

Reliability and Validity of the Emotional Eater Questionnaire in Romanian Adults
 and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Ethics Approval
2.2. Data Management and Data Analysis
3. Results
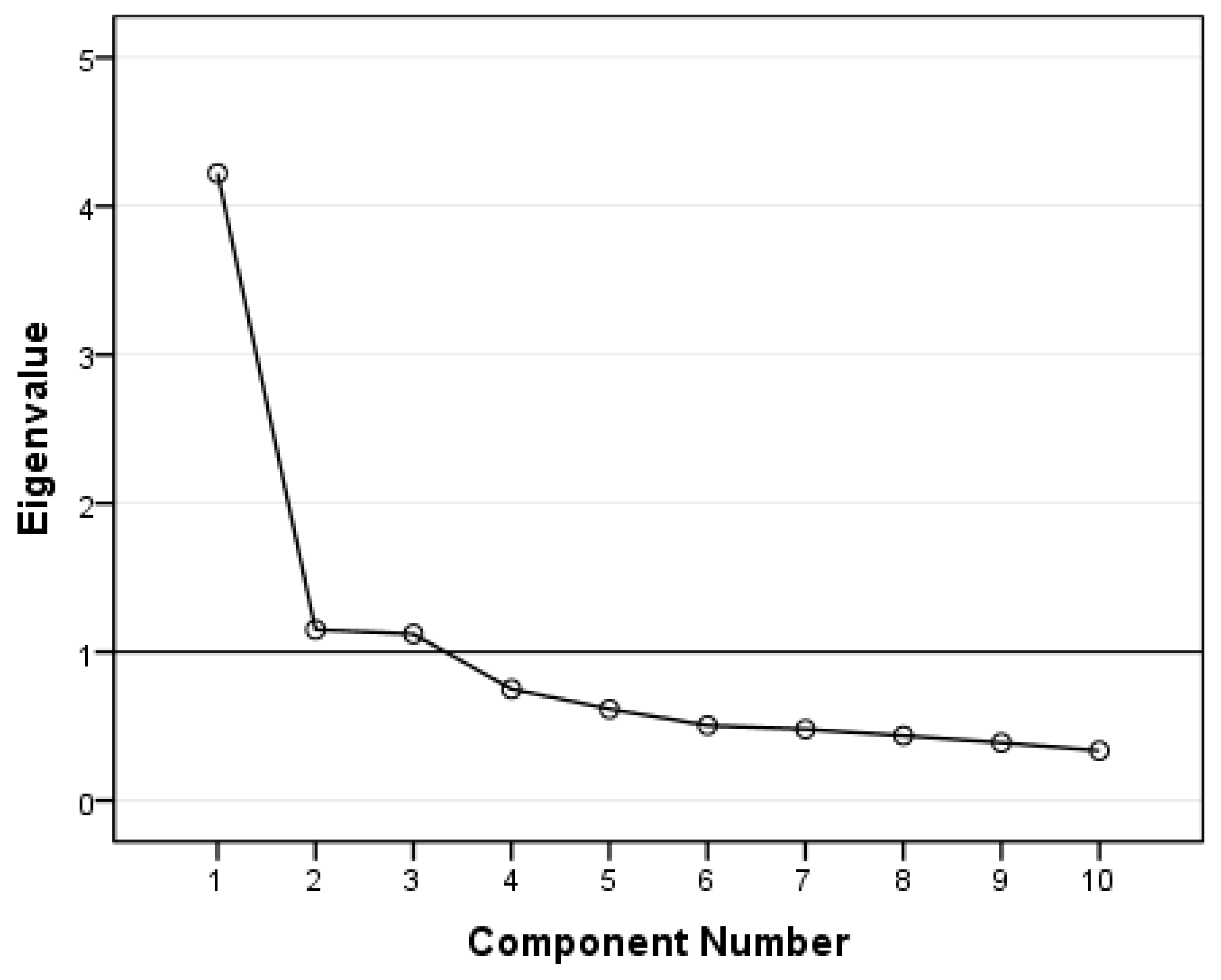
3.1. Construct Validity
3.2. Concurrent Validity
3.3. Reliability
3.4. Convergent Validity
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ans, A.H.; Anjum, I.; Satija, V.; Inayat, A.; Asghar, Z.; Akram, I.; Shrestha, B. Neurohormonal Regulation of Appetite and Its Relationship with Stress: A Mini Literature Review. Cureus 2018, 10, e3032. [Google Scholar] [CrossRef] [PubMed]
- Chrousos, G.P. Stress and Disorders of the Stress System. Nat. Rev. Endocrinol. 2009, 5, 374–381. [Google Scholar] [CrossRef] [PubMed]
- van Strien, T. Causes of Emotional Eating and Matched Treatment of Obesity. Curr. Diab. Rep. 2018, 18, 35. [Google Scholar] [CrossRef] [PubMed]
- Chao, A.M.; Jastreboff, A.M.; White, M.A.; Grilo, C.M.; Sinha, R. Stress, Cortisol, and Other Appetite-Related Hormones: Prospective Prediction of 6-Month Changes in Food Cravings and Weight. Obesity 2017, 25, 713–720. [Google Scholar] [CrossRef]
- LeBlanc, E.L.; Patnode, C.D.; Webber, E.M.; Redmond, N.; Rushkin, M.; O’Connor, E.A. Behavioral and Pharmacotherapy Weight Loss Interventions to Prevent Obesity-Related Morbidity and Mortality in Adults: An Updated Systematic Review for the U.S. Preventive Services Task Force; U.S. Preventive Services Task Force Evidence Syntheses, Formerly Systematic Evidence Reviews; Agency for Healthcare Research and Quality (US): Rockville, MD, USA, 2018. [Google Scholar]
- Langeveld, M.; DeVries, J.H. The Long-Term Effect of Energy Restricted Diets for Treating Obesity. Obesity 2015, 23, 1529–1538. [Google Scholar] [CrossRef]
- Willem, C.; Gandolphe, M.-C.; Roussel, M.; Verkindt, H.; Pattou, F.; Nandrino, J.-L. Difficulties in Emotion Regulation and Deficits in Interoceptive Awareness in Moderate and Severe Obesity. Eat. Weight Disord. 2019, 24, 633–644. [Google Scholar] [CrossRef]
- Chwyl, C.; Berry, M.P.; Manasse, S.M.; Forman, E.M. Rethinking Emotional Eating: Retrospective and Momentary Indices of Emotional Eating Represent Distinct Constructs. Appetite 2021, 167, 105604. [Google Scholar] [CrossRef]
- Bianciardi, E.; Imperatori, C.; Innamorati, M.; Fabbricatore, M.; Monacelli, A.M.; Pelle, M.; Siracusano, A.; Niolu, C.; Gentileschi, P. Measuring Knowledge, Attitudes, and Barriers to Medication Adherence in Potential Bariatric Surgery Patients. Obes. Surg. 2021, 31, 4045–4054. [Google Scholar] [CrossRef]
- Aparicio, E.; Canals, J.; Arija, V.; Henauw, S.D.; Michels, N. The Role of Emotion Regulation in Childhood Obesity: Implications for Prevention and Treatment. Nutr. Res. Rev. 2016, 29, 17–29. [Google Scholar] [CrossRef]
