholar] [CrossRef]
- Le Strat, Y.; Le Foll, B. Obesity and Cannabis Use: Results from 2 Representative National Surveys. Am. J. Epidemiol. 2011, 174, 929–933. [Google Scholar] [CrossRef]
- Rajavashisth, T.B.; Shaheen, M.; Norris, K.C.; Pan, D.; Sinha, S.K.; Ortega, J.; Friedman, T.C. Decreased Prevalence of Diabetes in Marijuana Users: Cross-Sectional Data from the National Health and Nutrition Examination Survey (NHANES) III. BMJ Open 2012, 2, e000494. [Google Scholar] [CrossRef]
- Vidot, D.C.; Prado, G.; Hlaing, W.M.; Florez, H.J.; Arheart, K.L.; Messiah, S.E. Metabolic Syndrome Among Marijuana Users in the United States: An Analysis of National Health and Nutrition Examination Survey Data. Am. J. Med. 2016, 129, 173–179. [Google Scholar] [CrossRef]
- Millar, S.A.; Stone, N.L.; Bellman, Z.D.; Yates, A.S.; England, T.J.; O’Sullivan, S.E. A Systematic Review of Cannabidiol Dosing in Clinical Populations. Br. J. Clin. Pharmacol. 2019, 85, 1888–1900. [Google Scholar] [CrossRef]
- Arendt, B.M.; Mohammed, S.S.; Ma, D.W.L.; Aghdassi, E.; Salit, I.E.; Wong, D.K.H.; Guindi, M.; Sherman, M.; Heathcote, E.J.; Allard, J.P. Non-Alcoholic Fatty Liver Disease in HIV Infection Associated with Altered Hepatic Fatty Acid Composition. Curr. HIV Res. 2011, 9, 128–135. [Google Scholar] [CrossRef]
- Martínez-Sanz, J.; Calvo, M.V.; Serrano-Villar, S.; Montes, M.L.; Martín-Mateos, R.; Burgos-Santamaría, D.; Díaz-Álvarez, J.; Talavera-Rodríguez, A.; Rosas, M.; Moreno, S.; et al. Effects of HIV Infection in Plasma Free Fatty Acid Profiles among People with Non-Alcoholic Fatty Liver Disease. J. Clin. Med. 2022, 11, 3842. [Google Scholar] [CrossRef]
- De Almeida, C.F.; da Silva, P.S.; Cardoso, C.S.D.A.; Moreira, N.G.; Antunes, J.C.; de Andrade, M.M.; Silva, J.; Araujo, M.C.; Peres, W.A.F.; do Brasil, P.E.A.A.; et al. Relationship between Dietary Fatty Acid Intake with Nonalcoholic Fatty Liver Disease and Liver Fibrosis in People with HIV. Nutrients 2021, 13, 3462. [Google Scholar] [CrossRef]
- Kelly, E.M.; Dodge, J.L.; Bacchetti, P.; Sarkar, M.; French, A.L.; Tien, P.C.; Glesby, M.J.; Golub, E.T.; Augenbraun, M.; Plankey, M.; et al. Moderate Alcohol Use Is Not Associated with Fibrosis Progression in Human Immunodeficiency Virus/Hepatitis C Virus–Coinfected Women: A Prospective Cohort Study. Clin. Infect. Dis. 2017, 65, 2050–2056. [Google Scholar] [CrossRef]
- Kirkegaard-Klitbo, D.M.; Fuchs, A.; Stender, S.; Sigvardsen, P.E.; Kühl, J.T.; Kofoed, K.F.; Køber, L.; Nordestgaard, B.G.; Bendtsen, F.; Mocroft, A.; et al. Prevalence and Risk Factors of Moderate-to-Severe Hepatic Steatosis in Human Immunodeficiency Virus Infection: The Copenhagen Co-Morbidity Liver Study. J. Infect. Dis. 2020, 222, 1353–1362. [Google Scholar] [CrossRef]
- Carrieri, M.P.; Lions, C.; Sogni, P.; Winnock, M.; Roux, P.; Mora, M.; Bonnard, P.; Salmon, D.; Dabis, F.; Spire, B. Association between Elevated Coffee Consumption and Daily Chocolate Intake with Normal Liver Enzymes in HIV-HCV Infected Individuals: Results from the ANRS CO13 HEPAVIH Cohort Study. J. Hepatol. 2014, 60, 46–53. [Google Scholar] [CrossRef]
- Carrieri, M.P.; Protopopescu, C.; Marcellin, F.; Rosellini, S.; Wittkop, L.; Esterle, L.; Zucman, D.; Raffi, F.; Rosenthal, E.; Poizot-Martin, I.; et al. Protective Effect of Coffee Consumption on All-Cause Mortality of French HIV-HCV Co-Infected Patients. J. Hepatol. 2017, 67, 1157–1167. [Google Scholar] [CrossRef]
- Carrieri, M.P.; Protopopescu, C.; Marcellin, F.; Wittkop, L.; Lacombe, K.; Esterle, L.; Sogni, P.; Salmon-Ceron, D. The Impact of Coffee Consumption on Fibrosis and Steatosis in HIV-HCV Co-Infected Patients. J. Hepatol. 2018, 68, 845–847. [Google Scholar] [CrossRef]
- Yaya, I.; Marcellin, F.; Costa, M.; Morlat, P.; Protopopescu, C.; Pialoux, G.; Santos, M.E.; Wittkop, L.; Esterle, L.; Gervais, A.; et al. Impact of Alcohol and Coffee Intake on the Risk of Advanced Liver Fibrosis: A Longitudinal Analysis in HIV-HCV Coinfected Patients (ANRS CO-13 HEPAVIH Cohort). Nutrients 2018, 10, 705. [Google Scholar] [CrossRef]
- Sprinz, E.; Lazzaretti, R.K.; Kuhmmer, R.; Ribeiro, J.P. Dyslipidemia in HIV-Infected Individuals. Braz. J. Infect. Dis. 2010, 14, 575–588. [Google Scholar] [CrossRef]
- Grunfeld, C.; Pang, M.; Doerrler, W.; Shigenaga, J.K.; Jensen, P.; Feingold, K.R. Lipids, Lipoproteins, Triglyceride Clearance, and Cytokines in Human Immunodeficiency Virus Infection and the Acquired Immunodeficiency Syndrome. J. Clin. Endocrinol. Metab 1992, 74, 1045–1052. [Google Scholar] [CrossRef]
- Funderburg, N.T.; Mehta, N.N. Lipid Abnormalities and Inflammation in HIV Inflection. Curr. HIV/AIDS Rep. 2016, 13, 218–225. [Google Scholar] [CrossRef] [PubMed]
- Oosthuizen, W.; van Graan, A.; Kruger, A.; Vorster, H.H. Polyunsaturated Fatty Acid Intake Is Adversely Related to Liver Function in HIV-Infected Subjects: The THUSA Study. Am. J. Clin. Nutr. 2006, 83, 1193–1198. [Google Scholar] [CrossRef] [PubMed]
- Stonehouse, W.; Kruger, A.; Smuts, C.M.; Loots, D.T.; Wentzel-Viljoen, E.; Vorster, H.H. Plasma Polyunsaturated Fatty Acids and Liver Enzymes in HIV-Infected Subjects: The Prospective Urban and Rural Epidemiology (PURE) Study. Am. J. Clin. Nutr. 2010, 91, 729–735. [Google Scholar] [CrossRef] [PubMed]
- Fogacci, F.; Strocchi, E.; Veronesi, M.; Borghi, C.; Cicero, A.F.G. Effect of Omega-3 Polyunsaturated Fatty Acids Treatment on Lipid Pattern of HIV Patients: A Meta-Analysis of Randomized Clinical Trials. Mar. Drugs 2020, 18, 292. [Google Scholar] [CrossRef]
- Morvaridzadeh, M.; Sepidarkish, M.; Yavari, M.; Tahvilian, N.; Heydarian, A.; Khazdouz, M.; Farsi, F.; Persad, E.; Heshmati, J. The Effects of Omega-3 Fatty Acid Supplementation on Inflammatory Factors in HIV-Infected Patients: A Systematic Review and Meta-Analysis of Randomized Clinical Trials. Cytokine 2020, 136, 155298. [Google Scholar] [CrossRef]
- Seth, A.; Sherman, K.E. Fatty Liver Disease in Persons with HIV Infection. Top. Antivir. Med. 2019, 27, 75–82. [Google Scholar]
- Chaudhry, A.A.; Sulkowski, M.S.; Chander, G.; Moore, R.D. Hazardous Drinking Is Associated with an Elevated Aspartate Aminotransferase to Platelet Ratio Index in an Urban HIV-Infected Clinical Cohort. HIV Med. 2009, 10, 133–142. [Google Scholar] [CrossRef]