- Forman, E.M.; Butryn, M.L.; Hoffman, K.L.; Herbert, J.D. An Open Trial of an Acceptance-Based Behavioral Intervention for Weight Loss. Cogn. Behav. Pract. 2009, 16, 223–235. [Google Scholar] [CrossRef]
- O’Reilly, G.A.; Cook, L.; Spruijt-Metz, D.; Black, D.S. Mindfulness-Based Interventions for Obesity-Related Eating Behaviours: A Literature Review. Obes. Rev. 2014, 15, 453–461. [Google Scholar] [CrossRef] [PubMed]
- Reinelt, T.; Petermann, F.; Bauer, F.; Bauer, C. Emotion Regulation Strategies Predict Weight Loss during an Inpatient Obesity Treatment for Adolescents. Obes. Sci. Pract. 2020, 6, 293–299. [Google Scholar] [CrossRef] [PubMed]
- Garaulet, M.; Canteras, M.; Morales, E.; López-Guimera, G.; Sánchez-Carracedo, D.; Corbalán-Tutau, M.D. Validation of a Questionnaire on Emotional Eating for Use in Cases of Obesity: The Emotional Eater Questionnaire (EEQ). Nutr. Hosp. 2012, 27, 645–651. [Google Scholar] [CrossRef] [PubMed]
- González, M. Validación del Cuestionario de Comedor Emocional (CCE) en Chile. Gen 2018, 72, 21–24. [Google Scholar]
- Nashwan, A.J.; Villar, R.C.; Al-Qudimat, A.R.; Kader, N.; Alabdulla, M.; Abujaber, A.A.; Al-Jabry, M.M.; Harkous, M.; Philip, A.; Ali, R.; et al. Quality of Life, Sleep Quality, Depression, Anxiety, Stress, Eating Habits, and Social Bounds in Nurses during the Coronavirus Disease 2019 Pandemic in Qatar (The PROTECTOR Study): A Cross-Sectional, Comparative Study. J. Pers. Med. 2021, 11, 918. [Google Scholar] [CrossRef]
- Skolmowska, D.; Głąbska, D.; Guzek, D. Body Mass and Emotional Eating: Emotional Eater Questionnaire (EEQ) in the Polish Adolescents’ COVID-19 Experience (PLACE-19) Study. Nutrients 2022, 14, 828. [Google Scholar] [CrossRef]
- Arslantaş, H.; Dereboy, F.; Yüksel, R.; İnalkaç, S. Validity and Reliability of the Turkish Version of the Emotional Eater Questionnaire (EEQ-TR). Turk. J. Psychiatry 2020, 31, 122–130. [Google Scholar] [CrossRef]
- López-Moreno, M.; Garcés-Rimón, M.; Miguel, M.; Iglesias López, M.T. Adherence to Mediterranean Diet, Alcohol Consumption and Emotional Eating in Spanish University Students. Nutrients 2021, 13, 3174. [Google Scholar] [CrossRef]
- Navarro-Cruz, A.R.; Kammar-García, A.; Mancilla-Galindo, J.; Quezada-Figueroa, G.; Tlalpa-Prisco, M.; Vera-López, O.; Aguilar-Alonso, P.; Lazcano-Hernández, M.; Segura-Badilla, O. Association of Differences in Dietary Behaviours and Lifestyle with Self-Reported Weight Gain during the COVID-19 Lockdown in a University Community from Chile: A Cross-Sectional Study. Nutrients 2021, 13, 3213. [Google Scholar] [CrossRef]
- Bernabéu, E.; Marchena, C.; Iglesias, M.T. Factor Structure and Psychometric Properties of Emotional Eater Questionnaire (EEQ) in Spanish Colleges. Int. J. Environ. Res. Public. Health 2020, 17, 9090. [Google Scholar] [CrossRef]
- Barcın-Güzeldere, H.K.; Devrim-Lanpir, A. The Association Between Body Mass Index, Emotional Eating and Perceived Stress during COVID-19 Partial Quarantine in Healthy Adults. Public Health Nutr. 2022, 25, 43–50. [Google Scholar] [CrossRef] [PubMed]
- Sumalla-Cano, S.; Forbes-Hernández, T.; Aparicio-Obregón, S.; Crespo, J.; Eléxpuru-Zabaleta, M.; Gracia-Villar, M.; Giampieri, F.; Elío, I. Changes in the Lifestyle of the Spanish University Population during Confinement for COVID-19. Int. J. Environ. Res. Public. Health 2022, 19, 2210. [Google Scholar] [CrossRef] [PubMed]
- Madalı, B.; Alkan, Ş.B.; Örs, E.D.; Ayrancı, M.; Taşkın, H.; Kara, H.H. Emotional Eating Behaviors during the COVID-19 Pandemic: A Cross-Sectional Study. Clin. Nutr. ESPEN 2021, 46, 264–270. [Google Scholar] [CrossRef] [PubMed]
- Geisinger, K.F. Testing and Assessment in Cross-Cultural Psychology. In Handbook of Psychology: Assessment Psychology; Graham, J.R., Naglieri, J.A., Eds.; John Wiley & Sons, Inc.: Hoboken, NJ, USA, 2003; Volume 10, pp. 95–117. ISBN 978-0-471-38407-6. [Google Scholar]
- Serban, D.M.; Serban, C.L.; Ursoniu, S.; Putnoky, S.; Moleriu, R.D.; Putnoky, S. Mindful Eating Questionnaire: Validation and Reliability in Romanian Adults. Int. J. Environ. Res. Public. Health 2022, 19, 10517. [Google Scholar] [CrossRef] [PubMed]
- Tavakol, M.; Dennick, R. Making Sense of Cronbach’s Alpha. Int. J. Med. Educ. 2011, 2, 53–55. [Google Scholar] [CrossRef]
- Koo, T.K.; Li, M.Y. A Guideline of Selecting and Reporting Intraclass Correlation Coefficients for Reliability Research. J. Chiropr. Med. 2016, 15, 155–163. [Google Scholar] [CrossRef]
- Framson, C.; Kristal, A.R.; Schenk, J.M.; Littman, A.J.; Zeliadt, S.; Benitez, D. Development and Validation of the Mindful Eating Questionnaire. J. Am. Diet. Assoc. 2009, 109, 1439–1444. [Google Scholar] [CrossRef]
- Sidani, S.; Guruge, S.; Miranda, J.; Ford-Gilboe, M.; Varcoe, C. Cultural Adaptation and Translation of Measures: An Integrated Method. Res. Nurs. Health 2010, 33, 133–143. [Google Scholar] [CrossRef]
- Zachary, Z.; Brianna, F.; Brianna, L.; Garrett, P.; Jade, W.; Alyssa, D.; Mikayla, K. Self-Quarantine and Weight Gain Related Risk Factors during the COVID-19 Pandemic. Obes. Res. Clin. Pract. 2020, 14, 210–216. [Google Scholar] [CrossRef]
- López-Moreno, M.; López, M.T.I.; Miguel, M.; Garcés-Rimón, M. Physical and Psychological Effects Related to Food Habits and Lifestyle Changes Derived from COVID-19 Home Confinement in the Spanish Population. Nutrients 2020, 12, 3445. [Google Scholar] [CrossRef]
- Al-Musharaf, S. Prevalence and Predictors of Emotional Eating among Healthy Young Saudi Women during the COVID-19 Pandemic. Nutrients 2020, 12, 2923. [Google Scholar] [CrossRef] [PubMed]
- Bemanian, M.; Mæland, S.; Blomhoff, R.; Rabben, Å.K.; Arnesen, E.K.; Skogen, J.C.; Fadnes, L.T. Emotional Eating in Relation to Worries and Psychological Distress Amid the COVID-19 Pandemic: A Population-Based Survey on Adults in Norway. Int. J. Environ. Res. Public. Health 2021, 18, 130. [Google Scholar] [CrossRef] [PubMed]