- Baum, M.K.; Rafie, C.; Lai, S.; Sales, S.; Page, J.B.; Campa, A. Alcohol Use Accelerates HIV Disease Progression. AIDS Res. Hum. Retrovir. 2010, 26, 511–518. [Google Scholar] [CrossRef]
- Hahn, J.A.; Samet, J.H. Alcohol and HIV Disease Progression: Weighing the Evidence. Curr. HIV/AIDS Rep. 2010, 7, 226–233. [Google Scholar] [CrossRef]
- Balagopal, A.; Philp, F.H.; Astemborski, J.; Block, T.M.; Mehta, A.; Long, R.; Kirk, G.D.; Mehta, S.H.; Cox, A.L.; Thomas, D.L.; et al. Human Immunodeficiency Virus-Related Microbial Translocation and Progression of Hepatitis C. Gastroenterology 2008, 135, 226–233. [Google Scholar] [CrossRef]
- Szabo, G. Mechanisms of Alcohol-Mediated Hepatotoxicity in Human-Immunodeficiency-Virus-Infected Patients. WJG 2011, 17, 2500. [Google Scholar] [CrossRef]
- Ganesan, M.; New-Aaron, M.; Dagur, R.S.; Makarov, E.; Wang, W.; Kharbanda, K.K.; Kidambi, S.; Poluektova, L.Y.; Osna, N.A. Alcohol Metabolism Potentiates HIV-Induced Hepatotoxicity: Contribution to End-Stage Liver Disease. Biomolecules 2019, 9, 851. [Google Scholar] [CrossRef]
- New-Aaron, M.; Thomes, P.G.; Ganesan, M.; Dagur, R.S.; Donohue, T.M.; Kusum, K.K.; Poluektova, L.Y.; Osna, N.A. Alcohol-Induced Lysosomal Damage and Suppression of Lysosome Biogenesis Contribute to Hepatotoxicity in HIV-Exposed Liver Cells. Biomolecules 2021, 11, 1497. [Google Scholar] [CrossRef]
- Sebastiani, G.; Saeed, S.; Lebouche, B.; de Pokomandy, A.; Szabo, J.; Haraoui, L.-P.; Routy, J.-P.; Wong, P.; Deschenes, M.; Ghali, P.; et al. Vitamin E Is an Effective Treatment for Nonalcoholic Steatohepatitis in HIV Mono-Infected Patients. AIDS 2020, 34, 237–244. [Google Scholar] [CrossRef]
- Guzmán-Fulgencio, M.; García-Álvarez, M.; Berenguer, J.; Jiménez-Sousa, M.Á.; Cosín, J.; Pineda-Tenor, D.; Carrero, A.; Aldámiz, T.; Álvarez, E.; López, J.C.; et al. Vitamin D Deficiency Is Associated with Severity of Liver Disease in HIV/HCV Coinfected Patients. J. Infect. 2014, 68, 176–184. [Google Scholar] [CrossRef]
- Terrier, B.; Carrat, F.; Geri, G.; Pol, S.; Piroth, L.; Halfon, P.; Poynard, T.; Souberbielle, J.-C.; Cacoub, P. Low 25-OH Vitamin D Serum Levels Correlate with Severe Fibrosis in HIV-HCV Co-Infected Patients with Chronic Hepatitis. J. Hepatol. 2011, 55, 756–761. [Google Scholar] [CrossRef]
- El-Maouche, D.; Mehta, S.H.; Sutcliffe, C.G.; Higgins, Y.; Torbenson, M.S.; Moore, R.D.; Thomas, D.L.; Sulkowski, M.S.; Brown, T.T. Vitamin D Deficiency and Its Relation to Bone Mineral Density and Liver Fibrosis in HIV–HCV Coinfection. Antivir. Ther. 2013, 18, 237–242. [Google Scholar] [CrossRef]
- Milic, J.; Menozzi, V.; Schepis, F.; Malagoli, A.; Besutti, G.; Franconi, I.; Raimondi, A.; Carli, F.; Mussini, C.; Sebastiani, G.; et al. Liver Steatosis and Nonalcoholic Fatty Liver Disease with Fibrosis Are Predictors of Frailty in People Living with HIV. AIDS 2020, 34, 1915–1921. [Google Scholar] [CrossRef]
- Nordmann, S.; Vilotitch, A.; Roux, P.; Esterle, L.; Spire, B.; Marcellin, F.; Salmon-Ceron, D.; Dabis, F.; Chas, J.; Rey, D.; et al. Daily Cannabis and Reduced Risk of Steatosis in Human Immunodeficiency Virus and Hepatitis C Virus-Co-Infected Patients (ANRS CO13-HEPAVIH). J. Viral Hepat. 2018, 25, 171–179. [Google Scholar] [CrossRef]
- Barré, T.; Rojas Rojas, T.; Lacombe, K.; Protopopescu, C.; Poizot-Martin, I.; Nishimwe, M.L.; Zucman, D.; Esterle, L.; Billaud, E.; Aumaitre, H.; et al. Cannabis Use and Reduced Risk of Elevated Fatty Liver Index in HIV-HCV Co-Infected Patients: A Longitudinal Analysis (ANRS CO13 HEPAVIH). Expert Rev. Anti-Infect. Ther. 2021, 19, 1147–1156. [Google Scholar] [CrossRef]
- Fuster, D.; So-Armah, K.; Cheng, D.M.; Coleman, S.M.; Gnatienko, N.; Lioznov, D.; Krupitsky, E.M.; Freiberg, M.S.; Samet, J.H. Lack of Association between Recent Cannabis Use and Advanced Liver Fibrosis among HIV-Positive Heavy Drinkers. Curr. HIV Res. 2021, 19, 324–331. [Google Scholar] [CrossRef] [PubMed]
- Kelly, E.M.; Dodge, J.L.; Sarkar, M.; French, A.L.; Tien, P.C.; Glesby, M.J.; Golub, E.T.; Augenbraun, M.; Plankey, M.; Peters, M.G. Marijuana Use Is Not Associated with Progression to Advanced Liver Fibrosis in HIV/Hepatitis C Virus–Coinfected Women. Clin. Infect. Dis. 2016, 63, 512–518. [Google Scholar] [CrossRef] [PubMed]
- Brunet, L.; Moodie, E.E.M.; Rollet, K.; Cooper, C.; Walmsley, S.; Potter, M.; Klein, M.B. Marijuana Smoking Does Not Accelerate Progression of Liver Disease in HIV–Hepatitis C Coinfection: A Longitudinal Cohort Analysis. Clin. Infect. Dis. 2013, 57, 663–670. [Google Scholar] [CrossRef]
- Kpewou, D.E.; Mensah, F.O.; Appiah, C.A.; Alidu, H.W.; Badii, V.S. Serum Vitamin E Deficiency among People Living with HIV and Undergoing Antiretroviral Therapy at Ho Teaching Hospital, Ghana. Heliyon 2021, 7, e07339. [Google Scholar] [CrossRef] [PubMed]
- Tang, A.M.; Graham, N.M.; Semba, R.D.; Saah, A.J. Association between Serum Vitamin A and E Levels and HIV-1 Disease Progression. AIDS 1997, 11, 613–620. [Google Scholar] [CrossRef]
- Graham, S.M.; Baeten, J.M.; Richardson, B.A.; Bankson, D.D.; Lavreys, L.; Ndinya-Achola, J.O.; Mandaliya, K.; Overbaugh, J.; McClelland, R.S. Higher Pre-Infection Vitamin E Levels Are Associated with Higher Mortality in HIV-1-Infected Kenyan Women: A Prospective Study. BMC Infect. Dis. 2007, 7, 63. [Google Scholar] [CrossRef]
- Guaraldi, G.; Milic, J. Vitamin E as a ‘Bridge’ Therapy for Nonalcoholic Steatohepatits in HIV: What Is Waiting on the Other Side of the Bridge? AIDS 2020, 34, 317–319. [Google Scholar] [CrossRef]
- Dao, C.N.; Patel, P.; Overton, E.T.; Rhame, F.; Pals, S.L.; Johnson, C.; Bush, T.; Brooks, J.T. The Study to Understand the Natural History of HIV and AIDS in the Era of Effective Therapy (SUN) Investigators Low Vitamin D among HIV-Infected Adults: Prevalence of and Risk Factors for Low Vitamin D Levels in a Cohort of HIV-Infected Adults and Comparison to Prevalence among Adults in the US General Population. Clin. Infect. Dis. 2011, 52, 396–405. [Google Scholar] [CrossRef]
- Chokuda, E.; Reynolds, C.; Das, S. Association of Low Vitamin D with Complications of HIV and AIDS: A Literature Review. Infect. Disord. Drug Targets 2020, 20, 122–142. [Google Scholar] [CrossRef]
- Goh, S.S.L.; Lai, P.S.M.; Tan, A.T.B.; Ponnampalavanar, S. Reduced Bone Mineral Density in Human Immunodeficiency Virus-Infected Individuals: A Meta-Analysis of Its Prevalence and Risk Factors: Supplementary Presentation. Osteoporos. Int. 2018, 29, 1683. [Google Scholar] [CrossRef]
- Milazzo, L.; Mazzali, C.; Bestetti, G.; Longhi, E.; Foschi, A.; Viola, A.; Vago, T.; Galli, M.; Parravicini, C.; Antinori, S. Liver-Related Factors Associated with Low Vitamin D Levels in HIV and HIV/HCV Coinfected Patients and Comparison to General Population. Curr. HIV Res. 2011, 9, 186–193. [Google Scholar] [CrossRef]
- Mandorfer, M.; Payer, B.A.; Schwabl, P.; Steiner, S.; Ferlitsch, A.; Aichelburg, M.C.; Stättermayer, A.F.; Ferenci, P.; Obermayer-Pietsch, B.; Grabmeier-Pfistershammer, K.; et al. Revisiting Liver Disease Progression in HIV/HCV-Coinfected Patients: The Influence of Vitamin D, Insulin Resistance, Immune Status, IL28B and PNPLA3. Liver Int. 2015, 35, 876–885. [Google Scholar] [CrossRef]
- Branch, A.D.; Barin, B.; Rahman, A.; Stock, P.; Schiano, T.D. Vitamin D Status of HIV-Positive Patients with Advanced Liver Disease Enrolled in the Solid Organ Transplantation in HIV Multi-Site Study. Liver Transplant. 2014, 20, 156–164. [Google Scholar] [CrossRef]
- Moreno-Pérez, O.; Portilla, J.; Escoín, C.; Alfayate, R.; Reus, S.; Merino, E.; Boix, V.; Bernabeu, A.; Giner, L.; Mauri, M.; et al. Impact of Vitamin D Insufficiency on Insulin Homeostasis and Beta Cell Function in Nondiabetic Male HIV-Infected Patients: Vitamin D, Insulin Homeostasis and HIV. HIV Med. 2013, 14, 540–548. [Google Scholar] [CrossRef]
- Bugianesi, E.; Moscatiello, S.; Ciaravella, M.F.; Marchesini, G. Insulin Resistance in Nonalcoholic Fatty Liver Disease. Curr. Pharm. Des. 2010, 16, 1941–1951. [Google Scholar] [CrossRef]
- Costiniuk, C.T.; Jenabian, M.-A. Cannabinoids and Inflammation: Implications for People Living with HIV. AIDS 2019, 33, 2273–2288. [Google Scholar] [CrossRef]
- Barré, T.; Sogni, P.; Zaegel-Faucher, O.; Wittkop, L.; Marcellin, F.; Carrieri, P.; Gervais, A.; Levier, A.; Rosenthal, E.; Salmon-Céron, D.; et al. Cannabis Use as a Protective Factor Against Overweight in HIV-Hepatitis C Virus Co-Infected People (ANRS CO13 HEPAVIH Cohort). AIDS Educ. Prev. 2022, 34, 272–290. [Google Scholar] [CrossRef]
- Carrieri, M.P.; Serfaty, L.; Vilotitch, A.; Winnock, M.; Poizot-Martin, I.; Loko, M.-A.; Lions, C.; Lascoux-Combe, C.; Roux, P.; Salmon-Ceron, D.; et al. Cannabis Use and Reduced Risk of Insulin Resistance in HIV-HCV Infected Patients: A Longitudinal Analysis (ANRS CO13 HEPAVIH). Clin. Infect. Dis. 2015, 61, 40–48. [Google Scholar] [CrossRef]
- Cohen, K.; Weizman, A.; Weinstein, A. Positive and Negative Effects of Cannabis and Cannabinoids on Health. Clin. Pharmacol. Ther. 2019, 105, 1139–1147. [Google Scholar] [CrossRef]
- Mboumba Bouassa, R.-S.; Needham, J.; Nohynek, D.; Singer, J.; Lee, T.; Bobeuf, F.; Samarani, S.; Del Balso, L.; Paisible, N.; Vertzagias, C.; et al. Safety and Tolerability of Oral Cannabinoids in People Living with HIV on Long-Term ART: A Randomized, Open-Label, Interventional Pilot Clinical Trial (CTNPT 028). Biomedicines 2022, 10, 3168. [Google Scholar] [CrossRef]
- Canada, H. Household Food Insecurity in Canada: Overview. Available online: https://www.canada.ca/en/health-canada/services/food-nutrition/food-nutrition-surveillance/health-nutrition-surveys/canadian-community-health-survey-cchs/household-food-insecurity-canada-overview.html (accessed on 9 February 2023).
- Gregory, C.A. Food Insecurity, Chronic Disease, and Health Among Working-Age Adults. Available online: https://ageconsearch.umn.edu/record/261813/ (accessed on 20 February 2023).
- Liu, Y.; Eicher-Miller, H.A. Food Insecurity and Cardiovascular Disease Risk. Curr. Atheroscler. Rep. 2021, 23, 24. [Google Scholar] [CrossRef] [PubMed]
- Seligman, H.K.; Schillinger, D. Hunger and Socioeconomic Disparities in Chronic Disease. N. Engl. J. Med. 2010, 363, 6–9. [Google Scholar] [CrossRef] [PubMed]
- Nkambule, S.J.; Moodley, I.; Kuupiel, D.; Mashamba-Thompson, T.P. Association between Food Insecurity and Key Metabolic Risk Factors for Diet-Sensitive Non-Communicable Diseases in Sub-Saharan Africa: A Systematic Review and Meta-Analysis. Sci. Rep. 2021, 11, 5178. [Google Scholar] [CrossRef] [PubMed]
- Kardashian, A.; Serper, M.; Terrault, N.; Nephew, L.D. Health Disparities in Chronic Liver Disease. Hepatology 2022. early view. [Google Scholar] [CrossRef] [PubMed]
- Golovaty, I.; Tien, P.C.; Price, J.C.; Sheira, L.; Seligman, H.; Weiser, S.D. Food Insecurity May Be an Independent Risk Factor Associated with Nonalcoholic Fatty Liver Disease among Low-Income Adults in the United States. J. Nutr. 2020, 150, 91–98. [Google Scholar] [CrossRef]
- Kardashian, A.; Dodge, J.L.; Terrault, N.A. Food Insecurity Is Associated with Mortality Among U.S. Adults with Nonalcoholic Fatty Liver Disease and Advanced Fibrosis. Clin. Gastroenterol. Hepatol. 2022, 20, 2790–2799.e4. [Google Scholar] [CrossRef]
- Pellowski, J.A.; Kalichman, S.C.; Matthews, K.A.; Adler, N. A Pandemic of the Poor: Social Disadvantage and the U.S. HIV Epidemic. Am. Psychol. 2013, 68, 197–209. [Google Scholar] [CrossRef]
- Muhammad, J.N.; Fernandez, J.R.; Clay, O.J.; Saag, M.S.; Overton, E.T.; Willig, A.L. Associations of Food Insecurity and Psychosocial Measures with Diet Quality in Adults Aging with HIV. AIDS Care 2019, 31, 554–562. [Google Scholar] [CrossRef]
- Tamargo, J.A.; Sherman, K.E.; Campa, A.; Martinez, S.S.; Li, T.; Hernandez, J.; Teeman, C.; Mandler, R.N.; Chen, J.; Ehman, R.L.; et al. Food Insecurity Is Associated with Magnetic Resonance–Determined Nonalcoholic Fatty Liver and Liver Fibrosis in Low-Income, Middle-Aged Adults with and without HIV. Am. J. Clin. Nutr. 2021, 113, 593–601. [Google Scholar] [CrossRef]
- Members, E.P.; Jensen, M.D.; Ryan, D.H.; Donato, K.A.; Apovian, C.M.; Ard, J.D.; Comuzzie, A.G.; Hu, F.B.; Hubbard, V.S.; Jakicic, J.M.; et al. Executive Summary: Guidelines (2013) for the Management of Overweight and Obesity in Adults. Obesity 2014, 22, S5–S39. [Google Scholar] [CrossRef]