- Betancourt-Núñez, A.; Torres-Castillo, N.; Martínez-López, E.; De Loera-Rodríguez, C.O.; Durán-Barajas, E.; Márquez-Sandoval, F.; Bernal-Orozco, M.F.; Garaulet, M.; Vizmanos, B. Emotional Eating and Dietary Patterns: Reflecting Food Choices in People with and without Abdominal Obesity. Nutrients 2022, 14, 1371. [Google Scholar] [CrossRef] [PubMed]
- Johnson, F.; Wardle, J. Variety, Palatability, and Obesity. Adv. Nutr. 2014, 5, 851–859. [Google Scholar] [CrossRef]
- Liu, S.; Globa, A.K.; Mills, F.; Naef, L.; Qiao, M.; Bamji, S.X.; Borgland, S.L. Consumption of Palatable Food Primes Food Approach Behavior by Rapidly Increasing Synaptic Density in the VTA. Proc. Natl. Acad. Sci. USA 2016, 113, 2520–2525. [Google Scholar] [CrossRef]
- Mehlig, K.; Bogl, L.H.; Hunsberger, M.; Ahrens, W.; Henauw, S.D.; Iguacel, I.; Jilani, H.; Molnár, D.; Pala, V.; Russo, P.; et al. Children’s Propensity to Consume Sugar and Fat Predicts Regular Alcohol Consumption in Adolescence. Public Health Nutr. 2018, 21, 3202–3209. [Google Scholar] [CrossRef]
- Werrij, M.Q.; Roefs, A.; Janssen, I.; Stapert, D.; Wolters, G.; Mulkens, S.; Hospers, H.J.; Jansen, A. Early Associations with Palatable Foods in Overweight and Obesity Are Not Disinhibition Related but Restraint Related. J. Behav. Ther. Exp. Psychiatry 2009, 40, 136–146. [Google Scholar] [CrossRef]
- Konttinen, H.; van Strien, T.; Männistö, S.; Jousilahti, P.; Haukkala, A. Depression, Emotional Eating and Long-Term Weight Changes: A Population-Based Prospective Study. Int. J. Behav. Nutr. Phys. Act. 2019, 16, 28. [Google Scholar] [CrossRef]
- Quick, V.M.; Byrd-Bredbenner, C.; Neumark-Sztainer, D. Chronic Illness and Disordered Eating: A Discussion of the Literature. Adv. Nutr. 2013, 4, 277–286. [Google Scholar] [CrossRef]
- Vancampfort, D.; Koyanagi, A.; Ward, P.B.; Veronese, N.; Carvalho, A.F.; Solmi, M.; Mugisha, J.; Rosenbaum, S.; De Hert, M.; Stubbs, B. Perceived Stress and Its Relationship With Chronic Medical Conditions and Multimorbidity Among 229,293 Community-Dwelling Adults in 44 Low-and Middle-Income Countries. Am. J. Epidemiol. 2017, 186, 979–989. [Google Scholar] [CrossRef]
- Choi, O.; Kim, J.; Lee, Y.; Lee, Y.; Song, K. Association between Stress and Dietary Habits, Emotional Eating Behavior and Insomnia of Middle-Aged Men and Women in Seoul and Gyeonggi. Nutr. Res. Pract. 2021, 15, 225–234. [Google Scholar] [CrossRef] [PubMed]
- Yoldas Ilktac, H.; Savci, C.; Cil Akinci, A. Nutritional Behavior during the COVID-19 Pandemic: The Association of Fear and Sleep Quality with Emotional Eating. Eat. Weight Disord. 2022, 27, 2673–2683. [Google Scholar] [CrossRef] [PubMed]
- Lorig, F.; Kießl, G.R.R.; Laessle, R.G. Stress-Related Cortisol Response and Laboratory Eating Behavior in Obese Women. Eat. Weight Disord. 2016, 21, 237–243. [Google Scholar] [CrossRef] [PubMed]