- Vilar-Gomez, E.; Martinez-Perez, Y.; Calzadilla-Bertot, L.; Torres-Gonzalez, A.; Gra-Oramas, B.; Gonzalez-Fabian, L.; Friedman, S.L.; Diago, M.; Romero-Gomez, M. Weight Loss Through Lifestyle Modification Significantly Reduces Features of Nonalcoholic Steatohepatitis. Gastroenterology 2015, 149, 367–378.e5. [Google Scholar] [CrossRef]
- Fernández, T.; Viñuela, M.; Vidal, C.; Barrera, F. Lifestyle Changes in Patients with Non-Alcoholic Fatty Liver Disease: A Systematic Review and Meta-Analysis. PLoS ONE 2022, 17, e0263931. [Google Scholar] [CrossRef]
- Pugliese, N.; Plaz Torres, M.C.; Petta, S.; Valenti, L.; Giannini, E.G.; Aghemo, A. Is There an ‘Ideal’ Diet for Patients with NAFLD? Eur. J. Clin. Investig. 2022, 52, e13659. [Google Scholar] [CrossRef]
- Kawaguchi, T.; Charlton, M.; Kawaguchi, A.; Yamamura, S.; Nakano, D.; Tsutsumi, T.; Zafer, M.; Torimura, T. Effects of Mediterranean Diet in Patients with Nonalcoholic Fatty Liver Disease: A Systematic Review, Meta-Analysis, and Meta-Regression Analysis of Randomized Controlled Trials. Semin. Liver Dis. 2021, 41, 225–234. [Google Scholar] [CrossRef]
- Haigh, L.; Kirk, C.; El Gendy, K.; Gallacher, J.; Errington, L.; Mathers, J.C.; Anstee, Q.M. The Effectiveness and Acceptability of Mediterranean Diet and Calorie Restriction in Non-Alcoholic Fatty Liver Disease (NAFLD): A Systematic Review and Meta-Analysis. Clin. Nutr. 2022, 41, 1913–1931. [Google Scholar] [CrossRef]
- Kouvari, M.; Boutari, C.; Chrysohoou, C.; Fragkopoulou, E.; Antonopoulou, S.; Tousoulis, D.; Pitsavos, C.; Panagiotakos, D.B.; Mantzoros, C.S. ATTICA study Investigators Mediterranean Diet Is Inversely Associated with Steatosis and Fibrosis and Decreases Ten-Year Diabetes and Cardiovascular Risk in NAFLD Subjects: Results from the ATTICA Prospective Cohort Study. Clin. Nutr. 2021, 40, 3314–3324. [Google Scholar] [CrossRef]
- Yurtdaş, G.; Akbulut, G.; Baran, M.; Yılmaz, C. The Effects of Mediterranean Diet on Hepatic Steatosis, Oxidative Stress, and Inflammation in Adolescents with Non-Alcoholic Fatty Liver Disease: A Randomized Controlled Trial. Pediatr. Obes. 2022, 17, e12872. [Google Scholar] [CrossRef]
- George, E.S.; Reddy, A.; Nicoll, A.J.; Ryan, M.C.; Itsiopoulos, C.; Abbott, G.; Johnson, N.A.; Sood, S.; Roberts, S.K.; Tierney, A.C. Impact of a Mediterranean Diet on Hepatic and Metabolic Outcomes in Non-Alcoholic Fatty Liver Disease: The MEDINA Randomised Controlled Trial. Liver Int. 2022, 42, 1308–1322. [Google Scholar] [CrossRef]
- Khodami, B.; Hatami, B.; Yari, Z.; Alavian, S.M.; Sadeghi, A.; Varkaneh, H.K.; Santos, H.O.; Hekmatdoost, A. Effects of a Low Free Sugar Diet on the Management of Nonalcoholic Fatty Liver Disease: A Randomized Clinical Trial. Eur. J. Clin. Nutr. 2022, 76, 987–994. [Google Scholar] [CrossRef]
- Visseren, F.L.J.; Mach, F.; Smulders, Y.M.; Carballo, D.; Koskinas, K.C.; Bäck, M.; Benetos, A.; Biffi, A.; Boavida, J.-M.; Capodanno, D.; et al. 2021 ESC Guidelines on Cardiovascular Disease Prevention in Clinical Practice. Eur. Heart J. 2021, 42, 3227–3337. [Google Scholar] [CrossRef]
- Kistler, K.D.; Brunt, E.M.; Clark, J.M.; Diehl, A.M.; Sallis, J.F.; Schwimmer, J.B. Physical Activity Recommendations, Exercise Intensity, and Histological Severity of Nonalcoholic Fatty Liver Disease. Am. J. Gastroenterol. 2011, 106, 460–468. [Google Scholar] [CrossRef] [PubMed]
- Ryu, S.; Chang, Y.; Jung, H.-S.; Yun, K.E.; Kwon, M.-J.; Choi, Y.; Kim, C.-W.; Cho, J.; Suh, B.-S.; Cho, Y.K.; et al. Relationship of Sitting Time and Physical Activity with Non-Alcoholic Fatty Liver Disease. J. Hepatol. 2015, 63, 1229–1237. [Google Scholar] [CrossRef] [PubMed]
- Keating, S.E.; Hackett, D.A.; George, J.; Johnson, N.A. Exercise and Non-Alcoholic Fatty Liver Disease: A Systematic Review and Meta-Analysis. J. Hepatol. 2012, 57, 157–166. [Google Scholar] [CrossRef] [PubMed]
- Bacchi, E.; Negri, C.; Targher, G.; Faccioli, N.; Lanza, M.; Zoppini, G.; Zanolin, E.; Schena, F.; Bonora, E.; Moghetti, P. Both Resistance Training and Aerobic Training Reduce Hepatic Fat Content in Type 2 Diabetic Subjects with Nonalcoholic Fatty Liver Disease (the RAED2 Randomized Trial). Hepatology 2013, 58, 1287–1295. [Google Scholar] [CrossRef]
- Hashida, R.; Kawaguchi, T.; Bekki, M.; Omoto, M.; Matsuse, H.; Nago, T.; Takano, Y.; Ueno, T.; Koga, H.; George, J.; et al. Aerobic vs. Resistance Exercise in Non-Alcoholic Fatty Liver Disease: A Systematic Review. J. Hepatol. 2017, 66, 142–152. [Google Scholar] [CrossRef]
- Romero-Gómez, M.; Zelber-Sagi, S.; Trenell, M. Treatment of NAFLD with Diet, Physical Activity and Exercise. J. Hepatol. 2017, 67, 829–846. [Google Scholar] [CrossRef]
- Chauhan, M.; Singh, K.; Thuluvath, P.J. Bariatric Surgery in NAFLD. Dig. Dis. Sci. 2022, 67, 408–422. [Google Scholar] [CrossRef]
- Hallsworth, K.; Fattakhova, G.; Hollingsworth, K.G.; Thoma, C.; Moore, S.; Taylor, R.; Day, C.P.; Trenell, M.I. Resistance Exercise Reduces Liver Fat and Its Mediators in Non-Alcoholic Fatty Liver Disease Independent of Weight Loss. Gut 2011, 60, 1278–1283. [Google Scholar] [CrossRef]
- Kwak, M.-S.; Kim, D.; Chung, G.E.; Kim, W.; Kim, Y.J.; Yoon, J.-H. Role of Physical Activity in Nonalcoholic Fatty Liver Disease in Terms of Visceral Obesity and Insulin Resistance. Liver Int. 2015, 35, 944–952. [Google Scholar] [CrossRef]
- Bae, J.C.; Suh, S.; Park, S.E.; Rhee, E.J.; Park, C.Y.; Oh, K.W.; Park, S.W.; Kim, S.W.; Hur, K.Y.; Kim, J.H.; et al. Regular Exercise Is Associated with a Reduction in the Risk of NAFLD and Decreased Liver Enzymes in Individuals with NAFLD Independent of Obesity in Korean Adults. PLoS ONE 2012, 7, e46819. [Google Scholar] [CrossRef]
- Worm, N. Beyond Body Weight-Loss: Dietary Strategies Targeting Intrahepatic Fat in NAFLD. Nutrients 2020, 12, 1316. [Google Scholar] [CrossRef]
- Lai, J.C.; Tandon, P.; Bernal, W.; Tapper, E.B.; Ekong, U.; Dasarathy, S.; Carey, E.J. Malnutrition, Frailty, and Sarcopenia in Patients with Cirrhosis: 2021 Practice Guidance by the American Association for the Study of Liver Diseases. Hepatology 2021, 74, 1611–1644. [Google Scholar] [CrossRef]
- Eslamparast, T.; Montano-Loza, A.J.; Raman, M.; Tandon, P. Sarcopenic Obesity in Cirrhosis-The Confluence of 2 Prognostic Titans. Liver Int. 2018, 38, 1706–1717. [Google Scholar] [CrossRef]
- Anema, A.; Vogenthaler, N.; Frongillo, E.A.; Kadiyala, S.; Weiser, S.D. Food Insecurity and HIV/AIDS: Current Knowledge, Gaps, and Research Priorities. Curr. HIV/AIDS Rep. 2009, 6, 224–231. [Google Scholar] [CrossRef]
- Duran, A.C.F.L.; Almeida, L.B.; Segurado, A.a.C.; Jaime, P.C. Diet Quality of Persons Living with HIV/AIDS on Highly Active Antiretroviral Therapy. J. Hum. Nutr. Diet 2008, 21, 346–350. [Google Scholar] [CrossRef]
- Vancampfort, D.; Mugisha, J.; De Hert, M.; Probst, M.; Firth, J.; Gorczynski, P.; Stubbs, B. Global Physical Activity Levels among People Living with HIV: A Systematic Review and Meta-Analysis. Disabil. Rehabil. 2018, 40, 388–397. [Google Scholar] [CrossRef]
- Erlandson, K.M.; MaWhinney, S.; Wilson, M.; Gross, L.; McCandless, S.A.; Campbell, T.B.; Kohrt, W.M.; Schwartz, R.; Brown, T.T.; Jankowski, C.M. Physical Function Improvements with Moderate or High-Intensity Exercise Among Older Adults with or without HIV Infection. AIDS 2018, 32, 2317–2326. [Google Scholar] [CrossRef]
- Erlandson, K.M.; Lake, J.E. Fat Matters: Understanding the Role of Adipose Tissue in Health in HIV Infection. Curr. HIV/AIDS Rep. 2016, 13, 20–30. [Google Scholar] [CrossRef]
- Engelson, E.S.; Agin, D.; Kenya, S.; Werber-Zion, G.; Luty, B.; Albu, J.B.; Kotler, D.P. Body Composition and Metabolic Effects of a Diet and Exercise Weight Loss Regimen on Obese, HIV-Infected Women. Metabolism 2006, 55, 1327–1336. [Google Scholar] [CrossRef]
- Terry, L.; Sprinz, E.; Stein, R.; Medeiros, N.B.; Oliveira, J.; Ribeiro, J.P. Exercise Training in HIV-1-Infected Individuals with Dyslipidemia and Lipodystrophy. Med. Sci. Sport. Exerc. 2006, 38, 411–417. [Google Scholar] [CrossRef]
- Mutimura, E.; Crowther, N.J.; Cade, T.W.; Yarasheski, K.E.; Stewart, A. Exercise Training Reduces Central Adiposity and Improves Metabolic Indices in HAART-Treated HIV-Positive Subjects in Rwanda: A Randomized Controlled Trial. AIDS Res. Hum. Retrovir. 2008, 24, 15–23. [Google Scholar] [CrossRef] [PubMed]
- Becofsky, K.; Wing, E.J.; McCaffery, J.; Boudreau, M.; Wing, R.R. A Randomized Controlled Trial of a Behavioral Weight Loss Program for Human Immunodeficiency Virus-Infected Patients. Clin. Infect. Dis. 2017, 65, 154–157. [Google Scholar] [CrossRef] [PubMed]
- Reeds, D.N.; Pietka, T.A.; Yarasheski, K.E.; Cade, W.T.; Patterson, B.W.; Okunade, A.; Abumrad, N.A.; Klein, S. HIV Infection Does Not Prevent the Metabolic Benefits of Diet-Induced Weight Loss in Women with Obesity: Effects of Weight Loss in HIV+ Women. Obesity 2017, 25, 682–688. [Google Scholar] [CrossRef] [PubMed]
- Lake, J.E. The Fat of the Matter: Obesity and Visceral Adiposity in Treated HIV Infection. Curr. HIV/AIDS Rep. 2017, 14, 211–219. [Google Scholar] [CrossRef] [PubMed]
- Stanley, T.L.; Fourman, L.T.; Feldpausch, M.N.; Purdy, J.; Zheng, I.; Pan, C.S.; Aepfelbacher, J.; Buckless, C.; Tsao, A.; Kellogg, A.; et al. Effects of Tesamorelin on Non-Alcoholic Fatty Liver Disease in HIV: A Randomised, Double-Blind, Multicentre Trial. Lancet HIV 2019, 6, e821–e830. [Google Scholar] [CrossRef]
- Munro, S.; Dinatale, E.; Hartley, S.; St. Jacques, M.; Oursler, K.A. Barriers and Health Beliefs Related to Weight Management Among Veterans with Human Immunodeficiency Virus. Mil. Med. 2017, 182, e1596–e1602. [Google Scholar] [CrossRef]
- Policarpo, S.; Machado, M.V.; Cortez-Pinto, H. Telemedicine as a Tool for Dietary Intervention in NAFLD-HIV Patients during the COVID-19 Lockdown: A Randomized Controlled Trial. Clin. Nutr. ESPEN 2021, 43, 329–334. [Google Scholar] [CrossRef]
- Cinque, F.; Cespiati, A.; Lombardi, R.; Costantino, A.; Maffi, G.; Alletto, F.; Colavolpe, L.; Francione, P.; Oberti, G.; Fatta, E.; et al. Interaction between Lifestyle Changes and PNPLA3 Genotype in NAFLD Patients during the COVID-19 Lockdown. Nutrients 2022, 14, 556. [Google Scholar] [CrossRef]
- Montemayor, S.; Mascaró, C.M.; Ugarriza, L.; Casares, M.; Gómez, C.; Martínez, J.A.; Tur, J.A.; Bouzas, C. Intrahepatic Fat Content and COVID-19 Lockdown in Adults with NAFLD and Metabolic Syndrome. Nutrients 2022, 14, 3462. [Google Scholar] [CrossRef]
- López-González, Á.A.; Altisench Jané, B.; Masmiquel Comas, L.; Arroyo Bote, S.; González San Miguel, H.M.; Ramírez Manent, J.I. Impact of COVID-19 Lockdown on Non-Alcoholic Fatty Liver Disease and Insulin Resistance in Adults: A before and after Pandemic Lockdown Longitudinal Study. Nutrients 2022, 14, 2795. [Google Scholar] [CrossRef]
- Kwon, O.Y.; Choi, J.; Jang, Y. The Effectiveness of EHealth Interventions on Lifestyle Modification in Patients with Nonalcoholic Fatty Liver Disease: Systematic Review and Meta-Analysis. J. Med. Internet Res. 2023, 25, e37487. [Google Scholar] [CrossRef]
- Yarasheski, K.E.; Cade, W.T.; Overton, E.T.; Mondy, K.E.; Hubert, S.; Laciny, E.; Bopp, C.; Lassa-Claxton, S.; Reeds, D.N. Exercise Training Augments the Peripheral Insulin-Sensitizing Effects of Pioglitazone in HIV-Infected Adults with Insulin Resistance and Central Adiposity. Am. J. Physiol.-Endocrinol. Metab. 2011, 300, E243–E251. [Google Scholar] [CrossRef]
- Matthews, L.; Kleiner, D.E.; Chairez, C.; McManus, M.; Nettles, M.J.; Zemanick, K.; Morse, C.G.; Benator, D.; Kovacs, J.A.; Hadigan, C. Pioglitazone for Hepatic Steatosis in HIV/Hepatitis C Virus Coinfection. AIDS Res. Hum. Retrovir. 2015, 31, 961–966. [Google Scholar] [CrossRef]
- Kamolvisit, S.; Chirnaksorn, S.; Nimitphong, H.; Sungkanuparph, S. Pioglitazone for the Treatment of Metabolic-Associated Fatty Liver Disease in People Living with HIV and Prediabetes. Cureus 2021, 13, e19046. [Google Scholar] [CrossRef]
- Ajmera, V.H.; Cachay, E.; Ramers, C.; Vodkin, I.; Bassirian, S.; Singh, S.; Mangla, N.; Bettencourt, R.; Aldous, J.L.; Park, D.; et al. Novel MRI Assessment of Treatment Response in HIV-Associated NAFLD: A Randomized Trial of an SCD1 Inhibitor (ARRIVE Trial). Hepatology 2019, 70, 1531–1545. [Google Scholar] [CrossRef]
- ISRCTN-ISRCTN15410818: Investigating the Impact of Maraviroc on Liver Inflammation in Patients with HIV and Fatty Liver Disease. Available online: https://www.isrctn.com/ISRCTN15410818 (accessed on 10 February 2023).