- Bailly, N.; Maître, I.; Amand, M.; Hervé, C.; Alaphilippe, D. The Dutch Eating Behaviour Questionnaire (DEBQ). Assessment of Eating Behaviour in an Aging French Population. Appetite 2012, 59, 853–858. [Google Scholar] [CrossRef] [PubMed]
- Dakanalis, A.; Zanetti, M.A.; Clerici, M.; Madeddu, F.; Riva, G.; Caccialanza, R. Italian Version of the Dutch Eating Behavior Questionnaire. Psychometric Proprieties and Measurement Invariance across Sex, BMI-Status and Age. Appetite 2013, 71, 187–195. [Google Scholar] [CrossRef]
- Samuel, L.; Cohen, M. Expressive Suppression and Emotional Eating in Older and Younger Adults: An Exploratory Study. Arch. Gerontol. Geriatr. 2018, 78, 127–131. [Google Scholar] [CrossRef]
- Elran Barak, R.; Shuval, K.; Li, Q.; Oetjen, R.; Drope, J.; Yaroch, A.L.; Fennis, B.M.; Harding, M. Emotional Eating in Adults: The Role of Sociodemographics, Lifestyle Behaviors, and Self-Regulation—Findings from a U.S. National Study. Int. J. Environ. Res. Public. Health 2021, 18, 1744. [Google Scholar] [CrossRef]
- Gross, J.J. Emotion Regulation: Affective, Cognitive, and Social Consequences. Psychophysiology 2002, 39, 281–291. [Google Scholar] [CrossRef]
- Klump, K.L.; Keel, P.K.; Racine, S.E.; Burt, S.A.; Burt, A.S.; Neale, M.; Sisk, C.L.; Boker, S.; Hu, J.Y. The Interactive Effects of Estrogen and Progesterone on Changes in Emotional Eating across the Menstrual Cycle. J. Abnorm. Psychol. 2013, 122, 131–137. [Google Scholar] [CrossRef]
- Hildebrandt, B.A.; Racine, S.E.; Keel, P.K.; Burt, S.A.; Neale, M.; Boker, S.; Sisk, C.L.; Klump, K.L. The Effects of Ovarian Hormones and Emotional Eating on Changes in Weight Preoccupation across the Menstrual Cycle. Int. J. Eat. Disord. 2015, 48, 477–486. [Google Scholar] [CrossRef]
- Fowler, N.; Keel, P.K.; Burt, S.A.; Neale, M.; Boker, S.; Sisk, C.L.; Klump, K.L. Associations between Ovarian Hormones and Emotional Eating across the Menstrual Cycle: Do Ovulatory Shifts in Hormones Matter? Int. J. Eat. Disord. 2019, 52, 195–199. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variables | Percentage (Count) | |
|---|---|---|
| Gender | Males | 27.5% (55) |
| Females | 72.5% (145) | |
| Excellent or very good perceived health status | Yes | 24.0% (48) |
| No | 76.0% (152) | |
| High level of perceived stress | Yes | 51.5% (103) |
| No | 48.5% (97) | |
| Relationship | In a relationship | 78.9% (146) |
| Single | 21.1% (39) | |
| Age (years) | 37.9 (11.7) * | |
| BMI (kg/m2) | 30.1 (4.8) * | |
| EEQ | Structure | ||
|---|---|---|---|
| Disinhibition | Type of Food | Guilt | |
| 6. Do you eat more of your favourite food and with less control when you are alone? | 0.789 | 0.109 | 0.103 |
| 10. How often do you feel that food controls you, rather than you controlling food? | 0.708 | 0.314 | 0.203 |
| 5. Do you eat when you are stressed, angry or bored? | 0.703 | 0.379 | −0.133 |