- Guaraldi, G.; Maurice, J.B.; Marzolini, C.; Monteith, K.; Milic, J.; Tsochatzis, E.; Bhagani, S.; Morse, C.G.; Price, J.C.; Ingiliz, P.; et al. New Drugs for NASH and HIV Infection: Great Expectations for a Great Need. Hepatology 2020, 71, 1831–1844. [Google Scholar] [CrossRef]
- Maurice, J.B.; Lemoine, M. Are Separate Clinical Trials Still Required in Nonalcoholic Steatohepatitis for Patients with and Without Human Immunodeficiency Virus (HIV)? Clin. Infect. Dis. 2021, 72, 908–909. [Google Scholar] [CrossRef]
- Ryom, L.; Cotter, A.; De Miguel, R.; Béguelin, C.; Podlekareva, D.; Arribas, J.; Marzolini, C.; Mallon, P.; Rauch, A.; Kirk, O.; et al. 2019 Update of the European AIDS Clinical Society Guidelines for Treatment of People Living with HIV Version 10.0. HIV Med. 2020, 21, 617–624. [Google Scholar] [CrossRef]
- Cervo, A.; Milic, J.; Mazzola, G.; Schepis, F.; Petta, S.; Krahn, T.; Lebouche, B.; Deschenes, M.; Cascio, A.; Guaraldi, G.; et al. Prevalence, Predictors, and Severity of Lean Nonalcoholic Fatty Liver Disease in Patients Living with Human Immunodeficiency Virus. Clin. Infect. Dis. 2020, 71, e694–e701. [Google Scholar] [CrossRef]
- De, A.; Duseja, A.; Badhala, P.; Taneja, S.; Sharma, A.; Arora, S. Indian Patients with Human Immunodeficiency Virus Infection Have High Prevalence but Mild Severity of Non-Alcoholic Fatty Liver Disease. Diabetes Metab. Syndr. Clin. Res. Rev. 2022, 16, 102679. [Google Scholar] [CrossRef]
- Long, M.T.; Noureddin, M.; Lim, J.K. AGA Clinical Practice Update: Diagnosis and Management of Nonalcoholic Fatty Liver Disease in Lean Individuals: Expert Review. Gastroenterology 2022, 163, 764–774.e1. [Google Scholar] [CrossRef] [PubMed]
- Mohammed, S.S.; Aghdassi, E.; Salit, I.E.; Avand, G.; Sherman, M.; Guindi, M.; Heathcote, J.E.; Allard, J.P. HIV-Positive Patients With Nonalcoholic Fatty Liver Disease Have a Lower Body Mass Index and Are More Physically Active Than HIV-Negative Patients. JAIDS J. Acquir. Immune Defic. Syndr. 2007, 45, 432–438. [Google Scholar] [CrossRef] [PubMed]
- Wong, V.W.-S.; Wong, G.L.-H.; Chan, R.S.-M.; Shu, S.S.-T.; Cheung, B.H.-K.; Li, L.S.; Chim, A.M.-L.; Chan, C.K.-M.; Leung, J.K.-Y.; Chu, W.C.-W.; et al. Beneficial Effects of Lifestyle Intervention in Non-Obese Patients with Non-Alcoholic Fatty Liver Disease. J. Hepatol. 2018, 69, 1349–1356. [Google Scholar] [CrossRef] [PubMed]
- Milani, C.; Duranti, S.; Bottacini, F.; Casey, E.; Turroni, F.; Mahony, J.; Belzer, C.; Delgado Palacio, S.; Arboleya Montes, S.; Mancabelli, L.; et al. The First Microbial Colonizers of the Human Gut: Composition, Activities, and Health Implications of the Infant Gut Microbiota. Microbiol. Mol. Biol. Rev. 2017, 81, e00036-17. [Google Scholar] [CrossRef] [PubMed]
- Honda, K.; Littman, D.R. The Microbiome in Infectious Disease and Inflammation. Annu. Rev. Immunol. 2012, 30, 759–795. [Google Scholar] [CrossRef]
- Turnbaugh, P.J.; Ley, R.E.; Mahowald, M.A.; Magrini, V.; Mardis, E.R.; Gordon, J.I. An Obesity-Associated Gut Microbiome with Increased Capacity for Energy Harvest. Nature 2006, 444, 1027–1031. [Google Scholar] [CrossRef]
- Zhang, H.; DiBaise, J.K.; Zuccolo, A.; Kudrna, D.; Braidotti, M.; Yu, Y.; Parameswaran, P.; Crowell, M.D.; Wing, R.; Rittmann, B.E.; et al. Human Gut Microbiota in Obesity and after Gastric Bypass. Proc. Natl. Acad. Sci. USA 2009, 106, 2365–2370. [Google Scholar] [CrossRef]
- Wang, P.-X.; Deng, X.-R.; Zhang, C.-H.; Yuan, H.-J. Gut Microbiota and Metabolic Syndrome. Chin. Med. J. 2020, 133, 808–816. [Google Scholar] [CrossRef]
- Qin, J.; Li, Y.; Cai, Z.; Li, S.; Zhu, J.; Zhang, F.; Liang, S.; Zhang, W.; Guan, Y.; Shen, D.; et al. A Metagenome-Wide Association Study of Gut Microbiota in Type 2 Diabetes. Nature 2012, 490, 55–60. [Google Scholar] [CrossRef]
- Wang, Z.; Klipfell, E.; Bennett, B.J.; Koeth, R.; Levison, B.S.; DuGar, B.; Feldstein, A.E.; Britt, E.B.; Fu, X.; Chung, Y.-M.; et al. Gut Flora Metabolism of Phosphatidylcholine Promotes Cardiovascular Disease. Nature 2011, 472, 57–63. [Google Scholar] [CrossRef]
- Boursier, J.; Diehl, A.M. Implication of Gut Microbiota in Nonalcoholic Fatty Liver Disease. PLoS Pathog. 2015, 11, e1004559. [Google Scholar] [CrossRef]
- Schnabl, B.; Brenner, D.A. Interactions between the Intestinal Microbiome and Liver Diseases. Gastroenterology 2014, 146, 1513–1524. [Google Scholar] [CrossRef]
- Boursier, J.; Mueller, O.; Barret, M.; Machado, M.; Fizanne, L.; Araujo-Perez, F.; Guy, C.D.; Seed, P.C.; Rawls, J.F.; David, L.A.; et al. The Severity of NAFLD Is Associated with Gut Dysbiosis and Shift in the Metabolic Function of the Gut Microbiota. Hepatology 2016, 63, 764–775. [Google Scholar] [CrossRef]
- Krajmalnik-Brown, R.; Ilhan, Z.-E.; Kang, D.-W.; DiBaise, J.K. Effects of Gut Microbes on Nutrient Absorption and Energy Regulation. Nutr. Clin. Pract. 2012, 27, 201–214. [Google Scholar] [CrossRef]
- Le Chatelier, E.; Nielsen, T.; Qin, J.; Prifti, E.; Hildebrand, F.; Falony, G.; Almeida, M.; Arumugam, M.; Batto, J.-M.; Kennedy, S.; et al. Richness of Human Gut Microbiome Correlates with Metabolic Markers. Nature 2013, 500, 541–546. [Google Scholar] [CrossRef]
- Del Chierico, F.; Nobili, V.; Vernocchi, P.; Russo, A.; De Stefanis, C.; Gnani, D.; Furlanello, C.; Zandonà, A.; Paci, P.; Capuani, G.; et al. Gut Microbiota Profiling of Pediatric Nonalcoholic Fatty Liver Disease and Obese Patients Unveiled by an Integrated Meta-Omics-Based Approach. Hepatology 2017, 65, 451–464. [Google Scholar] [CrossRef]
- Ley, R.E.; Turnbaugh, P.J.; Klein, S.; Gordon, J.I. Microbial Ecology: Human Gut Microbes Associated with Obesity. Nature 2006, 444, 1022–1023. [Google Scholar] [CrossRef]
- Loomba, R.; Seguritan, V.; Li, W.; Long, T.; Klitgord, N.; Bhatt, A.; Dulai, P.S.; Caussy, C.; Bettencourt, R.; Highlander, S.K.; et al. Gut Microbiome-Based Metagenomic Signature for Non-Invasive Detection of Advanced Fibrosis in Human Nonalcoholic Fatty Liver Disease. Cell Metab. 2017, 25, 1054–1062.e5. [Google Scholar] [CrossRef]
- Aron-Wisnewsky, J.; Vigliotti, C.; Witjes, J.; Le, P.; Holleboom, A.G.; Verheij, J.; Nieuwdorp, M.; Clément, K. Gut Microbiota and Human NAFLD: Disentangling Microbial Signatures from Metabolic Disorders. Nat. Rev. Gastroenterol. Hepatol. 2020, 17, 279–297. [Google Scholar] [CrossRef]
- Svegliati-Baroni, G.; Patrício, B.; Lioci, G.; Macedo, M.P.; Gastaldelli, A. Gut-Pancreas-Liver Axis as a Target for Treatment of NAFLD/NASH. Int. J. Mol. Sci. 2020, 21, 5820. [Google Scholar] [CrossRef]
- Pérez-Montes de Oca, A.; Julián, M.T.; Ramos, A.; Puig-Domingo, M.; Alonso, N. Microbiota, Fiber, and NAFLD: Is There Any Connection? Nutrients 2020, 12, 3100. [Google Scholar] [CrossRef] [PubMed]
- Dillon, S.M.; Frank, D.N.; Wilson, C.C. The Gut Microbiome and HIV-1 Pathogenesis: A Two-Way Street. AIDS 2016, 30, 2737–2751. [Google Scholar] [CrossRef] [PubMed]
- Vesterbacka, J.; Rivera, J.; Noyan, K.; Parera, M.; Neogi, U.; Calle, M.; Paredes, R.; Sönnerborg, A.; Noguera-Julian, M.; Nowak, P. Richer Gut Microbiota with Distinct Metabolic Profile in HIV Infected Elite Controllers. Sci. Rep. 2017, 7, 6269. [Google Scholar] [CrossRef] [PubMed]
- Bourgi, K.; Wanjalla, C.; Koethe, J.R. Inflammation and Metabolic Complications in HIV. Curr. HIV/AIDS Rep. 2018, 15, 371–381. [Google Scholar] [CrossRef]
- Nowak, P.; Troseid, M.; Avershina, E.; Barqasho, B.; Neogi, U.; Holm, K.; Hov, J.R.; Noyan, K.; Vesterbacka, J.; Svärd, J.; et al. Gut Microbiota Diversity Predicts Immune Status in HIV-1 Infection. AIDS 2015, 29, 2409–2418. [Google Scholar] [CrossRef]
- Dubourg, G.; Surenaud, M.; Lévy, Y.; Hüe, S.; Raoult, D. Microbiome of HIV-Infected People. Microb. Pathog. 2017, 106, 85–93. [Google Scholar] [CrossRef]
- Lozupone, C.A.; Rhodes, M.E.; Neff, C.P.; Fontenot, A.P.; Campbell, T.B.; Palmer, B.E. HIV-Induced Alteration in Gut Microbiota: Driving Factors, Consequences, and Effects of Antiretroviral Therapy. Gut Microbes 2014, 5, 562–570. [Google Scholar] [CrossRef]
- Díaz-Delfín, J.; Domingo, P.; Giralt, M.; Villarroya, F. Maraviroc Reduces Cytokine Expression and Secretion in Human Adipose Cells without Altering Adipogenic Differentiation. Cytokine 2013, 61, 808–815. [Google Scholar] [CrossRef]
- Pérez-Matute, P.; Pérez-Martínez, L.; Aguilera-Lizarraga, J.; Blanco, J.R.; Oteo, J.A. Maraviroc Modifies Gut Microbiota Composition in a Mouse Model of Obesity: A Plausible Therapeutic Option to Prevent Metabolic Disorders in HIV-Infected Patients. Rev. Española Quimioter. 2015, 28, 200–206. [Google Scholar]
- Yanavich, C.; Perazzo, H.; Li, F.; Tobin, N.; Lee, D.; Zabih, S.; Morata, M.; Almeida, C.; Veloso, V.G.; Grinsztejn, B.; et al. A Pilot Study of Microbial Signatures of Liver Disease in Those with HIV Mono-Infection in Rio de Janeiro, Brazil. AIDS 2022, 36, 49–58. [Google Scholar] [CrossRef]
- Li, W.; Dowd, S.E.; Scurlock, B.; Acosta-Martinez, V.; Lyte, M. Memory and Learning Behavior in Mice Is Temporally Associated with Diet-Induced Alterations in Gut Bacteria. Physiol. Behav. 2009, 96, 557–567. [Google Scholar] [CrossRef]
- De Filippo, C.; Cavalieri, D.; Di Paola, M.; Ramazzotti, M.; Poullet, J.B.; Massart, S.; Collini, S.; Pieraccini, G.; Lionetti, P. Impact of Diet in Shaping Gut Microbiota Revealed by a Comparative Study in Children from Europe and Rural Africa. Proc. Natl. Acad. Sci. USA 2010, 107, 14691–14696. [Google Scholar] [CrossRef]
- Wu, G.D.; Chen, J.; Hoffmann, C.; Bittinger, K.; Chen, Y.-Y.; Keilbaugh, S.A.; Bewtra, M.; Knights, D.; Walters, W.A.; Knight, R.; et al. Linking Long-Term Dietary Patterns with Gut Microbial Enterotypes. Science 2011, 334, 105–108. [Google Scholar] [CrossRef]
- Rinninella, E.; Cintoni, M.; Raoul, P.; Lopetuso, L.R.; Scaldaferri, F.; Pulcini, G.; Miggiano, G.A.D.; Gasbarrini, A.; Mele, M.C. Food Components and Dietary Habits: Keys for a Healthy Gut Microbiota Composition. Nutrients 2019, 11, 2393. [Google Scholar] [CrossRef]
- Maurice, J.B.; Garvey, L.; Tsochatzis, E.A.; Wiltshire, M.; Cooke, G.; Guppy, N.; McDonald, J.; Marchesi, J.; Nelson, M.; Kelleher, P.; et al. Monocyte-Macrophage Activation Is Associated with Nonalcoholic Fatty Liver Disease and Liver Fibrosis in HIV Monoinfection Independently of the Gut Microbiome and Bacterial Translocation. AIDS 2019, 33, 805–814. [Google Scholar] [CrossRef]
- Angeli, P.; Bernardi, M.; Villanueva, C.; Francoz, C.; Mookerjee, R.P.; Trebicka, J.; Krag, A.; Laleman, W.; Gines, P. EASL Clinical Practice Guidelines for the Management of Patients with Decompensated Cirrhosis. J. Hepatol. 2018, 69, 406–460. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
| Author, Year, Country | Study Design | Nutrients | Study Cohort | Patients’ Characteristics (Sex, Age, BMI) | HIV Features (Duration of HIV Infection, cART, Viral Suppression) | Diagnostic Method for NAFLD/ NASH/Liver Fibrosis | Main Findings |
|---|---|---|---|---|---|---|---|
| Arendt et al., 2011, Canada [81] | Cross-sectional | Fatty Acids | 48 participants:
|
| HIV/NAFLD: 95% on cART, | HS: liver biopsy |
|
| Martínez-Sanz et al., 2022, Spain [82] | Cross-sectional | Fatty Acids | 53 participants:
|
| HIV/NAFLD: 100% on cART, 100% with viral suppression | HS: Abdominal Ultrasound |
|
| De Almeida et al., 2021, Brazil [83] | Cross-sectional | Fatty Acids, Carbohydrates, Fibers | 451 PWH | M 40%, age 45 (IQR 36–53) years, BMI 25 (23–29) kg/m2 | Duration HIV 10 (5–17) years, 97% on cART, 84% with viral suppression |
|
|
| Kelly et al., 2017, Canada/U.S. [84] | Prospective, median FU 10 years | Alcohol | 686 HIV/HCV-coinfected patients | F 100%, age 39.7 (±6) years, BMI 26.1 (±6), kg/m2 | 29% on cART | Liver fibrosis: FIB-4 |
|
| Kirkegaard-Klitbo et al., 2020, Danmark [85] | Cross-sectional | Alcohol | 453 PWH | M 86%, age 52.4 (46.8–61.0) years, BMI 24.7 (22.4–27.5) kg/m2 | Duration HIV 16 (8.3–23.1) years, 99% on cART, 97% with viral suppression | HS: computed tomography |
|
| Carrieri et al., 2014, France [86] | Prospective, median FU 3.3 years | Coffee, chocolate | 990 HIV/HCV coinfected patients (ANRS CO13 HEPAVIH cohort) | M 70%, age 45 (42–48) years | 91% on cART, 71% with viral suppression | N/A |
|
| Carrieri et al., 2017, France [87] | Prospective, median FU 5 years | Coffee | 1028 HIV/HCV coinfected patients (ANRS CO13 HEPAVIH cohort) | M 70%, age 49 (46–52) years | 94.5% on ART, 82.5% with viral suppression | Liver fibrosis: FIB-4 |
|
| Carrieri et al., 2018, France [88] | Cross-sectional | Coffee | 918 HIV/HCV coinfected patients (ANRS CO13 HEPAVIH cohort) | N/A | N/A | HS: N/A Liver fibrosis: LSM by TE and FIB-4 |
|
| Yaya et al., 2018, France [89] | Cross-sectional | Coffee | 1019 HIV/HCV coinfected patients (ANRS CO13 HEPAVIH cohort) | M 70%, age 47.8 (±6.4) years | 95% on cART | Liver fibrosis: FIB-4 |
|
| Author, Year, Country | Study Design | Nutrients of Interest | Study Cohort | Patients’ Characteristics (Sex, Age, BMI) | HIV Features (Duration of HIV Infection, cART, Viral Suppression) | Diagnostic Method for NAFLD/ NASH/Liver Fibrosis | Main Findings |
|---|---|---|---|---|---|---|---|
| Sebastiani et al., 2020, Canada [105] | Single-center, open-label, single-arm, clinical trial, FU 4 years | Vitamin E | 27 PWH with NASH | M 81%, age 54 (51–59) years, BMI 28 (25–32) kg/m2 | Duration HIV 23 (15–29) years, 100% on cART, 100% with viral suppression |
|
|
| Guzman-Fulgencio et al., 2013, Spain [106] | Cross-sectional | Vitamin D | 174 HIV/HCV-coinfected patients | M 75%, age 40.8 (37.3; 44.6) years, | 86% on cART, 71% with viral suppression | Liver fibrosis: liver biopsy |
|
| Terrier et al., 2011, France [107] | Cross-sectional | Vitamin D | 189 HIV/HCV-coinfected patients | M 77%, Age 39.5 (±4.8) years, BMI 22.7 (±3.2) kg/m2 | Duration HIV 12 (0.5–18.5) years, 82% on cART, 70% with <400 HIV-RNA copies | Liver fibrosis: liver biopsy |
|
| Milazzo et al., 2011, Italy [108] | Cross-sectional | Vitamin D | 237 patients
|
|
| Liver fibrosis: FIB-4, liver biopsy (20% of the cohort) |
|
| Mandorfer et al., 2015, [109] | Cross-sectional | Vitamin D | 86 HIV/HCV-coinfected patients | M 71%, age 38.7 (+9.6) years, BMI 23.2 (+4) kg/m2 | 71% on cART | Liver fibrosis: liver biopsy | Vitamin D deficiency was independently associated with liver fibrosis progression and higher portal pressure |