| 9. When you overeat while on a diet, do you give up and start eating without control, particularly food that you think is fattening? | 0.667 | 0.207 | 0.217 |
| 8. Do you feel less control over your diet when you are tired after work at night? | 0.648 | −0.020 | 0.397 |
| 2. Do you crave specific foods? | 0.107 | 0.774 | 0.170 |
| 3. Is it difficult for you to stop eating sweet things, especially chocolate? | 0.162 | 0.757 | 0.173 |
| 4. Do you have problems controlling the amount of certain types of food you eat? | 0.467 | 0.670 | 0.040 |
| 1. Do the weight scales have a great power over you? Can they change your mood? | 0.012 | 0.299 | 0.815 |
| 7. Do you feel guilty when eat “forbidden” foods, like sweets or snacks? | 0.361 | 0.069 | 0.783 |
| Cronbach’s Alpha (n = 200) | Intraclass Correlation Coefficient (n = 25) | |
|---|---|---|
| EEQ | 0.841 | 0.775 |
| Disinhibition | 0.829 | 0.780 |
| Type of food | 0.709 | 0.673 |
| Guilt | 0.654 | 0.584 |
| Variables | Measures | EE Score | p-Value | |
|---|---|---|---|---|
| Gender | Male | Mean (SD) | 10.7 (5.5) | <0.001 * |
| Female | 14.8 (5.7) | |||
| Excellent or very good perceived health status | Yes | Mean (SD) | 11.9 (6.0) | 0.017 * |
| No | 14.3 (5.8) | |||
| High level of perceived stress | Yes | Mean (SD) | 11.8 (5.5) | <0.001 * |
| No | 15.4 (5.8) | |||
| BMI (kg/m2) | r | 0.202 | 0.004 ** | |
| Age (years) | r | −0.190 | 0.007 ** | |
| Unstandardised Coefficients | Standardized Coefficient | 95% CI for B | |||
|---|---|---|---|---|---|
| B | Standard Error | Beta | |||
| Constant | 2.148 | 2.685 | −3.147 | 7.444 | |
| Feminine Gender | 4.247 | 0.825 | 0.321 | 2.619 | 5.875 |
| Lower perceived health status | 2.291 | 0.920 | 0.166 | 0.477 | 4.106 |
| High level of perceived stress | 2.543 | 0.728 | 0.215 | 1.108 | 3.978 |
| BMI (kg/m2) | 0.228 | 0.078 | 0.184 | 0.075 | 0.380 |
| Age (years) | −0.165 | 0.034 | −0.327 | −0.232 | −0.099 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Putnoky, S.; Serban, D.M.; Banu, A.M.; Ursoniu, S.; Serban, C.L. Reliability and Validity of the Emotional Eater Questionnaire in Romanian Adults. Nutrients 2023, 15, 26. https://doi.org/10.3390/nu15010026
Putnoky S, Serban DM, Banu AM, Ursoniu S, Serban CL. Reliability and Validity of the Emotional Eater Questionnaire in Romanian Adults. Nutrients. 2023; 15(1):26. https://doi.org/10.3390/nu15010026
Chicago/Turabian StylePutnoky, Salomeia, Denis Mihai Serban, Ancuta Mioara Banu, Sorin Ursoniu, and Costela Lacrimioara Serban. 2023. "Reliability and Validity of the Emotional Eater Questionnaire in Romanian Adults" Nutrients 15, no. 1: 26. https://doi.org/10.3390/nu15010026
APA StylePutnoky, S., Serban, D. M., Banu, A. M., Ursoniu, S., & Serban, C. L. (2023). Reliability and Validity of the Emotional Eater Questionnaire in Romanian Adults. Nutrients, 15(1), 26. https://doi.org/10.3390/nu15010026