| El-Maouche et al., 2013 U.S. [110] | Cross-sectional | Vitamin D | 116 HIV/HCV-coinfected patients | M 63%, age 49.9 (46.5–53.3) years | 64% on cART, 79% with <400 HIV-RNA copies | Liver fibrosis: liver biopsy |
|
| Milic et al., 2020, Italy [111] | Cross-sectional | Vitamin D | 707 PWH | M 76%, age 53.5 (±8.2) years, BMI 24.6 (±4.2) kg/m2 | 100% on cART, 99% with viral suppression |
| Vitamin D deficiency was associated with NAFLD with liver fibrosis |
| Nordmann et al., 2018, France [112] | Cross-sectional | Cannabinoids | 838 HIV/HCV-coinfected patients (ANRS CO13 HEPAVIH cohort) | M 70%, age 44.9 (44.5–45.4) years | 92% on cART, 84% with viral suppression | HS: abdominal ultrasound | Daily cannabis use was independently associated with lower prevalence of HS |
| Barré et al., 2021, France [113] | Prospective, FU 5 years | Cannabinoids | 997 HIV/HCV-coinfected patients (ANRS CO13 HEPAVIH cohort) | N/A | N/A | HS: fatty liver index | Regular cannabis use was associated with a 55% lower risk of elevated fatty liver index |
| Fuster et al., 2021, Russia [114] | Cross-sectional | Cannabinoids | 248 PWH with high prevalence of alcohol abuse (93%) and HCV coinfection (88%) | M 73%, age 33 (30–37) years, BMI 22.5 (20.8–24.5) kg/m2 | N/A | Liver fibrosis: FIB-4, APRI, LSM by TE | Cannabis use was not associated with advanced liver fibrosis |
| Kelly et al., 2016, USA [115] | Prospective, FU 11 years | Cannabinoids | 575 HIV/HCV-coinfected patients | Entry visit: F 100%, age 40 (±6) years, BMI 26 (±6) kg/m2Last visit: F 100%, age 51 (±7) years, BMI 26 (±7) kg/m2 | Entry visit: 6% on cART, 7% with viral suppression Last visit: 63% on cART, 33% with viral suppression | Liver fibrosis: FIB-4, APRI | Cannabis use was not associated with progression to significant liver fibrosis |
| Brunet et al., 2014, Canada [116] | Prospective, FU 2.7 years | Cannabinoids | 690 HIV/HCV-coinfected patients | M 73%, age 43.9 (38.4–49.2) years, BMI 24.0 (21.2–26.8) kg/m2 | Duration HIV 18.0 (10.4–24.5) years, 54% with viral suppression | Liver fibrosis and cirrhosis: APRI | Cannabis use was not associated with liver fibrosis progression or cirrhosis |
| Author, Year, Country | Study Design | Lifestyle Intervention | Study Cohort | Patients’ Characteristics (Sex, Age, BMI) | HIV Features (Duration of HIV Infection, cART, Viral Suppression) | Diagnostic Method for NAFLD/ NASH | Main Findings |
|---|---|---|---|---|---|---|---|
| Sebastiani et al., 2020, Canada [105] | 24-week single-center, open-label, single-arm, clinical trial; FU 4 years | At baseline standardized dietary and physical activity recommendations plus a nutritional consultation | 27 PWH with NASH receiving vitamin E | M 81%, age 54 (51–59) years, BMI 28 (25–32) kg/m2 | Duration HIV 23 (15–29) years, 100% on cART, 100% with viral suppression | NASH: CAP + cytokeratin 18 (100% of the cohort); liver biopsy (15% of the cohort) | Standard lifestyle recommendations with nutritional consultations were not associated to BMI changes, after 48 months of follow-up |
| Stanley et al., 2019, USA [178] | 48-week, randomized, double-blind, multicenter trial | Nutritional counselling from clinical research nutritionists at baseline, 6 months, and 12 months | 61 PWH with NAFLD:
|
|
| NAFLD by HFF ≥ 5% with MRS | Nutritional counselling was not associated with significant weight loss, waist circumference reduction, changes in daily caloric, macronutrient, and alcohol intake or hours of physical activity, after 48 months of follow-up |
| Policarpo et al., 2021, Portugal [180] | Single-center, randomized control trial | Detailed tailored nutritional plan based on MD with a caloric deficit of 500 kcal driven by the nutritionist, plus exercise training counselling | 55 PWH with NAFLD
|
|
| NAFLD by abdominal ultrasound |
|
| Yarasheski et al., 2011, USA [185] | Single-center, randomized control trial | Exercise training program based on 1.5–2 h/day, 3 days/week, of supervised, progressive, combined aerobic conditioning and resistance training driven by a certified exercise trainer | 39 PWH with insulin resistance and central adiposity:
|
|
| HS by 1H-MRS |
|
| Author, Year, Country | Study Design | Treatment | Sample Size | Diagnostic Method for NAFLD/NASH/Liver Fibrosis | Main Findings |
|---|---|---|---|---|---|
| Sebastiani et al., 2020, Canada [105] | 24-week, single-center, open-label, single-arm trial | Vitamin E | 27 PWH with NASH |
| 24-week vitamin E treatment decreased liver inflammation (with ALT −27 units/L), steatosis (with CAP −22 dB/m), and hepatocyte apoptosis (with cytokeratin 18–123 units/L) |
| Matthews et al., 2015, U.S. [186] | 48-week, randomized, double-blind, placebo-controlled trial | Pioglitazone | 13 HIV/HCV-coinfected patients with NAFLD:
| NAFLD by HFF ≥ 5% with MRS | 48-week pioglitazone treatment significantly decreased hepatic fat from baseline (15.1% ± 7.0%) to week 48 (7.6% ± 3.9%), with a mean difference of −7.4% (p = 0.02), whereas placebo administration did not change hepatic fat content |
| Kamolvisit et al., 2021, Thailand [187] | 48-week, randomized, placebo-controlled trial | Pioglitazone | 98 PWH with prediabetes and MAFLD:
|
| 48-week pioglitazone treatment decreased HS and liver fibrosis, with a significantly higher change in CAP and LSM compared to placebo (−23.5 dB/m vs. 10.2 dB/m, p < 0.001 and −0.184 kPa vs. 0.554 kPa, p = 0.0016, respectively) |
| Ajmera et al., 2019, U.S. [188] | 12-week, double-blind, randomized, investigator-initiated, placebo-controlled trial | Aramchol | 50 PWH with NAFLD:
|
| 12-week Aramchol treatment did not reduce HS and liver fibrosis or change body fat and muscle composition |
| Stanley et al., 2019, U.S. [178] | 48-week, randomized, double-blind, multicenter trial | Tesamorelin | 61 PWH with NAFLD:
|
| 48-week tesamorelin treatment reduced hepatic fat content by 37% and prevented progression of liver fibrosis, with a significantly lower rate of liver fibrosis progression in the tesamorelin group compared to placebo (10.5% vs. 37.5%, p = 0.04) |
| MASH study, 2020, UK [189] | 48-week, multicenter, open-label, single-arm trial | Maraviroc | 13 PWH with NASH | NASH and liver fibrosis by liver biopsy | 48-week maraviroc treatment did not change HS, liver fibrosis, or NASH features |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cinque, F.; Cespiati, A.; Lombardi, R.; Guaraldi, G.; Sebastiani, G. Nutritional and Lifestyle Therapy for NAFLD in People with HIV. Nutrients 2023, 15, 1990. https://doi.org/10.3390/nu15081990
Cinque F, Cespiati A, Lombardi R, Guaraldi G, Sebastiani G. Nutritional and Lifestyle Therapy for NAFLD in People with HIV. Nutrients. 2023; 15(8):1990. https://doi.org/10.3390/nu15081990
Chicago/Turabian StyleCinque, Felice, Annalisa Cespiati, Rosa Lombardi, Giovanni Guaraldi, and Giada Sebastiani. 2023. "Nutritional and Lifestyle Therapy for NAFLD in People with HIV" Nutrients 15, no. 8: 1990. https://doi.org/10.3390/nu15081990
APA StyleCinque, F., Cespiati, A., Lombardi, R., Guaraldi, G., & Sebastiani, G. (2023). Nutritional and Lifestyle Therapy for NAFLD in People with HIV. Nutrients, 15(8), 1990. https://doi.org/10.3390/nu15081990